
Abstract
Aggressive fibromatosis (AF) is a rare benign tumor, which occurs in the deep part of bone and muscle fibrous tissue. Clinical and pathological features can be challenging for definitive diagnosis. Here, we report a rare case of a large AF in the axilla. Interestingly, 18 F-fluorodeoxyglucose-positron emission tomography/computed tomography showed significant increase in standard uptake value. Surgical resection yielded a spindle cell tumor likely of fibromatosis origin which was positive for β-catenin expression.
Introduction
Fibromatosis is a benign tumor caused by the proliferation of differentiated fibroblasts, and aggressive fibromatosis (AF) is a subtype of fibromatosis, also known as desmoid tumor or desmoid-type fibromatosis (DF), which is a monoclonal fibroblastic proliferative disease.Citation1 The disease occurs frequently in the abdomen and extremities but very rarely in the axillae. While metastatic spread is typically not seen, the disease often presents as a local infiltrating mass with significant compressive features. Despite lack of negative impact on survival, recurrence rates can be high. We encountered a rare case of large AF in axilla where immunohistochemical studies showed strong β-catenin expression. Interestingly, 18 F-fluorodeoxyglucose (FDG)-positron emission tomography/computed tomography (PET/CT) imaging showed significant uptake similar to that observed in malignant tumors.
Case report
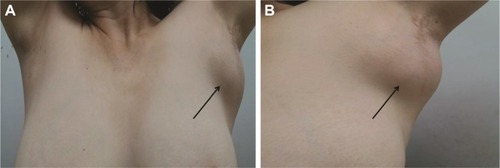
A 54-year-old female patient with no smoking or alcohol consumption history presented with a left axillary mass. She had undergone bilateral accessory breast resection 20 years earlier. This left axillary mass was first noted in 2012 but the patient declined treatment until December 2016. By then, the tumor had reached 10×8 cm2 limiting left upper arm motor function (). There was no pain or sensory complaints related to this large tumor.
Figure 1 Preoperative axillary photo of patient.
Ultrasound examination revealed two regular hypoechoic masses (5×3 mm2) in the left breast. Color doppler signal demonstrated absent blood flow. In addition, there was an irregular and inhomogeneous low echogenic mass in the subcutaneous soft tissue deep within the left axilla measuring 8 cm in longest diameter () with irregular borders and scant blood flow signal. Plain and contrast-enhanced magnetic resonance imaging (MRI) examination of breast revealed that a nodular and oval acoustic shadow with clear and smooth border in the upper inner quadrant of the left breast. In contrast, the mass within the left axilla revealed irregular borders and signal (). FDG-PET/CT showed that the saccharometabolism of the left axillary mass was inhomogeneous with increased standard uptake value (SUV) max value of 3.80. The lesion could not be easily separated from adjacent muscle including the musculi teres minor, the subscapalaris, and the scapula itself (). A core needle biopsy demonstrated fibrous tissue with glassy degeneration and focal vascular hyperplasia (). As these results precluded a definitive diagnosis, surgical excision was recommended and performed.
Figure 2 Imaging of ultrasound and MRI examination of breast.
Abbreviation: MRI, magnetic resonance imaging.
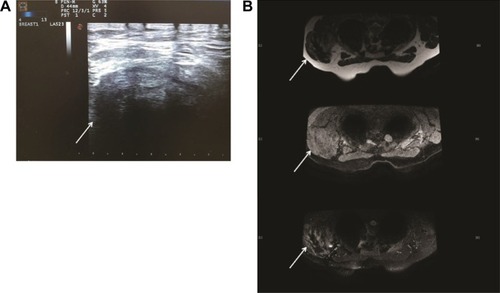
Figure 3 Imaging of 18 F-fluorodeoxyglucose (FDG) PET/CT.
