
Abstract
Vaginal paraganglioma is a rare and unusual tumor occurring in the vaginal wall. It is a solitary primary paraganglioma, especially in atypical sites. Herein, we report an unusual case of a 17-year-old woman who had not experienced vomiting, or hypertension. She was found to have an immobile solid mass in the right side of her vaginal wall. Positron emission tomography/computed tomography scans revealed a well-defined solid ovoid mass adjacent to the bladder and pelvic floor. Tumor markers were within the normal range. A transient blood pressure increase occurred during the biopsy. After oral administration of antihypertensive drugs, surgery was performed to completely remove the mass. Histopathological examination indicated that it was a paraganglioma of the vagina. Repeat computed tomography examination did not reveal any local recurrence or distant metastasis during the 12-month follow-up period.
Introduction
Derived from neural crest cells, paraganglioma is formed by chromaffin or nonchromaffin neural epithelioid cells, which are related to sympathetic or parasympathetic nerves.Citation1 Until now, there has been no uniform standard for its phase division and treatment.Citation2 Paragangliomas are mostly distributed in paraganglion-gathering areas, such as the adrenal glands, neck, mediastinum, or retroperitoneum,Citation3–Citation5 but rarely occur in the vaginal wall. This report will analyze one case of a young woman who suffered from vaginal paraganglioma, together with a review of other relevant literature.
Case report
A 17-year-old woman with no history of marriage or pregnancy was hospitalized because of irregular vaginal bleeding over 5 months. She had no history of genetic disease, coagulation dysfunction, or liver cirrhosis, but had asthma. Physical examination revealed a blood pressure of 140/100 mmHg, a pulse rate of 95/minute, and no superficial lymph nodes could be palpated. Since the patient had had no sex, abdomen ultrasound was used instead of vaginal ultrasound. This showed that her uterus appeared normal in its dimensions, shape, and position. Both ovaries seemed normal for site, dimension, and echo structure. There was no free fluid in the Douglas pouch, while her pelvic computed tomography (CT) showed a 40 × 32 mm regular-margin hyperdense abnormal signal in the right vagina wall adjacent to the bladder. The results of positron emission tomography (PET)/CT were as follows: mass of soft-tissue density in the right vaginal wall and unusual hypermetabolism of fluorodeoxyglucose (FDG) matched with the tumor appearance; nodular soft-tissue density shadow in the pelvic cavity and hypermetabolism of FDG may have indicated the same lesion in the right vaginal wall. During biopsy of the vaginal tumor under intravenous anesthesia, her blood pressure suddenly rose to 160/100 mmHg, and then came back to 130/90 mmHg after examination. The pathological diagnosis was vaginal paraganglioma.
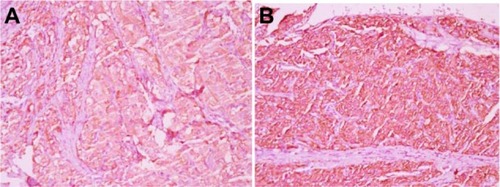
After oral administration of sustained-release metoprolol and nifedipine tablets for 1 week, the woman had vaginal tumorectomy and reconstruction performed, and she had smooth blood pressure throughout the operation. The tumor mass was gray-white and taupe, with a size of 35×30×25 mm (). Microscopically, polygon-like oncocytes were spread in nest or cluster forms. Abundant acidophilic granulates within the cytoplasm and round or oval karyons could be clearly identified. The tumor cells were clustered in small nests or irregular trabecular structures demarcated by delicate fibrous stroma and capillaries in the Zellballen pattern. In the tumor stroma, blood sinus, blood capillary, and little fibrous tissue could be found (). Synaptophysin, chromogranin A, protein S-100, neuron-specific enolase, cell proliferation-associated antigen Ki67, and vimentin were all positive, while smooth-muscle actin, human melanoma-associated antigen (HMB-45), and cytokeratin were negative in immunohistochemistry assay ().
Figure 1 Surgical specimen of paraganglioma of vagina.

Figure 2 Vaginal tumor cells.
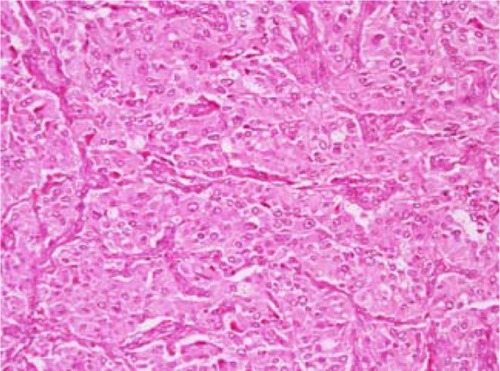
Figure 3 Positive immunohistochemical staining for chromogranin (400×) (A); positive immunohistochemical staining for synaptophysin (400×) (B).
