
Abstract
Objective
The purpose of this study was to evaluate the frequency of RASSF1A hypermethylation in patients with acute myeloid leukemia (AML), in an attempt to modify the current molecular model for disease prognosis.
Materials and methods
Aberrant RASSF1A promoter methylation levels were assessed in 226 newly diagnosed non-M3 AML patients and 30 apparently healthy controls, by quantitative methylation-specific polymerase chain reaction. Meanwhile, RASSF1A mRNA levels were detected by real-time quantitative polymerase chain reaction. Furthermore, hematological characteristics, cytogenetic abnormalities, and genetic aberrations were assessed. Finally, associations of RASSF1A hypermethylation with clinical outcomes were evaluated.
Results
RASSF1A hypermethylation was observed in 23.0% of patients with non-M3 AML (52/226), but not in controls. Meanwhile, hypermethylation of the RASSF1A promoter was significantly associated with ASXL1 mutation. Furthermore, the log-rank test revealed that RASSF1A hypermethylation indicated decreased relapse-free survival (RFS) and overall survival (OS) in patients with non-M3 AML (P=0.012 and P=0.014, respectively). In multivariate analysis, RASSF1A hypermethylation was an independent prognostic factor for RFS (P=0.040), but not for OS (P=0.060).
Conclusion
Hypermethylation of the RASSF1A promoter is associated with ASXL1 mutation in non-M3 AML patients, likely indicating poor outcome. These findings provide a molecular basis for stratified diagnosis and prognostic evaluation.
Introduction
Acute myeloid leukemia (AML), a clonal oncohematological disorder, is characterized by disrupted maturation and programmed cell death (apoptosis), accompanied by uncontrolled proliferation of immature hematopoietic progenitor cells and subsequent suppression of functionally normal hematopoiesis.Citation1,Citation2 Recent advances in genetics have greatly improved our understanding of the molecular mechanisms underlying leukemic transformation.Citation3,Citation4 DNA methylation of CpG islands within gene promoter regions, the most extensively and systematically studied epigenetic mechanism, is crucial for gene regulation during normal hematological cell development.Citation5 Hypermethylation within the promoters of anti-oncogenes appears to be especially common in some or all types of human hematopoietic neoplasms.Citation6–Citation8 To date, many genes have been shown to contribute to leukemogenesis via epigenetic silencing. Our previous reports indicated aberrant hypermethylation of CTNNA1, CHFR1, and miR-193a in several myeloid malignancies.Citation9–Citation11
RASSF1A, considered an important tumor suppressor gene, is located on chromosome 3p21.Citation12 RASSF1A represents potential Ras effectors and plays vital biological roles in cancer progression.Citation13 Several studies have shown that RASSF1A is expressed in normal tissues, including hematopoietic cells; however, its expression is significantly lower in human cancer.Citation14
The current study aimed to assess the methylation levels of the RASSF1A promoter by quantitative methylation-specific polymerase chain reaction (qMS-PCR) in bone marrow (BM) biopsy specimens from non-M3 AML patients. The overarching objective was to identify a subset of patients who might harbor aberrant methylation levels, and in a complementary approach, to comparatively examine the clinical characteristics of these patients. In addition, chromosomal abnormalities and gene mutations known to be associated with AML were assessed for their associations with RASSF1A hypermethylation. Furthermore, to predict the clinical impact of our findings, we evaluated relapse-free survival (RFS) and overall survival (OS) in relation to RASSF1A methylation levels in the study population.
Materials and methods
Patients
This study included 226 newly diagnosed patients with non-M3 AML visiting the Chinese PLA General Hospital and China-Japan Friendship Hospital, from July 2006 to March 2015, and 30 healthy controls. Written informed consent was obtained from each subject for sample preservation and genetic assays. The study was approved by the ethics committees of the Chinese PLA General Hospital and China-Japan Friendship Hospital. BM samples were collected during routine clinical examination, and those with more than 50% blastocysts, identified by morphologic assessment, were selected. The clinical characteristics of patients are described in . All patients with non-M3 AML received intensive induction therapy with high-dose cytarabine-based regimens or monotherapy with decitabine (demethylating treatment) followed by consolidation therapy. Twenty-nine patients underwent allogeneic hematopoietic stem cell transplantation, and 26 received autologous hematopoietic stem cell transplantation.
