
Abstract
Background
Phosphodiesterase type 5 inhibitor (PE5i) administration may stimulate the proliferation and survival of melanocytes. However, discrepancies remain regarding the association between PDE5i use and melanoma risk in observational studies in humans.
Aim
To evaluate the association between PDE5i use and melanoma in a meta-analysis.
Materials and methods
Studies were identified by searching the PubMed and Embase databases. A random-effects model was applied to synthesize the data. A stratified study was performed to evaluate the influence of study characteristics on outcomes.
Results
Four prospective cohort studies and three case–control studies with 1,534,615 male participants and 16,053 melanoma cases were incorporated. Patients who received a PDE5i had a significantly increased risk for melanoma (adjusted risk ratio [RR] =1.12, 95% CI =1.03–1.33, P=0.008) with moderate heterogeneity (I2=54%). Cohort studies (adjusted RR =1.22, 95% CI =1.02–1.46, P=0.03) largely contributed to this result rather than case–control studies. Subsequent stratified analyses revealed that sildenafil was associated with an increased risk of melanoma (adjusted RR =1.26, 95% CI =1.07–1.50, P=0.007), but tadalafil and vardenafil were not. Also, PDE5i use was associated with a significantly increased risk of in situ melanoma (adjusted RR =1.31, 95% CI =1.01–1.69, P=0.04), but not of localized or nonlocalized melanoma.
Conclusion
PDE5i use may be associated with a significantly increased risk for melanoma in men. However, further research is needed to determine whether the association is causative.
Introduction
Melanoma is a malignant tumor that has been correlated with endogenous factors such as skin–eye–hair color, family history, and the presence of common or atypical nevi, as well as exogenous factors such as excessive sun exposure.Citation1 Biologically, many dysfunctions of molecular pathways have been demonstrated to be involved in the pathogenesis of melanoma, and the activation of the RAS/RAF/mitogen-activated protein kinase and extracellular signal-regulated kinase (ERK) kinase (MEK)/ERK signaling pathway is one of the main key signals that determine the pathogenesis and progression of melanoma.Citation1–Citation3 Moreover, activation of the RAS/RAF/ERK/MEK pathway has been recognized to be a result of BRAF somatic mutation (OMIM*164757), which causes the downregulation of cyclic guanosine monophosphate (cGMP)–specific phosphodiesterase (PDE) 5A and lowers cGMP degradation, leading to an increase in intracellular Ca2+.Citation4–Citation6 These mechanisms have been considered to be important for the invasion and metastasis of melanocytes, and treatments targeting these signaling pathways have shown promising therapeutic efficacy in patients with melanoma.Citation7,Citation8
Phosphodiesterase type 5 inhibitors (PDE5is), including sildenafil, tadalafil, and vardenafil, are a category of medications approved for the treatment of erectile dysfunction.Citation9–Citation11 These medications function as inhibitors of cGMP-specific PDE5A, which mimic the effects of the RAS/RAF/ERK/MEK pathway and may thereby contribute to the development and progression of melanoma. Indeed, some experimental studies in cell lines in vitro have indicated that the administration of a PDE5i was associated with enhanced proliferation and survival of melanocytes.Citation12–Citation14 However, the results of subsequent observational studies regarding the relationship between PDE5i use and melanoma risk were not always consistent.Citation15–Citation20 The discrepancies of these results may be due to the differences in the included participants, regimens of PDE5i administration, and limited sample sizes of some related studies, which may be underpowered to detect a significant result.Citation21 Therefore, in this study, we performed a meta-analysis of observational studies to elucidate the association between PDE5i use and risk of melanoma. Moreover, we also aimed to evaluate whether the relationship between PDE5i use and risk of melanoma was significantly affected by the individual application of PDE5i.
Materials and methods
The Meta-analysis of Observational Studies in EpidemiologyCitation22 and Cochrane’s Handbook guidelinesCitation23 were followed during the performance of this meta-analysis.
