
Abstract
Prophylactic cranial irradiation (PCI) lowers the risk of brain metastasis (BM) and increases survival in small cell lung cancer (SCLC) patients, but it also entails a risk of neurocognitive dysfunction (NCD). One strategy to mitigate this neurotoxicity is hippocampus-avoiding (HA) whole-brain radiation therapy, as the hippocampus is mainly responsible for radiation-related NCD and hippocampal or perihippocampal metastases are rare. A few prospective clinical trials have demonstrated a reduction in NCD following HA whole-brain radiation therapy. The 59-year-old male patient described in this report had limited-stage SCLC and a complete response to thoracic chemoradiotherapy. Seven months after receiving HA-PCI of 25 Gy in 10 fractions using intensity-modulated radiation therapy, a 36 mm solitary metastasis was detected in the right perihippocampal region. The mass was surgically removed but the patient died 2 months later. The development of a solitary HA region metastasis is uncommon, considering that metastasis in this area usually occurs in patients with high numbers of BMs. Our case demonstrates the need for further validation of HA-PCI for SCLC patients in terms of both neurocognitive protection and the absence of compromise in terms of BM prevention.
Introduction
Prophylactic cranial irradiation (PCI) is the standard of care for patients with small cell lung cancer (SCLC) who have had a good response to chemoradiation for their primary disease.Citation1 In a meta-analysis, PCI was shown to reduce the incidence of brain metastasis (BM) from 58% to 33% and to improve overall survival by 5.4% at 3 years.Citation2 However, a side effect of PCI is neurocognitive dysfunction (NCD). In the clinical trials of the Radiation Therapy Oncology Group (RTOG), PCI increased the risk of NCD in lung cancer patients, who did not develop BM, by almost threefold.Citation3 Common manifestations of NCD include decreased short-term memory, impaired cognition, fatigue, and depression.Citation4,Citation5
Injury to the hippocampus is mainly responsible for NCD following whole-brain radiation therapy (WBRT).Citation6 Preclinical and clinical evidence have shown a correlation between hippocampal radiation injury and NCD.Citation7,Citation8 Therefore, one strategy to mitigate NCD is to reduce the irradiation dose to the hippocampus during WBRT. Modern, sophisticated radiation therapy (RT) techniques allow the delivery of hippocampus-avoiding (HA) WBRT, in both the treatment of BM and during PCI.Citation9,Citation10 However, the risk of subsequent metastasis in this conformal avoidance region must be evaluated to determine the clinical feasibility of HA-WBRT.
In this article, we report the outcome of a patient with limited-stage SCLC who received HA-PCI but subsequently developed a solitary BM in the hippocampal avoidance region.
Case report
A 59-year-old male was admitted to the hospital due to blood-tinged sputum. He was a current smoker with a 30-year smoking history. Chest computed tomography (CT) revealed an 18 mm mass in the right upper lobe with enlarged right prevascular, upper paratracheal, hilar, interlobar, and bilateral lower paratracheal lymph nodes. Distant metastasis was not detected on an 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET)/CT, whole-body bone scan or on magnetic resonance imaging (MRI) of the brain. Endobronchial ultrasound-guided biopsy identified metastatic small cell carcinoma bilaterally in the lower paratracheal nodes. Written informed consent was provided by the patient to have the case details and any accompanying images published.
Definitive concurrent chemoradiotherapy was administered for this limited-stage SCLC, with a total of 64 Gy delivered in 32 fractions using static seven-field intensity-modulated radiotherapy (IMRT). Chemotherapy, consisting of cisplatin and etoposide, was commenced simultaneously with IMRT. Four cycles of chemotherapy were administered over a 3-week interval. Chest CT and 18F-FDG-PET/CT performed 2 months after chemoradiation showed a complete response in both the primary lung tumor and the regional lymph nodes.