Table 1 Analysis of clinical characteristics and outcome in two groups
Clinical end points
Complete remission (CR) was defined as no anemia, bleeding, infection, leukemic cell infiltration, circulating leukemic blastocysts, or evidence of extramedullary leukemia, with a recovery of morphologically normal BM and blood cell amounts. In addition, BM cells and primitive promyelocytic-stage cells (or immature cells) were <5%, with normal erythroid–megakaryocyte system. Relapse was defined as ≥5% BM blastocysts, circulating leukemic blastocysts, or the emergence of extramedullary leukemic cells. OS was determined from leukemia diagnosis to death, censoring patients alive at the last follow-up. RFS was determined from the date of CR to relapse or death from any cause, censoring patients alive at the last follow-up.
DNA isolation, bisulfite modification, and qMS-PCR
Genomic DNA was extracted and purified from BM specimens with Genomic DNA Purification Kit (Promega, Madison, WI, USA). Then, 1 μg of genomic DNA was treated with sodium bisulfate using EpiTect Kit (Qiagen, Hilden, Germany). Bisulfite-treated DNA was amplified by qMS-PCR using primers and probes specific for RASSF1A and MYOD1 (reference gene) (shown in ). Polymerase chain reaction (PCR) was carried out in a 40 μL volume with 20 μL MethyLight Master Mix (Qiagen), 0.25 μM of each primer, RASSF1A or MYOD1 gene probes, and 20 ng bisulfite-treated DNA. PCR conditions consisted of an initial denaturation step of 95°C for 5 minutes, followed by 40 cycles of denaturation for 15 seconds at 95°C and annealing for 60 seconds at 61°C. Standard curves were established for RASSF1A and MYOD1 using 10-fold serial dilutions of five different plasmid concentrations. Relative methylation levels of RASSF1A were calculated by the ratio of RASSF1A copies to that of MYOD1.
Karyotype analysis and fluorescence in situ hybridization (FISH)
A total of 226 patients were submitted to cytogenetic analysis of BM samples at diagnosis by the direct method or 24-hour culture. The cytogenetic assays were performed independently by at least two cytogenetic technicians or pathologists. Metaphase chromosomes were assessed by G-banding, with chromosomal abnormalities presented according to the International System for Human Cytogenetic Nomenclature.Citation15 Simultaneous presentation of at least three unrelated cytogenetic abnormalities in one clone was defined as complex cytogenetic abnormalities. Cytogenetic abnormalities were divided into favorable, intermediate, and unfavorable karyotype groups, based on published criteria accepted by the Southwest Oncology Group (SWOG).Citation16 Besides, −5/5q-, −7/7q-, inv(16)/t(16;16), and 11q23 rearrangement abnormalities were confirmed by FISH.
Real-time quantitative polymerase chain reaction (RT-qPCR)
Total RNA was isolated from BM samples from patients with non-M3 AML at diagnosis, with the Qiazol isolation reagent (Qiagen). Then, cDNA was obtained using a reverse transcription kit (Promega). Quantification of RASSF1A and ABL1 transcripts was performed by RT-qPCR with specific primers and probes (). The PCR volume was 40 μL, including 20 μL TaqMan Universal Master Mix (Life Technologies), 0.25 μM of each primer, RASSF1A and ABL1 gene probes, and 20 ng cDNA. The PCR program comprised 40 cycles of denaturation for 15 seconds at 95°C and annealing for 60 seconds at 60°C. Standard curves were generated for the RASSF1A and ABL1 genes by 10-fold serial dilutions of five different plasmid concentrations. Relative expression of RASSF1A was determined as the ratio of RASSF1A copies to that of ABL1.
Detection of gene mutations
To assess the associations of gene mutations occurring in AML patients with the methylation status of the RASSF1A promoter region, DNA sequencing was conducted to detect NPM1, FLT3-ITD, ASXL1, IDH1, DNMT3A, RUNX1, U2AF1, TET2, SRSF2, NRAS, CEBPA, KIT, and SF3B1 with hyperfrequency-mutation sequences, as previously reported.Citation9,Citation10,Citation17–Citation22 The primers used for sequencing are shown in .
