
Abstract
Patients with refractory or relapsed (R/R) acute lymphoblastic leukemia (ALL) have a dismal prognosis of around 5% long-term survival when treated with cytotoxic chemotherapy and allogenic stem cell transplantation. T-cell immunobased strategies open up new therapeutic perspectives. Blinatumomab is the first of a new class of antibody constructs that was labeled bispecific T-cell engager (BiTE): it consists of two single chain variable fragment connected with a flexible linker, one side binding CD3, the other CD19. The tight binding and the close proximity to the CD19-positive B-cells and leukemic cells leads to non-major histocompatibility complex-restricted T-cell activation, polyclonal T-cell expansion and direct target cell killing. Applied by continuous infusion, blinatumomab achieves morphological complete response rates ranging from 39% to 69% in R/R ALL patients (compared to 25% after second-line chemotherapy) with prolonged overall survival (blinatumomab median overall survival, 7.7 months vs chemotherapy, 4.0 months). In comparison to conventional cytotoxic second-line protocols blinatumomab has a favorable safety profile. The main adverse event is related to the mode of action of blinatumomab: the induction of a cytokine-release syndrome that can be managed by interruption and/or the application of steroids or tocilizumab. Another typical complication is the occurrence of neurological side effects, such as seizures and encephalopathy. This neurotoxicity is reversible after application of steroids and/or withdrawal of blinatumomab. Blinatumomab has proven to be a powerful therapeutic option in R/R ALL patients both adult and pediatric because of its efficacy and limited toxicity.
Introduction
Precursor B-cell acute lymphoblastic leukemia (ALL) is a disease with ambiguous prognosis. Although in specific subgroups such as pediatric ALL the outcome is favorable, patients with refractory or relapsed (R/R) ALL or patients with persisting or resurfacing minimal residual disease (MRD) have a high risk of relapse. Progress has been achieved in risk stratification strategies based on MRD response assessment and identification of risk-associated genetic alterations.Citation1 Furthermore, new classes of agents such as proteasome inhibitors and new tyrosine kinase inhibitors have been introduced into the therapy of R/R ALL.Citation2,Citation3 Despite these improvements, the prognosis remains poor for patients in high risk groups.
T-cell based therapeutic strategies offer a new approach for the treatment of ALL overcoming several obstacles in the R/R ALL patient group such as chemoresistance or organ damage limiting further intensive cytotoxic therapy. Bispecific T-cell engager (BiTE) monoclonal antibody constructs activate T-memory effector cells and conduct them toward target cells with a certain surface antigen. The most prominent and advanced agent of this group is blinatumomab (Blincyto®), a CD3/CD19-bispecific construct that has proven its clinical value in the therapy of R/R CD19-positive ALL. This review is dedicated to the clinical usage of blinatumomab. Other bispecific constructs are currently evaluated on the basis of the BiTE blueprint (eg, CD3/EpCAM)Citation4 or further bispecific antibody constructs directed mainly against CD19, CD20 and CD22.Citation5 All of these antibody-based approaches engage the patient’s immune system. T-cell activation appears to be the most effective strategy but requires a significant number of activated T-cells. In patients with heavy pretreatment or recent allogenic hematopoietic stem cell transplantation (HSCT) blinatumomab may fail to induce sufficient T-cell activation to eliminate the CD19 positive cells.Citation6,Citation7
An alternative approach is the direct genetic manipulation of a patient’s T-cells: collected and purified CD3 positive T-cells are stably transfected by retro- or lentiviruses with a chimeric T-cell receptor (CAR). This CAR has an extracellular single chain variable fragment (scFv) head that binds with the specificity of a monoclonal antibody and can be chosen ad libitum. The intracellular part of the CAR mediates T-cell receptor (TCR) signaling when the scFv binds and leads to activation of the modified T-cell.Citation8,Citation9
Acute lymphoblastic leukemia
Epidemiology and biology
ALL is a hematological malignancy characterized by proliferation of immature lymphoid progenitor cells. The incidence of ALL is as low as 1.7/100,000 per year. It shows two peaks: the first one in preschool age with an incidence of 4.5/100,000 per year and the second one starting to increase at an age of around 50 years (incidence of 2/100,000 per year).Citation10 Although ALL is the most common malignancy in childhood accounting for nearly 30% of all pediatric cancer cases and 80% of all leukemias, it is rare in higher age and constitutes <1% of all malignancies regarding all age groups.Citation10
This review focuses on the role of blinatumomab in the therapy of ALL and, therefore, on CD19-positive precursor B-cell ALL. CD19 is expressed throughout long phases of B-cell development, expression starting at late pro-B-cell stage (CD34+CD10+CD19+), it persists during the complete B-cell development and does not disappear until maturation into plasma cell stage.Citation11 Almost every precursor B-cell ALL expresses CD19 consistently on the malignant blasts.Citation12 CD19 mediates costimulatory signals with CD21 and CD81 and seems to be essential for maintenance of the malignant proliferation by enhancing PI3K- and RAS-signaling.Citation13
ALL risk stratification used to be based on clinical, biological and genetic parameters. Age, sex, white blood cell count and central nervous system (CNS) involvement at diagnosis have a prognostic value. Immunophenotype, cytogenetic and molecular features still play an important role, but detection of MRD has proven to be the single most significant prognostic parameter and has replaced most of the clinical prognostic factors.Citation14 Besides the situation of frank relapse, the assessment of MRD is used to determine the indication for therapy with blinatumomab.
