
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objective
The study aimed to screen microRNAs (miRNAs) that can be used for the early detection of colorectal cancer (CRC) based on differential expression of miRNA in serum.
Materials and methods
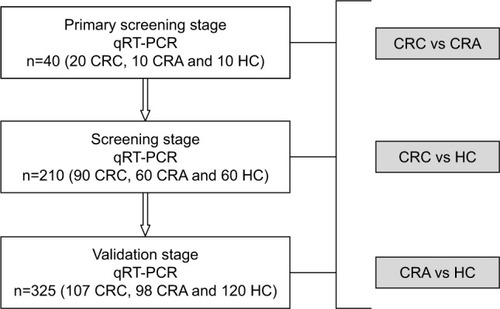
A three-stage study was designed with a total of 217 CRCs, 168 colorectal adenomas (CRAs), and 190 healthy controls (HCs). A quantitative reverse transcription polymerase chain reaction was performed in three stages. We screened 528 miRNA expression profiles in the sera of 40 patients (CRC n=20, CRA n=10, and HC n=10) for candidate miRNAs, then 210 serum samples (CRC n=90, CRA n=60, and HC n=60) were used for screening of candidate miRNAs. Three hundred and twenty-five independent individual samples (CRC n=107, CRA n=98, and HC n=120) were used to validate the most differentially-expressed miRNAs in the screening stage, and binary logistic regression was used in the validation stage. A receiver operating characteristic curve was drawn to evaluate the diagnostic accuracy.
Results
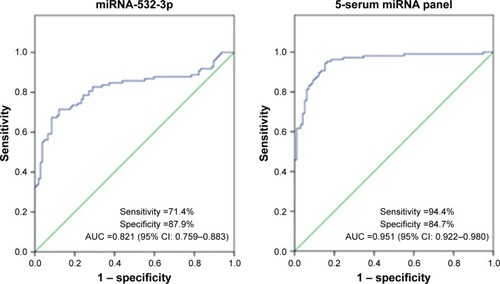
A 5-serum miRNA panel (miRNA-1246, miRNA-202-3p, miRNA-21-3p, miRNA-1229-3p, and miRNA-532-3p) effectively distinguished CRCs from HCs with 91.6% sensitivity and 91.7% specificity. The area under the curve (AUC) was 0.960 (95% confidence interval [CI]: 0.937–0.983). In addition, the panel also accurately distinguished CRCs from CRAs with 94.4% sensitivity and 84.7% specificity. The AUC was 0.951 (95% CI: 0.922–0.980).
Conclusion
Our 5-serum miRNA panel accurately distinguished CRCs from CRAs and HCs with high sensitivity and specificity. The 5-serum miRNA panel may be a promising prospect for application as a nonintrusive and inexpensive method for the early detection of CRC.
Keywords:
Introduction
Colorectal cancer (CRC) is one of the most common malignant tumors. The incidence of CRC among malignant tumors in males and females ranks third and second, respectively. In fact, 1.3 million people are diagnosed with CRC and there are nearly 700,000 deaths annually worldwide; CRC ranks fourth among cancer-related deaths.Citation1 In China, the number of new cases of CRC in 2015 exceeded 3,763,000 and the number of CRC-specific deaths was approximately 1,910,000.Citation2 In recent years, with the improvement in living standards and Westernization of lifestyles, the incidence and mortality of CRC have shown a rising trend year after year. Indeed, most patients with CRC are in an advanced stage at the time of diagnosis and have lost curability. The current study showed that the mortality rate of CRC was highly correlated with the stage of disease. The 5-year survival rate for stage I CRC approaches 90%, but is only 12% for stage IV.Citation3 It is evident that early detection of CRC and appropriate treatment are important. Currently, the common methods for early detection of CRC include the plasma carcinoembryonic antigen (CEA) level, fecal occult blood testing, and fiberoptic colonoscopy; however, the plasma CEA level and fecal occult blood testing are not highly sensitive, and therefore their value is limited.Citation4–Citation6 Colonoscopy is considered the gold standard for detection of CRC; however, colonoscopy is still limited as an effective approach for early detection due to poor patient compliance, resulting from discomfort during bowel preparation and the examination, as well as the potential complications.Citation7 Therefore, a new method which is less invasive, highly accurate, and of clinical value for the early detection of CRC is warranted.