Statistical analysis
All statistical analyses were performed with the SPSS 18.0 software (SPSS, Chicago, IL, USA). Data were presented as median and range. Pearson chi-square and Fisher’s exact tests were adopted to compare the patient groups. The associations of the methylation status of the RASSF1A promoter with clinical parameters were assessed by Pearson’s and Spearman’s rank correlations. Patients were followed up for a median time of 36 months (range, 5–100 months). The Kaplan–Meier method was used to estimate survival, and differences between groups were analyzed by log-rank test. To adjust for clinical and molecular prognostic variables, a multivariate Cox model was utilized to assess the associations of survival with age, chromosomal abnormalities, RASSF1A methylation level, and mutation status. For all analyses, P<0.05 was considered statistically significant.
Results
DNA methylation status and RASSF1A gene expression in AML patients
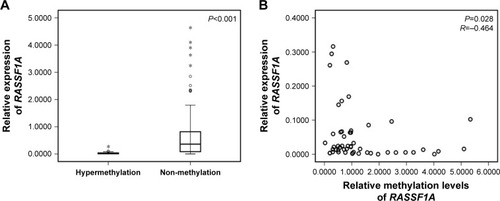
RASSF1A gene promoter methylation levels were assessed in BM samples from 226 AML patients and 30 healthy donors. RASSF1A hypermethylation was found in 23% (52/226) of AML patients, but not in healthy donors. Among the 52 patients, median RASSF1A hypermethylation level was 1.0279, ranging from 0.1967 to 5.336. Gene expression analysis showed significantly decreased RASSF1A levels in patients with RASSF1A hypermethylation compared with the non-methylation group (, P<0.001). Moreover, there was a significant negative association of RASSF1A mRNA levels with hypermethylation in both patient groups (, P=0.028, R=−0.364).
Figure 1 (A) Relative expression of the RASSF1A gene was detected in the patients with RASSF1A hypermethylation and the cases with non-methylation, and significant difference was found between the two groups. *Singular value. (B) There was a negative correlation between RASSF1A methylation levels and RASSF1A transcript levels (R=−0.464, P=0.028).
RASSF1A hypermethylation is associated with chromosomal abnormalities
To further assess the cytogenetic abnormalities in both patient groups (with or without RASSF1A gene hypermethylation), various karyotypes were compared between the two groups. As shown in , RASSF1A hypermethylation was highly associated with unfavorable chromosomal abnormalities (P=0.049) and complex karyotype (P=0.016). There were no significant differences in other karyotypes between the RASSF1A hypermethylation and non-methylation groups.
Table 2 Comparison of genetic alterations between patients with acute myeloid leukemia with or without hypermethylation of the RASSF1A promoter
Patients with aberrant RASSF1A methylation show higher ASXL1 mutation frequencies
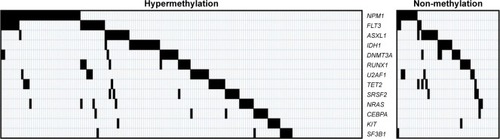
In the present study, ASXL1, CEBPA, DNMT3A, FLT3, IDH1, KIT, NPM1, NRAS, RUNX1, SF3B1, SRSF2, U2AF1, and TET2 mutations were assessed in all 226 patients with non-M3 AML. The mutation spectra in both hypermethylation and non-methylation patient groups are shown in . As shown in , cases with aberrant RASSF1A methylation levels displayed a higher probability of ASXL1 mutation (P=0.036). In the present work, a total of 22 patients showed ASXL1 mutations, including 9 and 13 in the hypermethylation and non-hypermethylation groups, respectively.
Figure 2 Spectrum of gene mutations in 226 non-M3 AML patients with hypermethylation and non-methylation of the RASSF1A gene.
