
Abstract
Background
Tyrosine kinase with immunoglobulin and epidermal growth factor homology domains 2 (Tie2)-expressing monocytes (TEMs) are a highly proangiogenic subset of myeloid cells, which are characterized by expressing the angiopoietin receptor Tie2 with pro-tumor activity.
Purpose
The present study aimed to determine the clinical value of circulating TEMs (cTEMs) for cervical cancer.
Patients and Methods
Peripheral blood mononuclear cells (PBMCs) were obtained from 7 healthy volunteers, 17 uterine fibroid patients, 24 cervical intraepithelial neoplasia (CIN) II patients, 31 CIN III patients and 99 patients with cervical cancer. The cTEMs were evaluated by the ratio of Tie2+ CD14+ cells to all CD14+ monocytes in the PBMCs through flow cytometry. The diagnostic value of cTEM was assessed by receiver operating characteristic (ROC) curves and the correlation between cTEM and clinicopathological characters in cervical cancer patients was analyzed.
Results
The proportion of cTEMs was gradually increasing from healthy volunteers to patients with non-invasive lesions, then to cervical cancer patients. The area under the ROC curve was 0.913 when the level of cTEMs was used to distinguish cervical cancer from all the other women ranging from healthy volunteers to CIN III patients. In cervical cancer, an increased cTEM fraction was significantly correlated with advanced tumor stage, larger tumor size, lymph node metastasis (LNM), deep stromal infiltration, parametrial involvement and lymph-vascular space invasion and was an independent risk factor for LNM.
Conclusion
The cTEM proportion might be a promising biomarker for the malignant transformation of cervical lesions and the progression of cervical cancer.
Introduction
Cervical cancer is the fourth most common cancer among women worldwide with estimated 570,000 newly diagnosed cases and 311,000 deaths globally in 2018.Citation1 The incidence of cervical cancer in developed counties has been decreasing due to the widely applied screening program and the vaccination against human papillomavirus infection. However, cervical cancer is still a challenge in underdeveloped or developing countries and areas, where about 85% of the global burden of cervical cancer occurs.Citation2,Citation3 As we know, cervical cancer is associated high-risk human papillomavirus (HPV) infection. HPV DNA and oncogenes E6 and E7 are specific biomarkers for HPV-related cervical lesions and have been implicated in the screening for cervical cancer.Citation4 In addition, p16, p53 and ki67 signals in pap smear samples and cervix biopsy samples are helpful for the detection of high-grade precancerous lesions.Citation5 Cervical biopsy is an invasive procedure and should only be used in patients with suspicious high-grade cervical intraepithelial neoplasia (CIN) or invasive cancer. The pap smear sampling is less invasive, but the interval between two consecutive samplings should be at least 3 months to avoid false-negative results.Citation4 New biomarkers, especially those can be measured without invasive sampling, will be helpful for improving the diagnosis and management of this disease.
Angiogenesis is a hallmark of malignant tumors and an important target of therapy. It is known that tumor-infiltrating myeloid cells participate in angiogenesis and tumor progression. In 2005, De Palma et al reported a subpopulation of monocytes expressing the tyrosine kinase with immunoglobulin and epidermal growth factor homology domains 2 (Tie2).Citation6 Tie2 is the receptor for angiopoietins and the binding of Tie2 and angiopoietins conveys proangiogenic signals.Citation7 The Tie2-expressing monocytes (TEMs) have been identified as a subtype of tumor-associated macrophages (TAMs) that exhibit a remarkable pro-angiogenic function in tumor tissueCitation8,Citation9 and proposed as a candidate biomarker and a potential therapeutic target of diseases such as glioma, arthritis and thrombus recanalization.Citation10–Citation12 It has been found that the tumor-infiltrating TEMs were predominantly from circulating TEMs (cTEMs) rather than tissue-resident macrophages.Citation13 However, the clinical value of cTEMs in cervical cancer remains unclear.
