
Abstract
Evidence of the prognostic role of serine peptidase inhibitor Kazal type 1 (SPINK1) in prostate cancer (PCa) is controversial. The aim of this study was, therefore, to evaluate the association between SPINK1 and clinical outcomes in PCa. Searches were made of PubMed, Medline, Embase, and the China Biology Medicine disc (CBMdisc) up to January 2017. The Newcastle–Ottawa Scale was used to assess the risk of bias of included studies. RevMan software was used to perform meta-analysis, and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) method was employed for assessing the quality of the evidence. Ten studies with 17,161 patients were included in the analysis. Random-effect models were adopted for all outcomes with significant heterogeneities. In patients treated with radical prostatectomy, SPINK1 was associated with biochemical recurrence (BCR) (hazard ratio [HR] =1.41, 95% confidence interval [CI]: 1.01–1.97; P=0.04), but not PCa-specific mortality (HR =0.93, 95% CI: 0.33–2.57; P=0.88), and overall survival (OS) (HR =0.89, 95% CI: 0.58–1.35; P=0.57). In metastatic PCa, SPINK1 was significantly associated with castration-resistant PCa-free survival (HR =3.87, 95% CI: 1.87–8.00; P=0.0003) and OS (HR =2.59, 95% CI: 1.16–5.78; P=0.02). However, the quality of the evidence was very low for all study outcome measures. In conclusion, although SPINK1 was not a predictor of PCa mortality or OS among patients who underwent radical prostatectomy, it may have prognostic value in metastatic PCa.
Introduction
Prostate cancer (PCa) is the most common as well as the third leading cause of cancer-related deaths among men in Western countries.Citation1 In previous decades, signifi-cant breakthroughs have been made in the diagnosis, treatment, and understanding of the genesis of PCa. However, advances in several areas, such as validated biomarkers in facilitating prostate-specific antigen screening, management of metastatic disease, and prognostic biomarkers to assist clinicians in predicting outcomes and decision making, still need to be made.Citation2 So far, numerous biomarkers, including the expression of the E 26 (ETS) family of fusion genes, and serine peptidase inhibitor Kazal type 1 (SPINK1) overexpression, have been discovered in PCa.
In 1983, Huhtala et al first identified SPINK1 in urine samples of patients with gynecological cancers, which suggested that it may have significance as a tumor marker.Citation3 Subsequently, SPINK1 was found to be abnormally expressed in solid tumors, including PCa.Citation4 As a result of this, further studies were devoted to investigating whether this peptide was associated with the prognosis of PCa. Thus, Tomlins et al performed an analysis of molecular subtypes of PCa using SPINK1 and ETS-related gene (ERG) to predict clinical outcomes, and demonstrated the significant prognostic role of SPINK1 in PCa subtypes;Citation5 however, conflicting findings have been reported. Some studies found significant associations between SPINK1 and clinical outcomes while others demonstrated insignificant or even contrary correlations.Citation5–Citation9
Therefore, we have conducted a systematic review and meta-analysis to evaluate the prognostic value of SPINK1 expression in patients with PCa. We have also assessed the current best evidence using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach.
Materials and methods
Two researchers (XMZ and XXY) independently performed the searches, study selection, quality assessment, and data extraction of included studies. Disagreements were resolved by discussion or with the help of a third investigator (HZ).
Eligibility and exclusion criteria for study selection
The eligibility criteria included: 1) patients with pathologically confirmed PCa, 2) cohort or cross-sectional studies investigating the associations between SPINK1 and PCa clinical outcomes, and 3) no language restrictions for published studies. Exclusion criteria included reviews, reports that only focused on laboratory findings of expression profiles of SPINK1 without clinical prognostic outcome measures, and studies with only published abstracts.
Outcome measures included: 1) biochemical recurrence (BCR), 2) PCa-specific mortality (PCSM), 3) overall survival (OS), and 4) castration-resistant PCa (CRPC)-free survival. The definition of CRPC is provided in our previous study.Citation10
Data resources and searches
Searches were made using PubMed (1950-2017.1), Med-line (1966-2017.1), Embase (1947–2017.1), and the China Biology Medicine disc (CBMdisc, 1978–2017.1). The following terms and keywords were used: “trypsin inhibitor, Kazal pancreatic”, “SPINK1”, “pancreatic secretory trypsin inhibitor”, “PSTI”, “tumor-associated trypsin inhibitor”, “TATI”, and “prostate cancer”. References in selected studies were searched for more studies, and experts in the field were consulted.