Database searching
The PubMed and Embase databases were systematically searched for potential relevant records using the following searching terms: “phosphodiesterase type 5 inhibitors”, “PDE5 inhibitors”, “PDE5i”, “avanafil”, “lodenafil”, “mirodenafil”, “sildenafil”, “tadalafil”, “udenafil”, or “vardenafil”, combined with “melanoma”. This search was limited to human studies and English language publications. The references of the original and review articles were also manually analyzed. The final literature search was performed on April 14, 2017.
Inclusion and exclusion criteria
Articles were included in this meta-analysis if the following criteria were met: 1) published as full-length articles or abstracts of scientific sessions in English; 2) reported as cohort studies or case–control studies; 3) included an adult population of ≥18 years of age; 4) identified use of PDE5i as exposure of interest; 5) included those not treated with a PDE5i as controls; 6) compared the risk of melanoma between participants who used a PDE5i vs those who did not; 7) reported the adjusted hazards ratio, relative risk (RR), or odds ratio and their corresponding 95% CIs for melanoma risk between the PDE5i users and controls. For studies that included overlapping participants, those with a larger sample size were included in the meta-analysis. Irrelevant studies, editorials, review articles, and experimental studies in cell lines or animals were excluded.
Data extraction and quality evaluation
Two authors independently performed the literature search, data extraction, and quality assessment according to the predefined inclusion criteria. Discrepancies were resolved by consensus. The extracted data included the following: 1) name of the first author, year of publication, and country where the study was conducted; 2) the general characteristics and source of the study participants; 3) the range of the study years; 4) the total number of participants, PDE5i users, and melanoma cases; 5) the follow-up durations for the included cohort studies; 6) the strategies used to confirm a diagnosis for melanoma; and 7) the adjusted variables for reporting the association between PDE5i use and melanoma risk. The quality of each study was evaluated using the Newcastle–Ottawa Scale,Citation24 which ranged from 1 to 9 stars, and each study was evaluated based on three aspects: the selection of the study groups, the comparability of these groups, and the ascertainment of the outcome of interest.
Statistical analyses
RR was used as the general measure for the association between the use of PDE5i and risk of melanoma across studies, and the most adequately adjusted data were extracted for subsequent meta-analyses. The data of RRs and their corresponding standard errors were calculated from 95% CIs or P-values, and were logarithmically transformed to stabilize variance and normalize the distribution.Citation23 Cochrane’s Q-test and I2-test were applied to evaluate the heterogeneity among the included studies.Citation25 Significant heterogeneity was confirmed if I2 was >50%. A random-effects model was used to synthesize the RR data, because this model is expected to retrieve a more generalized result via the incorporation of potential heterogeneity.Citation23 Sensitivity analyses were performed by removing one study at a time to test the robustness of the results.Citation26 Stratified analyses were performed to evaluate whether the associations between PDE5i use and melanoma risk were different according to different study characteristics such as the study design (cohort studies or case–control studies), the timing of PDE5i administration (recent use or early use), the number of prescriptions (the lowest or highest prescription categories), the individual PDE5i used (sildenafil, tadalafil, or vardenafil), and the stages of melanoma evaluated (in situ, localized, or nonlocalized). Since the definitions of the recent use of PDE5i were not consistent among the included studies, the definitions included from the original articles were used. In addition, since the cut-offs for the categorization of the PDE5i prescriptions were also not consistent among these included studies, the definitions from the original articles were used, and the associations between PDE5i use and melanoma risk were summarized in the lowest and highest prescription categories, respectively. Potential publication bias was assessed by funnel plots using Egger regression asymmetry test.Citation27 RevMan (Version 5.1; Cochrane Collaboration, Oxford, UK) and STATA software (Version 12.0; Stata Corporation, College Station, TX, USA) were used for the meta-analysis and statistical analysis.
