
Abstract
Mechanical thrombectomy has emerged as a promising treatment for acute ischemic stroke caused by large vessel occlusion. However, cases involving cancerous emboli retrieved during endovascular embolectomy are rare. We present a case of a 65-year-old man with a history of heavily treated rectal cancer, who developed a middle cerebral artery (MCA) infarction due to metastatic adenocarcinoma. The patient presented with sudden onset right-side weakness, right facial palsy, global aphasia, and left gaze deviation, with a National Institutes of Health Stroke Scale (NIHSS) score of 16. Following intravenous thrombolysis, endovascular thrombectomy was performed, achieving nearly complete recanalization. Pathological examination of the retrieved thrombus revealed metastatic adenocarcinoma of rectal origin. The patient’s neurological deficits gradually improved, and he was successfully discharged to undergo further palliative therapy. This case underscores the importance of considering mechanical thrombectomy for patients with advanced solid organ malignancy presenting with acute ischemic stroke, even when the etiology could be a tumor embolus. Our findings highlight the potential for mechanical thrombectomy to restore neurological function in such cases, allowing patients to proceed to the next level of care with a reasonably good post-stroke quality of life.
Introduction
Arterial thromboembolic (ATE) events are much less common in cancer patients than cancer-associated venous thromboembolism.Citation1 In a Danish registry cohort study, the cumulative incidence of ATE at one year of cancer diagnosis was 2.11 per 1000 patient-years.Citation2 In the study, ATE was defined as either myocardial infarction, unspecified or ischemic cerebral infarction, or peripheral arterial embolism, presumably associated with the paraneoplastic hypercoagulable state. In an interesting study to look into the nature of Trousseau’s syndrome-related arterial thrombus from patients with cancer-associated stroke using immunohistochemical tests, the thrombus composition in cancer patients contained more platelets and fewer erythrocytes than non-cancer patients.Citation3 Other than cancer procoagulant-related ATE, the other type of tumor-associated intracranial embolism is caused by direct tumor embolism pumped up by the heart, most commonly from a benign tumor such as atrial myxoma, cardiac papillary fibroelastoma, or advanced squamous cell carcinoma of the lung.Citation4–7
Mechanical thrombectomy is a promising treatment for acute ischemic stroke caused by occlusion of a large vessel.Citation8,Citation9 Its add-on efficacy over intravenous thrombolysis alone has been proven in multiple trials.Citation10,Citation11 However, retrieved thrombi from the endovascular embolectomy that were pathologically proven to be cancerous emboli are rarely reported. Herein, we report a case of middle cerebral artery (MCA) infarction due to metastatic adenocarcinoma from pre-existing, heavily pre-treated rectal cancer that progressed to lung metastases and cardiac invasion.
Case Report
A 65-year-old man was admitted to our hospital due to a sudden onset of right-side weakness. On arrival, he was found to have right facial palsy, right hemiparesis, global aphasia, and left gaze deviation. His National Institutes of Health Stroke Scale (NIHSS) score was 16. Initial laboratory investigations with complete blood count, electrolytes, and renal and liver function were unremarkable. An electrocardiogram revealed normal sinus rhythm. He was a patient with rectal cancer treated with low anterior resection, adjuvant radiotherapy, and chemotherapy seven years ago. Fourteen months earlier, he developed left parieto-occipital region brain metastasis, for which he underwent craniotomy with safe maximal tumor excision and consolidative whole brain radiotherapy with a total radiation dose of 3000 cGy. No mutations were detected in any of the RAS and B-RAF hotspots. Subsequently, 17 cycles of bevacizumab plus FOLFIRI-type biochemotherapy were administered. He also had a medical history of hypertension but had no diabetes mellitus, dyslipidemia, or coronary heart disease. The reported baseline modified Rankin Score (mRS) is 0.
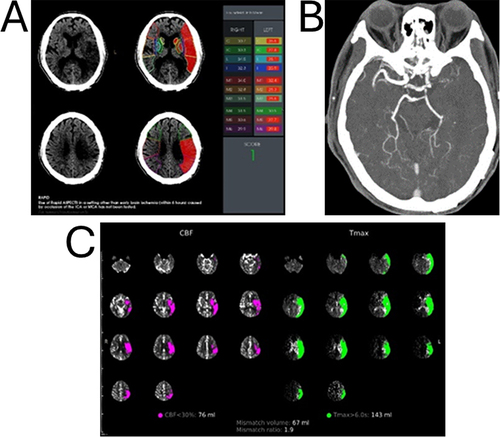
Computerized tomography (CT) brain scan showed postoperative hypodensity in the left parietal lobe resulted from previous brain surgery and a faint hypodensity in the left frontotemporoparietal lobe. There was no definite ischemic change or hemorrhage (). Low-dose intravenous recombinant tissue plasminogen activator (rt-PA, alteplase, dose at 0.6 mg/kg) was administered 210 minutes after symptom onset. CT angiography (CTA) showed complete occlusion of the left proximal M1 (). Computed tomography perfusion (CTP), RAPID map (IschemaView), showing a perfusion deficit (Tmax > 6 seconds) 143 mL and ischemic core (CBF < 30%) of 76 mL at left MCA territory ().