In this study, we detected the percentage of cTEMs (Tie2+ CD14+) to monocytes (CD14+) in the peripheral blood from female healthy volunteers, patients with precancerous cervix disease and invasive cervical cancer, and evaluated the performance of cTEMs in screening and predicting progression of cervical cancer.Citation14
Patients and Methods
Ethics Statement
This non-interventional clinical investigation was conducted according to the principles expressed in the Declaration of Helsinki. The analysis of blood samples was approved by the Ethics Committee of Tongji Medical College, Huazhong University of Science and Technology (IORG0003571), and informed consent was obtained from all the patients and healthy volunteers.
Patients and Blood Samples
fBlood samples were collected from enrolled 7 healthy volunteers, 17 uterine fibroid patients, 24 CIN II patients, 31 CIN III patients and 99 cervical cancer patients between September 2017 and March 2018. The diagnoses of patients were pathologically confirmed and patients with squamous cell carcinoma or adenocarcinoma were included. Exclusion criteria: 1) chemotherapy or radiotherapy before surgery; 2) co-morbidities of other malignant diseases and conditions with abnormal hemopoietic function or immunity, such as autoimmune diseases, tuberculosis, HIV infection, undergoing chemotherapy or taking immunosuppressive drugs. The clinical stage of cervical cancer was determined according to the International Federation of Gynecology and Obstetrics (FIGO) 2009. Blood was obtained before the beginning of primary treatment. Healthy volunteers were apparently free of chronic and inflammatory diseases and gynecological ultrasound abnormal. Clinical, routine laboratory, histopathological and outcome data were retrieved from medical records after surgery.
Cytometric and Cell Sorting of cTEMs
Ethylenediamine tetra-acetic acid (EDTA) treated whole blood was processed at room temperature. Peripheral blood mononuclear cells (PBMCs) were isolated from 2 mL of the whole blood by Ficoll-Paque (TBD Science, Tianjin, China) density centrifugation. After single-cell suspensions prepared, they were incubated with the following antibodies for 30 min: CD14-APC (FAB3832A, R&D Systems, Inc.) and Tie2-PE (FAB3131P, R&D Systems, Inc.). Flow cytometry analysis and fluorescence-activated cell sorting (FACS) were immediately performed (MoFlo XDP, Beckman Coulter, USA). TEMs were identified by dual positive expression of CD14 and Tie2 (Tie2+ CD14+ cells), CD14+ for monocytes. The percentage of cTEMs was recorded, while the TEMs and Tie2-negative monocytes (TNegMs) were sorted cytometric (MoFlo XDP).
Cellular Immunofluorescence
The sorted cells were plated onto sterilized coverslips in 24-well plates (cat. no. 702,001; Wuxi NEST Biotechnology Co., Ltd.) in a humidified 37°C incubator (5% CO2) in Roswell Park Memorial Institute (RPMI) 1640 medium containing 10% fetal bovine serum (Gibco; Thermo Fisher Scientific, Inc.) and 1% penicillin-streptomycin. After incubation for 24 hours, the medium was carefully aspirated, and the coverslips were washed with PBS. The samples were then fixed in 4% paraformaldehyde for 30 min and followed by permeabilization with ice-cold acetone for 10 min. Subsequently, the cells were blocked in 10% BSA and incubated overnight at 4°C with antibodies against Tie2 (cat. no. AF313, 10ug/mL; R&D Systems) and CD14 (cat. no. ab181470, 1:1000 dilution; Abcam). Cy3-donkey anti-goat IgG (cat. no. SA00009-3, 1:100 dilution; Proteintech) and FITC-goat anti-mouse (cat. no. 172–1806, 1:200 dilution; Seracare) as the appropriate secondary antibodies were used. After counterstaining with DAPI (1:1000; Invitrogen; Thermo Fisher Scientific, Inc.), the cells were analyzed under a fluorescence microscope (IX73, Olympus Corporation).
Statistical Analysis
Statistical analyses were performed using SPSS software version 23 (SPSS Inc., Chicago, IL, USA). The percentages of cTEMs in different groups were compared using the Mann Whitney test. The Jonckheere–Terpstra test was used to evaluate the trend of cTEM percentage across groups of increasing severity of lesions. Receiver operating characteristic (ROC) curves were used to assess the diagnostic performance of cTEM and define the cut-off value for cervical cancer diagnosis. Univariate and multivariate binary logistic regression analysis were used to evaluate the risk for LNM in cervical cancer. All tests were two-sided, and P<0.05 are considered statistically significant.