Study selection and data extraction
Two investigators independently reviewed the titles and abstracts of the search results. The full text versions of studies, which were potentially eligible, were then assessed. Participant characteristics, experimental techniques, outcome measures, results, and other pertinent data of each included study were extracted and recorded on data extraction forms, which were designed according to the guidelines specified in the Cochrane Handbook.Citation11 We contacted authors to seek additional information where data were either not reported or not clear.
Assessment of risk of bias
Two reviewers (XMZ and XXY) independently assessed the risk of bias of included studies using the Newcastle–Ottawa Scale (NOS), which covers three main areas: selection, comparability, and outcome.Citation12 Each study was categorized as low risk of bias (>7 score), moderate risk of bias (5–7 score), or high risk of bias (<5 score).
Data synthesis
RevMan software (version 5.3) was used to perform meta-analysis. Hazard ratios (HRs) and the corresponding 95% confidence intervals (CIs) were synthesized with fixed or random effects models depending on the degree of heterogeneity. A random effect model was used when significant heterogeneity was considered at P<0.10 or I2>50%.
Subgroup analysis was considered for the different groups of patients in the studies. Publication bias was assessed by creating a funnel plot using RevMan software. We applied GRADE approach to assess the quality of evidence recommended by the Cochrane Handbook. This approach specifies four levels of quality, ranging from high to moderate, low, and very low.Citation11
Results
Study characteristics
Three hundred twenty-one studies were identified through electronic searches. One hundred one were excluded after duplicate publications. Full-texts of 38 studies were reviewed, and 13 published articles with 17,161 participants were finally included in the study ().Citation5–Citation8,Citation13–Citation21 Characteristics of the included studies are summarized in . All studies were retrospective cohorts published between 2008 and 2016, of which three were conducted in the USA,Citation5,Citation13,Citation17,Citation21 two in Germany,Citation14,Citation15 two in China,Citation16,Citation18 and one each in France,Citation6 Ireland,Citation7 Finland,Citation8 Korea,Citation19 and Canada.Citation20 Sample sizes ranged from 155 to 8,260. One study included patients with radical prostatectomy (RP) and/or transurethral resection of the prostate,Citation13 and two studies included metastatic PCa (mPCa).Citation8,Citation18 Overall, seven studies with nine cohorts investigated the associations between SPINK1 expression and clinical outcomes in patients with RP.Citation5–Citation7,Citation14–Citation17
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of search results.
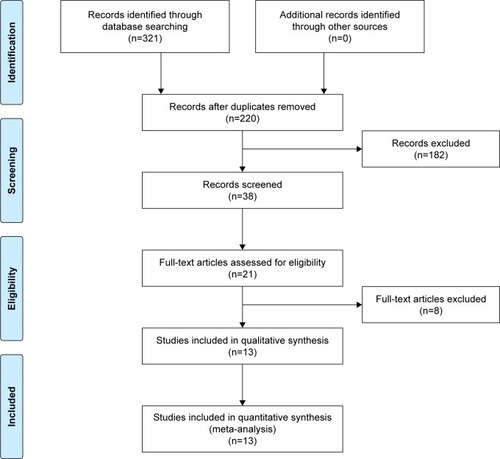
Table 1 Characteristics of included studies
Assessment of risk of bias for included studies
According to the NOS, all included studies were of high quality with scores ranging from 7 to 9 (average 7.9). The most common source of bias was from outcome measures, for which most studies were unclear about the length or adequacy of follow-up ().