Prognosis
Although >80% of pediatric patients survive the disease for 5 years and longer, the 5-year survival rate in adults is around 40% in developed countries.Citation10 With intense, pediatric-derived and mainly BFM-based protocols, >95% of pediatric and up to 80% of adult patients may achieve a first complete remission (CR).Citation15 Although this approach results in improved outcome for young adults,Citation16 it is associated with a high morbidity and mortality in elderly patients resulting in over 20% therapy-related deaths during induction treatment. Therefore, most protocols for elderly patients involve multidrug combinations that are less toxic than the BFM-based protocols.Citation15 The outcome drops significantly after first relapse: in adult ALL the 3-year survival rate after first relapse treatment is 11%, after second 6% and after third or higher salvage 4%.Citation17 The same holds true for pediatric ALL on a higher level with a 10-year survival rate of around 40% after first relapse.Citation18 These proportions demonstrate that for high risk groups new therapeutic strategies such as the T-cell-based immunotherapeutic approaches are urgently needed.
Blinatumomab
Mechanism of action
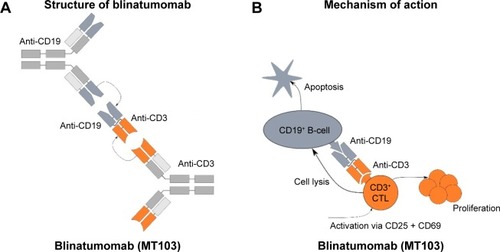
Blinatumomab is the first agent of a new class of antibody constructs that was labeled BiTE.Citation19 It contains two scFv, each formed by a pair of variable domains from heavy and light immunoglobulin chains. The two scFv proteins are connected with a flexible linker made of 25 amino acids (). Compared to the 150 kDa of a complete IgG antibody, the 55 kDa BiTE molecule is a small protein.
Figure 1 Blinatumomab: structure and mode of action.
Abbreviations: scFv, single chain variable fragment; TCR, T-cell receptor.
BiTE is a construct out of the fast growing field of bispecific antibodies which exhibit several advantages over monoclonal antibodies: adding CD3 as one component redirects T-cells to the target cell to enhance killing. Bispecific antibodies are able to bind two antigens simultaneously for either blocking two pathways or enhancing the specificity of the interaction.Citation20 The most frequent approach is the combination of a CD3 binding site with a tumor-specific target antigen, such as CD20, CD33, CEA, HER2 or CD2.Citation21 Bispecific antibodies in an IgG-like format have the advantage of a relatively long serum half-life, yet smaller molecules such as the scFv-based BiTEs are less immunogenic and have a better tissue penetration.Citation21 The first and till now only bispecific antibody that has advanced to Phase III trials is blinatumomab.Citation22
For blinatumomab the BiTE construct was armed with a mouse antibody recognizing CD3ε on one end, the constant part of the TCR complex that mediates its signaling. Therefore, blinatumomab is able to activate different fractions of T-cells including both CD8+ and CD4+ T-cells and regulatory T-cells (Tregs).Citation23 Binding itself does not activate the TCR unless a target cell is bound to the other scFv of the BiTE molecule. The second scFv construct of blinatumomab is the variable fragment of a murine anti-CD19 antibody. Application of blinatumomab in the presence of T-cells and CD19-positive cells (physiological B-cells as well as precursor B-cell leukemic blasts) leads to a very close linkage with multiple connections between the two different cell types which is caused by the small size and the flexibility of the internal linker of blinatumomab (). This close contact zone forms a cytolytic synapse and can be visualized by staining activated PKCθ which mediates the TCR activation: granzymes and perforin are exocytosed into the CD19 positive target cell and thereby induce its apoptosis.Citation24 The multiple, bivalent binding leads to a strong stimulus of the engaged T-cell which is independent of the TCR specificity and of major histocompatibility complex (MHC) class I antigen presentation or other costimulatory factors.Citation23 The strong activation of engaged T-cells leads to direct and serial lysis. Furthermore, blinatumomab induces polyclonal proliferation of activated T-cells which leads to an increased activity of blinatumomab 1–2 days after onset of application.Citation7,Citation25
Efficacy of blinatumomab in R/R ALL
In Phase II trials, blinatumomab was evaluated in patient cohorts with primary resistant or relapsed B-lineage ALL (R/R ALL), patient cohorts with poor outcome irrespective of the therapeutic regimen applied (). The first Phase II trial was conducted by the German Multicenter Study Group for Adult ALL (GMALL; NCT00198991 and NCT00198978): patients with persistent or relapsed MRD were included (15 patients with persistent, 5 patients with relapsed MRD). Within 4 cycles of blinatumomab with a dosage of 15 µg/m2/d, 80% of the patients became MRD negative. Five patients with BCR-ABL translocation resistant to tyrosine kinase inhibition (imatinib and/or dasatinib) were included, three of whom turned MRD negative. Nine of the responding patients received allogenic HSCT after blinatumomab treatment. After a median of 33 months, 61% of the patients persisted in CR.Citation26 The same study group, GMALL, was able to demonstrate a remarkable efficacy in R/R ALL with an open relapse of the leukemia, albeit not as good as in MRD level patients (NCT01209286). Because this trial was a Phase I with dose finding and because of a grade 4 cytokine-release syndrome (CRS) in one of the first 5 patients, the dosage of blinatumomab was lowered to 5 µg/m2/d for the first 7 days. Twenty-five of 36 patients (69%) achieved a complete or partial hematologic recovery within the first two blinatumomab cycles, of which 22 patients (61%) turned MRD negative. Thirteen of the responders (36% of the included patients) were able to proceed to allogenic HSCT. Median overall survival was 13.0 months with a medium follow-up time of 28.9 months, and median relapse-free survival was 8.8 months. Ten of the 36 patients (28%) were long-term survivors. All long-term survivors were MRD responders and showed a stronger T-cell expansion compared to the other patients.Citation27