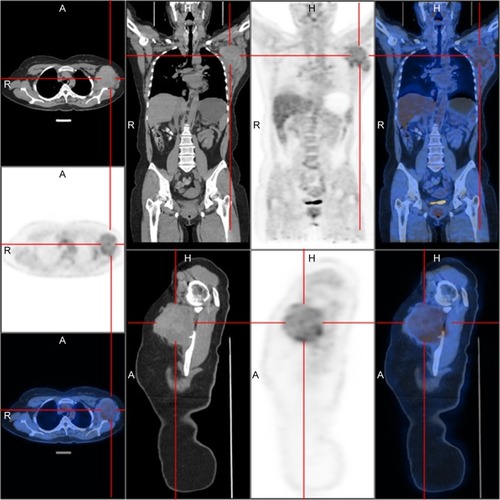
Figure 4 Image of core needle biopsy histologic diagnosis using hematoxylin and eosin staining (scale bar =2,000 μm; original ×100).

At the time of surgery, the mass was extremely hard with an incomplete capsule and could not be easily separated from surrounding tissues (). Indeed, adjacent structures were deformed and displaced because of the tumor’s mass effect which reached deep to the clavicle and invaded the surrounding tissues including: pectoralis major, brachial plexus, subscapalaris, latissimus dorsi, teres minor, and scapula. Intraoperative pathology result suggested a spindle cell tumor () which was confirmed on permanent paraffin sections with infiltration into striated muscle (). Tumorous tissue was negative for Bcl 2; and positive for β-catenin, smooth muscle actin, vimentin, and CD34 (). Based on these findings, the patient was diagnosed with a left axillary AF.
Figure 5 Intraoperative photo of the mass.
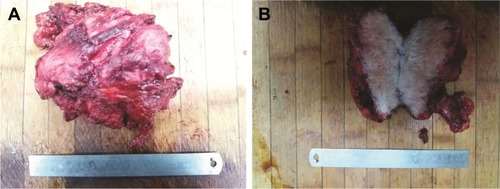
Figure 6 Image of paraffin pathology histologic diagnosis using hematoxylin and eosin staining (scale bar =2,000 μm; original ×100).
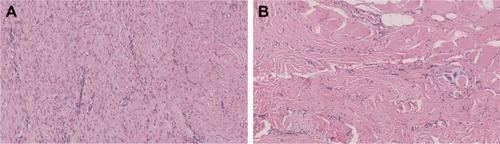
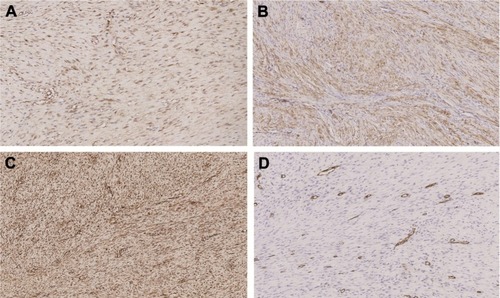
Figure 7 Expression of β-catenin, SMA, vimentin, and CD34 by IHC staining (scale bar =2,000 μm; original × 100).
Notes: (A) β-Catenin positive expression can be detected by IHC staining. (B) SMA positive expression can be detected by IHC staining. (D) CD34 positive expression can be detected by IHC staining.
After surgery, we asked for self- or family history of fibromatosis which were denied. The patient recovered soon without adjuvant medical or radiation therapy. After more than 1 year of follow-up, the patient remains in good condition, without cutaneous or muscle AF recurrence.
Discussion
AF is a subtype of fibromatosis, which refers to fibrous tissue tumors that occur in bones and muscles. AF is divided into superficial and deep types wherein the latter is also called desmoid tumors or DF representing a monoclonal cell proliferative disease.Citation1 DF is composed of spindle cells and collagen fibrils, which accounts for 0.03% of all tumors and about 3% of all soft tissue tumors.Citation2 DF is most frequently encountered in the abdomen, shoulders and limbs, and rarely in the axillae.Citation3,Citation4 Spindle cell tumors can occur in epithelial or mesenchymal tissues. There is no obvious effect on the survival rate of patients. However, the location of the DF can result in significant morbidities. These tumors often invade and compress surrounding tissuesCitation5 with a high recurrence rate.Citation2
Although there are some reports of AF, it is rare for them to develop in the axilla and reach to the deep side of the clavicle. The growth rate can be variable depending on the abundance of blood supply. In our case, we believe the rich axillary vasculature allowed the tumor to reach the 10.0×8.0×5.0 cm3 resulting in invasion of pectoralis major, latissimus dorsi, teres minor, scapula muscle, scapular nerve, and brachial plexus.