Table 2 Risk of bias for included studies
Associations between SPINK1 and clinical outcomes of PCa treated with RP
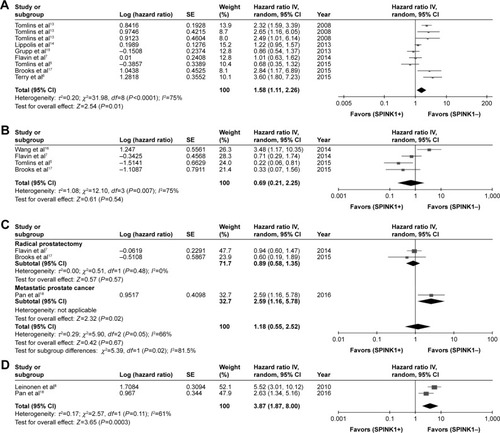
As shown in , a pooled analysis indicated that expression of SPINK1 was associated with poor BCR-free survival in patients with PCa, with a HR of 1.41 (95% CI: 1.01–1.97, P=0.04). No statistically significant associations were observed between SPINK1 expression and PCSM-free survival (HR =0.93, 95% CI: 0.33–2.57, P=0.88; ) and OS (HR =1.18, 95% CI: 0.55–2.52, P=0.67; ).
Figure 2 Forest plots of SPINK1 expression and survival outcomes.
Abbreviations: CI, confidence interval; CRPC, castration-resistant PC, ; df, degrees of freedom; SE, standard error; SPINK1, serine peptidase inhibitor Kazal type 1.
Associations between SPINK1 and clinical outcomes of mPCa
For patients with metastatic disease, SPINK1 expression was significantly associated with CRPC-free survival (HR =3.87, 95% CI: 1.87–8.00, P=0.0003; ), indicating that CRPC-free survival was shorter in patients with SPINK1-positive than SPINK1-negative tumors. Subgroup analysis suggested that SPINK1 expression was associated with shorter PCSM in patients with mPCa (HR =2.6, 95% CI: 1.04–6.5; P=0.04). However, only one study reported this outcome in mPCa patients.Citation21 Because only one study investigated OS among mPCa patients, data synthesis could not be conducted.Citation18 However, this study demonstrated that SPINK1 expression was negatively associated with OS (HR =2.59, 95% CI: 1.16–5.78; P=0.02).
Publication bias
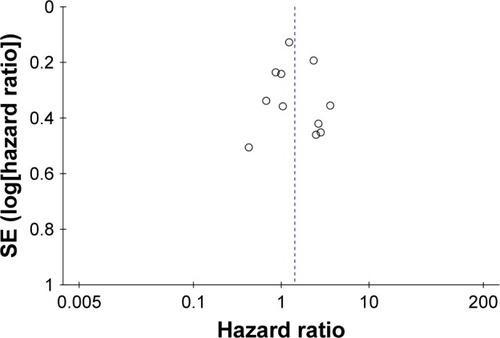
A funnel plot was used to assess the risk of publication bias. As shown in , clear asymmetry was uncovered in the plot, which meant we could not exclude publication bias. Potential reasons for funnel plot asymmetry might be variations in study size and delayed publication, among other factors. However, because of the limited studies included in the analysis, it was difficult to obtain verification for this.
Figure 3 Funnel plot created by outcome of biochemical recurrence-free survival.
Quality of evidence by GRADE approach
As shown in , the quality of the evidence for BCR-free, PCSM-free, CRPC-free, and OS was graded as very low in all instances. Serious inconsistencies were observed for BCR-free survival measures. Serious risk of bias, inconsistency, and imprecision were observed for PCSM- and CRPC-free survival outcomes as well. Finally, for OS, serious imprecision was found in both RP-treated and metastatic patients, and serious risk of bias was found in patients with metastatic disease.
Table 3 Summary of findings of graded quality of evidence for all outcomes
Discussion
This is the first systematic review and meta-analysis to evaluate the association between SPINK1 and prognosis of patients with PCa. In general, we included 13 cohort studies involving 17,161 patients. There were nine studies with 11 cohorts that reported BCR-free survival among men treated with RP. For PCSM-free survival, four studies were included in the final pooled analysis for RP patients and one for mPCa. However, only two studies reported CRPC-free survival and three studies reported OS. Eventually, we found that among patients treated with RP, SPINK1 was associated with BCR-free survival, but not PCSM-free survival or OS. In patients with metastatic disease, the associations were statistically significant between SPINK1- and CRPC-free survival and OS; however, both outcomes only included one study each. Although overall and cancer-specific survival were hard to evaluate, we still found a trend for an unfavorable role of SPINK1 in disease progression.
