
Abstract
Background
Ovarian adenosquamous carcinoma is an extremely rare type of ovarian histology. Platinum-refractory disease is also uncommon, but can be fatal because of the lack of available treatment options. To date, there is no study or case report on platinum-refractory ovarian adenosquamous carcinoma or its relevant treatment.
Case presentation
Herein, we report the case of a 38-year-old Chinese woman with platinum-refractory advanced ovarian adenosquamous carcinoma who received clinical benefit from poly adenosine diphosphate ([ADP] ribose) polymerase and programmed death-1 inhibitors after failure of prior multiline chemotherapies and antiangiogenic agents. The targeted therapy and immunotherapy-controlled disease deterioration and improved performance status. Thus far, the patient has survived longer than 15 months, and she is taking nivolumab as maintenance treatment.
Conclusion
Targeted therapy and immunotherapy may be options for rare categories of ovarian cancer, but this warrants more clinical evidence of efficacy and toxicity.
Background
Ovarian cancer is the leading cause of death among gynecologic malignancies. Adenosquamous carcinoma is an extremely rare primary malignant tumor of the ovary, accounting for <1% of all ovarian malignancies.Citation1 We searched the PubMed database (up to April 14, 2018) using the search terms “ovarian adenosquamous carcinoma” and “‘adenosquamous carcinoma’ and ‘ovary.’” Our search generated 11 articles, most of which were case reports without an established therapeutic regimen for ovarian adenosquamous carcinoma.
Standard initial multiple modality treatment for ovarian cancer includes primary debulking surgery followed by platinum-based chemotherapy regimens.Citation2 However, about 20%–25% of patients with ovarian cancer relapse during first-line chemotherapy;Citation3 these cases are classified as platinum-refractory by the Gynecologic Oncology Group. Platinum-refractory ovarian cancer is usually fatal because there are no other treatment options. No standard second-line or beyond chemotherapy regimens are superior in safety or efficacyCitation4 for platinum-refractory ovarian cancer.
To date, there is no study or case report on platinum-refractory ovarian adenosquamous carcinoma or any relevant treatment options. However, there may be targeted treatment options that have shown efficacy in other tumor types. Tumor angiogenesis plays a pivotal role in the growth and metastasis of ovarian cancer, mediated by vascular endothelial growth factor (VEGF) binding and signaling through cell surface VEGF receptors. Approximately 10%–15% of patients with ovarian cancer have deleterious germline BRCAmutations.Citation5 Programmed death ligand 1 (PD-L1), an immune checkpoint receptor ligand, is expressed in many types of human tumors and allows the tumor to escape the host immune system via programmed cell death-1 (PD-1) signaling. These signaling pathways may represent new treatment options for ovarian cancer. We present a woman with platinum-refractory advanced ovarian adenosquamous carcinoma treated using targeted and immune agents after failure to respond to multiple chemotherapies.
Case presentation
A 38-year-old woman was admitted to the Changhai Hospital in Shanghai on August 22, 2016, for abdominal aching pain and lumbago. She had been previously diagnosed with ovarian endometrial cysts through ultrasound at the Obstetrics and Gynecology Hospital of Fudan University in 2009. We determined that the patient had a mixed mass 7.0×5.2×6.5 cm3 in the left adnexal area and moderate ascites. The patient underwent debulking surgery on September 27, 2016, including curettage, total hysterectomy, bilateral adnexectomy, greater omentum resection, and appendectomy. Pathological examination revealed endometrioid adenocarcinoma with moderate differentiation; however, intermixed squamous differentiation in partial region was observed in the result of consultation from Fudan University Shanghai Cancer Center. Referring to immunohistochemical reevaluation, which was CAM5.2 (+), CK7 (+), PAX8 (+), CK20 (+) partly, Ki-67 (50%), vimentin (+) partly, P53 (−), WT1 (−), CD10 (+) partly, P63 (+) partly, β-catenin (+), ER (−), PR (−), and P16 (+) partly, adenosquamous carcinoma was confirmed ultimately (). The patient’s serum CA125 level was 245.00 U/mL and her serum CA19-9 level exceeded 1,200 U/mL on August 22, 2016, preoperatively, and they had decreased to 8.9 and 20.8 U/mL, respectively, on October 19, 2016, after surgery. She was diagnosed with International Federation of Gynecology and Obstetrics 2010 stage IIA disease according to the pathology and treated with intravenous docetaxel (75 mg/m2) and intravenous united intraperitoneal carboplatin (area under the cute =5, on days 1 and 2) for 2 cycles. During the first cycle, the serum CA19-9 increased over the normal range (). The response evaluation before the third cycle indicated PD according to the Response Evaluation Criteria in Solid Tumors 1.0 criteria. The patient’s positron emission tomography-computed tomography results revealed metastases in the apex of the left lung, retroperitoneal lymph nodes, left armpit, and right side of the pelvic cavity, which was further clarified by pelvic magnetic resonance imaging (MRI; ). In addition, her serum CA19-9 level almost tripled within a month.
