Abstract
We report the case of a 64-year-old woman with a gastrointestinal stromal tumor and a diffuse large cell lymphoma. For this case, we conducted a literature review in an attempt to correlate these two neoplasms on a molecular basis. Diffuse large cell lymphoma is a subtype of non-Hodgkin lymphomas. The etiologic factor of these lymphomas is considered to be the mutations or allelic losses of the TP53 tumor suppressor gene and the overexpression of the bcl-2 oncogene. Gastrointestinal stromal tumors are mesenchymal tumors, which are typically defined by the expression of c-KIT (CD117) and CD34 genes in the tumor cells. Although there are references to dispersants in the literature about patients with both non-Hodgkin lymphoma and gastrointestinal stromal tumors, there is no common molecular pathway between these two diseases. In conclusion, there is no indication that these two neoplasms are relevant on a molecular basis.
Introduction
A diffuse large-cell lymphoma (DLCL) of B-cell origin is a lymphoid neoplasm with diverse clinical manifestations. These neoplasms present as masses and grow rapidly, and cause symptoms when they infiltrate tissues or obstruct organs. These neoplasms can present either with B symptoms (fever, drenching night sweats, and weight loss) or pain when the lymphomatous mass enlarges rapidly.Citation1 Gastrointestinal stromal tumors (GISTs) are relatively rare mesenchymal neoplasms of the gastrointestinal tract. GISTs develop from the Cajal cells and are the most common mesenchymal tumors of the gastrointestinal tract. They usually occur in the upper gastrointestinal tract, in areas such as the stomach; GISTs of the small bowel, esophagus, and rectum are less common.Citation2 We report the case of a 64-year-old woman with a GIST and a DLCL. In this case, we conducted a literature review in an attempt to correlate these two neoplasms on a molecular basis.
Case presentation
A 64-year-old Caucasian female presented to the hospital with symptoms of infectious lung disease and weakness, with a medical history of rheumatoid arthritis, diabetes mellitus, and hypertension. She was accepted to the pulmonary department, where she was treated. During her treatment there, she was transfused with four units of packed red blood cells, and the computer tomography of her thorax revealed pathological lymph nodes of the mediastinum. Consequently, the patient was referred to the hematological department of our hospital with symptoms of fever starting 4 months before, drenching night sweats, weakness, and lung infection. She claimed a fever duration of 15 days, with three fever waves daily and a maximum body temperature of 40°C, followed by 10 days without fever. The physical examination revealed bulky axillary lymph nodes, and a biopsy of the left cervical lymph node was taken. The biopsy was positive for DLCL, including mediastinum B-cell lymphoma. The immunohistochemistry was CD20+, PAX-5+, CD79α+, CD30+, MUM1+, OCT-2+, LMP-1+, p53+, BCL2++/−, cyclin D1––/+, CD45RA−, CD45−, CD45RO−, CD3−, CD5−, CD4−, CD8−, CD10−, BCL6−, AKL-1−, and EMA-. The patient’s hematological check showed 32% hematocrit, 10.6 hemoglobin, 90 mean corpuscular volume, and 29 mean corpuscular hemoglobin after transfusion. Anisocytosis and hypochromia were also found, as well as rouleaux formation. The blood count revealed 6800 white blood cells and 200,000 platelets. The biochemical analysis showed elevated uric acid, aspartate transaminase, and alanine transaminase levels. Her beta-2 microglobulin was 8.00 mg/L. Afterwards, a whole-body Gallium 67 scan and a computed tomography (CT) scan of her upper abdomen, lower abdomen, and retroperitoneal area were performed in order to define the stage of the disease. The stage was determined to be IIB, and the patient was started on a chemotherapy regiment of cyclophosphamide, hydroxydaunorubicin, vincristin, prednisolone, and rituximab. Nine circles of rituximab followed. After the ninth circle of chemotherapy, the patient was urged to have a thorax, upper abdomen, lower abdomen, and retroperitoneal area CT as part of her follow-up treatment.