Table 1 Published clinical trials on blinatumomab
In the development and assessment of new agents, a decrease of efficacy with increase of included patients and treatment centers is a frequent observation. The same holds true for blinatumomab. The international multicenter trial NCT01466179 included 189 patients suffering from R/R ALL. Inclusion criteria were more stringent than in the previous studies: first relapse within 12 months of first remission, relapse within 12 months after allogenic HSCT or no response to or relapse after salvage therapy.Citation7,Citation26,Citation28,Citation37 In this trial a fixed, not body surface area dependent dosage, was applied: a reduced dosage of 9 µg/day for the first 7 days, then the full dosage of 28 µg/day to reduce the risk of severe CRS or neurological toxicity. The following cycles started with 28 µg/day. A complete response was shown by 33% of the patients and an additional 10% of the patients showed a partial hematological response. For all included patients, median overall survival was 6.1 months after a median follow-up of 9.8 months. Thirty-two patients achieving complete or partial hematological recovery (40% of the responders) were able to proceed to allogenic HSCT.Citation28
Out of this patient cohort, Barlev et al conducted an estimation study to compare the long-term survival with blinatumomab to survival without this option: at month 60, an estimated 12.6% of the blinatumomab-treated patients were alive compared to 5.4% without blinatumomab (historical data). The mean overall survival increased from 39.8 months before blinatumomab-treatment to 76.1 months afterwards.Citation29
A phase III randomized controlled trial TOWER (NCT02013167) compared blinatumomab with conventional second-line standard chemotherapy (FLAG, fludarabine + high-dose cytarabine arabinoside ± anthracycline or HiDAC, high-dose cytarabine arabinoside-based regimen ± anthracycline or high-dose methotrexate-based regimen or clofarabine based regimens) in patients with R/R ALL. The inclusion criteria were similar to the above-mentioned NCT01466179 trial and blinatumomab dosing was the same: 9 µg/day ×7 days, followed by 28 µg/day ×21 days, subsequent cycles 28 µg/day ×28 days. Both groups received up to 5 cycles of blinatumomab or chemotherapy for induction and consolidation. Maintenance therapy, when indicated, consisted of 4-week-blinatumomab cycles every 3 months or low dose chemotherapy for 1 year.Citation30
The data of the blinatumomab group (271 patients) correspond well with the NCT01466179 trial results: the rate of complete response ± hematological recovery was 44%, the median overall survival 7.7 months (median follow-up of 11.7 months). This was significantly superior to the chemotherapy group data (134 patients): complete response ± hematological recovery rate was 25%, median overall survival 4.0 months. In both groups, 24% of the patients proceeded to allogenic HSCT. The Kaplan–Meier curves for overall survival separated significantly within the first 3 months with longer survival for blinatumomab. Interestingly, the two curves converged again between 15 and 18 months.Citation30
The first clinical trial (Phase I/II) on pediatric ALL was recently published by von Stackelberg et al (NCT01471782, ). The same body surface area adjusted dosage as in adults was confirmed: 5 µg/m2/d for 7 days after the onset of blinatumomab, followed by 15 µg/m2/d for the remaining 3 weeks of the first and the subsequent cycles. Seventy patients received the complete dosage. After the first two cycles, 27 patients (39%) had achieved CR, 14 patients in this group (20%) became MRD negative. The numbers seem to be similar to the results in R/R adult ALL, yet it is too early to draw long-term conclusions.Citation7
The restriction of the approval for blinatumomab on Philadelphia chromosome-negative (Ph-) ALL is not based on biological reasons but motivated by the existence of an alternative specific treatment, the tyrosine kinase inhibitor class of drugs. Blinatumomab shows the same efficacy in CD19 positive Ph+ ALL than in Ph- ALL. Eighty-nine percent of the Ph+ ALL patients in the ALCANTARA trial reached a MRD response in case of achieving CR, irrespective of resistance to chemo- and tyrosine kinase inhibitor-therapy.Citation31
Pharmacokinetics and dosage
