
Abstract
Background/Aims
There are currently few reports describing the liquid-based cytological characteristics of small cell neuroendocrine carcinoma of the cervix. This study aimed to retrospectively analyze these features to reduce missed or misdiagnosis.
Methods
A total of 11 patients with histologically diagnosed small cell carcinoma of the cervix from three hospitals between 2017 and 2023 were included in this study. The cytological morphology of small cell carcinoma of the cervix and causes of missed or misdiagnosis were analyzed and summarized through a review of clinical data, liquid-based cytology, histology, immunohistochemistry, and human papillomaviruses (HPV) test results.
Results
In this study, the positivity rate of preliminary cytological screening was 63.6% (7/11); however, no cases were accurately diagnosed as small cell carcinoma of the cervix. A total of 36.4% (4/11) of small cell carcinoma of the cervix cases were cytologically negative; retrospective cytology found that two of these were false negatives. The main cytological features of small cell carcinoma of the cervix were summarized. Most of the liquid-based cytology smear cells were dense, and almost all cases showed clustered and scattered cytoplasm-scanty tumor cells. The tumor cells were all deeply stained and relatively consistent small cells. Most cases showed typical nuclear molding, chromatin stippling, and no obvious nucleoli. Mild nuclear smears, nuclear fragments, and mitotic figures were seen in most cases.
Conclusion
Liquid-based cytology has a high rate of missed diagnosis and misdiagnosis in small cell carcinoma of the cervix. This study confirms that reviewing cytology results can effectively reduce this proportion and that increasing understanding of small cell carcinoma of the cervix morphology is conducive to improving the cytology-based diagnosis rate.
Introduction
Cervical neuroendocrine carcinoma is a rare tumor that accounts for <5% of all cervical cancers, most of which are small cell neuroendocrine carcinoma of the cervix.Citation1 Small cell carcinoma of the cervix is more invasive and has a poorer prognosis than cervical squamous cell carcinoma and adenocarcinoma. The five-year survival rate of small cell carcinoma of the cervix ranges from 20% to 37%, which is significantly lower than those of squamous cell carcinoma (74.3%) and adenocarcinoma (64.6%). Regardless of the treatment, the prognosis for patients with advanced small cell carcinoma of the cervix is poor.Citation2,Citation3 However, patients diagnosed early may achieve long-term survival after receiving multimodal therapy. This highlights the importance of early diagnosis of small cell carcinoma of the cervix.Citation3–5
Due to the rarity of small cell carcinoma of the cervix, and because it is usually detected late due to visible masses, only a small percentage of cases undergo cytological screening prior to biopsy or surgery. Therefore, most reports describing the liquid-based cytological features of small cell carcinoma of the cervix are case reports and were carried out in a single institution.Citation6–9 Due to the low diagnostic yield of cytology for small cell carcinoma of the cervix and the number of missed diagnoses,Citation10,Citation11 a deeper understanding of liquid-based cytology in small cell carcinoma of the cervix is necessary.
In the present study, we retrospectively analyzed eligible small cell carcinoma of the cervix cases from three hospitals, comprehensively described the morphological features of small cell carcinoma of the cervix liquid-based cytology, and summarized possible causes of missed or misdiagnosis in combination with the literature.
Materials and Methods
This study is a retrospective study. By querying the case databases of three hospitals (Affiliated Hospital of Southwest Medical University, People’s Hospital of Deyang City, and Chengdu Women’s and Children’s Central Hospital) from January 2017 to September 2023, it was found that 21 cases, 7 cases and 18 cases of cervical small cell carcinoma were diagnosed, accounting for 1.3%, 0.8% and 1.6% of the total number of cervical cancers, respectively. Excluding cervical squamous cell carcinoma or adenocarcinoma cases with only a small amount of small cell carcinoma components, 11 cases of cervical small cell carcinoma with preoperative cytological screening were finally selected for study. All 11 patients were definitively diagnosed after secondary examination of histological sections by two experienced pathologists.
