
Abstract
Background and aim
Limited-stage combined small cell esophageal carcinoma (LS-C-SCEC) is a rare, poorly understood, underdiagnosed disease, with components of both small cell esophageal cancer and non–small cell esophageal cancer. We investigated the optimal treatment strategy and prognostic factors in patients with LS-C-SCEC.
Patients and methods
LS-C-SCEC patients included in the analysis (from our hospital and the literature) were treated between January 1966 and December 2013. Patient treatment strategies included surgery (S), chemotherapy (CT), and radiation therapy (RT). The primary end point was overall survival (OS); the secondary end points included tumor complete response rates, patterns of failure, and toxicity. Kaplan–Meier curves were compared with the log-rank test. Univariate and multivariate analyses were used to determine prognosticators for OS.
Results
A total of 72 patients were included in the analysis: 24 (33%) from our hospital and 48 (67%) from the literature. The median OS of all patients was 15.0 months. Patients who received CT had a significantly longer median OS than did those who did not (OS 22.8 months vs 10.0 months) (P=0.03). Patients treated with multimodality therapy (including RT+CT [18%], S+CT [40%], or S+RT+CT [17%]) vs monotherapy (typically, S [18%]) had significantly improved OS (15.5 months vs 9.3 months) (P=0.02) and complete response rates. On multivariate analysis, tumor location (upper third of the esophagus) and type of treatment (monotherapy) were the only factors predictive of poor OS.
Conclusion
Multimodality therapy (including RT+CT, S+CT, or S+RT+CT) improves OS for patients with LS-C-SCEC compared with monotherapy (typically, S). Additional studies are necessary to personalize multimodal treatment approaches to individual patients.
Introduction
The esophagus is the main site of extrapulmonary small cell carcinoma, and primary small cell esophageal carcinoma (SCEC) represents 1.0% to 2.8% of all esophageal cancers.Citation1,Citation2 The incidence of SCEC is highest in Southeast Asian countries, including Japan, Korea, and the People’s Republic of China.Citation3,Citation4 SCEC is similar to small cell lung cancer (SCLC) in that both have a high frequency of regional and distant spread at time of diagnosis and a poor overall prognosis.Citation5,Citation6
The term “combined SCEC” (C-SCEC) is defined by World Health Organization (WHO) as SCEC with an additional component of non–small cell carcinoma, including squamous cell carcinoma, adenocarcinoma, or other carcinoma. Limited-stage (LS) C-SCEC (LS-C-SCEC) is currently considered a subset of SCEC, although biologic evidence to support this classification scheme is lacking. An accurate understanding of LS-C-SCEC is of great practical importance; its optimal treatment strategy may be different than that of pure SCEC,Citation4,Citation7–Citation9 neuroendocrine esophageal carcinoma,Citation10 or non-SCEC,Citation11 akin to pure SCLC and combined SCLC (C-SCLC).Citation12,Citation13
Evidence behind the optimal therapeutic approaches to LS-C-SCEC is limited because of (1) the infrequency of the disease; (2) various treatment strategies (including surgery [S], chemotherapy [CT], radiotherapy [RT], and combinations of these treatments) have been reported to have similar outcomes;Citation4 and (3) the prognosis for pure SCEC and C-SCEC is reportedly similar.Citation4 Our previous study demonstrated that patients with pure LS-SCEC treated with RT+CT had an improved survival compared with those treated with S+CT.Citation8 We believe LS-C-SCEC is a unique disease, and its optimal management may be different than that of LS-SCEC. Therefore, we performed a retrospective study to evaluate the clinical features, optimal treatment strategy, and prognostic factors in patients with LS-C-SCEC.
Patients and methods
Study design and patient eligibility
Eligible patients with LS-C-SCEC were recruited from our hospital and the literature.Citation2,Citation5,Citation9,Citation14–Citation31 The inclusion criteria were: (1) a pathological diagnosis of primary LS-C-SCEC; (2) treatment, including S, RT, CT, or a combination of these; and (3) a report of overall survival (OS) time. The exclusion criteria for patients were as follows: (1) a diagnosis of pure esophageal carcinomas (eg, squamous cell carcinoma, adenocarcinoma, or small cell carcinoma); (2) a diagnosis of extensive stage C-SCEC; (3) uncontrolled comorbid conditions (metabolic or psychiatric); and (4) an unreported OS time. The study protocol was in accordance with the ethical guidelines of the 1995 Declaration of Helsinki and was approved by independent ethics committees at Tianjin Medical University Cancer Institute and Hospital.