Results
Literature search
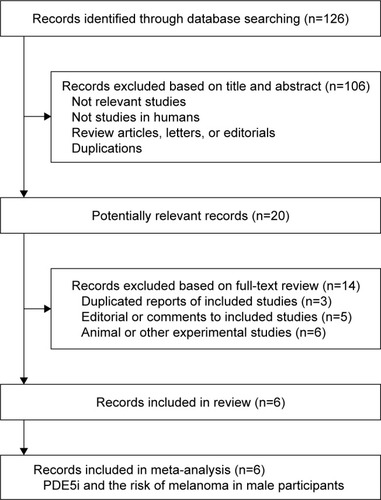
The literature search process is presented in . Briefly, 726 articles were identified via the initial literature search in the PubMed and Embase databases, and 706 articles were excluded after the screening of titles and abstracts, mainly due to the irrelevance of these articles to the purpose of this study. Subsequently, 20 potential relevant articles underwent full-text review. Among these, 14 articles were further excluded. Among these excluded articles, three articles were duplicate reports, five articles were editorial or comments, and six articles were experimental studies. Finally, six articlesCitation15–Citation20 were included in the meta-analysis.
Figure 1 Flowchart of study selection.
Characteristics and quality of the included studies
Since one of the included articlesCitation20 reported the data of two case–control studies (the Danish Nationwide Health Registries and the Kaiser Permanente Northern California), a total of seven studies with 1,534,615 participants and 16,053 melanoma cases were incorporated into our meta-analysis.Citation15–Citation20 The characteristics and quality scores of these included studies are summarized in . All of these studies were published after 2014. Among these, four studies were designed as cohort studies,Citation15,Citation17–Citation19 one study was a nested case–control study,Citation16 and two studies were case–control studies.Citation17 Furthermore, among these included studies, three studies were conducted in the USA,Citation15,Citation17,Citation20 two studies in the UK,Citation18,Citation19 and two studies in Northern Europe.Citation16,Citation20 As for the general characteristics of the included participants, six studies included males from the general populationCitation15–Citation17,Citation19,Citation20 and one study included males with erectile dysfunction.Citation18 The mean age of the included participants ranged from 57.0 to 74.5 years, and the indexed study year ranged from 1998 to 2015. Regarding the investigation of individual PDE5i, sildenafil users were analyzed in all of the included studies, while tadalafil and vardenafil users were evaluated in five studies. Melanoma diagnosis was confirmed according to the International Classification of Diseases version 9 or 10, or with the information of national cancer registries. All studies were adjusted for multiple variables (at least for age and race) in reporting the association between the use of PDE5i and melanoma risk. The Newcastle–Ottawa scale scores ranged from 6 to 9 in the included cohort studies.
Table 1 Characteristics of the included studies
Overall results for the association between PDE5i use and melanoma risk
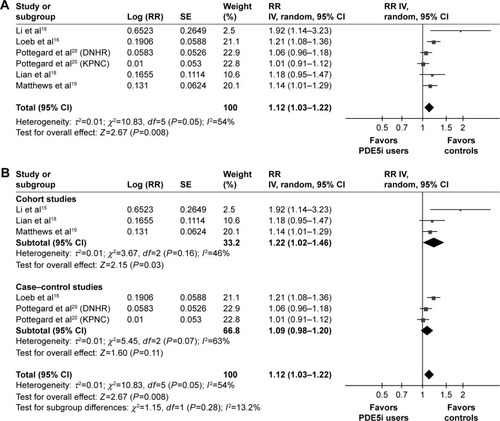
The pooled results of the six studies were analyzed with the random-effects model to evaluate the overall association between PDE5i use and risk of melanoma. The results revealed that PDE5i treatment was associated with a significantly increased risk for melanoma (adjusted RR =1.12, 95% CI =1.03–1.33, P=0.008; ). Furthermore, considerable heterogeneity was detected among the included studies (P for Cochrane’s Q-test =0.05, I2=54%). Sensitivity analyses conducted by omitting one study at a time did not significantly change these results, suggesting the robustness of the results. Subsequent subgroup analyses by study design revealed that PDE5i use was associated with a significantly increased risk for melanoma in these cohort studies (three studies,Citation15,Citation18,Citation19 adjusted RR =1.22, 95% CI =1.02–1.46, P=0.03, I2=46%; ), but the association was not significant in the pooled results for three case–control studiesCitation16,Citation20 (adjusted RR =1.12, 95% CI =1.03–1.22, P=0.11, I2=63%; ).