The cervical samples were processed using either the ThinPrepTM liquid-based cytological technique (Hologic, Massachusetts, USA)Citation12 or the SurePathTM liquid-based cytological technique (BD, New Jersey, USA)Citation13 in cytopathology laboratories, and finally stained with Papanicolaou staining. Two pathologists with extensive experience in diagnostic cytology assessed the slides for the following characteristics: background, cell density, cell arrangement, cell size, cytoplasm, and nuclear features. In cases containing squamous cell carcinoma or adenocarcinoma, only small cell carcinoma of the cervix components was selected for evaluation of cytological features. HPV typing was performed by fluorescent quantitative polymerase chain reaction (PCR) to detect 14 high-risk HPV-DNA types (Qiagen, Shenzhen, China).
Clinical staging was based on the latest International Federation of Gynecology and Obstetrics (FIGO) staging,Citation10 and follow-up visits were conducted by telephone. In accordance with the journal’s guidelines, we will provide our data for independent analysis by a selected team by the Editorial Team for the purposes of additional data analysis or for the reproducibility of this study in other centers if such is requested.
Results
Clinical Findings
There were 11 histologically confirmed cases of small cell carcinoma of the cervix during the study period (). Patient ages ranged from 39 to 73 years, with a median age of 49 years. All patients were Chinese women who had experienced childbirth. Among the 11 patients, nine presented with abnormal vaginal bleeding of variable duration, one patient presented with postcoital bleeding, and one patient presented with an aqueous secretion and persistent vaginitis. Based on the gross appearance description of the tumor in the case data, there were four cases with an exogenous mass, three cases with a nodular mass, two cases with a cauliflower-like mass, one case with an endogenous mass, and one case with a large ulcerative mass. No paraneoplastic syndrome was found in the patients. Six patients had tumor markers before treatment, and only one patient had a significant increase in Carbohydrate antigen 19-9 (CA19-9). There were two patients with FIGO stage IB2, four patients with stage IIA1, two patients with stage IIB, one patient with stage IIIC1, and two patients with stage IVB. Of the two patients with stage IVB, one had liver and lung metastases and one had brain metastases. In terms of treatment, 6 patients received radical hysterectomy with pelvic lymphadenectomy, all received chemotherapy, four received radiotherapy, and 5 patients who did not undergo radical surgery received chemoradiotherapy. Prognosis is shown in , but a longer follow-up period is needed to draw valid conclusions.
Table 1 Clinical Data of 11 Cases of Small Cell Carcinoma of the Cervix
Cytologic Findings
In this study, none of the 11 histologically confirmed cases received an accurate small cell carcinoma of the cervix diagnosis during initial cytological screening (). The positive rate of cytology screening was 63.6% (7/11). Among the cytologically positive cases, four were interpreted as squamous epithelial lesions, two were interpreted as glandular epithelial lesions, and one was considered a malignant tumor without classification. The reason for the unclassified case was due to heavy inflammation resulting in only a few tumor cells being sampled. About 36.4% (4/11) of small cell neuroendocrine carcinoma of cervix cases were missed, and review cytological revealed that two out of four cases were false negatives, one of which small cell neuroendocrine carcinoma of cervix cells were detected, and the other was reinterpreted as high grade squamous intraepithelial lesion, suspicious for adenocarcinoma. In the other two cases, cancerous cells were still not detected in the review cytological, and the retrospective histological sections revealed that the tumor cells showed a subepithelial growth pattern without involvement of surface epithelial cells.