Literature search strategy and data extraction
We searched MEDLINE for patients treated for SCEC between January 1966 and December 2013. A preliminary search was designed to find all articles including the terms “small cell carcinoma” or “oat cell carcinoma” combined with “esophagus” or “esophageal.” Three reviewers independently selected the patients and performed the data extraction, from these articles and their references. Discrepancies regarding stated information in articles were resolved by discussion among reviewers. All principal investigators who initially included these patients were contacted using the corresponding e-mail addresses listed in the respective studies. The message sent to the authors both acknowledged their original work and asked for permission to include their patients in the current study. Of the authors without functioning addresses, none objected to having his/her patients included in the current study. Further, principal investigators were asked to supplement information that was missing from the original publication.
Treatment schedule
S was defined as radical resection of the primary tumor and/or local lymphadenectomy. RT was administered with conventional fields (two anterior–posterior opposed fields and two anterior–posterior [AP-PA] oblique opposed fields), three-dimensional (3D) conformal radiotherapy (3D-CRT), or intensity-modulated radiotherapy (IMRT). Data gathered about CT included agent(s) used and number of CT cycles.
Outcome measurements and end points
The primary outcome was OS. Secondary outcomes included tumor response rate (complete response [CR] and partial response [PR], clinically assessed at the time of follow up), pattern of failure (eg, locoregional recurrence [LRR] and distant metastasis [DM]), and treatment toxicity. OS was defined as the time between date of pathological diagnosis and date of death. The patients taken from literature who were alive at the reported time of communication were coded as being lost to follow up.
Statistical analysis
A χ2 test or Fisher’s exact test were performed for qualitative data. OS curves were estimated by using the Kaplan–Meier technique and compared using the stratified log-rank test. Univariate analysis (UVA) and multivariate analysis (MVA) were performed using a Cox regression model. Predictors analyzed included sex, age (≤60 vs >60 years), tumor location (upper vs middle vs lower third), tumor size (≤5 vs >5 cm), combined additional components (squamous cell carcinoma vs adenocarcinoma vs others, and their combinations), the number of additional histological components (one vs two or more), CT regimen (platinum- vs non-platinum-based), and type of treatment (monotherapy vs combination therapy). Data were analyzed using Intercooled Stata, version 8.2 for Windows (Stata Corp, College station, TX, USA), with a P-value of <0.05 considered significant.
Results
Patient characteristics
A total of 72 patients were included in the analysis: 24 patients (33%) from our hospital and 48 patients (67%) from 21 publications.Citation2,Citation5,Citation9,Citation14–Citation31 The baseline characteristics of all patients are shown in . The characteristics of patients from our institution are summarized in . Among the 17 patients who underwent monotherapy, 13 (18%) were treated with S, two (3%) with CT, and two (3%) with RT. A total of 55 patients underwent multimodality therapy, including 13 (18%) patients who received CT+RT, 29 (40%) who received S+CT, one (1%) who received S+RT, and 12 (17%) who received S+CT+RT.
Table 1 Patient characteristics
Table 2 Patient characteristics, for study patients treated at our hospital
Overall survival
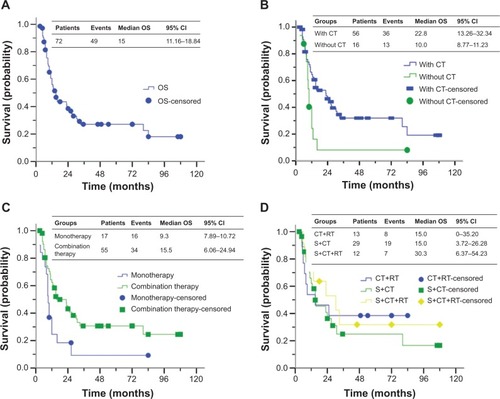
All patients were followed until death or December 2013. The median follow-up time was 15.0 (range 3–108) months. For the whole cohort, the median OS was 15.0 months; the 1-year, 2-year, and 3-year OS rates were 56%, 39%, and 27%, respectively (). Compared with patients without CT, patients with CT had significantly improved median OS (10.0 months vs 22.8 months) (P=0.03) (). Patients who received multimodality therapy (eg, RT+CT, S+CT, S+RT, or S+RT+CT) had significantly improved OS compared with those who received monotherapy with any technique (15.5 months vs 9.3 months) (P=0.02) (). The survival time showed a slight trend towards superiority of S+CT+RT over CT+RT or S+CT, although these differences were not statistically significant because of the small sample (P=0.73) ().