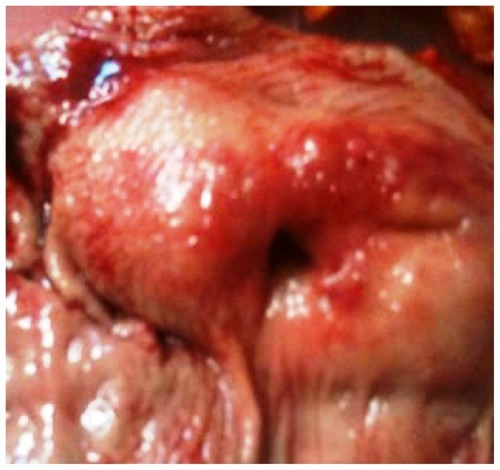
The CT scan revealed a well-demarcated spherical mass that arose from the muscularis propria layer of the stomach in the level of the pylori, with overlying mucosal ulceration (). The radiological image was compatible with that of a GIST, and the patient was accepted to the surgical department of our hospital. The patient complained of abdominal pain and discomfort, as well as belching. She was submitted for an esophagogastroduodenoscopy (EGD) and endoscopic ultrasonography. The EGD showed a polypoid mass with a 3-cm diameter, with ulceration on the mass located in the pyloric antrum, findings indicating a possible GIST (). A tumor resection was decided upon and the patient was submitted for subtotal gastrectomy with Billroth II reattachment. The surgical specimen () was sent for histological examination. The histological examination confirmed the GIST diagnosis and the immunohistochemistry showed that the tumor was CD117+, CD34+, and focally positive for NSE and GFAP antigens. Additionally, it was negative for the α-SMA, myosin, desmin, S-100, CD3, and CD20 antigens. The tumor was fully resected and the lymph nodes were not infiltrated.
Figure 1 Computed tomography of the upper abdomen.
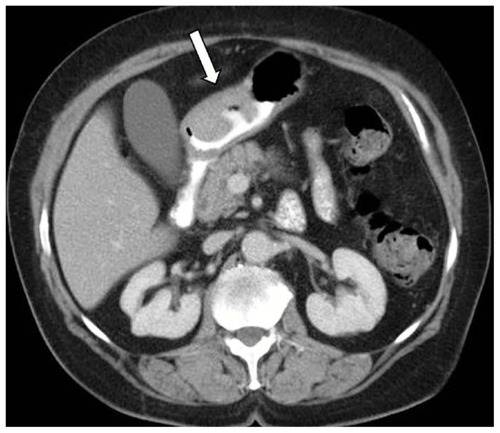
Figure 2 Esophagogastroduodenoscopy of the tumor in the gastric antrum.
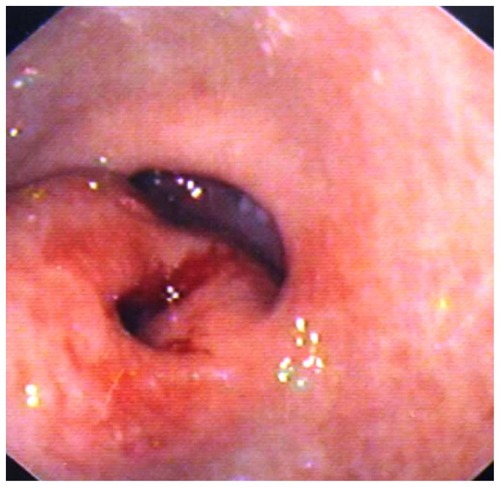
Figure 3 Gastrointestinal stromal tumor surgical specimen.
The 6-month follow-up included a thorax, upper abdomen, lower abdomen, and retroperitoneum area CT scan, as well as an EGD. The CT scans revealed a mild splenomegaly, while the other findings were normal. The endoscopy had no pathological findings.