Patients displaying aberrant RASSF1A methylation levels have adverse outcome
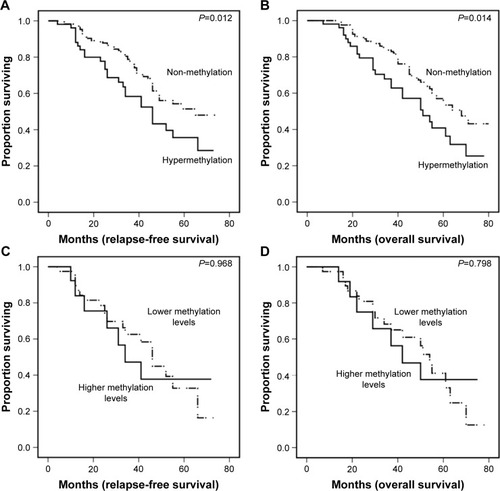
In the present study, we evaluated RFS and OS in both patient groups (with or without RASSF1A hypermethylation) (). All 226 patients with AML were enrolled, with a median follow-up of 41 months (mean, 5–80 months). Interestingly, non-M3 AML patients with RASSF1A hyper-methylation exhibited reduced RFS (P=0.012) and OS (P=0.014) compared with the non-hypermethylation group. To further assess the prognostic value of RASSF1A methylation levels, the patients were divided into two groups according to the 75th percentile of the initial transcript levels (). Consequently, 13 patients were assigned to the high methylation group, and the remaining to the low methylation group. Interestingly, patients with high RASSF1A methylation levels exhibited similar RFS (P=0.968) and OS (P=0.798) compared to the low methylation group.
Figure 3 (A and B) Among non-M3 AML patients, those with RASSF1A hypermethylation (n=52) had inferior relapse-free survival and overall survival compared to those with no hypermethylation (n=174) (P=0.012 and P=0.014, respectively). (C and D) Patients with higher RASSF1A methylation levels (n=13) did not show different relapse-free survival and overall survival compared to individuals with lower methylation levels (n=39) (P=0.968 and P=0.798, respectively).
Hypermethylation of the RASSF1A gene was entered into a multivariate model with variables significantly associated with prognosis in univariate analysis in the present cohort. Interestingly, RASSF1A hypermethylation and U2AF1 mutation were independent prognostic factors for RFS, but not for OS (). Meanwhile, age ≥60 years, unfavorable karyotype, RUNX1 mutation, FLT3-ITD, and DNMT3A mutation showed reduced RFS and OS.
Table 3 Univariate and multivariate analysis of clinical and molecular variables for RFS and OS in non-M3 AML patients
Discussion
Recent studies have revealed that leukemic cells exhibit various genetic and epigenetic abnormalities that contribute not only to cell transformation but also to disease progression. These novel insights not only provide clues for diagnostic stratification and prognostic evaluation but also play a key role in the appropriate selection of individuals for suitable targeted therapy.Citation23–Citation25 DNA hypermethylation, which causes transcriptional repression, has recently emerged as one of the most frequent changes occurring in cancers, including hematopoietic tumors, and is associated with malignant transformation, making it an intriguing novel target for therapeutic targeting of leukemia.Citation26 The use of irreversible DNA methyltransferase inhibitors, including 5-azacytidine (5-aza) and decitabine, appears to be a promising option for treating myeloid malignancies, including AML.Citation27–Citation29 RASSF1A is considered a candidate leukemia-suppressor gene;Citation12,Citation13 however, determining its exact effects on clinical outcome using BM samples from patients has been challenging. In addition, aberrant methylation levels of RASSF1A in a subpopulation of myeloid malignant patients were recently reported, but with no associations with gene mutations often detected in myeloid malignancies.Citation30 Hence, in the present study, the associations of RASSF1A methylation with hematological findings, cytogenetic and genetic aberrations, and clinical outcomes in AML patients were assessed.
As shown above, DNA hypermethylation of the RASSF1A promoter was a frequent genetic event in patients with non-M3 AML. Johan et al demonstrated that RASSF1A promoter methylation is found in AML and myelodys-plastic syndromes, by methylation-specific PCR.Citation31 Meanwhile, Avramouli et al found that RASSF1AA methylation does not frequently occur in chronic myeloid leukemia.Citation32 However, whether RASSF1A methylation is associated with other genetic aberrations of myeloid malignancies remains unclear. In this study, the qMS-PCR approach was employed to detect RASSF1A gene methylation levels. To the best of our knowledge, this is the first report assessing RASSF1A gene methylation levels.
Besides, RASSF1A methylation was evaluated in all French–American–British subtypes included in the current study, with no specific phenotype found to be highly associated. In addition, patients with aberrant methylation levels showed no decreased CR rate or one-year OS (data not shown).