Table 2 Histology, Cytology, HPV and Immunohistochemical Results of 11 Cases of Small Cell Carcinoma of the Cervix
The main cytological characteristics of 9 out of 11 malignant smears were summarized (). Tumor diathesis was observed in five cases, 7 cases (7/9) had abundant tumor cells, and two cases had rare tumor cells. Clustered and scattered tumor cells containing a small amount of cytoplasm were seen in all cases (9/9), and a small number of cells with a rosette-like or pseudoglandular arrangement were seen in 4 cases (4/9). The nuclei were all small, relatively consistent hyperchromatic cells, and nuclear atypia was seen. Nuclear molding is the most characteristic change observed in small cell carcinoma of the cervix; however, only 7 cases (7/9) in this study exhibited typical nuclear molding. Granular stippling chromatin was observed in all eight cases, and small nucleoli were occasionally observed. Only one case had no obvious granular stippling chromatin. Slight nuclear smearing was observed in six cases, and nuclear debris and nuclear mitoses were observed in seven cases. Among the small cell carcinoma of the cervix cases included in this study, cytological distinctions were created from two cases containing a small amount of squamous cell carcinoma and two cases containing a small amount of adenocarcinoma. These are not described in the above morphological features.
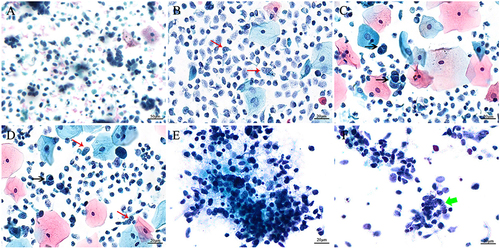
Figure 1 Liquid-based cytological morphology of cervical small cell neuroendocrine carcinoma. (A) Tumor cells are arranged in small clusters, and single cells are scattered (ThinPrep, Papanicolaou staining, 200×). (B–D) Dense tumor cells are predominantly single and scattered, with scanty cytoplasm, typical nuclear molding (shown by black arrows), chromatin stippling, a few small nucleoli (shown by red arrows) and nuclear debris, and superficial or intermediate squamous epithelial cells and neutrophils in the background (ThinPrep, Papanicolaou staining, 400×). (E) Tumor cells have mild nuclear smearing; nuclear debris and tumor diathesis are seen in the background (SurePath, Papanicolaou staining, 400×). (F) Occasional rosette-like or pseudoglandular arrangement of tumor cells was observed (shown by green arrow) (SurePath, Papanicolaou staining, 400×).
Histological Findings
Of the cases included in this study, six were diagnosed by hysterectomy and five were diagnosed by biopsy. Observations included diffuse growth of the tumors, small to medium-sized tumor cells with a scanty cytoplasm arranged in a sheet, and a nest or trabecular shape. More blood vessels and fibers were observed in the stroma. Nuclear division and necrosis were common (). Immunohistochemical staining in all cases showed that Synaptophysin (Syn), Chromogranin A (CgA), and Neural Cell Adhesion Molecules (CD56) were positive in at least one case. Inhibitor cyclin-dependent kinase 4A (P16) staining was performed in seven cases, all of which were diffusely positive. Among the 11 cases, only 7 cases had an HPV test before treatment, and all were positive. There were 5 cases of HPV18 infection and only 2 cases of HPV16 infection (). It seems that HPV18 infection is more common in small cell cervical cancer.
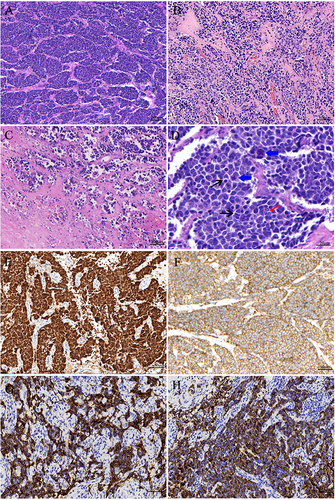
Figure 2 Histological morphology and immunohistochemistry of small cell neuroendocrine carcinoma of cervix. (A and B) Tumor cells are arranged in nests and trabeculae; abundant fibers and blood vessels are seen in the interstitium (100×, HE staining). (C) Tumor diathesis (100×, HE staining). (D) Tumor cells with scanty cytoplasm, typical nuclear molding (shown by black arrows), chromatin stippling, small nucleoli visible in a few tumor cells (shown by red arrows), nuclear mitosis easily visible (shown by blue arrows) (400×, HE staining). (E) Immunohistochemistry showing diffuse, positive P16 (200×). (F) Immunohistochemistry showing positive CD56 (200×). (G) Immunohistochemistry showing positive Syn (200×). (H) Immunohistochemistry showing positive CgA (200×).