Phase I clinical studies of blinatumomab have revealed a short serum half-life of 2–3 hours.Citation23 Therefore, application of blinatumomab was established as continuous infusion. This was facilitated by using a portable pump. Steady-state levels of blinatumomab were reached within 24 hours and persisted over the prolonged application period. Pharmacological studies revealed a mean volume of distribution of 4.52 L (±2.89) under steady-state conditions, mean half-life of 2.11 h (±1.42) and mean clearance of 2.92 L/h (±2.83).Citation32 These parameters are not influenced by age, sex, weight or renal function (if creatinine clearance is ≥30 mL/min). Patients with severe renal impairment or receiving dialysis were not included in the Phase I/II studies, so no recommendations for this patient group can be made. Yet renal excretion was low and, therefore, usage in selected cases might be justified. Hepatic dysfunction had no influence on blinatumomab clearance.Citation32,Citation33 Blinatumomab exhibits such a high efficacy that a dosage of 5 µg/m2 body surface per day (µg/m2/d) leads to a prompt and prolonged eradication of CD19-positive B-cells.Citation34 In patients with ALL, the increase of the dosage up to 30 µg/m2/d led to a significant rise of mainly neurotoxic but also inflammatory side effects.Citation7,Citation35 In patients with non-Hodgkin lymphoma (NHL) higher doses of blinatumomab were evaluated up to 90 µg/m2/d. Neurologic events led to the maximum-tolerated dose of 60 µg/m2/d in B-NHL, and stepwise dose escalation was tolerated better than a flat start with the target dose.Citation34 This trial by Bargou et al demonstrated a dose dependency of blinatumomab in inducing response in CD19-positive NHL.Citation34
Blinatumomab is applied as a 28-day cycle with a dosage of 28 µg/d respective (resp). 15 µg/m2/d in pediatric patients followed by a 14-day off-period before start of the following cycle. In order to prevent a CRS the first cycle is started with a dosage of 9 µg/d resp. 5 µg/m2/d in children for the first 7 days. Up to 5 cycles have been applied.Citation7,Citation28 Recently, the TOWER trial proposed a maintenance therapy of 4 additional cycles every 3 months.Citation30 It was observed repeatedly that peripheral T-cell levels of both CD4 and CD8 positive T-cells declined within a few hours after onset of blinatumomab due to redistribution of T-cells into the tissue and consumption by strong cytotoxic commitment. T-cell levels returned to baseline by days 1–2 and surmounted the initial level in many patients during the next days. This was explained by a polyclonal T-cell increase and is most probably the result of a T-cell proliferation induced by the initial activation by blinatumomab.Citation6,Citation25,Citation35 Treatment with blinatumomab led predominantly to an expansion of CD4+ T-cells with CD45RA/CCR7 phenotype and of effector memory CD8+ T-cells.Citation34,Citation36 In parallel, proinflammatory cytokines correlated with T-cell activation such as interferon gamma, tumor necrosis factor alpha, interleukin-2, interleukin-6, and interleukin-10 increased within day 1 and were detectable at elevated levels for 2 days. This transient elevation was often accompanied by fever which led to a CRS (see section below) in severe cases. This cytokine elevation was not observed in subsequent cycles.Citation35
Safety and tolerability
Since the first publications of clinical application of blinatumomab two specific adverse reactions stand out from the multitude of side effects in this heavily pretreated patient cohort. The first adverse reaction is the induction of a CRS which is directly correlated to the mode of action. The second striking side effect is frequent triggering of neurotoxicity.Citation19,Citation34 Systematic evaluation in clinical trials confirmed these observations.
Cytokine-release syndrome
In the trial of Topp et al with 36 patients, blinatumomab had to be terminated or discontinued due to severe CRS in 2 patients (6%). In total, 29 of the patients (81%) experienced fever/pyrexia ≤ grade 3.Citation37 In the large trial with 189 enrolled patients published in 2015 by Topp et al, only 3 patients (2%) developed grade 3 CRS.Citation28 Similarly, the TOWER trial reported CRS ≥ grade 3 in 13/267 (5%) patients receiving blinatumomab.Citation30
In a pediatric Phase I/II trial, grade 4 CRS was observed in 4 out of 49 patients (9%) of the dose escalation cohort. In Phase II extension cohort with the regular dosage of 5 µg/m2/d for the first 7 days and 15 µg/m2/d for the further treatment, only 4 of 70 patients (6%) developed ≥ grade 3 CRS.Citation7
The development of a CRS has to be expected within the first week of the first treatment cycle or the first days of the second cycle. Therefore, inpatient treatment is strongly advised during the first week of the first cycle and the first 5 days of the second cycle. CRS can be treated efficiently by withdrawal of blinatumomab, application of high-dose steroids and/or application of tocilizumab, a monoclonal IL-6-receptor antibody, the latter most probably not interfering with the efficacy of blinatumomab.Citation38
Neurotoxicity
Neurotoxic events such as seizures, irritability, disorientation, tremor and encephalopathy may be induced by activated T-cells binding CD19-positive cells in the CNS. The resulting cytokine release leads to local inflammation and disruption of the blood–brain barrier. The symptoms are, generally, reversible.Citation28,Citation38,Citation39 Neurotoxicity of blinatumomab is increased by but not limited to the occurrence of a CRS and appears after the first week of blinatumomab application.Citation28,Citation38 Topp et al reported neurological events causing a halt of blinatumomab application in 6 of 36 patients (17%).Citation37 The following larger study with 189 patients observed neurologic events grade 3 in 20 (11%) and grade 4 in 4 (2%) patients.Citation28 A pediatric Phase I/II study described 2 of 70 patients (3%) with grade 2 seizures which led to interruption of blinatumomab treatment.Citation7 The rate of neurotoxic events ≥ grade 3 in the randomized controlled TOWER trial was comparable between blinatumomab and chemotherapy with 25/267 (9%) vs 9/109 (8%), respectively.Citation30
Since neurotoxic adverse events also seem to be inflammation mediated, the therapeutic options are similar to those for the treatment of CRS: interruption of blinatumomab, application of high-dose steroids and/or application of tocilizumab.