Figure 1 OS of patients with LS-C-SCEC.
Abbreviations: CI, confidence interval; CT, chemotherapy; LS-C-SCEC, limited-stage combined small cell esophageal carcinoma; OS, overall survival; RT, radiotherapy; S, surgery.
Tumor response and patterns of failure
There were 56 patients had reported tumor response. A total 19 (19/56 [34%]) and 37 patients (37/56 [66%]) had a CR and PR, respectively. Among the 19 patients with CR, the treatment modality was S alone (1/19 [5%]), CT+RT (1/19 [5%]), S+CT (12/19 [63%]), and S+CT+RT (5/19 [27%]). Among the 37 patients with PR, the treatment modality was S alone (11/37 [30%]), CT+RT (2/37 [5%]), S+CT (19/37 [51%]), RT (1/37 [3%]), and S+CT+RT (4/37 [11%]).
A total 25 patients (25/72 [35%]) had reported patterns of failure: LRR without DM (8/44 [18%]); DM without LRR (12/44 [27%]); or LRR and DM (5/44 [11%]). Of the 17 patients who had DM, the most frequent sites were liver (6/17 [35%]), lung (3/17 [18%]), lymph nodes (3/17 [18%]), bone (2/17 [12%]), brain (1/17 [6%]), and diffuse metastasis (2/17 [12%]).
Prognostic factors
Patient clinical characteristics were evaluated to determine their prognostic value in terms of OS. UVA indicated that sex, age, tumor size, tumor/nodes/metastasis (TNM) classification stage, types of histological components, number of histological components, and CT type were not associated with OS (). UVA and MVA revealed that tumor location (upper third of the esophagus) and type of treatment (ie, monotherapy) were associated with worse OS ( and ).
Table 3 Univariate analysis of the prognostic factors for survival in patients with LS-C-SCEC
Table 4 Multivariate Cox regression analysis of predictors for OS in patients with LS-C-SCEC
Adverse events
Of all patients, only five (5/72 [7%]) patients had a reported adverse event secondary to treatment. All toxicities were minor (Radiation Therapy Oncology Group [RTOG] grade ≤2) and included esophagitis, leukopenia, anemia, thrombocytopenia, and bone marrow suppression. And these toxicities were resolved with routine treatment.
Discussion
LS-C-SCEC is a rare subtype of SCEC. The optimal treatment strategy for LS-C-SCEC is controversial. Previous studies have suggested that pure LS-SCEC and LS-C-SCEC have similar behavior and outcomes, perhaps independent of treatment.Citation4,Citation32 However, most of these reports are relatively small retrospective series, and LS-C-SCEC has been included as a subset of patients with LS-SCEC. The current retrospective study demonstrated that LS-C-SCEC should be treated as a unique disease entity. Moreover, LS-C-SCEC patients who received multimodality therapy (which included CT) have significantly improved OS compared with patients receiving monotherapy.
Generally, the size of biopsy and presence of crush artifact, as well as number of study specimens taken by routine biopsy contribute to the underdiagnosis of C-SCEC.Citation4,Citation33 In addition, change in histology during the treatment period also makes the diagnosis more challenging,Citation34 akin to C-SCLC.Citation35 In this study, the vast majority (55/72 [76%]) of patients were diagnosed by postoperative pathology, which illustrates the importance of histopathological diagnosis. Therefore, it is postulated that the incidence of C-SCEC may be underestimated. In this study, the most frequent histological component was squamous cell carcinoma, in agreement with a previous report.Citation36 The coexistence of pure SCEC with squamous cell carcinoma or other histologies in the same lesion is supported by the hypothesis that SCEC originates from amine precursor uptake and decarboxylation (APUD) cells or pluripotent stem cells.Citation37
We believe that the rarity of LS-C-SCEC is the primary reason that there is a lack of consensus regarding its optimal treatment. From a clinical standpoint, our data indicate that LS-C-SCEC has historically been treated similar to non-SCEC, in that S has been an integral treatment approach for LS-C-SCEC (76% of cases) and LS-SCEC.Citation8 Additionally, we note that patients with pure LS-SCEC have significantly improved OS compared with LS-C-SCEC.Citation8 The reason for this OS discrepancy is unclear and may be attributed to the fact that small cell carcinoma is typically more radiosensitive than non-SCEC or that the presence of a combined histology is secondary to multiple tumor cell lines.