Discussion
DLCL is a subtype of non-Hodgkin lymphomas. DLCLs represent a diverse spectrum of lymphoid neoplasms with variable clinical, histologic, immunophenotypic, cytogenetic, molecular, and genetic features,Citation3 and they are of B-cell origin. According to the literature, B-cell-restricted markers (CD19, CD20, CD22) are expressed in the majority of DLCLs. The most common activation antigens are expressed through the HLA-DR system. In contrast to the markers mentioned above, CD23 is less frequently expressed (0%–25%). The etiologic factor of these lymphomas is considered to be the mutations or allelic losses of the TP53 tumor suppressor gene (17p13.1). These changes are considered to be relevant with the evolution of these neoplasms.Citation4,Citation5 Another gene, the bcl-2 oncogene, is overexpressed in DLCLs.Citation6–Citation8 The bcl-2 is an important protein in the apoptotic pathway and is considered to have a critical role in drug resistance. The Bcl-2 protein is present in normal tissues, as well as in neoplastic ones, and high levels of this protein offer a survival advantage in B-cells by inhibiting apoptosis.Citation6–Citation8
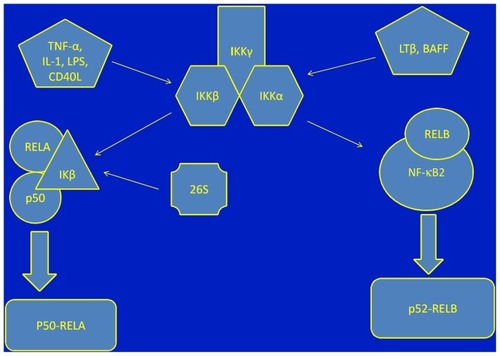
Mediastinal B-cell lymphoma is a recently identified subtype of diffuse large B-cell lymphoma.Citation9,Citation10 The pathogenesis of mediastinal B-cell lymphoma includes the activation of NF-κB pathways and the JAK2 genes.Citation11,Citation12 The NF-κB signaling pathway controls the cell death regulatory genes, resulting in the control of B-cell survival.Citation13,Citation14 There is a simultaneous decrease in the JAK signaling pathway.Citation15,Citation16 The two pathways mentioned above are a result of the increased expression of IL-13.Citation17 The signal transducer and activator of transcription-1, tumor necrosis factor, and tumor necrosis factor receptor-associated factor are increased.Citation16 Additionally, there is a nuclear translocation of the c-REL proteinCitation13,Citation18,Citation19 (). GISTs are mesenchymal tumors originating from the pluripotential mesenchymal stem cell, which is programmed to differentiate into the interstitial Cajal cell.Citation2 GISTs are typically defined by the expression of c-KIT (CD117) and CD34 in the tumor cells.Citation20 The c-KIT oncogene is located in chromosome 4.Citation21 The expression of CD117 is present in 85%–95% of GISTs. The remaining 3%–5% of c-KIT-negative GISTs is positive for PDGFRα mutations and PDGFRα mutations, and there is a small percentage of wild-type c-KIT mutations.Citation22,Citation23 The mutations in oncogenic KIT genes are present in exons 9, 11, 13, and 17.Citation24,Citation25 The mutations in exon 11 are most commonly deletions and substitutions, whereas duplications and insertions are less common. The locus of the mutation is codon 558 in 5′KIT.Citation26 As far as PDFGRα is concerned, there are mutations located in exons 12, 14, and 18. Both c-KIT and PDGRFα expression provoke a tyrosine kinase pathway in the cell.Citation27 The activation of this signaling system results in uncontrolled phosphorylation and tissue growth.Citation28 Because of the fact that 5%–15% of GISTs lack these mutations, scientists believe that there is an additional pathway that has not yet been discovered.Citation28
Figure 4 NF-κB activation pathways.
GISTs are malignant neoplasms, and this fact makes the tumor prognostic factors extremely important. The most important prognostic factors are sizes greater than 5 cm, mitotic activity (mitotic counts greater than one to five per ten high-powered fields), diffuse moderate atypia, and coagulation necrosis.Citation29,Citation30 The c-KIT oncogene was recently added to these mutation criteria ().
Table 1 Gastrointestinal stromal tumor staging systemCitation29
Although there have been impressive advances in targeted therapy, surgery resection with preservation of the pseudocapsule remains the primary mode of therapy for localized GISTs.Citation31 Surgical resection can be laparoscopic or even endoscopic in cases of patients who cannot be treated with an open surgery.Citation32,Citation33 Surgery is used in three main situations: as an initial treatment (primary surgery) after diagnosis, especially in solitary tumors, which can be easily removed; after neoadjuvant treatment in order to reduce the size of the neoplasm; and, occasionally, for symptomatic relief in advanced metastatic disease, known as debulking surgery.Citation31 It is considered very important that these tumors should be handled carefully in order to avoid tumor rupture and spread. Lymphadenectomy is not routinely recommended since GISTs rarely metastasize to the lymph nodes. Additionally, GISTs have poor response to conventional chemotherapy and radiation therapy.Citation31,Citation34
The last decade has seen significant progress in targeted therapy. Since Hirota et alCitation20,Citation35 discovered the role of c-KIT in GISTs, scientists have managed to find agents that block the molecular pathway of the oncogene proteins. In fact, scientists used imatinib and sunitinib maleate, the ATP binding agents of BCRABL, in the therapy of metastatic GISTs with very encouraging results.Citation28,Citation31,Citation36,Citation37 Those drugs bind and stabilize the inactivated form of the receptor tyrosine kinases, which leads to the inhibition of phosphorylation and downstream KIT-signaling activation.Citation28,Citation31,Citation36 Imatinib binds to a specific amino acid residue within the ATP binding pocket and in the activation loop,Citation31 whereas sunitinib interacts with different amino acids within the ATP binding pocket.Citation31 Additionally, disease progression is considered to be a result of c-KIT mutations in exons 13, 14, and 17, which decrease the tumor sensitivity to imatinib and additional chemotherapy.Citation28
Although there are reports of dispersants in the literature of patients with coexisting non-Hodgkin lymphoma and GISTs, there is nothing to the authors’ knowledge indicating that there is a common molecular pathway between these two diseases.