Discussion
Paraganglioma is a rare soft-tissue neuroendocrine tumor, and can be classified as pheochromocytoma and extra-adrenal paraganglioma depending on its pathogenic site. The latter is closely related to tumors in the extra-adrenal sympathetic and parasympathetic paraganglioma, and named after the anatomic site as well as its functional activity.Citation6 Paragangliomas have rarely been reported in the female genital tract, including in the ovary, broad ligament, uterus, and vulva.Citation7–Citation14 To the best of our knowledge, only five cases of vaginal paraganglioma have been reported since 1998, with a median age of 31. 3 years if including our case together.Citation15–Citation19
Furthermore, paragangliomas can be divided into functional and nonfunctional types according to their ability for synthesis, storage, and secretion of catecholamine, as well as production of various peptides, neurohormones, and chromaffin protein grains. Paraganglioma is typical in its clinical manifestations, such as paroxysmal or consecutive elevation of blood pressure, headache, dizziness, palpitation, sweating, fainting, and blurred vision. It is also known as catecholamine syndrome.Citation4,Citation6,Citation20,Citation21 Located in the vagina, paraganglioma has some special symptoms, such as irregular vaginal bleeding, vaginal pain, or finding a vaginal wall mass during routine gynecological examination. Sometimes, serious cardiovascular complications like hypertension, tachycardia, arrhythmia, or myocardial infarction may arise from the stimulation of surgery or coitus.Citation15,Citation17 In this case, the young woman had irregular vaginal bleeding, and suffered from dizziness, headache, and palpitation after physical exercise. Her blood pressure and heart rate fluctuated abnormally during the biopsy examination, which coincided with functional nonchromaffin paraganglioma.
It is difficult to make a preoperative diagnosis of vaginal paraganglioma due to the lack of specific symptoms, and it may be misdiagnosed as vaginal rhabdomyosarcoma, leiomyoma, or hemangioma, among others. Therefore, it should be definitively diagnosed based only on histological findings.Citation22
Ultrasound, CT, or magnetic resonance imaging is useful for delineating the location, while 18F-FDG-PET helps to estimate malignant, multiple, and metastatic lesions.Citation23,Citation24 In this case, the vaginal mass was not found by ultrasound, probably because it was not examined by transvaginal ultrasound, although it unusual hypermetabolism of FDG under PET/CT appeared, which matched with the tumor’s features. It has been reported that 123I-metaiodobenzylguanidine has strong affinity to chromaffin cell tissues when used as tracer imaging to effectively diagnose or locate paraganglioma. However, this detection technology had not been widely used.Citation25 Moreover, an assay of catecholamine and noradrenaline in blood and urine also helped to diagnosis paraganglioma. Patients with functional nonchromaffin paraganglioma may have an increase of catecholamine and noradrenaline in blood and urine, along with blood pressure elevation.Citation26 Such information was not available in this case.
Whenever it comes to either functional or nonfunctional vaginal paraganglioma, all the literature suggests that surgical operation currently seems to be the most effective treatment. Because it cannot be completely determined as functional vaginal paraganglioma before operation, the perioperative period is very important.Citation27 Usually, an α-receptor antagonist is used for catecholamine inhibition. It has been reported that interventional embolization of uterine artery was carried out in one case.Citation18 During the operation of the uterine artery, fluctuation of blood pressure, arrhythmia, pneumonedema, myocardial ischemia, or shock may be life-threatening. Those complications can be decreased to 3% by sufficient preoperative preparation.Citation28
It is widely recognized that paraganglioma is a slowly growing tumor, with no or low latent malignancy. However, it cannot be determined just by histological morphology. Instead, it should be judged malignant on the bases of neoplasm recurrence, metastasis of lymph nodes or nonchromaffin tissues, and invasion or infiltration to the adjacent apparatus.Citation29–Citation31 Due to the possibility of neoplasm recurrence and metastasis, as reported, patients need periodic checks and long-term follow-up.Citation27,Citation31 In this case, the woman had complete resection of the tumor as well as vaginal reconstruction performed. Repeat CT examination did not reveal any local recurrence or distant metastasis during the 12-month follow-up period. We suggested the patient have a yearly pelvic CT scan and gynecological examination.
Acknowledgments
This work was supported by Chongqing Medical Scientific Research Projects (grant 2013-2-026).
Disclosure
The authors report no conflicts of interest in this work.