Other severe adverse events
In a trial including 189 patients with R/R ALL, three deaths caused by severe infections (Escherichia coli, candida and unknown) were attributed to the therapy with blinatumomab by the investigators.Citation40 A heavily pretreated 5-year-old boy succumbed to cardiac failure under a grade 4 CRS and tumor lysis syndrome in Phase I part of the pediatric blinatumomab trial conducted by von Stackelberg et al.Citation7,Citation41 The same trial reports a fatal respiratory failure related to a grade 4 CRS.Citation7 Common adverse events were related to the mode of action of blinatumomab, such as pyrexia, fatigue, headache, tremor, edema, nausea and diarrhea. The most frequent grade ≥3 adverse events were anemia (36%), thrombocytopenia (21%) and hypokalemia (17%).Citation28,Citation37,Citation42
The TOWER trial compared blinatumomab therapy with intensive second-line chemotherapy in a randomized controlled fashion. In a cohort of 405 patients with R/R ALL it described adverse events ≥ grade 3 in 87% of patients in the blinatumomab group and in 92% in the chemotherapy group. Fatal events were reported in 19% vs 17% of the patients. After adjustment for treatment duration, the event rate for serious adverse events was 3.5 per patient-year in the blinatumomab cohort vs 6.4 per patient-year in the chemotherapy group.Citation30
CD19-depletion
Therapy with blinatumomab leads to a profound depletion of CD19-positive cells. CD19 expression is restricted to B-cell lineage committed cells. CD19 deficiency seems to be a very rare condition in humans. Only very few cases are described: in four patients of two unrelated families, a frameshift mutation leads to loss of function of the cytoplasmatic domain of the CD19 receptor.Citation43 Apart from hypogammaglobulinemia, no nonimmunological pathology was observed. The long-term off-target effects of blinatumomab, therefore, seem to be restricted to the impairment of the B-cell compartment. As we know from therapy with rituximab, a CD20 monoclonal antibody, recovery of the B-cells could take over a year with the need of long-term immunoglobulin substitution.Citation44
Escape mechanisms
By binding to the constant CD3ε component of the TCR, blinatumomab is capable of engaging multiple T-cell subsets such as CD3 positive CD8 and CD4 positive T-cells as well as regulatory (Tregs) T-cells.Citation23 The engaged T-cell may execute direct cytolysis or initiate its own proliferation; however, both effects are not restricted to specific T-cell subsets, specific TCRs, MHC class I molecules, neither are they dependent on a specific immune environment.Citation23 Therefore, the broad mode of T-cell engagement of blinatumomab may overcome escape mechanisms of other immune therapies induced by immune editing, MHC downregulation or modulation of the environment by specific selection pressure.Citation25,Citation45
Activity of blinatumomab depends on the expression of CD19 on the target cells. Emergence of CD19 negative ALL blast populations has been observed under CD19 targeted approaches such as blinatumomab or CD19-directed chimeric antigen receptor (CAR) T-cell therapy. Clinical data from the first trials and clinical observations show a CD19 negative relapse in 10%–20% of the patients.Citation26,Citation37 An important mechanism of CD19 escape relapse seems rather to be due to disrupted CD19 membrane trafficking than to the outgrowth of a CD19-negative progenitor cell or myeloid lineage shift.Citation46 MLL-rearranged ALL is a disease originating from very immature B-cell precursors. In a child with MLL-rearranged ALL, a CD19 negative relapse with myeloid phenotype was recently described under therapy with blinatumomab.Citation47 It will be essential to further describe the underlying biological processes of CD19 loss to predict and prevent relapses.