In the present study, cytogenetic aberrations and gene mutations associated with hematopoietic malignancies were assessed in the RASSF1A hypermethylation and non-hypermethylation groups. Close associations were found of RASSF1A hypermethylation with unfavorable chromosomal abnormalities and complex karyotype, which are considered poor cytogenetic markers in AML.Citation16 These findings suggested that RASSF1A hypermethylation could be considered a novel prognostic marker for AML. However, the molecular mechanism underlying the association of ASXL1 mutation with RASSF1A hypermethylation remains unknown and requires deeper fundamental research. It is worth noting that ASXL1 gene mutations are more frequent in patients with RASSF1A hypermethylation. Recent studies demonstrated that ASXL1 mutation is a reliable marker of poor outcome in AML.Citation33–Citation35 However, such a finding was not obtained in this study, likely because only the high-frequency target sequence of ASXL1 was detected.
We also evaluated patient survival curves in association with RASSF1A hypermethylation. Interestingly, patients with RASSF1A hypermethylation had reduced RFS compared with the non-methylation group, providing a theoretical basis for specific molecularly targeted therapy using demethylating agents.
In recent years, great progress has been made in understanding epigenetic changes in leukemia, providing a solid theoretical basis for molecular detection and diagnostic stratification, and shedding light on the development of hematologic disorders.Citation36–Citation38 RASSF1A was shown to act as a leukemia-associated gene, probably playing a vital role in the occurrence of AML and other hematopoietic malignancies.
Conclusion
In the current study, our analysis of RASSF1A promoter methylation status and its potential association with cytogenetic and molecular characteristics and clinical outcomes revealed vital points into the involvement of the RASSF1A gene in the pathogenesis of leukemia.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (Grant No 81300425 and 81300450) and the Key Program of Capital Development Foundation (No 2007-2040).
Supplementary materials
Table S1 Primers and probes for detection of MYOD1 and RASSF1A methylation levels
Table S2 Primers and probes for detection of ABL1 and RASSF1A mRNA levels
Table S3 Primers of gene mutations for sequencing
Disclosure
The authors report no conflicts of interest in this work.
References
- FerraraFSchifferCAAcute myeloid leukaemia in adultsLancet2013381986548449523399072
- LevineRLMolecular pathogenesis of AML: translating insights to the clinicBest Pract Res Clin Haematol201326324524824309525
- KhaledSAl MalkiMMarcucciGAcute myeloid leukemia: biologic, prognostic and therapeutic insightsOncology (Williston Park)201630431832927085330
- JabbourECortesJRavandiFO’BrienSKantarjianHTargeted therapies in hematology and their impact on patient care: chronic and acute myeloid leukemiaSemin Hematol201350427128324246694
- PastoreFLevineRLEpigenetic regulators and their impact on therapy in acute myeloid leukemiaHaematologica2016101326927826928248
- Conway O’BrienEPrideauxSChevassutTThe epigenetic landscape of acute myeloid leukemiaAdv Hematol2014201410317524778653
- HennessyBTGarcia-ManeroGKantarjianHMGilesFJDNA methylation in haematological malignancies: the role of decitabineExpert Opin Investig Drugs2003121219851993
- SchoofsTMüller-TidowCDNA methylation as a pathogenic event and as a therapeutic target in AMLCancer Treat Rev201137Suppl 1S13S1821612874
- LiMGaoLLiZCTNNA1 hypermethylation, a frequent event in acute myeloid leukemia, is independently associated with an adverse outcomeOncotarget2016721314543146527129146
- GaoLLiuFZhangHSunJMaYCHFR hypermethylation, a frequent event in acute myeloid leukemia, is independently associated with an adverse outcomeGenes Chromosomes Cancer201655215816826542416
- LiYGaoLLuoXEpigenetic silencing of microRNA-193a contributes to leukemogenesis in t(8;21) acute myeloid leukemia by activating the PTEN/PI3K signal pathwayBlood2013121349950923223432
- van der WeydenLAdamsDJThe Ras-association domain family (RASSF) members and their role in human tumourigenesisBiochim Biophys Acta200717761588517692468