Figure 2 Forest plots for the meta-analysis of the association between PDE5i use and risk of melanoma presented as adjusted RR.
Abbreviations: df, degrees of freedom; DNHR, Danish Nationwide Health Registries; IV, inverse variance; KPNC, Kaiser Permanente Northern California; PDE5i, phosphodiesterase type 5 inhibitor; RR, risk ratio; SE, standard error.
Stratified analysis of the association between PDE5i use and risk of melanoma
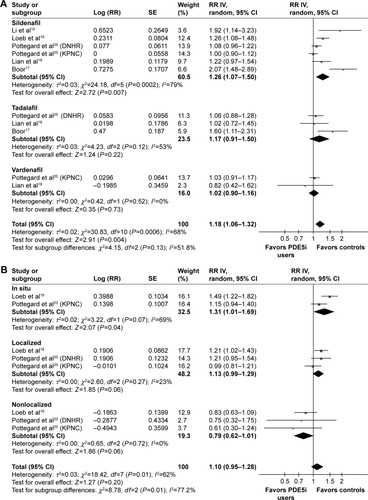
A stratified analysis was performed according to the timing of PDE5i use, the number of prescriptions, the individual PDE5I used, and the stage of melanoma. Two studiesCitation15,Citation16 provided stratified data according to the timing of PDE5i use, and these pooled results revealed that recent use of PDE5i was associated with a significantly increased risk for melanoma (adjusted RR =1.38, 95% CI =1.02–1.86, P=0.04, I2=35%; ), whereas early use of these medications was not (adjusted RR =1.46, 95% CI =0.76–2.80, P=0.26, I2=77%; ). Moreover, the stratified analysis of five studiesCitation16,Citation18–Citation20 indicated that PDE5i use was associated with an increased risk of melanoma in both the lowest (adjusted RR =1.10, 95% CI =1.00–1.20, P=0.04, I2=40%; ) and highest (adjusted RR =1.14, 95% CI =1.01–1.29, P=0.04, I2=32%; ) prescription categories. Further analyses regarding the individual use of PDE5i revealed that the use of sildenafil was associated with a significantly increased risk for melanoma (six studies,Citation15–Citation18,Citation20 adjusted RR =1.26, 95% CI =1.07–1.50, P=0.007, I2=79%; ), whereas use of tadalafil (three studies,Citation17,Citation18,Citation20 adjusted RR =1.17, 95% CI =0.91–1.50, P=0.22, I2=53%; ) or vardenafil (two studies,Citation18,Citation20 adjusted RR =1.02, 95% CI =0.90–1.16, P=0.73, I2=0%; ) was not. Finally, the stratified analysis according to the stage of melanoma revealed that PDE5i use was associated with a significantly increased risk for in situ melanoma (two studies,Citation16,Citation20 adjusted RR =1.31, 95% CI =1.01–1.69, P=0.04, I2=69%; ), showed a trend toward increased risk for localized melanoma (three studies,Citation16,Citation20 adjusted RR =1.13, 95% CI =0.99–1.29, P=0.06, I2=23%; ), and showed a trend toward reduced risk for nonlocalized melanoma (three studies,Citation16,Citation20 adjusted RR =0.79, 95% CI =0.62–1.01, P=0.06, I2=0%; ).
Figure 3 Forest plots for the meta-analysis of the association between PDE5i use and risk of melanoma presented as adjusted RR.