MicroRNAs (miRNAs) are a class of noncoding single-stranded RNA molecules (approximately 21–23 nucleotides in length) coded by endogenous genes and specifically bound to the 3′ untranslated region of target mRNAs to inhibit translation and promote degradation.Citation8 miRNAs participate in a variety of vital biological processes, including cell differentiation, proliferation, and apoptosis. The mechanism of its action may be related to miRNA-related single nucleotide polymorphisms.Citation9–Citation12 It has been reported that abnormally-expressed miRNA, as an oncogene or tumor suppressor, plays an important role in cancer initiation and progression, including lung, liver, pancreatic, bladder, gastric, ovarian, and colorectal cancers.Citation13–Citation17 There are a variety of miRNAs in human blood that are usually derived from lysis of apoptotic or necrotic cells and secretion of specific cells.Citation18 miRNAs remain stable by binding to Argonaute 2 proteinCitation19 or through the autospecific hairpin structure,Citation20 which prevents degradation by ribonuclease in the blood and facilitates quantitative detection. In 2008, Lawrie et alCitation21 first reported the quantitative detection of miRNA in serum samples, proving the feasibility for the approach. An increasing number of studies on various diseases, especially on tumors, have focused on circulation miRNA.Citation22,Citation23 However, in our study, more samples were included and the method of quantitative reverse transcription polymerase chain reaction (qRT-PCR) cost less. The objective of the current study was to identify differentially-expressed miRNAs and to determine the feasibility of their use in the early detection of CRC.
Materials and methods
Study subjects
The study was approved by the Ethics Committee of the Chinese PLA General Hospital, and all patients signed written informed consent forms. The inclusion criteria were as follows: (1) colonoscopy; (2) no inflammatory bowel diseases, hereditary adenomatous polyposis, family history of tumors, and other tumors in the preceding or corresponding periods; (3) colorectal adenomas (CRAs) and CRCs should have pathologic confirmation; and (4) no preoperative chemotherapy for patients with CRC. The patients with CRC were staged according to the TNM staging system of the American Joint Committee on Cancer.Citation49 A total of 575 patients were enrolled from the Department of Gastrointestinal Surgical Oncology, Department of Gastroenterology, and Medical Examination Center of the Chinese PLA General Hospital between April 2013 and December 2014. Their general statistical information is presented in . The collection of all blood samples followed a uniform protocol, ie, a 5-mL vacuum blood collection tube (VACUETTE®; Greiner Bio-One, Frickenhausen, Germany) was used to collect blood, and the sample was allowed to stand for 2 h at room temperature to fully coagulate, and then centrifuged at 1,500 rpm (2,390×g) at 4°C for 7 min. The centrifugation was completed within 4 h after blood collection. The serum samples collected after centrifugation were stored in a −80°C refrigerator.
Table 1 Clinical characteristics of patients
Study design
Our study was divided into three stages (primary screening, screening, and validation). The study design is shown in .
Figure 1 Study design.
Primary screening and screening stages
During the primary screening stage, we screened 528 miRNA expression profiles in 40 serum samples, and CRCs, CRAs, and healthy controls (HCs) were compared in pairs. One hundred and five miRNAs were differentially expressed (–). The primary screening criteria for differentially-expressed miRNAs were as follows: (1) mean cycle threshold (Ct) <32 and SD within groups <2; (2) 5 Cts less than the negative control (no template control); and (3) the Ct value of the same sample was standardized on the same plate with an external reference (cel-miR-67) to obtain the ∆Ct value for comparison between groups and to select the most differentially-expressed miRNAs.