Figure 1 (A) Baseline axial CT performed 360 min after the symptom onset showing a faint hypodensity in the left frontotemporoparietal lobe with a RAPID-ASPECTS of score 1. (B) CTA showed a complete occlusion of the left M1. (C) The RAPID-CTP analysis demonstrated a complete infarct volume of 76 milliliters (mL), entailing a small infarcted core within a large volume of penumbra in the right internal carotid artery vascular territory. The configured Tmax > 6-second volume representing the combination of the infarcted core volume and hypoperfused brain was 143 mL in the left cerebral hemisphere, deriving a mismatch ratio of 1.9.
Endovascular thrombectomy was then performed under general anesthesia. The onset to puncture time is 280 minutes. Digital subtraction angiography (DSA) with left internal carotid artery (ICA) injection revealed left proximal M1 thrombosis (). Stent-retriever (SR) thrombectomy was subsequently performed by placement of a 4 mm x 40 mm Solitaire X (Medtronic) stent across the thrombus (). After intrathrombus deployment of the SR two times, near-complete recanalization (by the thrombolysis in cerebral infarction (TICI) classification 2b) was achieved (). Large amounts of reddish-brown thrombus were found in the SR (). The neurological deficits improved gradually, but right-sided sensory disturbance remained. Pathological examination of the retrieved thrombus revealed metastatic adenocarcinoma of rectal origin ( and ). On a contrast-enhanced CT and a PET/CT of the chest, a mass in the left hilar region was revealed, infiltrating the pulmonary vein and left atrium ( and ). The patient was successfully discharged and underwent cetuximab-based palliative therapy. He succumbed to cancer progression four months after intracranial tumor embolectomy.
Figure 2 (A) Digital subtraction angiography (DSA), left internal carotid artery injection, anteroposterior (AP) view, showing proximal left middle cerebral artery (MCA) M1 occlusion with intraluminal filling defect due to thrombosis. (B) DSA, AP view, showing a 4-mm × 40-mm Solitaire X (Medtronic) stent-retriever (SR) un-sheathed in the affected MCA with reopening of the vessel. (C) DSA, AP view, post-thrombectomy, showing successful recanalization and restoration of blood flow.
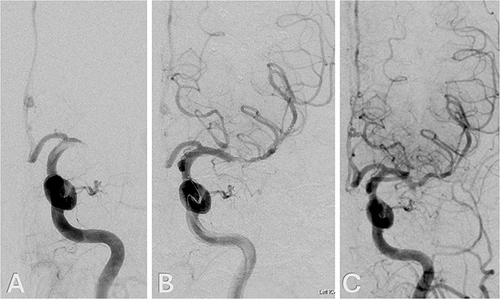
Figure 3 (A) Photograph showing a reddish brown gelatinous thrombus extracted by the stent-retriever. Panels B and C. Photomicrographs of the retrieved thrombi, Hematoxylin and eosin stain, x 100 (B) and x 400 (C), showing fibrin and blood admixed with metastatic adenocarcinoma, which is composed of tubular or fused glands, with pseudostratified epithelium, consistent with colorectal origin. Immunohistochemical stains showed CK7-negative, CD20-positive, and CDX-2-positive.
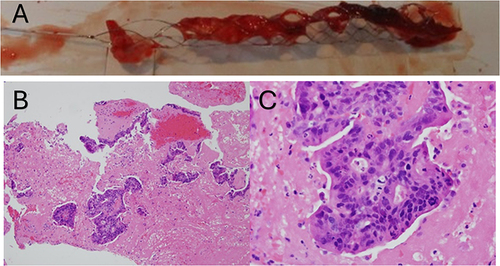
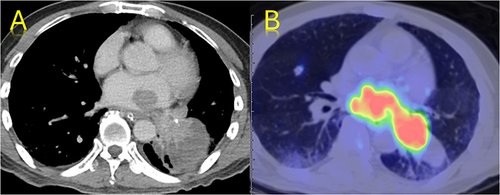
Figure 4 (A) Contrast-enhanced axial CT and (B) PET/CT fusion images of the thorax showing a left lung mass invading the left atrium and pulmonary vein.