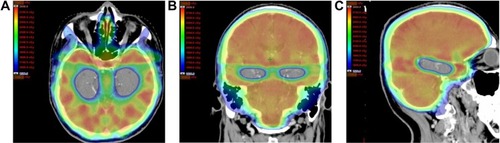
HA-PCI was performed 3 months after completion of thoracic chemoradiotherapy. The IMRT techniques followed the RTOG 0933 protocol,Citation11 a Phase II trial of HA-WBRT for patients with BM. For CT (Brilliance CT Big Bore; Philips Medical Systems, Cleveland, OH, USA) simulation, the patient was immobilized in the supine position with an aquaplast mask placed over his head. Planning CT scan images were fused with axial brain MRI. The hippocampus was contoured bilaterally on the fused MRI–CT image set and expanded by 5 mm to generate the HA region. The planning target volume was defined as the whole-brain parenchyma, excluding the HA region. The volumes of the hippocampus, HA region, and whole-brain parenchyma were 5.1 cm3, 30.4 cm3, and 1,343.8 cm3, respectively. The percentage of brain volume occupied by the HA region was 2.3%. An IMRT plan was created using the Eclipse RT planning system (Varian Medical Systems, Inc., Palo Alto, CA, USA). The plan consisted of nine static fields to cover the planning target volume, with a dose of 25 Gy administered in 10 fractions while avoiding the hippocampus (). The minimum, maximum, and mean doses to the hippocampus were 7.6 Gy, 13.6 Gy, and 8.7 Gy, respectively. IMRT was performed using a Novalis Tx system (Varian Medical Systems and BrainLab, Feldkirchen, Germany). The patient tolerated the treatments well, with no severe complications.
Figure 1 Radiotherapy planning image with the dose distribution illustrated in color.
Abbreviation: HA, hippocampus-avoiding.
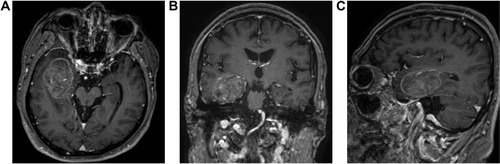
Brain MRI at 7 months after HA-PCI completion showed a 36×31 mm, well-marginated, heterogeneously enhancing mass in the right HA (perihippocampal) region with surrounding edema (). The patient’s symptoms included lower extremity weakness and dysarthria. The mass was surgically removed and identified by pathology as metastatic small cell carcinoma. The patient subsequently received palliative RT for spinal metastasis, and chemotherapy, but he died 9 months after HA-PCI.
Figure 2 Brain magnetic resonance images showing a 36×31 mm metastatic mass in the right perihippocampal area.
Discussion
The efficacy of HA-WBRT in reducing NCD has been assessed in prospective clinical trials,Citation11,Citation12 including RTOG 0933, a Phase II multi-institutional study of HA-WBRT (30 Gy in 10 fractions) for patients with BM.Citation11 The trial included patients with BMs located outside a 5 mm margin around the hippocampus, with a total of 100 patients analyzed. The mean relative decline in delayed recall from baseline to 4 months, as assessed on the Hopkins Verbal Learning Test – Revised, was significantly lower than that in the historical control (7% vs 30%, P<0.001); also, there was no decline in quality-of-life scores. Of the 67 patients who developed intracranial progression, only three (4.5%) experienced progression in the HA area. However, the patients included in the study mostly had non-small cell lung cancer (NSCLC) and breast cancer; those with SCLC were excluded from that clinical trial.
Although sample size was small (20 patients), a recent prospective study demonstrated the potential benefit of HA-PCI for SCLC patients in limiting the neuropsychological sequelae of brain radiation.Citation13 Two patients developed a metastasis in a region under-dosed during HA-PCI. Neither involved the hippocampal dentate gyrus, but one involved the HA region. Both patients developed additional concurrent metastases in the fully treated brain regions. In the current case, BM was detected in the HA region 7 months after IMRT-based HA-PCI. A distinctive feature of this case was that the BM was solitary. No concurrent BM outside the HA region was evident, and no other BM was shown prior to death.
One of the rationales for the use of HA-WBRT is that the hippocampus and perihippocampal area are uncommon sites of BM. Two retrospective studies examined the incidence of hippocampal metastasis exclusively in SCLC patients.Citation14,Citation15 Guo et alCitation14 assessed a total of 1,594 BMs (at presentation or follow-up) in 180 SCLC patients. HA region metastasis was detected in 22 (12.2%) patients: 13 perihippocampal (≤ 5 mm of hippocampus) and nine hippocampal metastases. Kundapur et alCitation15 evaluated 70 SCLC patients with BM either at presentation (de novo) or after conventional WBRT for BM. Of the 59 patients with de novo BM, three (5%) had HA region metastasis: two hippocampal and one perihippocampal. Collectively, there were 359 (range: 1–33) de novo BMs, with only three (0.8%) within ≤ 5 mm of hippocampal tissue. In 20 patients, metastatic disease in the brain progressed after WBRT, but a perihippocampal metastasis developed in only one patient (5%).