Unfortunately, the rarity of these tumors precludes clear diagnostic and treatment guidelines. At present, the first choice of management includes MRI and core needle biopsy examination. However, it is important to note that final diagnosis required permanent sections examination of surgically excised tissue.Citation6 In particular, immunohistochemistry (IHC) detection of β-catenin expression can be used as one feature supportive of the diagnosis of AF.Citation7–Citation9 More recently, FDG PET/CT has been widely applied for clinical staging. It should be emphasized, however, that the increased SUV values can be noted in both benign- and malignant-behaving tumors.Citation10 Some researchers defined malignancy based on the 2.5 times of threshold of SUV max.Citation11 In this regard, DF is similar to breast fibroadenomas where 18 F-FDG PET/CT thresholds cannot reliably distinguish benign from malignant diseases.Citation10
Surgical treatment is the preferred approach to the management of patients with suspected AF. It has been reported that radical surgery is the most important treatment to avoid disease recurrence.Citation2 Negative resection margins can ensure long-term remission. Nevertheless, the extent of surgical resection currently remains controversial.Citation12 In fact, more recent reports have advocated active surveillance as a reasonable management strategy. At the other end of the spectrum, chemotherapy and radiation can be considered in some unresectable or incompletely resected tumors.Citation13,Citation14 Additional studies reported that the location of DF affected the patient’s event-free survival (EFS) after the treatment.Citation14 In particular, disease involving the abdominal wall, abdominal cavity, breast, digestive viscera, and lower limbs appear to behave favorably. For these anatomical sites, the EFS was similar between surgical treatment and active surveillance. By comparison, unfavorable locations show significantly improved EFS for surgical treatment.Citation14 However, in the case presented here, the axillary location is considered to be one of the “unfavorable sites” due to complex and critical neural and vascular supplies. Moreover, the patient’s left upper arm was functionally affected by the extra-large size of the tumor providing more rationale for surgical intervention.
As indicated earlier, radiotherapy can also be an effective form of treatment for AF, especially for DF in the limbs.Citation15 Janssen et al found that with analysis of 1,295 cases, the risk of local recurrence following surgical resection was two times higher in the presence of positive margins. In such cases, postoperative adjuvant radiotherapy seems to reduce the risk of recurrence.Citation13 Although radiotherapy can lead to growth arrest, it can also be associated with side effects such as pain, limb edema, and skin toxicity.Citation16
In recent years chemotherapy and biologically targeted therapies have also received attention.Citation17 Park et al used combination chemotherapy of methotrexate and vinblastine for unresectable AF.Citation18 The results showed that half of patients presenting with pain experienced tumor size reduction. The most common adverse reaction was the anticipated liver enzyme elevation in nearly 80% of patients. Low-dose methotrexate and vincristine combination therapy was effective and well-tolerated.Citation18 It has been reported that non-steroidal anti-inflammatory drugs (NSAIDs), hormones and tyrosine kinase inhibitors (TKIs) were all feasible options for long-term control of AF. However, the mechanism underlying the efficacy of TKI remains unclear.Citation18 For NSAIDs, Pruksakorn et al completed successful steroid injections in eight patients with recurrent AF.Citation19
Conclusion
AF is a benign tumor with local infiltration and growth potential. In particular, β-catenin can be used as tissue biomarker for diagnosis and prognostic value. FDG PET/CT can also provide additional information to assist with surgical planning. Radiotherapy may have some beneficial effect by reducing the risk of recurrence in cases of incomplete resection. In contrast, the role of steroids, NSAIDs, and targeted therapies remains to be determined.