We noticed that the significant associations between clinical outcomes and SPINK1 expression were more prominent among patients with mPCa. The distinction between metastatic and nonmetastatic disease implied that SPINK1 might have different roles at different stages of PCa progression. In 2015, Huang et al found that SPINK1 was upregulated at primary sites of patients with nodal mPCa.Citation20 Furthermore, knockdown of SPINK1 in vitro could inhibit cell invasion but not proliferation. This finding might explain why SPINK1 was associated with adverse prognosis in aggressive prostate tumors, as opposed to less or no association with clinical outcomes in patients with less aggressive tumors. However, these findings are not conclusive because of the limited number of studies and small sample sizes reported in patients with metastatic disease. Further explorations of SPINK1 in advanced PCa are needed to verify these conclusions.
Although more evident in metastatic diseases, SPINK1 may play a role in patients treated with RP. The insufficient value of SPINK1 as an independent prognostic factor suggests there is an essential need to incorporate it with other biomarkers. In 2015, Tomlins et al combined SPINK1 and ETS gene fusions (most commonly involving ERG) to stratify patients into different molecular subtypes based on risks of clinical outcomes.Citation5 Although the best evidence indicated that ERG alone had no association with BCR- or PCSM-free survival, the combination of ERG and SPINK1 was associated with Gleason scores.Citation22,Citation23
The results of all studies included in this analysis were inconsistent. Therefore this meta-analysis was initiated to systematically assess these studies in the hope of understanding the real evidence for the prognostic role of SPINK1 in PCa. However, the differences among the included studies were too great to be conclusive. It is possible the disparities among these studies were as a result of issues with experimental, clinical, and/or statistical designs. The techniques and conditions for detecting the expression of SPINK1 in each study may also have been different. In addition, ethnicity, regional differences, and baseline characteristics of patients in the included studies might have contributed to the inconsistent results. Meanwhile, there were several limitations in our study. First, in the meta-analyses of all outcomes (BCR-, PCSM-, CRPC-free, and OS), significant heterogeneities were observed (). Heterogeneities could be derived from different sample sizes or follow-up lengths among studies. Next, the quality of the evidence evaluated by the GRADE approach was very low, resulting in conservative recommendations. Moreover, because of the inherent characteristic of the slow progressive nature of most PCa, it is difficult to obtain overall or PCa-specific survival in many studies. The analyses of CRPC-free survival and OS were restricted by the limited number of studies. More studies are needed to further investigate these outcomes. In addition, we were unable to extract eligible data for final analyses even in some studies that reported similar outcomes.
Most of the patients were treated with RP, and only a few had metastatic disease. It has been proven that biomarkers expressed at different disease sites or periods of disease progression might not reflect the current immune-active microenvironment. For instance, programmed death ligand-1 (PD-L1), a novel biomarker in PCa, is discordantly expressed in metastatic sites and primary tumors.Citation24,Citation25 Therefore, we believe it is necessary to further evaluate the association between SPINK1 expression and clinical outcomes in metastatic patients, especially the expression of SPINK1 in the metastatic site or stage.
Conclusion
This is the first systematic review and meta-analysis to evaluate the association between SPINK1 and clinical outcomes among patients with PCa. We found that patients with SPINK1-positive PCa had shorter BCR-free survival (RP group), CRPC-free survival (mPCa), and OS (mPCa) than SPINK1-negative patients. SPINK1 was not a predictor of PCa mortality or OS among patients treated with RP. However, very low quality of evidence assessed by the GRADE approach suggests that high-quality data are necessary to further verify these conclusions.
Author contributions
NC and HZ conceived the study. XMZ and XXY carried out the search process and screened for included studies. XMZ, XXY, GXS, and YJY extracted the data and assessed risk of bias for included studies. XMZ, PFS, and JDL conducted the analysis. XMZ and XXY were involved in writing the paper. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This work was supported by the Natural Science Foundation of China (NSFC 81402110, 81672547, 81272820, and 81172439) and the Science and Technology Support Program of Sichuan Province (2015SZ0230-3).
Disclosure
The authors report no conflicts of interest in this work.