Figure 1 Immunohistochemical analysis showing (A) CAM5.2 (+) and (B) Ki-67 (50%).
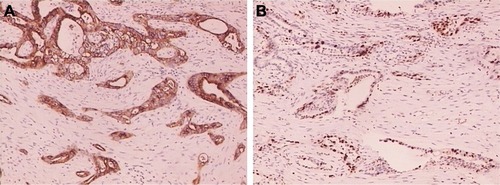
Figure 2 Serum CA19-9 and CA125 levels during treatment.
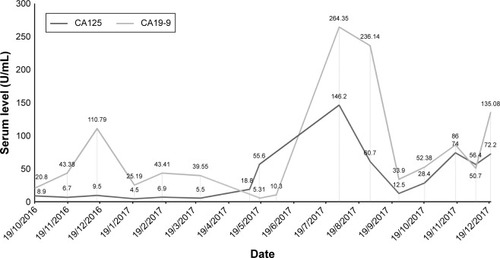
Figure 3 Pelvic MRI showing the right side pelvic cavity metastasis.
Abbreviation: MRI, magnetic resonance imaging.
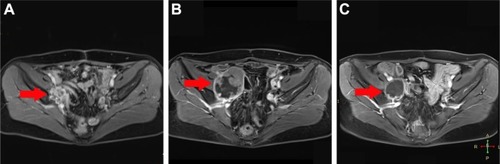
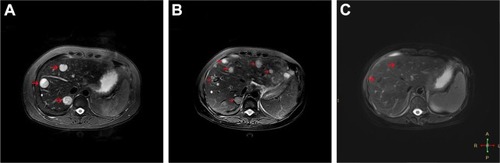
After her first relapse, the patient was treated with intravenous paclitaxel (135 mg/m2) and nedaplatin (80 mg/m2) as second-line chemotherapy. During the treatment, the patient’s serum CA19-9 level decreased to within the normal range. However, as with the first-line chemotherapy, after 2 cycles, her serum CA19-9 level was found to be increased to 43.41 U/mL, and pelvic MRI indicated that the mass in the right side of the pelvic cavity had increased in size since the previous report (). We recommended that the patient be administered the antiangiogenic therapy bevacizumab. She received 1 cycle of epirubicin (48 mg/m2), cyclophosphamide (4 mg/kg), and bevacizumab (15 mg/kg), which was discontinued because multiple new metastases were observed by liver MRI just a month later (). The patient then switched antiangiogenic therapies from bevacizumab to oral apatinib (500 mg/d) on April 6, 2017. However, apatinib treatment did not adequately control the disease, and the patient experienced grade 2 fatigue, hand–foot skin reaction, and proteinuria, which were not well managed. Her Eastern Cooperative Oncology Group performance status was 3. The patient stopped apatinib treatment after a month because of the side effects.
Figure 4 Liver MRI showing multiple metastases.
Abbreviation: MRI, magnetic resonance imaging.