Aldoss et al have observed a number of CD19-positive ALL relapses in an extramedullary, lymphoma-like pattern.Citation48 Such manifestations might be overcome by higher dosages of blinatumomab, as recommended for NHL.Citation34
Prediction factors
Therapy with blinatumomab is highly expensive. Furthermore, it prohibits any simultaneous immunosuppressive cytotoxic therapy for the period of application. Therefore, it would be of high interest to predict patient cohorts which will benefit from such a high-priced therapy and those in which it will only lead to a delay of further cytotoxic therapy. We learned from the exploration of MRD that the initial therapeutic response of ALL has a strong correlation with outcome.Citation49 Zugmaier et al described a similar observation: of 10 long-surviving patients, all belonged to the group of 25 patients who had reached MRD negativity within the first two cycles in a cohort of 36 R/R ALL patients. In addition, long-term survivors had a stronger T-cell expansion compared to the patients with an overall survival of <30 months.Citation27
In a recent study, Duell et al were able to predict the response to blinatumomab with the level of regulatory T-cells at start of blinatumomab therapy. Regulatory T-cells were T-cells defined by coexpression of CD4/CD25/FOXP3. Patients responding had a mean of 4.8% of regulatory T-cells (22 patients, 95% confidence interval: 1.8%–8.3%) compared to 10.3% in nonresponders (20 patients, 95% confidence interval: 3.4%–65.9%). The cutoff of 8.525% regulatory T-cells was able to identify all blinatumomab responders and excluded 70% of the nonresponders. The study described a 1.7-fold upregulation of PD-1 on the regulatory T-cells in vitro under exposure to blinatumomab. To overcome the regulatory T-cell-mediated resistance to blinatumomab the authors propose a prior in vivo depletion of regulatory T-cells and discuss the feasibility of a simultaneous therapy with a PD-1 inhibitor.Citation50
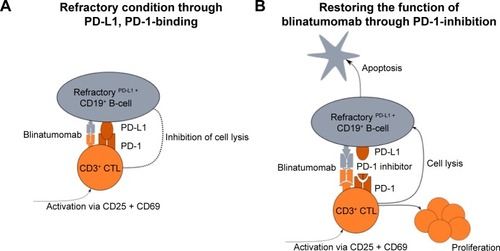
An interesting in vitro study of ALL patient samples suggests a correlation between PD-L1 expression on ALL blasts and resistance to blinatumomab therapy: PD-L1 expression on leukemic cells was higher in relapsed or blinatumomab-refractory ALL patients compared to leukemic cells of primary, nonblinatumomab treated ALL patients. Correspondingly, the expression of the T-cell exhaustion marker PD-1 was higher in ALL patients compared to healthy controls. Kohnke et al described a patient resistant to blinatumomab, who displayed an increase of PD-L1 expressing B-precursor ALL cells.Citation51 These observations support a model in which the PD-1/PD-L1-mediated T-cell suppression leads to resistance to blinatumomab therapy (). Treatment of patient-derived cells with a PD-1 inhibitor was able to re-sensitize those cells to the action of blinatumomab (). In fact, one ALL patient refractory to blinatumomab showed a response after the simultaneous application of pembrolizumab, a PD-1 inhibitor with blinatumomab.Citation52 These data are promising starting points for further research in the prediction of individual blinatumomab efficacy.
Figure 2 PD-L1 expression is a possible escape mechanism for the action of blinatumomab.
Abbreviation: ALL, acute lymphoblastic leukemia.
Conclusion and outlook
Blinatumomab is a BiTE construct that exhibits activity in adult and pediatric patients with R/R ALL in an MRD or open leukemic setting. Its efficacy is significantly higher in respect of induction of complete response and survival duration compared to cytotoxic second-line treatment protocols and displays a favorable safety profile.Citation30 The main risk is the induction of a CRS that has to be expected within the first week of the first cycle or the first days of the second cycles. Neurotoxicity seems to be time related to CRS and also occurs during the first days of blinatumomab application. Therefore, inpatient treatment is strongly advised during the first days of blinatumomab application. The mode of application is comparably straightforward: Blinatumomab is applied continuously over 4 weeks by a small portable pump. As soon as the risk period of the first week is over, it can be administered in an out-patient setting. Blinatumomab shows efficacy in any malignoma expressing superficial CD19, irrespective of genetic alterations such as the Philadelphia translocation.Citation31
A direct comparison to other T-cell therapies such as CAR-T-cell application is pending. Although first clinical CAR-T-cell trials report higher response rates, the severity of side effects (both CRS and neurotoxicity) seems to be a challenging obstacle of this approach. Furthermore, a CART-cell graft has to be produced individually for each patient, a complex and technically demanding procedure compared to the standardized application of blinatumomab.
Different study groups aim to incorporate blinatumomab into frontline therapy of ALL (). Three trials (Phases II and III by the NCI and M.D. Anderson Cancer Center) are evaluating first-line induction therapy with and without blinatumomab in adult ALL (NCT02003222, NCT02143414, NCT02877303). As an immunotherapy inducing T-cell response blinatumomab is thought to be more active upfront than in the immunocompromised setting of a heavily pretreated patient with R/R ALL. The combination of blinatumomab with chemotherapy might reduce the risk of CD19 negative outgrowth of leukemic blasts, but clinical data supporting this assumption are pending. The mode of combination, simultaneous application or sequential application still has to be established. Any immunosuppressive chemotherapy counteracts an immunotherapy, yet the combination with targeted therapy and nonmyelosuppressive components such as tyrosine kinase inhibitors or l-asparaginase should be feasible.
Table 2 Clinical trials in ALL that are currently recruiting
Blinatumomab has proven to be a useful tool for bridging ALL high risk patients to HSCT because of its efficacy in R/R ALL and its limited toxicity. The same reasons turn blinatumomab into an attractive option for elderly patients and patients with multiple morbidities.
The application of blinatumomab is actually entering common clinical practice in R/R ALL patients. Even in such a heavily pretreated patient cohort this immunobased approach has proven strong efficacy. It still has to demonstrate its equivalence to other efficient T-cell-based approaches, such as CAR-T-cell therapy. But blinatumomab is paving its way down to the treatment of patient groups with lower risk profiles and into first-line therapy where the competitive pressure of complex CAR-T-cell therapies might be lower.
Disclosure
The authors report no conflicts of interest in this work.