Results
Percentage of cTEMs Increases in Cervical Cancer Patients
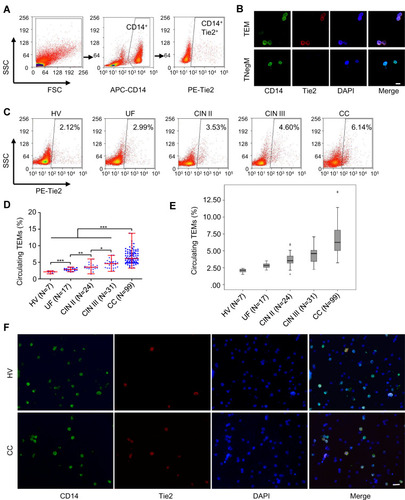
To determine whether the percentage of cTEMs increases in cervical cancer, we detected the cTEMs in all subjects. FACS was used to isolate TEMs and TNegMs from peripheral blood (). Cellular immunofluorescence assay was used to confirm the concomitant expression of Tie2 and CD14 in TEMs, while no expression of Tie2 in TNegMs (). Flow cytometry was used to evaluate the proportion of cTEMs to monocytes in the peripheral blood of 7 healthy volunteers, 17 uterine fibroid patients, 24 CIN II patients, 31 CIN III patients and 99 cervical cancer patients (). The percentage of cTEMs in cervical cancer patients (median, 6.14%; range, 3.23% −13.78%) was significantly higher than that in healthy volunteers (median, 2.12%; range, 1.53% −2.43%, P<0.001), uterine fibroid patients (median, 2.99%; range, 2.14% −3.53%; P<0.001), CIN II (median, 3.53%; range, 1.53% −6.00%; P<0.001) and CIN III patients (median, 4.60%; range, 2.25% −7.08%; P<0.001, ). Moreover, the increasing trend in the percentage of cTEMs with the increasing severity of cervical lesions was confirmed by the Jonckheere–Terpstra test (P<0.001, ). In PBMCs of healthy volunteers and cervical cancer patients, TEMs were detectable using immunofluorescence staining with CD14 and Tie2 antibodies ().
Figure 1 TEMs increased in peripheral blood of CC patients. (A) Detection of cTEMs in the peripheral blood (flow cytometric analysis). (B) Representative images of immunofluorescence assays for CD14 (green) and Tie2 (red) expression in TEMs and TNegMs which were isolated by FACS. Cell nuclei were labeled with DAPI (blue). Both CD14 (green) and Tie2 (red) were expressed in TEMs, while only CD14 (green) was expressed in TNegMs. Scale bar, 20 μm. (C) The percentage of cTEMs (Tie+CD14+) in total CD14+ monocytes was detected in peripheral blood of 7 HV, 17 UF, 24 CIN II, 31 CIN III and 99 CC patients. (D) The percentage of cTEMs is significantly increased in CC patients (Mann–Whitney u-test). *P<0.05, ** P<0.01 and *** P<0.001. (E) Boxplot of the Jonckheere–Terpstra test for the trend of percentage of cTEMs changing with the severity of cervical lesions. P<0.001. (F) Representative images of immunofluorescence assays for CD14 (green) and Tie2 (red) expression in PBMCs of HV and CC patient. Cell nuclei were labeled with DAPI (blue). Scale bar, 20 μm.