The patient underwent whole-exome sequencing by gene capture, high-throughput sequencing, and real time quantitative polymerase chain reaction (RT-Q-PCR) in April 2017, which revealed moderate plasma expression of PD-L1 () and mutations in BRCA1 and BRCA2 at 7% and 5% frequency, respectively. This indicated that the patient might be sensitive to PD-1/PD-L1 and poly (ADP-ribose) polymerase (PARP) inhibitors. As the relevant medicines have not been approved on the Chinese mainland, the patient went to Hong Kong Integrated Oncology Centre to seek further therapy.
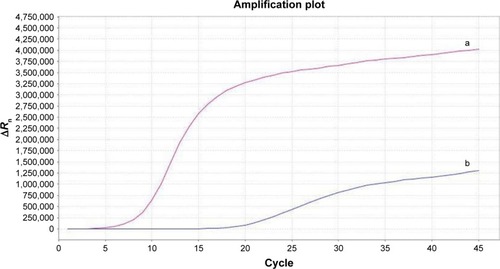
Figure 5 Moderate expression of PD-L1 detected by RT-Q-PCR.
Abbreviation: PD-L1, programmed death ligand 1; RT-Q-PCR, real time quantitative polymerase chain reaction.
In this medical institution, the patient was treated with olaparib (300 mg, bid) and pembrolizumab (100 mg, q21d) beginning May 9, 2017, and the dosage of olaparib was increased (350 mg, bid) a month and a half later. After 4 cycles, pelvic MRI showed that the mass in the right side of the pelvic cavity had been reduced approximately 65% ().
In the first cycle of this regimen, her serum CA19-9 level decreased to 5.31 U/mL. However, during following cycles, the patient’s serum CA19-9 and CA125 levels gradually increased to all-time highs of 264.35 and 146.2 U/mL, respectively. Liver MRI indicated an increased number of metastases and enlarged lymph nodes in the retroperitoneum and both the lesser and greater curvature of the stomach on August 2, 2017 (). The patient was then switched to nivolumab (160 mg, q14d) and pazopanib (600 mg, qd) for 8 cycles beginning August 7, 2017. The patient’s serum CA19-9 and CA125 level decreased sharply and returned to within the normal range in 2 months, followed by a slow increase (). After 6 cycles, liver MRI revealed that the metastases in the retroperitoneal lymph nodes and both the lesser and greater curvature of the stomach had shrunk (). During the treatment, the patient felt pain in the neck, and cervical MRI showed new metastases in the C4–C7 vertebral body and part of the adnexa. The 2 agents were administered until her serum CA19-9 and CA125 level increased remarkably again on November 17, 2017. On November 21, 2017, the doctors at the Hong Kong Integrated Oncology Centre administered a combination of nivolumab with nab-paclitaxel (270 mg, q14d). The patient has received 3 cycles of this regimen and has seen a decline in the serum level of the tumor markers. Since receiving immunotherapies, the patient has experienced pneumonia and intermittent moderate fever, which were controlled by antibiotics, and her Eastern Cooperative Oncology Group (ECOG) performance status was 1. Thus far, she has survived for more than 15 months. The patient provided written informed consent for the publication of the case details and the accompanying images.
Discussion and conclusion
Approximately 80% of ovarian cancer patients go into remission after standard initial multiple modality treatment, including primary debulking surgery followed by platinum chemotherapy.Citation2,Citation6 Platinum sensitivity is a major determinant of prognosis and, therefore, patients with platinum-refractory disease have poor prognosis. Platinum-refractory ovarian cancer patients have shorter progression-free survival and overall survival (OS) than progressive platinum-resistant patients with ovarian cancer.Citation7
Ovarian endometriosis can lead to squamous differentiation in endometrioid adenocarcinomas,Citation8 which are classified as adenosquamous carcinomas if they are malignant. Despite only part of the tumor consisting of malignant squamous cells, adenosquamous carcinoma was confirmed by immunohistochemical reevaluation in this case. Previous reports about ovarian adenosquamous carcinomas, almost all case reports, have been unable to determine prognosis of this type of malignant tumor. In the 5 cases where outcome was assessed, reported by Shoji et al,Citation9 the median OS was 12 months (range: 3–36 months), and 4 of the 5 patients with stage Ic disease showed recurrence and died within 13 months. Despite adverse prognostic factors, which were platinum-refractory and advanced-stage disease (stage IIa), the patient’s OS has exceeded 15 months in our case.