Other retrospective studies have analyzed BM in patients whose primary tumors were mainly NSCLC, breast cancer, and melanoma, but also SCLC. BM in the HA region was detected in <10% of the patients.Citation16–Citation20 Gondi et alCitation16 determined a rate of 8.6% (n=32) in 371 patients with BM. This rate was not significantly different between patients with SCLC (10.5%; n=38) and NSCLC (9.0%; n=155). However, a higher rate in SCLC than in other malignancies has also been reported. In a study by Harth et al,Citation17 BM centered within 5 mm around the hippocampus occurred in 27.3% of SCLC patients. Although there were only 11 SCLC patients, this rate contrasted with that of 8% in overall 100 patients. Wan et alCitation18 demonstrated that BM in regions of neural stem cells accounted for 2.7% of all BMs in 44 SCLC patients, compared with 0.82% of all BMs in the 283 NSCLC patients.
HA-WBRT will be of greater relevance for prophylactic than for therapeutic purposes. In BM treatment, particularly in brain oligometastases, stereotactic radiosurgery omitting WBRT is gaining acceptance.Citation21,Citation22 Stereotactic radiosurgery targets only the metastatic tumor volume, sparing all of the noninvolved brain parenchyma. Most of the ongoing prospective clinical trials of HA-WBRT in lung cancer patients are evaluating the efficacy of HA-PCI rather than therapeutic WBRT.Citation6 In addition, patients with NSCLC may be more suitable HA-PCI candidates versus patients with SCLC, as the former have a lower tendency of BM occurrence within the HA area.Citation17,Citation18 However, PCI has not been shown to confer a survival benefit in NSCLC.Citation23,Citation24
A known risk factor for HA region metastasis is a large number of BMs.Citation14,Citation18 The current case was therefore unusual as this patient had a single BM in the HA region. Although this solitary BM was removed by surgical resection, stereotactic radiosurgery may be a good alternative.Citation25
While PCI is accepted as the standard of care for patients with lung cancer, it is used suboptimally because of neurotoxicity concerns.Citation26 The rapid development of RT technology has enabled the realization of HA-PCI. This novel approach will find widespread acceptance following its rigorous validation in prospective clinical trials to examine its ability to confer neurocognitive protection and, importantly, to retain the efficacy of BM prevention.
Acknowledgments
This work was supported by the Soonchunhyang University Research Fund.
Disclosure
The author reports no conflicts of interest in this work.
References
- PechouxCLSunASlotmanBJDe RuysscherDBelderbosJGoreEMProphylactic cranial irradiation for patients with lung cancerLancet Oncol2016177e277e29327396646
- AuperinAArriagadaRPignonJPProphylactic cranial irradiation for patients with small-cell lung cancer in complete remission. Prophylactic cranial irradiation overview collaborative groupN Engl J Med1999341747648410441603
- GondiVPaulusRBrunerDWDecline in tested and self-reported cognitive functioning after prophylactic cranial irradiation for lung cancer: pooled secondary analysis of Radiation Therapy Oncology Group randomized trials 0212 and 0214Int J Radiat Oncol Biol Phys201386465666423597420
- SunABaeKGoreEMPhase III trial of prophylactic cranial irradiation compared with observation in patients with locally advanced non-small-cell lung cancer: neurocognitive and quality-of-life analysisJ Clin Oncol2011293279286
- QuXMMishraMVBaumanGSCost-effectiveness of prophylactic cranial irradiation with hippocampal avoidance in limited stage small cell lung cancerRadiother Oncol2017122341141528109544
- ZhaoRKongWShangJZheHWangYYHippocampal-sparing whole-brain radiotherapy for lung cancerClin Lung Cancer201718212713128340924
- PospisilPKazdaTHynkovaLPost-WBRT cognitive impairment and hippocampal neuronal depletion measured by in vivo metabolic MR spectroscopy: results of prospective investigational studyRadiother Oncol2017122337337928063694