The serum sample size was expanded (n=210) and candidate miRNAs (105 miRNAs in the primary screening stage) satisfying the above three criteria for primary screening were rescreened. The screening criteria were as follows: (1) the results of primary screening and screening were compared, and miRNAs with consistent expression patterns or mean Ct differences between groups >1 were selected; (2) mean Ct <30; and (3) the Ct value of the same sample was standardized on the same plate with an external reference (cel-miR-67) to obtain the ∆Ct value for comparison between groups and to select the most differentially-expressed miRNAs. Validation was conducted on miRNAs which satisfied all three screening criteria.
Validation stage
During the screening stage, we identified 10 most significant miRNAs. There were 5 miRNAs in group of HC vs CRA, 9 miRNAs in groups of CRA vs HC, and 9 miRNAs in group of CRC vs HC. But some miRNAs are repetitive (, and ). Three hundred and twenty-five serum samples (CRC n=107, CRA n=98, and HC n=120) were used to validate the difference and binary logistic regression was based on data from the validation stage. We validated the 5 miRNAs with the most significant difference (). A receiver operating characteristic curve was drawn and a relevant mathematical model was established for detection of CRC.
Table 2 Different expression of microRNAs in individuals with colorectal cancer compared to healthy controls (screening stage)
Table 3 Different expression of microRNAs in individuals with colorectal cancer compared to colorectal adenoma (screening stage)
Extraction of serum total RNA
During extraction of total RNA, 1 μL of cel-miR-67 (20 nM/L; Quantobio, Beijing, China) was added to each sample as an external reference. A total of 0.25 mL of serum was used in the extraction of total RNA following the procedures in the miRNA extraction kit (Biochain, Beijing, China). A Nanodrop2000c spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA) was used to measure the quality of total RNA and the OD260-to-OD280 ratio was within 1.8–2.1.
Quantitative reverse transcription polymerase chain reaction
During the screening and validation stages, we used a three-step qRT-PCR. PolyA polymerase (NEB, Beijing, China) was used to add an A tail for the miRNA primer and mature miRNA. The reaction system was in a volume of 20 μL at 37°C for 1 h. Then, cRNA was synthetized by reverse transcription. One microliter of universal reverse transcription primer (Quantobio) of the tested 528 miRNAs was added to each reaction tube and incubated at 70°C for 5 min, 4°C for 2–10 min, 50°C for 50 min, and 70°C for 15 min. cDNA was obtained. qPCR was performed on an ABI 7900 High Throughput Rapid Real-time Fluorescence Quantitative PCR Amplifier (Applied Biosystems; Thermo Fisher Scientific) at 95°C for 5 min, followed by 40 cycles at 95°C for 15 s and 60°C for 45 s. The melting analysis was added to evaluate the specificity of the PCR products: 95°C for 15 s, 60°C for 15 s, and then 95°C for 15 s. Quantification of the PCR product was evaluated by the level of fluorescence emitted by SYBR Green (SYBR® Premix Ex Taq™ II; TaKaRa, Beijing, China).
Statistical analysis
The ∆Ct value was used to represent the relative level of expression of a single miRNA. A two-tailed t-test was used between two independent samples to identify significantly-expressed miRNA. Binary logistic regression was used during the validation stage and a receiver operating characteristic curve was drawn to calculate the area under the curve (AUC) and assess the diagnostic value of miRNA for CRC. Based on relevant parameters in binary logistic regression, we established a mathematical diagnosis equation for detection of CRC. SPSS software (version 17.0; SPSS, Inc., Chicago, IL, USA) was used to perform all statistical analyses. Differences were considered significant at p<0.05.