Conclusion
Although there are references to dispersants in the literature about patients with both non-Hodgkin lymphoma and GISTs, there is no common molecular pathway between these two diseases.Citation38 Genetic surveys have been done to try to establish a connection between lymphomas and GISTs,Citation39 but there are no encouraging results. We believe that there should be further scientific interest on this field.
Authors’ contributions
M Karanikas, N Machairiotis, P Zarogoulidis, and A Stylianaki wrote the manuscript. N Lyratzopoulos, A Mitrakas, and A Polychronidis performed the surgery. N Courcoutsakis evaluated the radiographic findings. M Spanoudakis treated the patient while he was a member of the Hematology Department, University General Hospital of Alexandroupolis, Democritus University of Thrace, Alexandroupolis, Greece. G Kouklakis, M Karanikas, N Lyratzopoulos, A Mitrakas, and A Polychronidis treated the patient.
Disclosure
The authors report no conflicts of interest in this work.
References
- EvansLSHancockBWNon-Hodgkin lymphomaLancet2003362937813914612867117
- KindblomLGRemottiHEAldenborgFMeis-KindblomJMGastrointestinal pacemaker cell tumor (GIPACT): gastrointestinal stromal tumors show phenotypic characteristics of the interstitial cells of CajalAm J Pathol19981525125912699588894
- HarrisNLJaffeESSteinHA revised European-American classification of lymphoid neoplasms: a proposal from the International Lymphoma Study GroupBlood1994845136113928068936
- MahadevanDFisherRINovel therapeutics for aggressive non-Hodgkin’s lymphomaJ Clin Oncol201129141876188421483007
- NakamuraHSaidJWMillerCWKoefflerHPMutation and protein expression of p53 in acquired immunodeficiency syndrome-related lymphomasBlood19938239209268338955
- GascoyneRDAdomatSAKrajewskiSPrognostic significance of Bcl-2 protein expression and Bcl-2 gene rearrangement in diffuse aggressive non-Hodgkin’s lymphomaBlood19979012442519207459
- MiyashitaTReedJCBcl-2 oncoprotein blocks chemotherapy-induced apoptosis in a human leukemia cell lineBlood19938111511578417786
- PasqualucciLTrifonovVFabbriGAnalysis of the coding genome of diffuse large B-cell lymphomaNat Genet201143983083721804550
- LazzarinoMOrlandiEPaulliMPrimary mediastinal B-cell lymphoma with sclerosis: an aggressive tumor with distinctive clinical and pathologic featuresJ Clin Oncol19931112230623138246020
- BarthTFLeithäuserFJoosSBentzMMollerPMediastinal (thymic) large B-cell lymphoma: where do we stand?Lancet Oncol20023422923412067685
- BentzMBarthTFBruderleinSGain of chromosome arm 9p is characteristic of primary mediastinal B-cell lymphoma (MBL): comprehensive molecular cytogenetic analysis and presentation of a novel MBL cell lineGenes Chromosomes Cancer200130439340111241792
- van BesienKKeltaMBahagunaPPrimary mediastinal B-cell lymphoma: a review of pathology and managementJ Clin Oncol20011961855186411251018
- KarinMCaoYGretenFRLiZWNF-kappaB in cancer: from innocent bystander to major culpritNat Rev Cancer20022430131012001991
- FeuerhakeFKutokJLMontiSNFkappaB activity, function, and target-gene signatures in primary mediastinal large B-cell lymphoma and diffuse large B-cell lymphoma subtypesBlood200510641392139915870177
- SteidlCGascoyneRDThe molecular pathogenesis of primary mediastinal large B-cell lymphomaBlood2011118102659266921700770
- SavageKJMontiSKutokJLThe molecular signature of mediastinal large B-cell lymphoma differs from that of other diffuse large B-cell lymphomas and shares features with classical Hodgkin lymphomaBlood2003102123871387912933571
- RoyBBhattacharjeeAXuBFordDMaizelALCathcartMKIL-13 signal transduction in human monocytes: phosphorylation of receptor components, association with Jaks, and phosphorylation/activation of statsJ Leukoc Biol200272358058912223527