- SonYYangMWangHMoonCHippocampal dysfunctions caused by cranial irradiation: a review of the experimental evidenceBrain Behav Immun20154528729625596174
- LeeKLenardsNHolsonJWhole-brain hippocampal sparing radiation therapy: volume-modulated arc therapy vs intensity-modulated radiation therapy case studyMed Dosim2016411152126235550
- RongYEvansJXu-WelliverMDosimetric evaluation of intensity-modulated radiotherapy, volumetric modulated arc therapy, and helical tomotherapy for hippocampal-avoidance whole brain radiotherapyPLoS One2015104e012622225894615
- GondiVPughSLTomeWAPreservation of memory with conformal avoidance of the hippocampal neural stem-cell compartment during whole-brain radiotherapy for brain metastases (RTOG 0933): a phase II multi-institutional trialJ Clin Oncol201432343810381625349290
- LinSYYangCCWuYMEvaluating the impact of hippocampal sparing during whole brain radiotherapy on neurocognitive functions: a preliminary report of a prospective phase II studyBiomed J201538543944925994802
- RedmondKJHalesRKAnderson-KeightlyHProspective study of hippocampal-sparing prophylactic cranial irradiation in limited-stage small cell lung cancerInt J Radiat Oncol Biol Phys201798360361128581401
- GuoWLHeZYChenYClinical features of brain metastases in small cell lung cancer: an implication for hippocampal sparing whole brain radiation therapyTransl Oncol2017101545827940373
- KundapurVEllchukTAhmedSGondiVRisk of hippocampal metastases in small cell lung cancer patients at presentation and after cranial irradiation: a safety profile study for hippocampal sparing during prophylactic or therapeutic cranial irradiationInt J Radiat Oncol Biol Phys201591478178625752392
- GondiVTomeWAMarshJEstimated risk of perihippocampal disease progression after hippocampal avoidance during whole-brain radiotherapy: safety profile for RTOG 0933Radiother Oncol201095332733120392503
- HarthSAbo-MadyanYZhengLEstimation of intracranial failure risk following hippocampal-sparing whole brain radiotherapyRadiother Oncol2013109115215824100152
- WanJFZhangSJWangLZhaoKLImplications for preserving neural stem cells in whole brain radiotherapy and prophylactic cranial irradiation: a review of 2270 metastases in 488 patientsJ Radiat Res201354228529123022606
- WuSGRaoMYZhouJDistribution of metastatic disease in the brain in relation to the hippocampus: a retrospective single-center analysis of 6064 metastases in 632 patientsOncotarget2015641440304403626536661
- GhiaATomeWAThomasSDistribution of brain metastases in relation to the hippocampus: implications for neurocognitive functional preservationInt J Radiat Oncol Biol Phys200768497197717446005
- BrownPDJaeckleKBallmanKVEffect of radiosurgery alone vs radiosurgery with whole brain radiation therapy on cognitive function in patients with 1 to 3 brain metastases: a randomized clinical trialJAMA2016316440140927458945
- KocherMSoffiettiRAbaciogluUAdjuvant whole-brain radiotherapy versus observation after radiosurgery or surgical resection of one to three cerebral metastases: results of the EORTC 22952–26001 studyJ Clin Oncol2011292134141
- GoreEMBaeKWongSJPhase III comparison of prophylactic cranial irradiation versus observation in patients with locally advanced non-small-cell lung cancer: primary analysis of radiation therapy oncology group study RTOG 0214J Clin Oncol2011293272278
- ParkHSDeckerRHWilsonLDYuJBProphylactic cranial irradiation for patients with locally advanced non-small-cell lung cancer at high risk for brain metastasesClin Lung Cancer201516429229725499149
- WonYKLeeJYKangYNStereotactic radiosurgery for brain metastasis in non-small cell lung cancerRadiat Oncol J201533320721626484304
- GiulianiMSunABezjakAUtilization of prophylactic cranial irradiation in patients with limited stage small cell lung carcinomaCancer2010116245694569920803612