Tumor angiogenesis, mediated through VEGF and VEGF receptors, plays a pivotal role in the growth and metastasis of ovarian cancer.Citation10 Bevacizumab, a monoclonal anti-VEGF-A antibody targeting tumor angiogenesis, has been investigated and widely adopted for cancer treatment in both first-line and recurrent settings.Citation11 Apatinib is one of the latest oral small molecule tyrosine kinase inhibitors that inhibits VEGFR-2 and has encouraging preclinical and clinical data in the treatment of ovarian cancer.Citation12,Citation13 Pazopanib is also an oral small molecule tyrosine kinase inhibitor that inhibits VEGFR-1, -2, and -3. In a Phase III randomized clinical trial, pazopanib maintenance therapy provided a median improvement of 5.6 months (hazard ratio, 0.77) in progression-free survival in patients with advanced ovarian cancer who had not progressed after first-line chemotherapy.Citation14 We used bevacizumab and apatinib successively combined with chemotherapy, but there seemed to be little response in this patient. The exact effect of pazopanib in combination with nivolumab cannot be determined, although taking into account previous experience, we would be inclined to ascribe a greater effect to nivolumab. El Helali et alCitation15 demonstrated that acquired platinum resistance could be associated with an improved response to antiangiogenic agents; however, as far as we know, anti-angiogenesis-targeted platinum-refractory ovarian cancer remains to be investigated.
Olaparib is a PARP inhibitor approved by the US Food and Drug Administration (FDA) as monotherapy for ovarian cancer patients with germline BRCA mutations who have been treated with 3 or more prior lines of chemotherapy. This approval was primarily based on a clinical trial involving 193 patients with platinum-resistant epithelial ovarian cancer (relapse within 6 months of platinum therapy) rather than patients with platinum-refractory disease.Citation16 The efficacy of olaparib is associated with platinum sensitivity. Another indication from the European Medical Agency described platinum sensitivity as a condition and allowed olaparib monotherapy in patients with relapsed BRCA1/2-mutant epithelial ovarian, fallopian tube, or primary peritoneal cancers. In a cohort of 50 ovarian cancer patients with germline BRCA mutations who received olaparib, the clinical benefit rate was only 23% in patients with platinum-refractory disease, compared with 69% in platinum-sensitive patients.Citation17
PD-1, an immune checkpoint receptor expressed on T lymphocytes, is overexpressed in many types of human tumors in order to aid escape from the host immune system via PD-1/PD-L1 signaling. Nivolumab and pembrolizumab, anti-PD-1 monoclonal antibodies, block PD-1 signaling, and have been used to treat many tumors. Both nivolumab and pembrolizumab have been approved by the FDA for the treatment of metastatic melanoma.Citation18,Citation19 The FDA has also approved pembrolizumab as first-line therapy and beyond for patients with metastatic non-small-cell lung cancer whose tumors express PD-L1.Citation20 To the best of our knowledge, only a few Phase II trials of pembrolizumab in recurrent ovarian cancer are ongoing or completed, some of which focus on platinum-resistant cases.Citation21–Citation23 In a Phase II trial involving 20 nivolumab-treated patients with platinum-resistant ovarian cancer, the best overall response was 15%, and the disease control rate was 45%.Citation24 Sun et alCitation25 found that nivolumab increases the antitumor effects of cisplatin in platinum-resistant ovarian cancer cells by inducing apoptosis and cell-cycle arrest in cancer cells. A large amount of data about similar indications, efficacy, and toxicity of nivolumab and pembrolizumab indicate their interchangeability.Citation26 Because anti-PD-1 mAbs nonspecifically activate T-cells, immune-mediated damage of tissue or immune-related adverse events can occur.Citation27 Hypophysitis, colitis, hepatitis, pneumonitis, and rash are the most common adverse effects of combining immunotherapy with other therapies, but these are usually reversible. A meta-analysis demonstrated that patients treated with PD-1 inhibitors showed a significantly lower rate of grade 3–4 adverse effects than did patients receiving chemotherapy.Citation28 In our case, the patient’s performance status improved compared to her performance status during other therapies, and she did not experience toxicities generally observed during treatment with conventional antitumor chemotherapy. She did contract pneumonia, which was well managed.