References
- BassanRHoelzerDModern therapy of acute lymphoblastic leukemiaJ Clin Oncol201129553254321220592
- DuXLChenQRecent advancements of bortezomib in acute lymphocytic leukemia treatmentActa Haematol2013129420721423295437
- RobertsKGLiYPayne-TurnerDTargetable kinase-activating lesions in Ph-like acute lymphoblastic leukemiaN Engl J Med2014371111005101525207766
- DeistingWRaumTKuferPBaeuerlePAMunzMImpact of diverse immune evasion mechanisms of cancer cells on T cells engaged by EpCAM/CD3-bispecific antibody construct AMG 110PLoS One20151010e014166926510188
- KlingerMBenjaminJKischelRStienenSZugmaierGHarnessing T cells to fight cancer with BiTE(R) antibody constructs – past developments and future directionsImmunol Rev2016270119320826864113
- SchlegelPLangPZugmaierGPediatric posttransplant relapsed/refractory B-precursor acute lymphoblastic leukemia shows durable remission by therapy with the T-cell engaging bispecific antibody blinatumomabHaematologica20149971212121924727818
- von StackelbergALocatelliFZugmaierGPhase I/Phase II study of blinatumomab in pediatric patients with relapsed/refractory acute lymphoblastic leukemiaJ Clin Oncol201634364381438927998223
- KowolikCMToppMSGonzalezSCD28 costimulation provided through a CD19-specific chimeric antigen receptor enhances in vivo persistence and antitumor efficacy of adoptively transferred T cellsCancer Res20066622109951100417108138
- JensenMCPopplewellLCooperLJAntitransgene rejection responses contribute to attenuated persistence of adoptively transferred CD20/CD19-specific chimeric antigen receptor redirected T cells in humansBiol Blood Marrow Transplant20101691245125620304086
- HowladerNNooneAMKrapchoMSEER Cancer Statistics Review, 1975–2013National Cancer InstituteBethesda, MD Available from: http://seer.cancer.gov/csr/1975_2013/Accessed July 9, 2017
- SanzEMunozAMonserratJOrdering human CD34+CD10−CD19+ pre/pro-B-cell andProc Natl Acad Sci U S A2010107135925593020231472
- van DongenJJOrfaoAEuroFlow Consortium: resetting leukemia and lymphoma immunophenotyping. Basis for companion diagnostics and personalized medicineLeukemia20122691899190722948488
- RickertRCNew insights into pre-BCR and BCR signalling with relevance to B cell malignanciesNat Rev Immunol201313857859123883968
- MullighanCGJehaSPeiDOutcome of children with hypo-diploid ALL treated with risk-directed therapy based on MRD levelsBlood2015126262896289926527677
- MarksDIThe challenges of managing older patients with acute lymphoblastic leukemiaAm Soc Clin Oncol Educ Book2015e343e35125993195
- LukenbillJAdvaniASThe treatment of adolescents and young adults with acute lymphoblastic leukemiaCurr Hematol Malig Rep201382919723559026
- GokbugetNDombretHRiberaJMInternational reference analysis of outcomes in adults with B-precursor Ph-negative relapsed/refractory acute lymphoblastic leukemiaHaematologica2016101121524153327587380
- TallenGRateiRMannGLong-term outcome in children with relapsed acute lymphoblastic leukemia after time-point and site-of-relapse stratification and intensified short-course multidrug chemotherapy: results of trial ALL-REZ BFM 90J Clin Oncol201028142339234720385996
- NagorsenDBargouRRuttingerDKuferPBaeuerlePAZugmaierGImmunotherapy of lymphoma and leukemia with T-cell engaging BiTE antibody blinatumomabLeuk Lymphoma200950688689119455460
- WuJFuJZhangMLiuDAFM13: a first-in-class tetravalent bispecific anti-CD30/CD16A antibody for NK cell-mediated immunotherapyJ Hematol Oncol201589626231785
- FanGWangZHaoMLiJBispecific antibodies and their applicationsJ Hematol Oncol2015813026692321
- BrinkmannUKontermannREThe making of bispecific antibodiesMAbs20179218221228071970
- OffnerSHofmeisterRRomaniukAKuferPBaeuerlePAInduction of regular cytolytic T cell synapses by bispecific single-chain antibody constructs on MHC class I-negative tumor cellsMol Immunol200643676377116360021
- BrischweinKSchlerethBGullerBMT110: a novel bispecific single-chain antibody construct with high efficacy in eradicating established tumorsMol Immunol20064381129114316139892
- HoffmannPHofmeisterRBrischweinKSerial killing of tumor cells by cytotoxic T cells redirected with a CD19−/CD3-bispecific single-chain antibody constructInt J Cancer200511519810415688411
- ToppMSGokbugetNZugmaierGLong-term follow-up of hematologic relapse-free survival in a phase 2 study of blinatumomab in patients with MRD in B-lineage ALLBlood2012120265185518723024237
- ZugmaierGGokbugetNKlingerMLong-term survival and T-cell kinetics in relapsed/refractory ALL patients who achieved MRD response after blinatumomab treatmentBlood2015126242578258426480933
- ToppMSGokbugetNSteinASSafety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: a multicentre, single-arm, phase 2 studyLancet Oncol2015161576625524800
- BarlevALinVWKatzAHuKCongZBarberBEstimating long-term survival of adults with Philadelphia chromosome-negative relapsed/refractory B-precursor acute lymphoblastic leukemia treated with blinatumomab using historical dataAdv Ther201734114815527873237