Discussion
Small cell carcinoma of the cervix is a poorly differentiated neuroendocrine tumor. The pathogenesis of the disease is still unclear. In the past, it was believed that small cell carcinoma of the uterine cervix originated from the presence of silversmith cells, which are part of the diffuse endocrine system in the normal cervix.Citation14 However, studies have found that small cell carcinoma often coexists with squamous cell carcinoma or adenocarcinoma, and it is speculated that it may originate from the reserve cells under the cervical columnar epithelium.Citation15 This study observed the high frequency of HPV infection in cervical small cell carcinoma, especially HPV18, and the association between HPV-induced carcinogenesis and P53 alterations may be related to tumor invasiveness and metastasis.Citation16,Citation17
Summary of Main Results
None of the cases of small cell carcinoma of the cervix included in this study were given an accurate diagnosis on initial cytological screening, and the vast majority of them were adjudged to be other cervical lesions, and of the cases with negative cytological adjudication, retrospective cytology revealed that half of the cases were false-negative. Summarizing the cytomorphological features of small cell carcinoma of the cervix, it was found that clustered, deeply stained and relatively consistent small cells were seen in almost all cases, and typical nuclear molding and chromatin stippling were seen in the vast majority of cases.
Results in the Context of Published Literature
Small cell carcinoma of the cervix exhibits early local spread and distant metastasis, indicating a poor prognosis. Therefore, early diagnosis is very important.Citation18,Citation19 The cytological and histological features of small cell carcinoma of the cervix are very similar to those of small cell lung cancer. However, due to the rarity of small cell carcinoma of the cervix cases, current studies have shown that cytological screening has a high rate of misdiagnosis and missed diagnosis. In a case series of 13 patients, only one patient was suspected of having small cell carcinoma of the cervix.Citation10 Park et alCitation20 and Gupta et alCitation21 reported a small cell carcinoma of the cervix cytological misdiagnosis rate of 77.8% (7/9) and 66.7% (2/3), respectively. Both of these studies reported the misdiagnoses as squamous epithelial lesions. Another study reported that the misdiagnosis rate of small cell carcinoma of the cervix was 53.8% (7/13).Citation11 Kim et alCitation22 reported that the diagnostic rate of small cell carcinoma of the cervix reached 66.7% (12/18), and the missed or misdiagnosis rates were 11.1% (2/18) and 22.2% (4/18), respectively. This is the highest rate of diagnosis of small cell carcinoma of the cervix by cytological preliminary screening to date. In this study, the positive rate of cytological preliminary screening was 63.6% (7/11), but none of these cases were accurately diagnosed as small cell carcinoma of the cervix. Based on the results summarized in this study and the literature, the causes of missed or misdiagnosis of small cell carcinoma of the cervix by cytology can be summarized as follows: 1. The cases of small cell carcinoma of the cervix are rare, and the cytopathologists do not know enough about them; 2. Small cell carcinoma of the cervix is an easily overlooked component in the presence of squamous or glandular epithelial lesions.Citation7,Citation11,Citation23 3. Some cases show that a subepithelial growth pattern or the tumor is located deeper in the endocervix where cytological brushes fail to pick up lesion cells.Citation10,Citation22 4. Heavy inflammation or necrosis results in insufficient sampling.Citation24 5. Because some of the cytological features of small cell carcinoma of the cervix overlap with other diseases, it is sometimes difficult to differentiate them.