References
- SiegelRLMillerKDJemalACancer statistics, 2016CA Cancer J Clin201666173026742998
- AttardGParkerCEelesRAProstate cancerLancet201638710013708226074382
- HuhtalaMLKahanpääKSeppäläMHalilaHStenmanUHExcretion of a tumor-associated trypsin inhibitor (TATI) in urine of patients with gynecological malignancyInt J Cancer19833167117146190763
- RasanenKItkonenOKoistinenHStenmanUHEmerging roles of SPINK1 in cancerClin Chem201662344945726656134
- TomlinsSAAlshalalfaMDavicioniECharacterization of 1577 primary prostate cancers reveals novel biological and clinicopathologic insights into molecular subtypesEur Urol201568455556725964175
- TerrySNicolaiewNBassetVClinical value of ERG, TFF3, and SPINK1 for molecular subtyping of prostate cancerCancer201512191422143025639219
- FlavinRPetterssonAHendricksonWKSPINK1 protein expression and prostate cancer progressionClin Cancer Res201420184904491124687926
- LeinonenKATolonenTTBrackenHAssociation of SPINK1 expression and TMPRSS2:ERG fusion with prognosis in endocrine-treated prostate cancerClin Cancer Res201016102845285120442300
- SmithSCTomlinsSAProstate cancer SubtyPINg biomarKers and outcome: is clarity emERGing?Clin Cancer Res2016201847334736
- ZhaoTLiaoBYaoJIs there any prognostic impact of intraductal carcinoma of prostate in initial diagnosed aggressively metastatic prostate cancer?Prostate201575322523225307858
- SchünemannHJOxmanADVistGEChapter 12: Interpreting results and drawing conclusionsHigginsJPTGreenSCochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]The Cochrane Collaboration201112.112.20
- WellsGSheaBO’ConnellDThe Newcastle–Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses Available from: www.ohri.ca/programs/clinical_epidemiology/oxford.aspAccessed March 15, 2016
- TomlinsSARhodesDRYuJThe role of SPINK1 in ETS rearrange ment-negative prostate cancersCancer Cell200813651952818538735
- LippolisGEdsjoAStenmanUHBjartellAA high-density tissue microarray from patients with clinically localized prostate cancer reveals ERG and TATI exclusivity in tumor cellsProstate Cancer Prostatic Dis201316214515023459095
- GruppKDiebelFSirmaHSPINK1 expression is tightly linked to 6q15- and 5q21-deleted ERG-fusion negative prostate cancers but unrelated to PSA recurrenceProstate201373151690169823843146
- WangCWangLSuBSerine protease inhibitor Kazal type 1 promotes epithelial-mesenchymal transition through EGFR signaling pathway in prostate cancerProstate201474768970124619958
- BrooksJDWeiWHawleySEvaluation of ERG and SPINK1 by immunohistochemical staining and clinicopathological outcomes in a multi-institutional radical prostatectomy cohort of 1067 patientsPLoS One2015107e013234326172920
- PanXZhangXGongJThe expression profile and prognostic value of SPINK1 in initially diagnosed bone metastatic prostate cancerProstate201676982383327159572
- NohBJSungJYKimYWChangSGParkYKPrognostic value of ERG, PTEN, CRISP3 and SPINK1 in predicting biochemical recurrence in prostate cancerOncol Lett20161163621363027284364
- HuangKCEvansADonnellyBBismarTASPINK1 overexpression in localized prostate cancer: a rare event inversely associated with ERG expression and exclusive of homozygous PTEN deletionPathol Oncol Res Epub20161013
- JohnsonMHRossAEAlshalalfaMSPINK1 defines a molecular subtype of prostate cancer in men with more rapid progression in an at risk, natural history radical prostatectomy cohortJ Urol201619651436144427238617
- PetterssonAGraffREBauerSRThe TMPRSS2:ERG rearrangement, ERG expression, and prostate cancer outcomes: a cohort study and meta-analysisCancer Epidemiol Biomarkers Prev20122191497150922736790
- HuangKCBeginLRPalanisamyNDonnellyBBismarTASPINK1 expression in relation to PTEN and ERG in matched primary and lymph node metastatic prostate cancer: implications for biomarker developmentUrol Oncol2015345235.e1e10
- MukherjiDJabbourMNSaroufimMProgrammed death-ligand 1 expression in muscle-invasive bladder cancer cystectomy specimens and lymph node metastasis: a reliable treatment selection biomarker?Clin Genitourin Cancer201614218318726775720
- GiraldoNABechtEPagèsFOrchestration and prognostic significance of immune checkpoints in the microenvironment of primary and metastatic renal cell cancerClin Cancer Res201521133031304025688160