Abbreviations: df, degrees of freedom; DNHR, Danish Nationwide Health Registries; IV, inverse variance; KPNC, Kaiser Permanente Northern California; PDE5i, phosphodiesterase type 5 inhibitor; RR, risk ratio; SE, standard error.
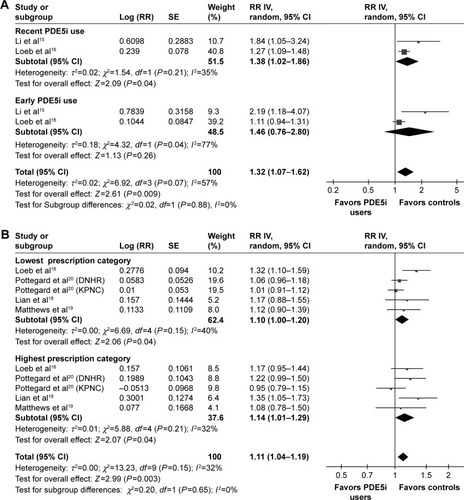
Figure 4 Forest plots for the meta-analysis of the association between PDE5i use and risk of melanoma presented as adjusted RR.
Abbreviations: df, degrees of freedom; DNHR, Danish Nationwide Health Registries; IV, inverse variance; KPNC, Kaiser Permanente Northern California; PDE5i, phosphodiesterase type 5 inhibitor; RR, risk ratio; SE, standard error.
Publication bias
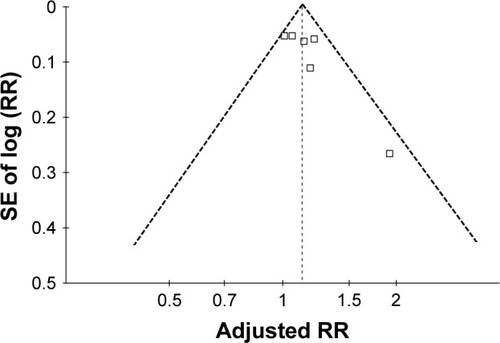
The funnel plot regarding the association between PDE5i use and risk of melanoma in the overall study is shown in . The funnel plot was symmetric on visual inspection. Based on the Egger regression test, no significant publication bias was detected for the association between PDE5i use and risk of melanoma (P=0.623).
Figure 5 Funnel plot for the association between PDE5i use and risk of melanoma.
Abbreviations: PDE5i, phosphodiesterase type 5 inhibitor; RR, risk ratio; SE, standard error.
Discussion
In this meta-analysis, upon pooling the results of all available studies, we found that the use of a PDE5i was associated with an increased risk of melanoma among male participants. Moreover, subgroup analyses indicated that the association between PDE5i use and risk of melanoma remained significant in the prospective cohort studies, in participants with recent PDE5i administration, and in participants with both the lowest and highest categories of PDE5i prescriptions. These results suggest that the association between PDE5i use and risk of melanoma appears to be sequential and probably is not dose dependent. Interestingly, we also found that the use of sildenafil was associated with a significantly increased risk for melanoma, whereas use of tadalafil or vardenafil was not. Moreover, PDE5i use was associated with a significantly increased risk for in situ melanoma, but not for localized or nonlocalized melanoma. Taken together, these results demonstrate that the use of a PDE5i, particularly sildenafil, may be associated with an increased risk of melanoma in men.