Results
Comparison between CRCs and HCs
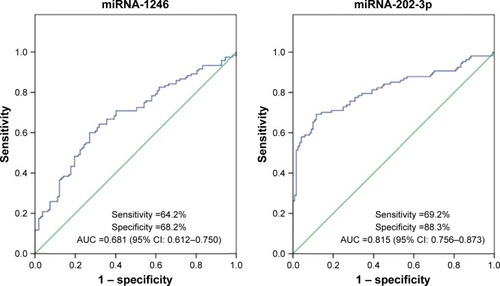
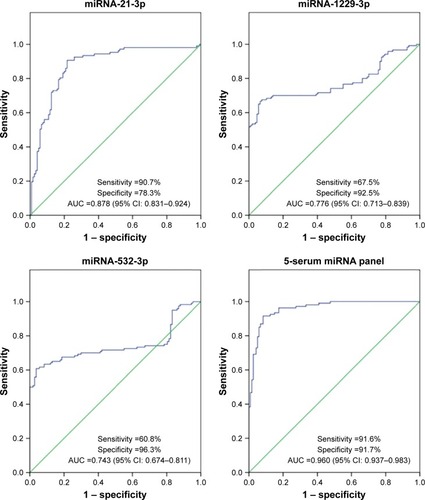
As compared with HCs, there was a significant difference in 9 miRNAs in the sera of patients with CRC during the screening stage (). After validation, a panel of 5 miRNAs (miRNA-1246, miRNA-202-3p, miRNA-21-3p, miRNA-1229-3p, and miRNA-532-3p) effectively distinguished CRCs (n=107) from HCs (n=120), with 91.6% sensitivity and 91.7% specificity. The AUC was 0.960 (95% confidence interval [CI]: 0.937–0.983) (). Based on relevant parameters in binary logistic regression, a diagnosis discriminant model was established according to the following equation:
Figure 2 Validation stage, colorectal cancers compared to healthy controls.
Abbreviations: AUC, area under the curve; miRNA, microRNA.
The cutoff value was 0.502. When Y1<0.502, the detection result was negative, and determined to be a HC. When Y1≥0.502, the detection result was positive, and determined to be a CRC.
Comparison between CRCs and CRAs
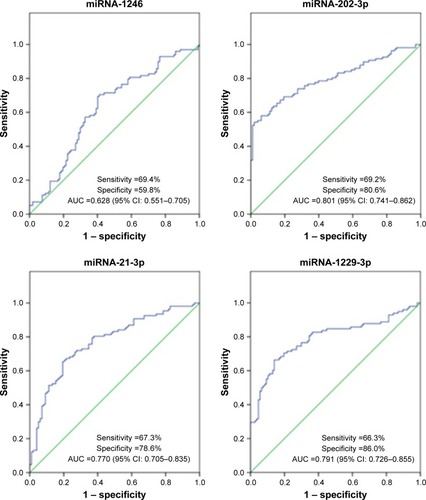
As compared with the CRA group, there was a significant difference in 9 miRNAs in the sera of patients with CRCs during the screening stage (). After validation, a panel of 5 miRNAs (miRNA-1246, miRNA-202-3p, miRNA-21-3p, miRNA-1229-3p, and miRNA-532-3p) effectively distinguished CRCs (n=107) from CRAs (n=98), with 94.4% sensitivity and 84.7% specificity. The AUC was 0.951 (95% CI: 0.922–0.980) (). Based on relevant parameters in binary logistic regression, a diagnosis discriminant model was established according to the following equation:
Figure 3 Validation stage, colorectal cancers compared to colorectal adenomas.
The cutoff value was 0.348. When Y2<0.348, the detection result was negative, and determined to be a CRA. When Y2≥0.348, the detection result was positive, and determined to be a CRC.