The Clinical Value of Percentage of cTEMs in Diagnosing Cervical Lesions
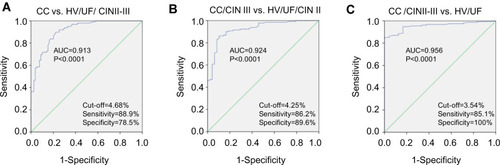
To determine the diagnostic value of percentage of cTEMs in cervical lesions, we performed receiver operating characteristic (ROC) curve analyses. For cervical cancer patients and non-cervical cancer patients, the optimal cut-off value of the percentage of cTEMs was 4.68%, with a sensitivity of 88.9% and a specificity of 78.5%. The area under the curve (AUC) was 0.913 (95% CI, 0.872 to 0.953; P<0.0001; ). The cut-off value at 4.25% yielded the best sensitivity (86.2%) and specificity (89.6%) for differentiating CIN III and cervical cancer patients from healthy volunteers, uterine fibroid patients and CIN II patients. And the AUC was 0.924 (95% CI, 0.882 to 0.966; P<0.0001; ). The ROC curve also showed that the optimal cut-off value of the percentage of cTEMs was 3.54% for differentiating CIN II, CIN III and cervical cancer patients from healthy volunteers and uterine fibroid patients. The diagnostic sensitivity and specificity were 85.1% and 100%, respectively, with an AUC of 0.956 (95% CI, 0.927 to 0.985; P<0.0001; ).
Figure 2 The diagnostic value of cTEM for cervical lesions. ROC analyses were performed in order to assess the diagnostic value of percentage of cTEMs for differentiating non-CC (HV, UF and CIN patients) from CC patients (A), HV, UF and CIN II from CIN III and CC patients (B), and for differentiating HV and UF from CIN and CC patients (C).
Percentage of cTEMs is Correlated with Cervical Cancer Progression
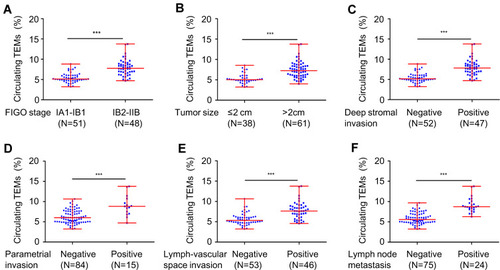
In order to evaluate whether the cTEMs frequency was correlated with the clinicopathological features of cervical cancer, we performed Mann–Whitney u-test (). Percentage of cTEMs was positively correlated with FIGO stage (P<0.001, ), tumor size (P<0.001, ), deep stromal invasion (P<0.001, ), parametrial invasion (P<0.001, ), lymph-vascular space invasion (P<0.001, ) and LNM (P<0.001, ). However, there were no significant correlations between cTEMs and age, histological type, or histologic grade ().
Table 1 The Relation of Circulating TEMs to Clinical-Pathological Parameters in Cervical Cancer
Figure 3 Percentage of cTEMs is correlated with CC progression. High level of cTEMs were significantly associated with FIGO stage (A), tumor size (B), deep stromal invasion (C), parametrial invasion (D), lymph-vascular space invasion (E) and LNM (F). ***P<0.001.
Percentage of cTEMs is a Predictor for Lymph Node Metastasis of Cervical Cancer
To assess the relationship between cTEMs and LNM, we performed univariate analysis and multivariate analysis of LNM in patients with cervical cancer (). Univariate analysis revealed FIGO stage (OR, 7.82; 95% CI, 2.26–23.52), deep stromal invasion (OR, 5.83; 95% CI, 1.96–17.42), lymph-vascular space invasion (OR, 8.62; 95% CI, 2.66–27.95), tumor size (OR, 8.50; 95% CI, 1.86–38.84), parametrial invasion (OR, 10.92; 95% CI, 3.21–37.21) and the percentage of cTEMs (OR, 20.00; 95% CI, 5.34–74.86) as risk factors for cervical cancer LNM. Multivariate analysis showed that parametrial invasion (OR, 5.94; 95% CI, 1.19–29.58) and percentage of cTEMs (OR, 6.25; 95% CI, 1.18–33.00) are independent risk factors in cervical cancer LNM prediction.
Table 2 Univariate Analysis and Multivariate Analysis of Lymph Node Metastasis in Patients with Cervical Cancer (N=99)
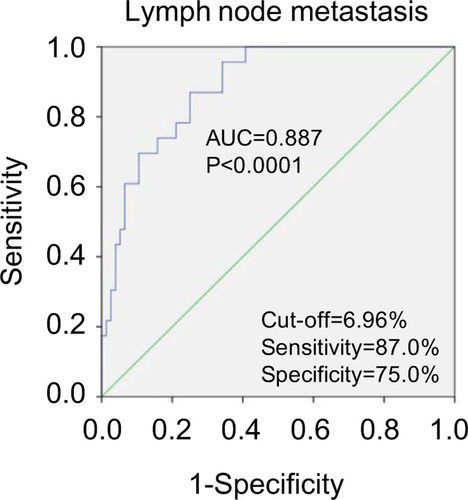
ROC analysis was further performed to assess the value of the percentage of cTEMs in predicting LNM. The optimal cut-off value of the percentage of cTEMs was 6.96%. The sensitivity and specificity were 87.0% and 75.0%, respectively, with the AUC of 0.887 (95% CI, 0.820–0.953, ).