In the liquid-based smear, the cell morphology of small cell carcinoma of the cervix and other lesions is distinguished mainly by the following characteristics.Citation21,Citation25–27 The tumor cells are arranged in small clusters without a specific structure and scattered individually, occasionally with a rosette arrangement. The tumor cells are relatively monomorphic, with nuclei 1.5–2 times the size of the intermediate squamous epithelium, scanty cytoplasm, chromatin stippling, small or absent nucleoli, and characteristic nuclear molding with slight nuclear smearing. Compared with a traditional smear, a liquid-based smear has superior identification performance because it better preserves the nucleus and structural features, avoids air-drying and degeneration artifacts, can increase cell density, and has a cleaner background with fewer inflammatory cells.Citation25,Citation27,Citation28
In order to avoid missed diagnosis and delayed treatment of cervical small cell carcinoma, it is very important to first identify it from benign diseases. At low magnification, small cell carcinoma of the cervix cells is easily mistaken for other cells such as neutrophils, lymphocytes, endometrial cells, and atrophied squamous epithelial cells. However, pathologists must look closely at the chromatin pattern and pleomorphism of the nuclei at high magnification. Generally, the nuclear membrane of benign lesions is smooth, chromatin is delicate, and cell arrangement is polar. If the characteristics of chromatin stippling, characteristic nuclear molding and scanty cytoplasm, it is helpful for the diagnosis of small cell carcinoma and its differentiation from benign lesions.
Second, common cytological differential diagnosis of small cell carcinoma of the cervix also includes high-grade squamous intraepithelial lesion (HSIL), squamous cell carcinoma, adenocarcinoma, lymphoma, and other uncommon malignant tumors. Therefore, the unique cytological features of small cell carcinoma of the cervix are key to differential diagnosis.Citation6,Citation21 Among these, the most difficult is differentiation between HSIL and squamous cell carcinoma, which was also the most misdiagnosed disease in this study (4/7). Compared with small cell carcinoma of the cervix, squamous cell carcinoma usually has clearer cell boundaries, richer and denser cytoplasm, and rougher chromatin. If it is a small cell variant of squamous cell carcinoma, it should be carefully sought for other easily identifiable squamous epithelial lesions.Citation10,Citation11 Small cell carcinoma of the cervix is easily misdiagnosed as endometrial adenocarcinoma or endocervical adenocarcinoma due to the small amount of rosette-like or pseudoglandular arrangements seen in small cell carcinoma of the cervix, which overlaps with the morphological features of glandular epithelial lesions. However, a review of small cell carcinoma of the cervix liquid-based smears revealed a lack of true glands, chromatin stippling, nuclear molding, and nuclear smearing, which is uncommon in adenocarcinoma. If cytoplasmic vacuoles, obvious nucleoli, and three-dimensional cell clusters are seen, the diagnosis of adenocarcinoma is supported.Citation10,Citation22,Citation26,Citation27 Differentiation of lymphoma and other uncommon malignant tumors is relatively rare and requires careful consideration of the medical history and cell morphology. Any suspicion of malignancy may be confirmed by immunocytochemical staining of the residual fluid or biopsy.Citation21,Citation25,Citation26
In the diagnosis of small cell carcinoma of the cervix, morphology is the cornerstone, but when morphological identification is difficult, the auxiliary diagnosis of neuroendocrine markers is still needed.Citation29 Rekhi et alCitation17 reported that CgA, Syn and CD56 are the best markers for the diagnosis of neuroendocrine tumors. The neuroendocrine markers used in this study were CgA, Syn and CD56. The results showed that at least one of the above indexes was positive. Similar results were found in other reports.Citation30 In recent years, a number of studies have confirmed that insulinoma-associated protein 1 (INSUM1) has good sensitivity and specificity for the diagnosis of cervical neuroendocrine carcinoma and is a promising diagnostic marker.Citation31–33 However, it should be noted that the expression of neuroendocrine markers can also be seen in a small number of other types of cervical cancer, and it seems to be related to poor prognosis.Citation34 Therefore, morphological evaluation combined with immunohistochemistry can obtain higher diagnostic specificity.