Discussion
The incidence of CRC is increasing year after year. A former study revealed that good prognosis can be achieved for the majority of CRC patients if there is early detection and appropriate treatment.Citation24 Therefore, early detection becomes key for disease prophylaxis. In recent years, circulating miRNAs have attracted increased attention from investigators, which have become markers for early tumor detection. Chen et alCitation25 reported that serum miRNA expression profiling of patients with CRC differs from the healthy population, and believed that part of the abnormally-expressed miRNA could be used for detection of CRC. Ng et alCitation26 reported that in patients with CRC, the level of miRNA-92a expression is significantly increased not only in cancer tissues, but in plasma as well. After resection of cancerous tissue during surgery, however, plasma miRNA-92a is restored to the normal level and it was confirmed that high miRNA-92a expression is unrelated to inflammatory bowel disease and gastric cancer. Huang et alCitation27 monitored the levels of miRNA-92a expression in 20 CRC patients before and after surgery. The results indicated an obvious decrease after surgery, which was consistent with the findings of Ng et al,Citation26 further confirming the value of miRNA92a in detection of CRC. Toiyama et alCitation28 tested abnormally-expressed miRNA in serum samples of patients with CRCs, CRAs, and HCs, and found that the level of miR-21 expression in sera of patients with CRAs and CRCs before surgery was increased and significantly decreased after surgery. They concluded that miR-21 is a potential marker for the early detection of CRC. Kanaan et alCitation29 reported that the sensitivity and specificity of distinguishing CRC from the control group based on increased miR-21 expression in plasma were up to 90%; however, miR-92a and miR-21 had poor organ specificity: miRNA-92a was increased in patients with acute leukemia and cervical cancer;Citation30,Citation31 and miR-21 was also highly expressed in patients with lung, breast, esophageal, and gastric cancers.Citation32 Therefore, it may be difficult to assess results when a single miRNA is used as a diagnostic marker. More and more investigators have proposed a combination of several miRNAs to improve diagnostic efficiency. Some studies have also confirmed the feasibility of a panel consisting of multiple circulating miRNAs in the early detection of CRC. Luo et alCitation33 showed that 9 differentially-expressed miRNAs (miR-18a, miR-20a, miR-21, miR-29a, miR-92a, miR-106b, miR-133a, miR-143, and miR-145) are present in the plasma of patients with CRC. The 9-miRNA panel accurately distinguished patients with CRC from patients with non-CRC, with an AUC of 0.745. Wang et alCitation34 reported that a panel consisting of miR-409-3p, miR-7, and miR-93 accurately diagnosed CRC with a sensitivity of 82%, specificity of 89%, and AUC of 0.897. Zheng et alCitation35 believed that a 4-serum miRNA panel (miR-19a-3p, miR-223-3p, miR-92a-3p, and miR-422a) diagnosed early CRC with an AUC up to 0.951. Moreover, the panel accurately identified CRCs, CRAs, and HCs with AUCs of 0.886 and 0.765, respectively. Zhu et alCitation36 showed that the serum levels of miR-19a-3p, miR-21-5p, and miR-425-5p expression in patients with CRC were higher than normal controls. The panel could be used in detection of CRC with an AUC of 0.830. Nevertheless, there are currently no relevant diagnostic products widely available for clinical use, probably because of the variety of races and samples, and different detection approaches. Therefore, we suggest that additional research data are warranted to provide theoretical support for clinical use.
A total of 575 serum samples were collected in this study, including 217 CRCs, 168 CRAs, and 190 HCs. qRT-PCR was used in all three stages. Through screening and validation, a 5-serum miRNA panel (miRNA-1246, miRNA-202-3p, miRNA-21-3p, miRNA-1229-3p, and miRNA-532-3p) was confirmed to differentiate CRCs from HCs, and CRCs from CRAs. The AUCs were 0.960 and 0.951, respectively, which were superior to previous studies.Citation33–Citation38 As compared with the CRC group, there was a significant difference in the serum level of expression of 5 miRNAs in the HC and CRA groups. All new diagnostic tests have limitations, especially pertaining to the sample size of the study. A total of 575 serum samples were included in our study, which is larger than other studies, thus ensuring the reliability of the test results. In addition, we adopted a three-step qRT-PCR to avoid the false-negative results in the two-step method caused by stem-loop primers, and adopted a mash-up of long and short primers to ensure high efficiency and accuracy of the amplification. Finally, we also established a mathematical model for CRC detection, which provides great convenience for future clinical application.