Figure 4 Percentage of cTEMs is an independent predictor of CC LNM.
Discussion
Our current study demonstrated the clinical significance of cTEMs in cervical cancer patients and the main findings include 1) the percentage of cTEMs in cervical cancer patients was significantly higher than in healthy volunteers, uterine fibroid patients, CIN II and CIN III patients; 2) increased percentage of cTEMs may represent as a potential diagnostic marker; 3) the percentage of cTEMs was significantly associated with FIGO stage, tumor size, deep stromal invasion, parametrial invasion, lymph-vascular space invasion and LNM; 4) the percentage of cTEMs was a predictor for LNM of cervical cancer. These results may indicate that cTEMs is a promising biomarker with potential value in screening and prognosis prediction for cervical cancer and real-time monitoring of disease progression.
The presence of TEMs has already been reported in many solid cancers such as colorectal cancer, pancreatic cancer, renal cancer and hepatocellular cancer.Citation13–Citation15 Recently, TEMs have been proposed as a candidate biomarker and a therapeutic target in the treatment of malignancy.Citation16–Citation18 Increased TEMs in peripheral blood and liver are considered as novel diagnostic markers for hepatocellular carcinoma.Citation19 However, whether the frequency of TEMs in cervical cancer patients differing from the normal range and correlated with clinical parameters have not been assessed yet.
In our current research, individual percentage of cTEMs in the peripheral blood samples was in the range reported previously.Citation13 And we confirmed TEMs were existed and increased in the peripheral blood of cervical cancer patients. It has been reported that the frequencies of TEMs in the peripheral blood of healthy individuals and colorectal cancer patients did not differ significantly, and the functional differences of TEMs between colorectal cancer patients and healthy individuals may be contributed by the upregulation of Tie2 expressed in TEMs in cancer patients.Citation20 However, we found that increased cTEMs was a common feature of cervical cancer patients, and may represent a potential biomarker. To determine the specificity of cTEM as a cervical cancer biomarker, control cohorts of healthy volunteers, women with uterine fibroid and women with cervical precancerous lesions were set up in the present study. Although the histological origins of uterine fibroid differ from cervical cancer, it is necessary to exclude the impact of this most common benign tumor in women on the percentage of cTEM that can potentially affect the biomarker performance in cervical cancer patients. Although cTEMs alone is insufficient for a diagnosis of cervical cancer, it is a possible biomarker to indicate the presence or progression of disease with benefits of non-invasive sampling, allowing real-time monitoring of disease evolution.
TEMs have been shown to promote the formation of tumor blood vessels and lead to neoplastic growth.Citation19 Associations between cTEMs and the clinical features have been reported. Matsubara et alCitation21 showed that TEMs in peripheral blood was significantly associated with a deterioration of liver function and poor prognosis in hepatocellular cancer patients, and Atanasov et alCitation17 reported that cTEMs affect outcomes in cholangiocarcinoma. Collectively, cTEMs may serve as a prognostic marker in various types of cancer. In support of this, we found that cTEMs were significantly positively associated with FIGO stage, tumor size, invasion of deep stromal, lymph-vascular space and LNM in cervical cancer.
Lymph node status remains the most important prognostic factor and major determinant of treatment in patients with early cervical cancer.Citation22 Our previous researchCitation23 and Guani et alCitation24 have demonstrated that the LNM is positively correlated with larger tumor size, deeper stromal invasion, parametrial invasion and lymph-vascular space invasion. Except for tumor size, all these risk factors cannot be measured before surgery. In usual, CT and MRI are used to evaluate the para-aortic LNM in cervical cancer. However, it is difficult for imaging techniques to distinguish metastatic lymph nodes from inflammation or infection, and the sensitivity of computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET) is only 57%, 54% and 66%, respectively.Citation25 In our study, we found that the percentage of cTEMs was an independent predictor for LNM. This could be a compensatory marker with the imaging techniques, to assess the possibility of LNM better.