Strengths and Weaknesses
The advantage of this study lies in summarizing the morphological characteristics of cervical small cell neuroendocrine carcinoma from a cytological perspective, confirming that reviewing cytology can effectively reduce missed and misdiagnosis, and combining with the literature analysis of the causes of missed and misdiagnosis as well as its differential diagnosis. As far as we know, the relevant literature is sparse with a small number of cases and has not systematically analyzed missed and misdiagnosis. Due to the rarity of the disease, despite multicentre studies, the number of cases is still not optimal to reliably assess the prognosis of patients, and immunocytochemistry was not performed on cytological specimens.
Implications for Practice and Future Research
This study has deepened the understanding of the cytological pattern of small cell carcinoma of the cervix and the reasons for missed and misdiagnosis. As cytological diagnosis of small cell carcinoma of the cervix is still difficult and cases are scarce, more multicentre studies are encouraged to enhance cytomorphological studies of small cell carcinoma of the cervix, and immunocytochemical staining of liquid-based cytology specimens is performed when necessary to improve the rate of early diagnosis.
Conclusion
Due to the rarity of small cell carcinoma of the cervix and its overlap with a small number of morphological features of other diseases, this study confirms that the specific diagnosis of small cell carcinoma of the cervix through cytology remains challenging. However, the results of this retrospective study, which reflects on the causes of missed and misdiagnosis, can be used to effectively improve the diagnosis rate and reduce missed diagnoses.
Ethics Approval and Informed Consent
The study was approved by the Ethics Committee of the Affiliated Hospital of Southwest Medical University (Approval No. KY2023295). Because the study was retrospective and the information was anonymous, the requirement for informed consent was waived. All procedures involving human individuals in our study were performed in accordance with the Declaration of Helsinki.
Disclosure
The authors report no conflicts of interest in this work.
Acknowledgments
We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript. I would also like to express my heartfelt thanks to my colleagues in pathology from the affiliated Hospital of Southwest Medical University for their contribution to the cytological and histological evaluation of some cases.
Additional information
Funding
References
- Tempfer CB, Tischoff I, Dogan A, et al. Neuroendocrine carcinoma of the cervix: a systematic review of the literature. BMC Cancer. 2018;18(1):530. doi:10.1186/s12885-018-4447-x
- Chu T, Meng Y, Wu P, et al. The prognosis of patients with small cell carcinoma of the cervix: a retrospective study of the SEER database and a Chinese multicentre registry. Lancet Oncol. 2023;24(6):701–708. doi:10.1016/S1470-2045(23)00185-7
- Salvo G, Flores Legarreta A, Ramalingam P, et al. Clinicopathologic characteristics, oncologic outcomes, and prognostic factors in neuroendocrine cervical carcinoma: a Neuroendocrine Cervical Tumor Registry study. Int J Gynecol Cancer. 2023;33(9):1359–1369. doi:10.1136/ijgc-2023-004708
- Xu F, Ma J, Yi H, et al. Clinicopathological Aspects of Small Cell Neuroendocrine Carcinoma of the Uterine Cervix: a Multicenter Retrospective Study and Meta-Analysis. Cell Physiol Biochem. 2018;50(3):1113–1122. doi:10.1159/000494538
- Chan JK, Loizzi V, Burger RA, Rutgers J, Monk BJ. Prognostic factors in neuroendocrine small cell cervical carcinoma: a multivariate analysis. Cancer. 2003;97(3):568–574. doi:10.1002/cncr.11086
- Rajasekaran S, Gupta P, Gupta N. Liquid-based cytology and immunocytochemistry in the evaluation of a vault lesion in a postmenopausal woman. Cytopathology. 2023;34(2):169–172. doi:10.1111/cyt.13196
- Okabe A, Ishida M, Noda Y, et al. Small-cell neuroendocrine carcinoma of the cervix accompanied by adenocarcinoma and high-grade squamous intraepithelial lesion. Diagn Cytopathol. 2022;50(10):E285–E288. doi:10.1002/dc.24997
- Shimojo N, Hirokawa YS, Kanayama K, et al. Cytological features of adenocarcinoma admixed with small cell neuroendocrine carcinoma of the uterine cervix. Cytojournal. 2017;14:12. doi:10.4103/1742-6413.207139
- Alphandery C, Dagrada G, Frattini M, Perrone F, Pilotti S. Neuroendocrine small cell carcinoma of the cervix associated with endocervical adenocarcinoma: a case report. Acta Cytol. 2007;51(4):589–593. doi:10.1159/000325803
- Zhou C, Hayes MM, Clement PB, Thomson TA. Small cell carcinoma of the uterine cervix: cytologic findings in 13 cases. Cancer. 1998;84(5):281–288.