Strickland et alCitation29 demonstrated that BRCA1/2-mutant ovarian cancers exhibit increased CD3+ and CD8+ TILs and increased PD-1/PD-L1 expression in the tumor microenvironment. Cross talk between PARP inhibitors and tumor-associated immunosuppression supports the combination of PARP inhibitors and PD-L1/PD-1 immune checkpoint blockade as a potential therapeutic approach.Citation30 The patient received benefit from the combined regimen after little response to platinum chemotherapy, non-platinum chemotherapy, and angiogenesis inhibitors, and she was facing rapid disease progression. However, this patient seemed to be progressively resistant to these drugs. Multiple resistance mechanisms against PARP inhibitors have been described, including somatic mutations in 53BP1, upregulation of drug efflux transporters such as PgP, and somatic mutations in BRCA genes leading to restoration of the open reading frame and thus BRCA function.Citation31 As far as we know, there is no report of resistance to PD-1/PD-L1 inhibitors.
There is no established chemotherapy regimen for ovarian adenosquamous carcinoma and no standard second-line and beyond chemotherapy regimen for platinum-refractory ovarian cancer. In our case, targeted therapies and immunotherapies were far superior to routine chemotherapy in controlling deterioration and improving performance status, leading to a prolongation of OS. We expect that more evidence of the efficacy and safety of single or combined regimens including targeted therapies and immunotherapies will be accumulated for rare categories of ovarian cancer in the future.
Data sharing statement
The data used in the case are available from the corresponding author on reasonable request.
Author contributions
AJL and SS drafted the manuscript. TS, XL, WC, RPY, and DYZ participated in collation of the clinical data. ZLC, JZ, DXZ, and CQY critically revised the paper. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (No 81603651). The authors thank the patient and her husband for their participation in this study and for the patients’ agreement to the publication of the report. We would like to thank Editage [www.editage.cn] for English language editing.
Disclosure
The authors report no conflicts of interests in this work.
References
- LeeJYNooSMChoNHA rare case of primary adenosquamous carcinoma arising from ovaryJ Women’s Med20103126129
- MorganRJJrArmstrongDKAlvarezRDOvarian cancer, version 1.2016: clinical practice guidelines in oncologyJ Natl Compr Canc Netw20161491134116327587625
- BookmanMAStandard treatment in advanced ovarian cancer in 2005: the state of the artInt J Gynecol Cancer200515Suppl 321222016343233
- OronskyBRayCMSpiraAITrepelJBCarterCACottrillHMA brief review of the management of platinum-resistant–platinum-refractory ovarian cancerMed Oncol201734610310928444622
- ZhangSRoyerRLiSFrequencies of BRCA1 and BRCA2 mutations among 1,342 unselected patients with invasive ovarian cancerGynecol Oncol2011121235335721324516
- JaysonGCKohnECKitchenerHCLedermannJAOvarian cancerLancet201438499511376138824767708
- SayalKGounarisIBasuBEpirubicin, cisplatin, and capecitabine for primary platinum-resistant or platinum-refractory epithelial ovarian cancer: results of a retrospective, single-institution studyInt J Gynecol Cancer201525697798425962114
- YuCQYuJHanJZhouQLShenWRegulatory mechanism of malignant behavior of endometriosis mediated by puerarinJ Chin Integr Med2009714347 Chinese
- ShojiTTakatoriEMurakamiKA case of ovarian adenosquamous carcinoma arising from endometrioid adenocarcinoma: a case report and systematic reviewJ Ovarian Res201691485427514842