There are several limitations in the present study. Detection of peripheral blood mononuclear cells has shortcomings of stability and repeatability, partially because of the differences in the absolute number of monocytes between individuals. So, in the present study, we used the ratio of cTEMs to monocytes but not the absolute number of TEMs as a biomarker. Moreover, the retrospective study design and relatively small sample size may cause biases in results. A multi-center, large-sample prospective study is needed to further validate the value of the percentage of cTEM as a biomarker for cervical cancer.
In summary, this study exhibited that cTEMs were significantly increasing in cervical cancer patients, and it may be expected to be a promising biomarker for diagnosis and predicting progression of cervical cancer.
Abbreviations
TEMs, Tie2-expressing monocytes; cTEMs, circulating TEMs; TNegMs, Tie2-negative monocytes; PBMCs, peripheral blood mononuclear cells; TAMs, tumor-associated macrophages; Ang-2, angiopoietin-2; FIGO, International Federation of Gynecology and Obstetrics; LNM, lymph node metastasis; ROC, receiver operating characteristic; AUC, area under the curve; OR, odds ratio; CI, confidence interval; CC, cervical cancer; CIN, cervical intraepithelial neoplasia.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant no. 81572572 and 81772781). Qing Han and Quan Zhang are co-first authors for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.2149230207593
- Lewis DR, Chen HS, Cockburn MG, et al. Early estimates of cancer incidence for 2015: expanding to include estimates for white and black races. Cancer. 2018;124(10):2192–2204. doi:10.1002/cncr.3131529509274
- Wang J, Bai Z, Wang Z, Yu C. Comparison of secular trends in cervical cancer mortality in China and the United States: an age-period-cohort analysis. Int J Environ Res Public Health. 2016;13(11):1148. doi:10.3390/ijerph13111148
- ASCCP. 2019 ASCCP risk-based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors. Available from: http://www.asccp.org. Accessed 717, 2020.
- Curry SJ, Krist AH, Owens DK, et al. Screening for cervical cancer: us preventive services task force recommendation statement. JAMA. 2018;320(7):674–686. doi:10.1001/jama.2018.1089730140884
- De Palma M, Venneri MA, Galli R, et al. Tie2 identifies a hematopoietic lineage of proangiogenic monocytes required for tumor vessel formation and a mesenchymal population of pericyte progenitors. Cancer Cell. 2005;8(3):211–226. doi:10.1016/j.ccr.2005.08.00216169466
- Zhang L, Qi Y, Min H, et al. Cooperatively responsive peptide nanotherapeutic that regulates angiopoietin receptor Tie2 activity in tumor microenvironment to prevent breast tumor relapse after chemotherapy. ACS Nano. 2019;13(5):5091–5102. doi:10.1021/acsnano.8b0814230986342
- Coffelt SB, Tal AO, Scholz A, et al. Angiopoietin-2 regulates gene expression in TIE2-expressing monocytes and augments their inherent proangiogenic functions. Cancer Res. 2010;70(13):5270–5280. doi:10.1158/0008-5472.CAN-10-001220530679
- Huang H, Lai JY, Do J, et al. Specifically targeting angiopoietin-2 inhibits angiogenesis, Tie2-expressing monocyte infiltration, and tumor growth. Clin Cancer Res. 2011;17(5):1001–1011. doi:10.1158/1078-0432.CCR-10-231721233403
- De Palma M, Murdoch C, Venneri MA, Naldini L, Lewis CE. Tie2-expressing monocytes: regulation of tumor angiogenesis and therapeutic implications. Trends Immunol. 2007;28(12):519–524. doi:10.1016/j.it.2007.09.00417981504