Discussion
Clinicians in the fields of emergency medicine, neurology, and oncology often possess a conservative or even annihilistic attitude towards a patient with advanced metastatic solid malignancy who developed a large cerebral vessel occlusion causing a massive cerebral infarct. A large Korean study estimated that among patients who underwent reperfusion therapy from the Korean national registry for such therapy, only 4.6% and 5.8% had active and nonactive cancer, respectively.Citation12 Another extensive national registry analysis demonstrated that out of 40,537 patients with large vessel occlusion who underwent mechanical thrombectomy, only 2.3% were also a patient with metastatic cancer.Citation13 The very low proportion of cancer patients in the statistics might suggest that much fewer patients with pre-existing cancer would be arranged to undergo the procedure even in need of it. The debate about the safety issue and effectiveness of mechanical thrombectomy for patients with active solid tumor cancer can be put to rest because recent multiple studies have all demonstrated comparable efficacy and safety attained in patients with no cancer.Citation7,Citation12–20
The post-embolectomy pathological report of the thrombus revealed blood admixed with metastatic adenocarcinomas, such as that in our case is extremely rare.Citation3,Citation18 All the large studies reported no cancerous cells in the embolectomy-retrieved thrombus. Studies that have looked into the composition of the thrombus mainly reported thrombi mixed with fibrin platelet components.Citation3,Citation21 For patients with cerebral cancerous embolism causing large vessel occlusion, intravenous thrombolysis as for cryptogenic ischemic infarction could be less effective than direct endovascular thrombectomy to remove the tumor clots. In addition, the first-line clinicians in the field of hyperacute stroke care often hesitate to administer intravenous alteplase, regarding it as relatively contraindicated in patients with advanced malignancy.
Mattingly et al from a North American stroke center reported their single-center experience of carrying out endovascular embolectomy in patients with active cancer. The results were encouraging, showing comparable recanalization grade and post-procedure hemorrhage rate with the larger pool of counterparts who did not have cancer.Citation19 Although individual patients were considered on a case-by-case basis, mechanical thrombectomy, when the capacity facilitates, should be strongly recommended to the patient in order to restore immediate recanalization and hopefully good neurological functional outcome. A recent meta-analysis performed by the investigators of the Mayo Clinic assimilating rare cases of cancer-associated cerebral embolism reveals some vital information about the long-term outcomes in patients who underwent mechanical thrombectomy with or without intravenous thrombolysis. Successful reperfusion, defined as TICI 2b–3, was achieved in nearly 90% of the patients; of them, approximately 60% achieved TICI 3. At follow-up, functional independence was observed in 30% of the treated cohort.Citation7 However, patients with active cancer would harbor a four-fold increase in the risk of death during six months’ follow-up, with approximately 46% of the patients dying when compared with patients who did not have cancer.Citation12
The uniqueness of this case analysis is not only its rarity. The patient regained the level of neurological function status prior to the massive stroke, which had helped him and the caregivers find adequate time to move on to the next level of care with reasonably good post-stroke quality of life. Successful reperfusion and restoring neurologic function will allow the patient and family more quality time together and a better quality of life, which is particularly important in patients with limited life expectancy. The main limitation noted in this case was that there was no adequate time to study the etiology of the ischemic stroke before the thrombectomy. Nevertheless, the potential risks of mechanical thrombectomy for such a subgroup of patients are similar to patients without cancer in terms of dissection, perforation, vessel spasm, emboli to distal branch, reocclusion, parenchymal hemorrhage, and symptomatic intracerebral hemorrhage, as revealed by a large retrospective cohort analysis.Citation12
Conclusion
In conclusion, this case presents a compelling example involving advanced rectal cancer with brain metastasis and a rare instance of stroke caused by metastatic adenocarcinoma arising from a metastatic lung tumor with left atrial invasion. It reminds us that the medical community in the arena of hyperacute stroke care needs to recommend mechanical thrombectomy in the first place, even the etiology of the acute ischemic stroke could be a tumor embolus in patients with advanced solid organ malignancy. Mechanical thrombectomy can be highly effective for acute ischemic stroke in cancer patients, offering significant improvements in neurological function and quality of life, even with advanced malignancy. Despite similar procedural risks to non-cancer patients, careful patient selection, and a multidisciplinary approach can optimize outcomes and provide meaningful palliative benefits.
Ethics Statement
The patient is deceased; therefore, we sought permission and obtained written consent for publication from the patient’s next of kin. A copy of the signed consent form has been submitted along with the manuscript to the journal. Institutional approval was not required to publish this case report. We wrote this case report adhering to the CARE guidelines to ensure all key details about the case were reported and submitted the checklist with the report.
Disclosure
The authors report no conflicts of interest in this work.