References
- DeLellisRALloydRHeitzPUEngCPathology and Genetics: Tumours of Endocrine OrgansLyonIARC2004
- RenardJClericiTLickerMTriponezFPheochromocytoma and abdominal paragangliomaJ Visc Surg2011148e409e41621862435
- KshirsagarAYDombateVDVinchurkarKMPareekVARetroperitoneal para-aortic paragangliomaInt Surg20059014114316466001
- EricksonDKudvaYCEbersoldMJBenign paragangliomas: clinical presentation and treatment outcomes in 236 patientsJ Clin Endocrinol Metab2001865210521611701678
- LuconAMFalciRJrPraxedesJNMulticentric pheochromocytoma and involvement of the inferior vena cavaSao Paulo Med J2001119868811276173
- LackEFWienekeJAParagangliomasCarterDGreensonJKReuterVEStolerMHSternberg’s Diagnostic Surgical Pathology3rd edPhiladelphiaLippincott Williams & Wilkins19992625648
- MahdaviASilberbergBMalviyaVKBraunsteinAHShapiroJGangliocytic paraganglioma arising from mature cystic teratoma of the ovaryGynecol Oncol20039048248512893225
- AlamowitchBMaussetVRuizAPhéochromocytome non sécrétant du ligament large révélé par une péritonite appendiculaire [Non-secreting pheochromocytoma of the broad ligament revealed by appendicular peritonitis]Presse Med199928225228 French10076596
- AronDCMarksWMAlperPRKaramJHPheochromocytoma of the broad ligament. Localization by computerized tomography and ultrasonographyArch Intern Med19801405505527362392
- BehamASchmidCFletcherCDAuböckLPickelHMalignant paraganglioma of the uterusVirchows Arch A Pathol Anat Histopathol19924204534571595196
- IsambertNGrosPCommegeillePParagangliome malin de l’uterus [Malignant paraganglioma of the uterus]Ann Med Interne (Paris)2000151311313 French10922962
- ColanTJDardickIO’ConnellGParaganglioma of the vulvaInt J Gynecol Pathol1991102032081709625
- YoungTWThrasherTVNonchromaffin paraganglioma of the uterus. A case reportArch Pathol Lab Med19821066086096897169
- ChishimaFTamuraMNakazawaTParaaortic paraganglioma arising in an ovarian carcinoma patient mimicking lymph node metastasisJ Obstet Gynaecol Res20103620420820178553
- HassanABennetABhallaSParaganglioma of the vagina: report of a case, including immunohistochemical and ultrastructural findingsInt J Gynecol Pathol20032240440614501825
- ParkesSERaafatFMorlandBJParaganglioma of the vagina: the first report of a rare tumor in a childPediatr Hematol Oncol1998155455519842649
- ShenJGChenYXXuDYFengYFTongZHVaginal paraganglioma presenting as a gynecologic mass: case reportEur J Gynaecol Oncol20082918418518459561
- AklMNNaiduSGMcCulloughAEMagtibayPMVaginal paraganglioma presenting as a pelvic massSurgery201014716917119744428
- BrustmannHParaganglioma of the vagina: report of a casePathol Res Pract200720318919217298868
- LandsbergLYoungJBPheochromocytomaFauciASBratunwaldEIsselbacherKJHarrison’s Principles of Internal Medicine14th edNew YorkMcgraw-Hill199820572060
- YoungWFJrParagangliomas: clinical overviewAnn N Y Acad Sci20061073212917102068
- CostantiniECochettiGPorenaMVaginal para-urethral myxoid leiomyoma: case report and review of the literatureInt Urogynecol J Pelvic Floor Dysfunct2008191183118518351279
- SahdevASohaibAMonsonJPGrossmanABChewSLReznekRHCT and MR imaging of unusual locations of extra-adrenal paragangliomas (pheochromocytomas)Eur Radiol200515859215290072
- RoyoPde LuisEManeroMGVellosoMJToledoGAlcázarJLPelvic paragangliomaJ Ultrasound Med20072626126517255192
- Var der HarstEde HerderWWBruiningHA[(123)I] metaiodobenzy and [(111)In] octreotide uptake in benign and malignant pheochromocytomasJ Clin Endocrinol Metab20018668569311158032
- LendersJWEisenhoferGMannelliMPacakKPhaeochromocytomaLancet200536666567516112304
- KazicMRZivaljevicVRMilanZBPaunovicIRPreoperative risk factors, morbidity and outcome of 145 patients during phaeochromocytoma resectionActa Chir Belg201111122322721954738
- WaldOShapiraOMMurarAIzharUParaganglioma of the mediastinum: challenges in diagnosis and surgical managementJ Cardiothorac Surg201051920356401
- AlvarengaCALopesJMVinagreJParaganglioma of seminal vesicle and chromophobe renal cell carcinoma: a case report and literature reviewSao Paulo Med J2012130576022344361
- ParkJSongCParkMPredictive characteristics of malignant pheochremocytomaKorean J Urol20115224124621556209
- FooSHChanSPAnandaVRajasingamVDopamine-secreting phaeochromocytomas and paragangliomas: clinical features and managementSingapore Med J201051e89e9320593136