Notably, although the results of our meta-analysis support the potential association between PDE5i use and risk of melanoma, at present, we could not determine whether the association between PDE5i use and melanoma is causative. The subgroup analysis in this study, which was conducted by including prospective cohort studies, only indicated that the use of PDE5i was independently associated with an increased risk of the subsequent incidence of melanoma in men, which supports a sequential relationship between PDE5i administration and melanoma incidence. This was further enhanced by analysis of adequately adjusted results. However, since the cut-offs for categorization of the number of PDE5i prescriptions varied among the included studies, we compared the association between PDE5i use and risk of melanoma in participants based on the lowest and highest prescription categories. Although these results revealed that PDE5i use was associated with an increased risk of melanoma in men with both the lowest and highest prescription categories, the differences in the results among subgroups were not statistically significant (P for subgroup interaction =0.65). This finding also does not support a dose–response dependency in the association between PDE5i use and melanoma risk. To the best of our knowledge, no randomized controlled trial (RCT) has evaluated whether patients who received PDE5i have a significantly increased melanoma incidence compared to controls. Since RCTs with an adequate sample size and a sufficient follow-up duration appear to be the most reliable strategy to determine whether PDE5i is causative of melanoma incidence, these studies are warranted to confirm our results. In addition, the stratified analysis in this study regarding the use of individual PDE5i indicates that sildenafil was associated with an increased melanoma incidence, but tadalafil or vardenafil were not. However, few studies have reported the relationship between the use of tadalafil or vardenafil and risk of melanoma (only two or three studies). Therefore, the associations between other PDE5is, besides sildenafil, and risk of melanoma deserve further evaluation.
The mechanisms underlying the potential association between PDE5i use and risk of melanoma could be explained through the pharmacologic effects of PDE5i, which mimics the inhibition of cGMP-specific PDE5A induced by the activation of the RAS/RAF/ERK/MEK pathway in melanocytes.Citation4 Direct evidence was reported in a recently published in vitro study, which discovered a cGMP-dependent growth-promoting pathway in murine and human melanoma cells and revealed that sildenafil treatment further increases intracellular cGMP concentrations, potentiating the activation of cell proliferation.Citation14 However, it remains to be determined whether other PDE5is, besides sildenafil, have a similar influence on the proliferation and survival of melanocytes. Moreover, results from recent studies have suggested that the association between PDE5i use and risk of melanoma may be complicated, and the role of myeloid-derived suppressor cells (MDSCs) may be important.Citation28 Activation of MDSCs has been associated with blocked antitumor immunity,Citation28 while PDE5is such as sildenafilCitation29 and tadalafilCitation30,Citation31 could suppress the activated MDSCs, thereby inhibiting the growth of tumor cells. The suppressive efficacy of PDE5i for MDSCs has been confirmed in melanoma-bearing animalsCitation30,Citation32 and human patients with melanoma,Citation30,Citation33,Citation34 and a recent study showed that the PDE5i tadalafil can improve the clinical outcomes for advanced melanoma patients by enhancing antitumor immunity.Citation35 Interestingly, considering the stage of melanoma, we found that PDE5i use was associated with a significantly increased risk for in situ melanoma and also exhibited a trend toward increased risk for localized melanoma and reduced risk for nonlocalized melanoma. These findings may reflect that, for patients with advanced melanoma, PDE5i may exert an adjunctive antitumor effect by suppressing activated MDSCs. Moreover, previous studies have indicated that a BRAF somatic mutation is a major cause to the activation of the RAS/RAF/ERK/MEK pathway and the subsequent cGMP-specific PDE5A inhibition in melano-cytes, which underlies the pathogenesis of melanoma related to BRAF somatic mutations. Considering that the potential stimulatory effect of PDE5i for melanoma is by mimicking the inhibitory effect of the RAS/RAF/ERK/MEK pathway for PDE5A, the carcinogenic effect of PDE5i may be insignificant in patients for whom the cGMP-specific PDE5A has already been inhibited via BRAF somatic mutation and activation of RAS/RAF/ERK/MEK signaling. Interestingly, melanoma patients with BRAF somatic mutations are more likely to have advanced melanoma with poor prognosis, as indicated by previous clinical studiesCitation36–Citation38 and a meta-analysis.Citation39 Therefore, the association between PDE5i use and risk of melanoma may become insignificant in patients with BRAF somatic mutations, who usually have a higher risk for advanced melanoma.