- Kim MJ, Kim NR, Cho HY, Lee SP, Ha SY. Differential diagnostic features of small cell carcinoma in the uterine cervix. Diagn Cytopathol. 2008;36(9):618–623. doi:10.1002/dc.20875
- Linder J, Zahniser D. ThinPrep Papanicolaou testing to reduce false-negative cervical cytology. Arch Pathol Lab Med. 1998;122(2):139–144.
- Fremont-Smith M, Marino J, Griffin B, Spencer L, Bolick D. Comparison of the SurePath liquid-based Papanicolaou smear with the conventional Papanicolaou smear in a multisite direct-to-vial study. Cancer. 2004;102(5):269–279. doi:10.1002/cncr.20599
- Chao A, Wu RC, Lin CY, Chang TC, Lai CH. Small cell neuroendocrine carcinoma of the cervix: from molecular basis to therapeutic advances. Biomed J. 2023;46(5):100633. doi:10.1016/j.bj.2023.100633
- Gurubalan G, Parwaiz A, Ajit S, Kumar T, Kumari M, Bhadani P. Small cell neuroendocrine carcinoma with adenocarcinoma and high grade squamous intraepithelial neoplasia of the cervix. Autops Case Rep. 2023;13:e2023452. doi:10.4322/acr.2023.452
- Wistuba II, Thomas B, Behrens C, et al. Molecular abnormalities associated with endocrine tumors of the uterine cervix. Gynecol Oncol. 1999;72(1):3–9. doi:10.1006/gyno.1998.5248
- Rekhi B, Patil B, Deodhar KK, et al. Spectrum of neuroendocrine carcinomas of the uterine cervix, including histopathologic features, terminology, immunohistochemical profile, and clinical outcomes in a series of 50 cases from a single institution in India. Ann Diagn Pathol. 2013;17(1):1–9. doi:10.1016/j.anndiagpath.2012.01.009
- Lee JM, Lee KB, Nam JH, et al. Prognostic factors in FIGO stage IB-IIA small cell neuroendocrine carcinoma of the uterine cervix treated surgically: results of a multi-center retrospective Korean study. Ann Oncol. 2008;19(2):321–326. doi:10.1093/annonc/mdm465
- Castle PE, Pierz A, Stoler MH. A systematic review and meta-analysis on the attribution of human papillomavirus (HPV) in neuroendocrine cancers of the cervix. Gynecol Oncol. 2018;148(2):422–429. doi:10.1016/j.ygyno.2017.12.001
- Park HJ, Choi YM, Chung CK, et al. Pap smear screening for small cell carcinoma of the uterine cervix: a case series and review of the literature. J Gynecol Oncol. 2011;22(1):39–43. doi:10.3802/jgo.2011.22.1.39
- Gupta P, Gupta N, Suri V, Rai B, Rajwanshi A. Cytomorphological features of cervical small cell neuroendocrine carcinoma in SurePath™ liquid-based cervical samples. Cytopathology. 2021;32(6):813–818. doi:10.1111/cyt.13030
- Kim Y, Ha HJ, Kim JS, et al. Significance of cytologic smears in the diagnosis of small cell carcinoma of the uterine cervix. Acta Cytol. 2002;46(4):637–644. doi:10.1159/000326968