- XuLZhouQLHanJEffects of Chinese herbal medicine Neiyi Recipe-medicated serum on angiopoiesis of endometriosis in the chick chorioallantoic membrane modelJ Chin Integr Med2012107800806
- McClungECWenhamRMProfile of bevacizumab in the treatment of platinum-resistant ovarian cancer: current perspectivesInt J Womens Health20168597527051317
- ZhangMTianZSunYSuccessful treatment of ovarian cancer with apatinib combined with chemotherapyMedicine (United States)201796454549
- DengLWangYLuWLiuQWuJJinJApatinib treatment combined with chemotherapy for advanced epithelial ovarian cancer: a case reportOnco Targets Ther2017101521152528352185
- du BoisAFloquetAKimJWIncorporation of pazopanib in maintenance therapy of ovarian cancerJ Clin Oncol201432303374338225225436
- El HelaliAMcCabeNDicksonNAcquired platinum resistance enhances tumour angiogenesis through activation of vascular mimicryCancer Res20177713152158
- KimGIsonGMcKeeAEFDA approval summary: olaparib monotherapy in patients with deleterious germline BRCA-mutated advanced ovarian cancer treated with three or more lines of chemotherapyClin Cancer Res201521194257426126187614
- McLachlanJBanerjeeSOlaparib for the treatment of epithelial ovarian cancerExpert Opin Pharmacother2016177995100326967466
- HazarikaMChukMKTheoretMRU.S. FDA approval summary: nivolumab for treatment of unresectable or metastatic melanoma following progression on ipilimumabClin Cancer Res201723143484348828087644
- BaroneAHazarikaMTheoretMRFDA approval summary: pembrolizumab for the treatment of patients with unresectable or metastatic melanomaClin Cancer Res201723195661566528179454
- Pai-ScherfLBlumenthalGMLiHFDA approval summary: pembrolizumab for treatment of metastatic non-small cell lung cancer: first-line therapy and beyondOncologist201722111392139928835513
- VargaAPiha-PaulSAOttPAPembrolizumab in patients (pts) with PD-L1-positive (PD-L1+) advanced ovarian cancer: updated analysis of KEYNOTE-028J Clin Oncol201735155513
- WenhamRMDormanDLeeJKApteSMShahzadMMChonHSPhase 2 trial of dose dense (weekly) paclitaxel with pembrolizumab in platinum resistant recurrent ovarian cancerInt J Gynecol Cancer201626877881
- MatulonisUAChenMPuhlmannMShentuYLedermannJKEYNOTE-100: phase 2 trial of pembrolizumab in patients with advanced recurrent ovarian cancerAnn Oncol201627Suppl 6296312
- HamanishiJMandaiMIkedaTSafety and antitumor activity of anti-PD-1 antibody, nivolumab, in patients with platinum-resistant ovarian cancerJ Clin Oncol201533344015402226351349
- SunLMLiuYCLiWNivolumab effectively inhibit platinum-resistant ovarian cancer cells via induction of cell apoptosis and inhibition of ADAM17 expressionEur Rev Med Pharmacol Sci20172161198120528387913
- PrasadVKaestnerVNivolumab and pembrolizumab: monoclonal antibodies against programmed cell death-1 (PD-1) that are interchangeableSemin Oncol201744213213528923211
- ZhuXLangJProgrammed death-1 pathway blockade produces a synergistic antitumor effect: combined application in ovarian cancerJ Gynecol Oncol2017285e6428657225
- GuanXWangHMaFQianHYiZXuBThe efficacy and safety of programmed cell death 1 and programmed cell death 1 ligand inhibitors for advanced melanoma: a meta-analysis of clinical trials following the PRISMA guidelinesMedicine (United States)20169511e3134
- StricklandKCHowittBEShuklaSAAssociation and prognostic significance of BRCA1/2-mutation status with neoantigen load, number of tumor-infiltrating lymphocytes and expression of PD-1/PD-L1 in high grade serous ovarian cancerOncotarget2016712135871359826871470
- JiaoSXiaWYamaguchiHPARP inhibitor upregulates PD-L1 expression and enhances cancer-associated immunosuppressionClin Cancer Res201723143711372028167507
- LimJSJTanDSPUnderstanding resistance mechanisms and expanding the therapeutic utility of PARP inhibitorsCancers201798109123