Proper standardization is crucial for accurate quantitation of miRNA expression by qRT-PCR. Kanaan et alCitation39 reported that a panel of 3 plasma miRNAs (miR-431, miR-15b, and miR-139-3p) distinguished stage IV CRC from controls and successfully used U6 as an internal control to standardize miRNA expression. Rice et alCitation40 recommended using RNU6 and miR-520d-5p as reliable internal controls in a study of plasma miRNA; however, some reports hold the view that U6 is not expressed constantly and easily degraded by RNase in the circulation; the stability is poor.Citation25,Citation41,Citation42 To date, no uniform standard for internal control has been established. Therefore, it has been proposed to use an external reference for standardization of the level of circulating miRNA expression.Citation43 Wang et alCitation44 concluded that the miRNA (cel-miR-39) of Caenorhabditis elegans is nonhomologous with humans and has good repeatability and high stability. Therefore, cel-miR-39 can be used for quantification of circulating miRNA by qRT-PCR. Zhu et alCitation36 reported that the serum levels of miR-19a-3p, miR-21-5p, and miR-425-5p expression in patients with CRC are significantly higher than in the control group. They also used cel-miR-39 as an external reference for standardized calculation of the relative expression of miRNAs. Cel-miR-67 is a miRNA of C. elegans. It has no homology with human miRNA and meets the requirement of external reference.Citation45 We successfully used cel-miR-67 (primer sequence, CAACCTCCTAGAAAGAGTA) as an external reference and obtained stable and repeatable results.
Wang et alCitation46 reported that upregulation of miRNA-1246 in CRC tissues may cause disease progression. The cause can be miRNA-1246 binding to CCNG2 in CRC cells, which inhibits the expression of cyclin 2 (CycG2). Lai and FriedmanCitation47 detected that miRNA-1246 is significantly increased in the sera of patients with CRC and suggested that miRNA-1246 could be used as a potential biomarker for early detection of CRC. Wang et alCitation48 showed low expression of miRNA-202-3p in cancer tissues in patients with CRC and demonstrated overexpression of miRNA-202-3p inhibited growth of CRC cells in vitro. However, we have not uncovered any reports that the three miRNAs (miR-21-3p, miR-532-3p, and miR-1229-3p) serve as markers for the early detection of CRC, as reported for the first time in the current study.
Conclusion
Circulating miRNAs can be considered to be important biomarkers for detection of CRC. We found 5 differentially-expressed miRNAs in serum, and as a non-invasive screening approach for CRC, with high sensitivity and specificity, the panel may be used for accurate early detection of CRC, which is a promising prospect for clinical application.
Acknowledgments
We thank Ms Xinxin Liu and Mr Gaoshang Song for their support. This work was supported by the 863 project of China (No 2014AA020802).
Supplementary materials
Figure S1 The 5 microRNAs have different expression in the 3 groups.
Abbreviations: CRA, colorectal adenoma; CRC, colorectal cancer; HC, healthy control.
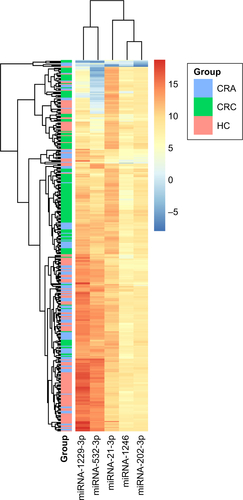
Table S1 Different expression of microRNAs in individuals with colorectal cancer compared to colorectal adenoma (primary screening stage)
Table S2 Different expression of microRNAs in individuals with colorectal adenoma compared to healthy controls (primary screening stage)
Table S3 Different expression of microRNAs in individuals with colorectal cancer compared to healthy controls (primary screening stage)
Table S4 Different expression of microRNAs in individuals with colorectal adenoma compared to healthy controls (screening stage)
Disclosure
The authors report no conflicts of interest in this work.