References
- Kok VC. Bidirectional risk between venous thromboembolism and cancer in East Asian patients: synthesis of evidence from recent population-based epidemiological studies. Cancer Manag Res. 2017;9:751–759. doi:10.2147/CMAR.S151331
- Mulder FI, Horváth-Puhó E, van Es N, et al. Arterial thromboembolism in cancer patients: a Danish population-based cohort study. JACC CardioOncol. 2021;3(2):205–218. doi:10.1016/j.jaccao.2021.02.007
- Park H, Kim J, Ha J, et al. Histological features of intracranial thrombi in stroke patients with cancer. Ann Neurol. 2019;86(1):143–149. doi:10.1002/ana.25495
- Hao Y, Fan C, Gao Y, et al. Cerebral embolism and MINOCA secondary to left atrial myxoma after occlusion of atrial septal defect by amplatzer occluder: a case report. Heart Surg Forum. 2024;27(1):E006–e013. doi:10.59958/hsf.5803
- Bandlamuri S, Custozzo A, Silva J, et al. Systematic review and case of thrombectomy for pediatric stroke due to myxoma embolism. World Neurosurg. 2024;183:e761–e771. doi:10.1016/j.wneu.2024.01.024
- An KR, Marshall TC, Cusimano RJ. Vasculitic rash and cerebral emboli in an adolescent with left atrial myxoma. BMJ Case Rep. 2024;17(2):e258822. doi:10.1136/bcr-2023-258822
- Toruno M, Al-Janabi O, Karaman I, et al. Mechanical thrombectomy for the treatment of large vessel occlusion due to cancer-related cerebral embolism: a systematic review. Interv Neuroradiol;2024. 15910199241230356. 10.1177/15910199241230356
- Cimflova P, Singh N, Ospel JM, et al. Association of stent-retriever characteristics in establishing successful reperfusion during mechanical thrombectomy: results from the ESCAPE-NA1 trial. Clin Neuroradiol. 2022;32(3):799–807. doi:10.1007/s00062-021-01123-0
- Tsai ST, Wang WC, Lin YT, et al. Use of a smartphone application to speed up interhospital transfer of acute ischemic stroke patients for thrombectomy. Front Neurol. 2021;12:606673. doi:10.3389/fneur.2021.606673
- Kobeissi H, Adusumilli G, Ghozy S, et al. Mechanical thrombectomy alone versus with thrombolysis for ischemic stroke: a meta-analysis of randomized trials. Interv Neuroradiol. 2023;1:15910199231154331.
- Berkhemer OA, Fransen PS, Beumer D, et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N Engl J Med. 2015;372(1):11–20. doi:10.1056/NEJMoa1411587
- Yoo J, Kim YD, Park H, et al. Immediate and long-term outcomes of reperfusion therapy in patients with cancer. Stroke. 2021;52(6):2026–2034. doi:10.1161/STROKEAHA.120.032380
- Aboul-Nour H, Maraey A, Jumah A, et al. Mechanical thrombectomy for acute ischemic stroke in metastatic cancer patients: a nationwide cross-sectional analysis. J Stroke. 2023;25(1):119–125. doi:10.5853/jos.2022.02334
- Aloizou AM, Richter D, Charles James J, et al. Mechanical thrombectomy for acute ischemic stroke in patients with malignancy: a systematic review. J Clin Med. 2022;11(16):4696. doi:10.3390/jcm11164696
- Ciolli L, Bigliardi G, Ferraro D, et al. Efficacy of mechanical thrombectomy in patients with ischemic stroke and cancer. J Clin Neurosci. 2021;91:20–22. doi:10.1016/j.jocn.2021.06.029
- Garg A, Chopra S, Starr M, et al. In-hospital outcomes and recurrence of acute ischemic stroke in patients with solid organ malignancy. Neurology. 2022;99(4):e393–e401. doi:10.1212/WNL.0000000000200601
- Jeon Y, Baik SH, Jung C, et al. Mechanical thrombectomy in patients with acute cancer-related stroke: is the stent retriever alone effective? J Neurointerv Surg. 2021;13(4):318–323. doi:10.1136/neurintsurg-2020-016144
- Magami S, Yoshida K, Nakao Y, et al. A single-center experience of mechanical thrombectomy for cancer-associated ischemic stroke. J Neuroendovasc Ther. 2024;18(2):37–46. doi:10.5797/jnet.oa.2023-0067
- Mattingly TK, Risco JE, Burch JE, et al. Endovascular therapy is effective for large vessel occlusion despite concurrent cancer. J Stroke Cerebrovasc Dis. 2022;31(6):106439. doi:10.1016/j.jstrokecerebrovasdis.2022.106439
- Sallustio F, Mascolo AP, Marrama F, et al. Safety and efficacy of reperfusion therapies for acute ischemic stroke patients with active malignancy. J Stroke Cerebrovasc Dis. 2019;28(8):2287–2291. doi:10.1016/j.jstrokecerebrovasdis.2019.05.018
- Johnson JN, Srivatsan A, Chueh J, et al. Impact of histological clot composition on preprocedure imaging and mechanical thrombectomy. Brain Circ. 2022;8(2):87–93. doi:10.4103/bc.bc_81_21