- DonningerHVosMDClarkGJThe RASSF1A tumor suppressorJ Cell Sci2007120Pt 183163317217878233
- HessonLBCooperWNLatifFThe role of RASSF1A methylation in cancerDis Markers2007231–2738717325427
- SimonsAShafferLGHastingsRJCytogenetic nomenclature: changes in the ISCN 2013 compared to the 2009 editionCytogenet Genome Res201314111623817294
- SlovakMLKopeckyKJCassilethPAKaryotypic analysis predicts outcome of preremission and postremission therapy in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group StudyBlood200096134075408311110676
- LiuFGaoLJingYDetection and clinical significance of gene rearrangements in Chinese patients with adult acute lymphoblastic leukemiaLeuk Lymphoma20135471521152623210573
- ShenYZhuYMFanXGene mutation patterns and their prognostic impact in a cohort of 1185 patients with acute myeloid leukemiaBlood2011118205593560321881046
- GuanLGaoLWangLThe frequency and clinical significance of IDH1 mutations in Chinese acute myeloid leukemia patientsPLoS One2013812e8333424376688
- ChenTCHouHAChouWCDynamics of ASXL1 mutation and other associated genetic alterations during disease progression in patients with primary myelodysplastic syndromeBlood Cancer J201441e17724442206
- HaferlachTNagataYGrossmannVLandscape of genetic lesions in 944 patients with myelodysplastic syndromesLeukemia201428224124724220272
- ItzyksonRKosmiderORennevilleAPrognostic score including gene mutations in chronic myelomonocytic leukemiaJ Clin Oncol201331192428243623690417
- YangJSchifferCAGenetic biomarkers in acute myeloid leukemia: will the promise of improving treatment outcomes be realized?Expert Rev Hematol20125439540722992234
- MuratiABrecquevilleMDevillierRMozziconacciMJGelsi-BoyerVBirnbaumDMyeloid malignancies: mutations, models and managementBMC Cancer20121230422823977
- ShihAHAbdel-WahabOPatelJPLevineRLThe role of mutations in epigenetic regulators in myeloid malignanciesNat Rev Cancer201212959961222898539
- JasielecJSalouraVGodleyLAThe mechanistic role of DNA methylation in myeloid leukemogenesisLeukemia20142891765177324913729
- SmithBDBeachCLMahmoudDWeberLHenkHJSurvival and hospitalization among patients with acute myeloid leukemia treated with azacitidine or decitabine in a large managed care population: a real-world, retrospective, claims-based, comparative analysisExp Hematol Oncol2014311024666795
- YunSVinceletteNDAbrahamIRobertsonKDFernandez-ZapicoMEPatnaikMMTargeting epigenetic pathways in acute myeloid leukemia and myelodysplastic syndrome: a systematic review of hypomethylating agents trialsClin Epigenetics201686827307795
- DingKFuRLiuHNachnaniDAShaoZHEffects of decitabine on megakaryocyte maturation in patients with myelodysplastic syndromesOncol Lett20161142347235227073478
- GriffithsEAGoreSDHookerCAcute myeloid leukemia is characterized by Wnt pathway inhibitor promoter hypermethylationLeuk Lymphoma20105191711171920795789
- JohanMFBowenDTFrewMEGoodeveACReillyJTAberrant methylation of the negative regulators RASSFIA, SHP-1 and SOCS-1 in myelodysplastic syndromes and acute myeloid leukaemiaBr J Haematol20051291606515801956
- AvramouliATsochasSMandalaEMethylation status of RASSF1A in patients with chronic myeloid leukemiaLeuk Res20093381130113219193434
- PaschkaPSchlenkRFGaidzikVIASXL1 mutations in younger adult patients with acute myeloid leukemia: a study by the German-Austrian Acute Myeloid Leukemia Study GroupHaematologica2015100332433025596267
- ShivarovVGueorguievaRIvanovaMTiuRVASXL1 mutations define a subgroup of patients with acute myeloid leukemia with distinct gene expression profile and poor prognosis: a meta-analysis of 3311 adult patients with acute myeloid leukemiaLeuk Lymphoma20155661881188325308295
- SchnittgerSEderCJerominSASXL1 exon 12 mutations are frequent in AML with intermediate risk karyotype and are independently associated with an adverse outcomeLeukemia2013271829123018865
- OdenikeOThirmanMJArtzASGodleyLALarsonRAStockWGene mutations, epigenetic dysregulation, and personalized therapy in myeloid neoplasia: are we there yet?Semin Oncol201138219621421421110
- TakahashiSCurrent findings for recurring mutations in acute myeloid leukemiaJ Hematol Oncol201143621917154
- GillHLeungAYKwongYLMolecular targeted therapy in acute myeloid leukemiaFuture Oncol201612682783826828965