- Nishiumi Y, Nishimura T, Kashu I, et al. Adenocarcinoma in situ admixed with small cell neuroendocrine carcinoma of the cervix: a case report with cytological features. Diagn Cytopathol. 2018;46(9):752–755. doi:10.1002/dc.23940
- Gupta N, John D, Dudding N, Crossley J, Smith JH. Factors contributing to false-negative and potential false-negative cytology reports in SurePath™ liquid-based cervical cytology. Cytopathology. 2013;24(1):39–43. doi:10.1111/j.1365-2303.2012.00992.x
- Giorgadze T, Kanhere R, Pang C, et al. Small cell carcinoma of the cervix in liquid-based Pap test: utilization of split-sample immunocytochemical and molecular analysis. Diagn Cytopathol. 2012;40(3):214–219. doi:10.1002/dc.21542
- Ng WK, Cheung LK, Li AS, Tse SK, Pang SW, Chow JC. Thin-layer cytology findings of small cell carcinoma of the lower female genital tract. Review of three cases with molecular analysis. Acta Cytol. 2003;47(1):56–64. doi:10.1159/000326476
- Ciesla MC, Guidos BJ, Selvaggi SM. Cytomorphology of small-cell (neuroendocrine) carcinoma on ThinPrep cytology as compared to conventional smears. Diagn Cytopathol. 2001;24(1):46–52. doi:10.1002/1097-0339(200101)24:1
- Reich O, Pickel H, Pürstner P. Exfoliative cytology of invasive neuroendocrine small cell carcinoma in a cervical cytologic smear. A case report. Acta Cytol. 1996;40(5):980–984. doi:10.1159/000334013
- Huang R, Yu L, Zheng C, et al. Diagnostic value of four neuroendocrine markers in small cell neuroendocrine carcinomas of the cervix: a meta-analysis. Sci Rep. 2020;10(1):14975. doi:10.1038/s41598-020-72055-x
- Tsunoda S, Jobo T, Arai M, et al. Small-cell carcinoma of the uterine cervix: a clinicopathologic study of 11 cases. Int J Gynecol Cancer. 2005;15(2):295–300. doi:10.1111/j.1525-1438.2005.15219.x
- Zou Q, Zhang L, Cheng Z, Guo X, Cao D. INSM1 Is Less Sensitive But More Specific Than Synaptophysin in Gynecologic High-grade Neuroendocrine Carcinomas: an Immunohistochemical Study of 75 Cases With Specificity Test and Literature Review. Am J Surg Pathol. 2021;45(2):147–159. doi:10.1097/PAS.0000000000001641
- Kuji S, Endo A, Kubota M, et al. Immunosensitivity and specificity of insulinoma-associated protein 1 (INSM1) for neuroendocrine neoplasms of the uterine cervix. J Gynecol Oncol. 2023;34(1):e1. doi:10.3802/jgo.2023.34.e1
- Kuji S, Watanabe R, Sato Y, et al. A new marker, insulinoma-associated protein 1 (INSM1), for high-grade neuroendocrine carcinoma of the uterine cervix: analysis of 37 cases. Gynecol Oncol. 2017;144(2):384–390. doi:10.1016/j.ygyno.2016.11.020
- Chavez-Blanco A, Taja-Chayeb L, Cetina L, et al. Neuroendocrine marker expression in cervical carcinomas of non-small cell type. Int J Gynecol Pathol. 2002;21(4):368–374. doi:10.1097/00004347-200210000-00006