Our study has limitations that should be considered when interpreting these results. First, our meta-analysis was based on a limited number of observational studies, and we did not have access to the individual patient-based data of the original studies. Although we conducted a stratified analysis to explore the potential influence of study characteristics on the association between PDE5i use and risk of melanoma, these results should be interpreted with caution. Second, as mentioned above, the results of our study could only suggest a possible association between PDE5i use and risk of melanoma. However, future studies, preferably RCTs, are needed to determine whether this relationship is causative. Moreover, as a meta-analysis of observational studies, although we combined the most adequately adjusted results, we could exclude the possibility of residual confounding factors, such as the frequencies of BRAF somatic mutations, which may influence the results of our study. In addition, when analyzing the potential influence of PDE5i prescriptions on the association between PDE5i use and risk of melanoma, we used the amount of prescriptions, which was not as accurate as the exact dose the participants actually took. This may further confound the results. Finally, our study participants were mostly Western men. Studies should also be performed to determine the association between PDE5i use and risk of melanoma in Asians.
Conclusion
PDE5i use may be associated with a significantly increased risk of melanoma in men. However, whether the association between PDE5i and melanoma is causative requires further investigation.
Author contributions
All authors contributed to the data analysis and drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
- Gray-SchopferVWellbrockCMaraisRMelanoma biology and new targeted therapyNature2007445713085185717314971
- SullivanRJFisherDEUnderstanding the biology of melanoma and therapeutic implicationsHematol Oncol Clin North Am201428343745324880940
- ThompsonJFScolyerRAKeffordRFCutaneous melanoma in the era of molecular profilingLancet2009374968736236519647595
- ArozarenaISanchez-LaordenBPackerLOncogenic BRAF induces melanoma cell invasion by downregulating the cGMP-specific phosphodiesterase PDE5ACancer Cell2011191455721215707
- FlahertyKTMcArthurGBRAF, a target in melanoma: implications for solid tumor drug developmentCancer2010116214902491320629085
- PackerLMEastPReis-FilhoJSMaraisRIdentification of direct transcriptional targets of (V600E)BRAF/MEK signalling in melanomaPigment Cell Melanoma Res200922678579819682280
- HauschildAGrobJJDemidovLVDabrafenib in BRAF-mutated metastatic melanoma: a multicentre, open-label, phase 3 randomised controlled trialLancet2012380983935836522735384
- WellbrockCHurlstoneABRAF as therapeutic target in melanomaBiochem Pharmacol201080556156720350535
- PalitVEardleyIAn update on new oral PDE5 inhibitors for the treatment of erectile dysfunctionNat Rev Urol201071160360921068761
- ScaglioneFDondeSHassanTAJanniniEAPhosphodiesterase type 5 inhibitors for the treatment of erectile dysfunction: pharmacology and clinical impact of the sildenafil citrate orodispersible tablet formulationClin Ther201739237037728139291
- VentimigliaECapogrossoPMontorsiFSaloniaAThe safety of phosphodiesterase type 5 inhibitors for erectile dysfunctionExpert Opin Drug Saf201615214115226752541
- KasumiSIn vitro effects of a phosphodiesterase inhibitor sildenafil on cellular motility of the oral malignant melanoma cellsJ Oral Maxillofac Surg2014729e96e97
- DhayadeSCNP-derived cGMP and Sildenafil promote melanoma growth in vitro and in vivo in miceNaunyn-Schmiedeberg’s Archives of Pharmacology20153881S13
- DhayadeSKaeslerSSinnbergTSildenafil potentiates a cGMP-dependent pathway to promote melanoma growthCell Rep201614112599261026971999
- LiWQQureshiAARobinsonKCHanJSildenafil use and increased risk of incident melanoma in US men: a prospective cohort studyJAMA Intern Med2014174696497024710960