References
- McGuireSWorld Cancer Report 2014Geneva, SwitzerlandWorld Health Organization, International Agency for Research on Cancer, WHO Press2015 Adv Nutr2016741841926980827
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211513226808342
- El-ShamiKOeffingerKCErbNLAmerican Cancer Society Colorectal Cancer Survivorship Care GuidelinesCA Cancer J Clin201565642845526348643
- FakihMGPadmanabhanACEA monitoring in colorectal cancer. What you should knowOncology (Williston Park)2006206579587 discussion 588, 594, 596 passim16773844
- YoungGPSymondsELAllisonJEAdvances in Fecal Occult Blood Tests: the FIT revolutionDig Dis Sci201560360962225492500
- LiebermanDScreening, surveillance and prevention of colorectal cancerGastrointest Endosc Clin N Am200818359560518674706
- NicholsonFBKormanMGAcceptance of flexible sigmoidoscopy and colonoscopy for screening and surveillance in colorectal cancer preventionJ Med Screen2005122899515949120
- LinSGregoryRIMicroRNA biogenesis pathways in cancerNat Rev Cancer201515632133325998712
- GopalakrishnanCKamarajBPurohitRMutations in microRNA binding sites of CEP genes involved in cancerCell Biochem Biophys20147031933194225115610
- BhaumikPGopalakrishnanCKamarajBPurohitRSingle nucleotide polymorphisms in microRNA binding sites:implications in colorectal cancerScientific WorldJournal2014201454715425654126
- KamarajBGopalakrishnanCPurohitRIn silico analysis of miRNA-mediated gene regulation in OCA and OA genesCell Biochem Biophys20147031923193225060099
- KumarAPurohitRUse of long term molecular dynamics simulation in predicting cancer associated SNPsPLoS Comput Biol2014104e100331824722014
- MeltzerPSCancer genomics: small RNAs with big impactsNature2005435704374574615944682
- VoliniaSCalinGALiuCGA microRNA expression signature of human solid tumors defines cancer gene targetsProc Natl Acad Sci U S A200610372257226116461460
- MichaelMZO’ConnorSMvan Holst PellekaanNGYoungGPJamesRJReduced accumulation of specific microRNAs in colorectal neoplasiaMol Cancer Res200311288289114573789
- CalinGACroceCMMicroRNA signatures in human cancersNat Rev Cancer200661185786617060945
- LuJGetzGMiskaEAMicroRNA expression profiles classify human cancersNature2005435704383483815944708
- ValadiHEkströmKBossiosASjöstrandMLeeJJLötvallJOExosome-mediated transfer of mRNAs and microRNAs is a novel mechanism of genetic exchange between cellsNat Cell Biol20079665465917486113
- ArroyoJDChevilletJRKrohEMArgonaute2 complexes carry a population of circulating microRNAs independent of vesicles in human plasmaProc Natl Acad Sci U S A2011108125003500821383194
- CreemersEETijsenAJPintoYMCirculating microRNAs: novel biomarkers and extracellular communicators in cardiovascular disease?Circ Res2012110348349522302755
- LawrieASCardiganRAWilliamsonLMMachinSJMackieIJThe dynamics of clot formation in fresh-frozen plasmaVox Sang200894430631418266780
- ChevilletJRLeeIBriggsHAHeYWangKIssues and prospects of microRNA-based biomarkers in blood and other body fluidsMolecules20141956080610524830712
- MitchellPSParkinRKKrohEMCirculating microRNAs as stable blood-based markers for cancer detectionProc Natl Acad Sci U S A200810530105131051818663219
- AkkocaANYanikSOzdemirZTTNM and Modified Dukes staging along with the demographic characteristics of patients with colorectal carcinomaInt J Clin Exp Med2014792828283525356145
- ChenXBaYMaLCharacterization of microRNAs in serum: a novel class of biomarkers for diagnosis of cancer and other diseasesCell Res20081810997100618766170