- KantarjianHSteinAGokbugetNBlinatumomab versus. chemotherapy for advanced acute lymphoblastic leukemiaN Engl J Med2017376983684728249141
- MartinelliGDombretHChevallierPComplete molecular and hematologic response in adult patients with relapsed/refractory (R/R) Philadelphia chromosome-positive B-precursor acute lymphoblastic leukemia (ALL) following treatment with blinatumomab: results from a phase 2 single-arm multicenter study (ALCANTARA). Abstract #679Presented at: The 2015 ASH Annual MeetingDecember 7, 2015Orlando, FL
- ZhuMWuBBrandlCBlinatumomab, a bispecific T-cell engager (BiTE((R))) for CD-19 targeted cancer immunotherapy: clinical pharmacology and its implicationsClin Pharmacokinet201655101271128827209293
- KaplanJBGrischenkoMGilesFJBlinatumomab for the treatment of acute lymphoblastic leukemiaInvest New Drugs20153361271127926383529
- BargouRLeoEZugmaierGTumor regression in cancer patients by very low doses of a T cell-engaging antibodyScience2008321589197497718703743
- KlingerMBrandlCZugmaierGImmunopharmacologic response of patients with B-lineage acute lymphoblastic leukemia to continuous infusion of T cell-engaging CD19/CD3-bispecific BiTE antibody blinatumomabBlood2012119266226623322592608
- WuJFuJZhangMLiuDBlinatumomab: a bispecific T cell engager (BiTE) antibody against CD19/CD3 for refractory acute lymphoid leukemiaJ Hematol Oncol2015810426337639
- ToppMSGokbugetNZugmaierGPhase II trial of the anti-CD19 bispecific T cell-engager blinatumomab shows hematologic and molecular remissions in patients with relapsed or refractory B-precursor acute lymphoblastic leukemiaJ Clin Oncol201432364134414025385737
- TeacheyDTRheingoldSRMaudeSLCytokine release syndrome after blinatumomab treatment related to abnormal macrophage activation and ameliorated with cytokine-directed therapyBlood2013121265154515723678006
- NagorsenDKuferPBaeuerlePABargouRBlinatumomab: a historical perspectivePharmacol Ther2012136333434222940266
- ToppMSGockbugetNSteinASCorrection to lancet oncol 2015; 16: 60, 61. Safety and activity of blinatumomab for adult patients with relapsed or refractory B-precursor acute lymphoblastic leukaemia: a multi-centre, single-arm, phase 2 studyLancet Oncol2015164e158
- DarvishiBFarahmandLJaliliNMajidzadehAKBlinatumomab provoked fatal heart failureInt Immunopharmacol201641424627816725
- ToppMSKuferPGokbugetNTargeted therapy with the T-cell-engaging antibody blinatumomab of chemotherapy-refractory minimal residual disease in B-lineage acute lymphoblastic leukemia patients results in high response rate and prolonged leukemia-free survivalJ Clin Oncol201129182493249821576633
- van ZelmMCReisliIvan derBMAn antibody-deficiency syndrome due to mutations in the CD19 geneN Engl J Med2006354181901191216672701
- RobertsDMJonesRBSmithRMImmunoglobulin G replacement for the treatment of infective complications of rituximab- associated hypogammaglobulinemia in autoimmune disease: a case seriesJ Autoimmun201557242925586449
- HolzelMBovierATutingTPlasticity of tumour and immune cells: a source of heterogeneity and a cause for therapy resistance?Nat Rev Cancer201313536537623535846
- BraigFBrandtAGoebelerMResistance to anti-CD19/CD3 BiTE in acute lymphoblastic leukemia may be mediated by disrupted CD19 membrane traffickingBlood2017129110010427784674
- RayesAMcMastersRLO’BrienMMLineage switch in MLL-rearranged infant leukemia following CD19-directed therapyPediatr Blood Cancer20166361113111526914337
- AldossISongJStillerTCorrelates of resistance and relapse during blinatumomab therapy for relapsed/refractory acute lymphoblastic leukemiaAm J Hematol Epub2017511
- Pongers-WillemseMJVerhagenOJTibbeGJReal-time quantitative PCR for the detection of minimal residual disease in acute lymphoblastic leukemia using junctional region specific TaqMan probesLeukemia19981212200620149844931
- DuellJDittrichMBedkeTFrequency of regulatory T cells determines the outcome of the T-cell-engaging antibody blinatumomab in patients with B-precursor ALLLeukemia Epub2017224
- KohnkeTKrupkaCTischerJKnoselTSubkleweMIncrease of PD-L1 expressing B-precursor ALL cells in a patient resistant to the CD19/CD3-bispecific T cell engager antibody blinatumomabJ Hematol Oncol2015811126449653
- FeuchtJKayserSGorodezkiDT-cell responses against CD19+ pediatric acute lymphoblastic leukemia mediated by bispecific T-cell engager (BiTE) are regulated contrarily by PD-L1 and CD80/CD86 on leukemic blastsOncotarget2016747769027691927708227
- RiberaJMFerrerARiberaJGenescaEProfile of blinatumomab and its potential in the treatment of relapsed/refractory acute lymphoblastic leukemiaOnco Targets Ther201581567157426170691
- GokbugetNZugmaierGKlingerMLong-term relapse-free survival in a phase 2 study of blinatumomab for the treatment of patients with minimal residual disease in B-lineage acute lymphoblastic leukemiaHaematologica20171024e132e13528082340