- LoebSFolkvaljonYLambeMUse of Phosphodiesterase Type 5 Inhibitors for Erectile Dysfunction and Risk of Malignant MelanomaJAMA2015313242449245526103029
- BoorPMelanoma in men treated with PDE5A inhibitors: A report from the RADAR (research on adverse drug events and reports) projectJ Am Acad Dermatol2016745 Suppl 1AB190
- LianYYinHPollakMNPhosphodiesterase type 5 inhibitors and the risk of melanoma skin cancerEur Urol201670580881527178449
- MatthewsALanganSMDouglasIJSmeethLBhaskaranKPhosphodiesterase type 5 inhibitors and risk of malignant melanoma: matched cohort study using primary care data from the UK clinical practice research datalinkPLoS Med2016136e100203727299522
- PottegardASchmidtSAOlesenABUse of sildenafil or other phosphodiesterase inhibitors and risk of melanomaBr J Cancer2016115789590027529513
- KearnsJTLapinBWangEAssociations between iCOGS single nucleotide polymorphisms and upgrading in both surgical and active surveillance cohorts of men with prostate cancerEur Urol201669222322826411806
- StroupDFBerlinJAMortonSCMeta-analysis of observational studies in epidemiology: a proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) groupJAMA2000283152008201210789670
- HigginsJGreenSCochrane Handbook for Systematic Reviews of Interventions Version 5.1.0The Cochrane Collaboration2011 Available from: www.cochranehandbook.orgAccessed April 14, 2017
- WellsGASheaBO’ConnellDThe Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses2010 Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.aspAccessed April 14, 2017
- HigginsJPThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- PatsopoulosNAEvangelouEIoannidisJPSensitivity of between-study heterogeneity in meta-analysis: proposed metrics and empirical evaluationInt J Epidemiol20083751148115718424475
- EggerMDavey SmithGSchneiderMMinderCBias in meta-analysis detected by a simple, graphical testBMJ199731571096296349310563
- SicaAMassarottiMMyeloid suppressor cells in cancer and autoimmunityJ Autoimmun Epub2017717
- SerafiniPMeckelKKelsoMPhosphodiesterase-5 inhibition augments endogenous antitumor immunity by reducing myeloid-derived suppressor cell functionJ Exp Med2006203122691270217101732
- MeyerCSevkoARamacherMChronic inflammation promotes myeloid-derived suppressor cell activation blocking antitumor immunity in transgenic mouse melanoma modelProc Natl Acad Sci U S A201110841171111711621969559
- NoonanKAGhoshNRudrarajuLBuiMBorrelloITargeting immune suppression with PDE5 inhibition in end-stage multiple myelomaCancer Immunol Res20142872573124878583
- UmanskyVSildenafil prolongs survival and reduces immunosuppression in ret transgenic mouse melanoma modelEur J Immunol200939S324
- WeedDTVellaJLReisIMTadalafil reduces myeloid-derived suppressor cells and regulatory T cells and promotes tumor immunity in patients with head and neck squamous cell carcinomaClin Cancer Res2015211394825320361
- CalifanoJAKhanZNoonanKATadalafil augments tumor specific immunity in patients with head and neck squamous cell carcinomaClin Cancer Res2015211303825564570
- HasselJCJiangHBenderCTadalafil has biologic activity in human melanoma. Results of a pilot trial with Tadalafil in patients with metastatic Melanoma (TaMe)Oncoimmunology201769e132644028932631
- BarbourAPTangYHArmourNBRAF mutation status is an independent prognostic factor for resected stage IIIB and IIIC melanoma: implications for melanoma staging and adjuvant therapyEur J Cancer201450152668267625070294
- Santiago-WalkerAGagnonRMazumdarJCorrelation of BRAF mutation status in circulating-free DNA and tumor and association with clinical outcome across four BRAFi and MEKi clinical trialsClin Cancer Res201622356757426446943
- SiroyAEAungPPTorres-CabalaCAClinical significance of BRAF V600E mutational status in capsular nevi of sentinel lymph nodes in patients with primary cutaneous melanomaHum Pathol201759485427666765
- KimSYKimSNHahnHJLeeYWChoeYBAhnKJMetaanalysis of BRAF mutations and clinicopathologic characteristics in primary melanomaJ Am Acad Dermatol201572610361046.e225819940