- NgEKChongWWJinHDifferential expression of microRNAs in plasma of patients with colorectal cancer: a potential marker for colorectal cancer screeningGut200958101375138119201770
- HuangZHuangDNiSPengZShengWDuXPlasma microRNAs are promising novel biomarkers for early detection of colorectal cancerInt J Cancer2010127111812619876917
- ToiyamaYTakahashiMHurKSerum miR-21 as a diagnostic and prognostic biomarker in colorectal cancerJ Natl Cancer Inst20131051284985923704278
- KanaanZRaiSNEichenbergerMRPlasma miR-21: a potential diagnostic marker of colorectal cancerAnn Surg2012256354455122868372
- OhyashikiJHUmezuTKobayashiCImpact on cell to plasma ratio of miR-92a in patients with acute leukemia: in vivo assessment of cell to plasma ratio of miR-92aBMC Res Notes2010334721182798
- KongQTangZXiangFDiagnostic value of serum hsa-mir-92a in patients with cervical cancerClin Lab201763233534028182350
- WangBZhangQThe expression and clinical significance of circulating microRNA-21 in serum of five solid tumorsJ Cancer Res Clin Oncol2012138101659166622638884
- LuoXStockCBurwinkelBBrennerHIdentification and evaluation of plasma microRNAs for early detection of colorectal cancerPLoS One201385e6288023690963
- WangSXiangJLiZA plasma microRNA panel for early detection of colorectal cancerInt J Cancer2015136115216123456911
- ZhengGDuLYangXSerum microRNA panel as biomarkers for early diagnosis of colorectal adenocarcinomaBr J Cancer2014111101985199225233400
- ZhuMHuangZZhuDA panel of microRNA signature in serum for colorectal cancer diagnosisOncotarget2017810170811709128177881
- CarterJVRobertsHLPanJA highly predictive model for diagnosis of colorectal neoplasms using plasma microRNA: improving specificity and sensitivityAnn Surg2016264457558427471839
- ChenWYZhaoXJYuZFThe potential of plasma miRNAs for diagnosis and risk estimation of colorectal cancerInt J Clin Exp Pathol2015867092710126261602
- KanaanZRobertsHEichenbergerMRA plasma microRNA panel for detection of colorectal adenomas:a step toward more precise screening for colorectal cancerAnn Surg2013258340040824022433
- RiceJRobertsHRaiSNGalandiukSHousekeeping genes for studies of plasma microRNA: a need for more precise standardizationSurgery201515851345135126094174
- ChenXLiangHGuanDA combination of Let-7d, Let-7g and Let-7i serves as a stable reference for normalization of serum microRNAsPLOS One2013811e7965224223986
- WulfkenLMMoritzROhlmannCMicroRNAs in renal cell carcinoma: diagnostic implications of serum miR-1233 levelsPLoS One201169e2578721984948
- LiuZLSliningerPJUniversal external RNA controls for microbial gene expression analysis using microarray and qRT-PCRJ Microbiol Methods200768348649617173990
- WangQHuangZNiSPlasma miR-601 and miR-760 are novel biomarkers for the early detection of colorectal cancerPLoS One201279e4439822970209
- LauNCLimLPWeinsteinEGBartelDPAn abundant class of tiny RNAs with probable regulatory roles in Caenorhabditis elegansScience2001294554385886211679671
- WangSZengYZhouJMMicroRNA-1246 promotes growth and metastasis of colorectal cancer cells involving CCNG2 reductionMol Med Rep201613127328026573378
- LaiXFriedmanAExosomal microRNA concentrations in colorectal cancer: a mathematical modelJ Theor Biol2017415708327993628
- WangQHuangZGuoWMicroRNA-202-3p inhibits cell proliferation by targeting ADP-ribosylation factor-like 5A in human colorectal carcinomaClin Cancer Res20142051146115724327274
- EdgeSBComptonCCThe American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNMAnn Surg Oncol20101761471147420180029