Acknowledgments
This study received approval from the ethics committee of The China Japan Union Hospital of Jilin University. The patient and family members also provided written informed consent to publish the case report details including photography.
Disclosure
The authors have no conflicts of interest in this work.
References
- FoaRRizzoSPetrellaFDe MariaFBellomiMRecurrent aggressive fibromatosis of the chest wallEcancermedicalscience2014846425368668
- HajjarWMAlShehriAFAlessaMAAl-NassarSALate presentation of aggressive fibromatosis involving head, neck and chest wallJ Coll Physicians Surg Pak2017271065465629056131
- LeeSHLeeHKSongJSJeongHSChest wall fibromatosis in the axillaArch Plast Surg201239217517722783521
- Martinez TruferoJPajares BernadITorres RamonIHernando CuberoJPazo CidRDesmoid-type fibromatosis: who, when, and how to treatCurr Treat Options Oncol20171852928439797
- SmithAJLewisJJMerchantNBLeungDHWoodruffJMBrennanMFSurgical management of intra-abdominal desmoid tumoursBr J Surg200087560861310792318
- ZhangYJGaoYSClinical features and surgical treatment of chest aggressive fibromatosisZhonghua Zhong Liu Za Zhi2016383232235 Chinese26988832
- YangSWangXJiangHWangYLiZLuHEffective treatment of aggressive fibromatosis with celecoxib guided by genetic testingCancer Biol Ther2017181075776028881160
- SkubitzKMBiology and treatment of aggressive fibromatosis or desmoid tumorMayo Clin Proc201792694796428578783
- SakaiTNishidaYHamadaSImmunohistochemical staining with non-phospho beta-catenin as a diagnostic and prognostic tool of COX-2 inhibitor therapy for patients with extra-peritoneal desmoid-type fibromatosisDiagn Pathol20171216628851389
- HofmanMSHicksRJHow we read oncologic FDG PET/CTCancer Imaging20161613527756360
- HainSFCurranKMBeggsADFogelmanIO’DohertyMJMaiseyMNFDG-PET as a “metabolic biopsy” tool in thoracic lesions with indeterminate biopsyEur J Nucl Med20012891336134011585292
- HaratiKJaenischABehrBEffect of surgical margins on prognosis in aggressive fibromatosis: a single-institutional analysis of 90 patientsOncol Lett20171455129513429113152
- JanssenMLvan BroekhovenDLCatesJMMeta-analysis of the influence of surgical margin and adjuvant radiotherapy on local recurrence after resection of sporadic desmoid-type fibromatosisBr J Surg2017104434735728199014
- PenelNLe CesneABonvalotSSurgical versus non-surgical approach in primary desmoid-type fibromatosis patients: a nationwide prospective cohort from the French Sarcoma GroupEur J Cancer20178312513128735069
- ZloteckiRAScarboroughMTMorrisCGExternal beam radiotherapy for primary and adjuvant management of aggressive fibromatosisInt J Radiat Oncol Biol Phys200254117718112182989
- ScheerLLodiMMoliereSKurtzJEMathelinCMedical treatment of mammary desmoid-type fibromatosis: which benefit?World J Surg Oncol20171518628420393
- PalassiniEFrezzaAMMarianiLLong-term efficacy of methotrexate plus vinblastine/vnorelbine in a large series of patients affected by desmoid-type fibromatosisCancer J2017232869128410293
- ParkKHChoiYJKimKWCombination chemotherapy with methotrexate and vinblastine for surgically unresectable, aggressive fibromatosisJpn J Clin Oncol201646984584927365524
- PruksakornDLorsomradeeSPhanphaisarnASafety and efficacy of intralesional steroid injection for aggressive fibromatosisWorld J Surg Oncol201715119529096658