- Lewis CE, De Palma M, Naldini L. Tie2-expressing monocytes and tumor angiogenesis: regulation by hypoxia and angiopoietin-2. Cancer Res. 2007;67(18):8429–8432. doi:10.1158/0008-5472.CAN-07-168417875679
- De Palma M, Naldini L. Tie2-expressing monocytes (TEMs): novel targets and vehicles of anticancer therapy? Biochim Biophys Acta. 2009;1796(1):5–10. doi:10.1016/j.bbcan.2009.04.00119362584
- Venneri MA, De Palma M, Ponzoni M, et al. Identification of proangiogenic TIE2-expressing monocytes (TEMs) in human peripheral blood and cancer. Blood. 2007;109(12):5276–5285. doi:10.1182/blood-2006-10-05350417327411
- Germano D, Daniele B. TIE2-expressing monocytes as a diagnostic marker for hepatocellular carcinoma correlates with angiogenesis. Hepatobiliary Surg Nutr. 2014;3(4):166–167. doi:10.3978/j.issn.2304-3881.2014.06.0425202690
- He YF, Wang CQ, Yu Y, et al. Tie2-expressing monocytes are associated with identification and prognoses of hepatitis B virus related hepatocellular carcinoma after resection. PLoS One. 2015;10(11):e0143657. doi:10.1371/journal.pone.014365726599011
- Atanasov G, Dino K, Schierle K, et al. Recipient hepatic tumor-associated immunologic infiltrates predict outcomes after liver transplantation for hepatocellular carcinoma. Ann Transplant. 2020;25:e919414. doi:10.12659/AOT.91941432165607
- Atanasov G, Dietel C, Feldbrugge L, et al. Angiogenic miRNAs, the angiopoietin axis and related TIE2-expressing monocytes affect outcomes in cholangiocarcinoma. Oncotarget. 2018;9(52):29921–29933. doi:10.18632/oncotarget.2569930042823
- Atanasov G, Potner C, Aust G, et al. TIE2-expressing monocytes and M2-polarized macrophages impact survival and correlate with angiogenesis in adenocarcinoma of the pancreas. Oncotarget. 2018;9(51):29715–29726. doi:10.18632/oncotarget.2569030038715
- Atanasov G, Dino K, Schierle K, et al. Angiogenic inflammation and formation of necrosis in the tumor microenvironment influence patient survival after radical surgery for de novo hepatocellular carcinoma in non-cirrhosis. World J Surg Oncol. 2019;17(1):217. doi:10.1186/s12957-019-1756-831830991
- Goede V, Coutelle O, Shimabukuro-Vornhagen A, et al. Analysis of Tie2-expressing monocytes (TEM) in patients with colorectal cancer. Cancer Invest. 2012;30(3):225–230. doi:10.3109/07357907.2011.63611422171993
- Matsubara T, Kanto T, Kuroda S, et al. TIE2-expressing monocytes as a diagnostic marker for hepatocellular carcinoma correlates with angiogenesis. Hepatology. 2013;57(4):1416–1425. doi:10.1002/hep.2596522815256
- Chen CS, Ou YC, Lin H, et al. Analysis of prognostic factors and clinical outcomes in uterine cervical carcinoma with isolated para-aortic lymph node recurrence. Am J Transl Res. 2019;11(12):7492–7502.31934296
- Li D, Cai J, Kuang Y, Cao J, Wang Z. Surgical-pathologic risk factors of pelvic lymph node metastasis in stage Ib1-IIb cervical cancer. Acta Obstet Gynecol Scand. 2012;91(7):802–809. doi:10.1111/j.1600-0412.2012.01415.x22486458
- Guani B, Balaya V, Magaud L, Lecuru F, Mathevet P. The clinical impact of low-volume lymph nodal metastases in early-stage cervical cancer: the senticol 1 and senticol 2 trials. Cancers. 2020;12(5):1061. doi:10.3390/cancers12051061
- Liu B, Gao S, Li S. A comprehensive comparison of CT, MRI, positron emission tomography or positron emission tomography/CT, and diffusion weighted imaging-MRI for detecting the lymph nodes metastases in patients with cervical cancer: a meta-analysis based on 67 studies. Gynecol Obstet Invest. 2017;82(3):209–222. doi:10.1159/00045600628183074