- SkarinATDorfmanDMNon-Hodgkin’s lymphomas: current classification and managementCA Cancer J Clin19974763513729371057
- Gutierrez-GarciaGCardesa-SalzmannTClimentFGene-expression profiling and not immunophenotypic algorithms predicts prognosis in patients with diffuse large B-cell lymphoma treated with immunochemotherapyBlood2011117184836484321441466
- HirotaSIsozakiKMoriyamaYGain-of-function mutations of c-kit in human gastrointestinal stromal tumorsScience199827953505775809438854
- BadalamentiGRodolicoVFulfaroFGastrointestinal stromal tumors (GISTs): focus on histopathological diagnosis and biomolecular featuresAnn Oncol200718Suppl 6vi136vi14017591808
- BaiCGHouXWWangFStem cell factor-mediated wild-type KIT receptor activation is critical for gastrointestinal stromal tumor cell growthWorld J Gastroenterol201218232929293722736916
- LambGAmbraleSLeeBGuptaRRafiyathSMLiuDRecent advances and novel agents for gastrointestinal stromal tumor (GIST)J Hematol Oncol2012512122569033
- WongNADeansZCRamsdenSCThe UK NEQAS for Molecular Genetics scheme for gastrointestinal stromal tumour: findings and recommendations following four rounds of circulationJ Clin Pathol201265978679022685257
- SuzukiKKanekoGKubotaKMalignant tumor, of the gastrointestinal stromal tumor type, in the greater omentumJ Gastroenterol2003381098598814614607
- LasotaJKubanWWardelmannEKIT codon 558 insertions in gastrointestinal stromal tumors. Analysis of 17 rare KIT mutantsHum Pathol200839121728173618715619
- KangHJKohKHYangEDifferentially expressed proteins in gastrointestinal stromal tumors with KIT and PDGFRA mutationsProteomics2006641151115716402362
- GramzaAWCorlessCLHeinrichMCResistance to tyrosine kinase inhibitors in gastrointestinal stromal tumorsClin Cancer Res200915247510751820008851
- MiettinenMSobinLHLasotaJGastrointestinal stromal tumors of the stomach: a clinicopathologic, immunohistochemical, and molecular genetic study of 1765 cases with long-term follow-upAm J Surg Pathol2005291526815613856
- SobinLHComptonCCTNM seventh edition: what’s new, what’s changed: communication from the International Union Against Cancer and the American Joint Committee on CancerCancer2010116225336533920665503
- TanCBZhiWShahzadGMustacchiaPGastrointestinal stromal tumors: a review of case reports, diagnosis, treatment, and future directionsISRN Gastroenterol2012201259596822577569
- JeongIHKimJHLeeSRMinimally invasive treatment of gastric gastrointestinal stromal tumors: laparoscopic and endoscopic approachSurg Laparosc Endosc Percutan Tech201222324425022678321
- NovitskyYWKercherKWSingRFHenifordBTLong-term outcomes of laparoscopic resection of gastric gastrointestinal stromal tumorsAnn Surg20062436738745 discussion 745–73716772777
- PidhoreckyICheneyRTKraybillWGGibbsJFGastrointestinal stromal tumors: current diagnosis, biologic behavior, and managementAnn Surg Oncol20007970571211034250
- HirotaSOhashiANishidaTGain-of-function mutations of platelet-derived growth factor receptor alpha gene in gastrointestinal stromal tumorsGastroenterology2003125366066712949711
- LaiECLauSHLauWYCurrent management of gastrointestinal stromal tumors – a comprehensive reviewInt J Surg201210733434022633986
- WardelmannELosenIHansVDeletion of Trp-557 and Lys-558 in the juxtamembrane domain of the c-kit protooncogene is associated with metastatic behavior of gastrointestinal stromal tumorsInt J Cancer2003106688789512918066
- HerbersAHKeuningJJStaging for CLL-type non-Hodgkin’s lymphoma reveals a gastrointestinal stromal tumourNeth J Med2005632747515766012
- ZimpferAWentPTzankovARare expression of KIT (CD117) in lymphomas: a tissue microarray study of 1166 casesHistopathology200445439840415469479