Compared with LS-C-SCEC patients treated without CT, our results suggest that patients treated with CT have a significantly improved OS. We believe CT is a necessary treatment for both pure SCEC and C-SCEC, akin to patients with SCLC and C-SCLC. In addition, our study demonstrated that multimodality therapy (which includes CT) is associated with improved OS versus monotherapy. The survival time showed a slight trend towards the superiority of S+CT+RT over CT+RT or S+CT, although these differences were not statistically significant because of fewer samples. Previous studies were consistent with our results, although these studies did not strictly focus on C-SCEC compared with other histologies.Citation10,Citation11,Citation38
RT is important in the treatment of small cell carcinoma and non–small cell carcinoma of other disease sites. In this study, a total of 28 patients (28/72 [39%]) received RT, either alone or in combination with S or CT. The indications and contraindications for RT (particularly as trimodality therapy with S and CT) in LS-C-SCEC should be evaluated in future prospective works.
Differences between pure SCEC and C-SCEC in terms of disease biology and pattern of metastatic spread constitute the subject of ongoing debate, and it is hypothesized that the C-SCEC has diverse biological characteristics that may influence tumor aggressiveness and treatment sensitivity. Our previous study demonstrated that the CRs were more likely to be seen in patients with pure SCEC who received RT+CT (100%) vs S+CT (88%);Citation8 in the current work, CRs were more likely to be seen in patients who received CT in combination with other treatment (18/19 [95%]), but not RT and/or S (1/19 [5%]). CT appears to be an important treatment modality for both pure SCEC and C-SCEC, as evidenced by rates of CR and OS.
Interestingly, there was a significant difference in the pattern of failure (ie, LRR and DM) between pure patients with LS-SCEC (LRR and DM [76%]) and LS-C-SCEC (LRR and DM [35%]). The incidence of brain metastasis appears to be low in either disease; thus, prophylactic brain irradiation for LS-C-SCEC appears unnecessary.
Previous works have shown that the adverse prognostic factors for SCEC are advanced stage of the disease, tumor location, patient’s performance status, and treatment type.Citation2,Citation5,Citation9,Citation14–Citation31 In the present study, UVA and MVA identified two independent negative prognostic factors of LS-C-SCEC: tumor location (upper third of the esophagus) and type of treatment (monotherapy, which was typically, S). Additionally, although previous reports have identified the number of histological components to be predictive of outcome in C-SCLC,Citation12,Citation13,Citation39 the present study did not identify histology (either count or subtype) as a predictor of outcome for LS-C-SCEC.
This study has potential weaknesses. First, it is retrospective and based largely on records kept by many institutions, which may have been heterogeneous in their diagnosis and management of patients. Second, the sample size of the present study may not have been optimal; however, LS-C-SCEC is a rare and likely underdiagnosed disease of patients, particularly during the past few decades when the patients were treated. Third, CT, RT, and S have differed widely and have evolved. Finally, some patient data were missing, and with a relatively small number of patients overall, we are unable to discuss the benefit of certain treatments (eg, concurrent vs sequential CT, or salvage therapy).
In conclusion, this study indicates that LS-C-SCEC is a unique disease that should be diagnosed and managed as an entity separate from LS-SCEC. Compared with monotherapy, multimodality therapy (which includes CT) is associated with improved OS for patients with LS-C-SCEC. We recommend that S+CT+RT, S+CT, or CT+RT should be considered as possible treatment approaches for LS-C-SCEC patients.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (grant number 81201754), the New Teacher Fund for Doctor Station, the Ministry of Education (grant number 20121202120014), the National Natural Science Foundation of China (grant numbers 81472797 and 81201753), and the Foundation of National Clinical Research Center for Cancer (grant number N14B04).
In particular, we would like to acknowledge the work of Drs K Takubo, K Sasajima, SJ Walker, M Mori, I Muto, SR Craig, F Casas, T Nishimaki, AR Poynton, K Shimizu, M Mitani, GH Pantvaidya, H Makino, J Yamamoto, M Furihata, YP Yun, GY Yu, K Chin, F Bibeau, T Terada, and J Li. We also thank the anonymous referee for his/her very helpful comments, which remarkably improved the quality of this paper.
Disclosure
The abstract of this paper was presented at the American Society for Radiation Oncology 56th Annual Meeting as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the journal International Journal of Radiation Oncology Biology Physics. The full paper has never been published.
The authors report no conflicts of interest in this work.
References
- HuncharekMMuscatJSmall cell carcinoma of the esophagus. The Massachusetts General Hospital experience, 1978 to 1993Chest199510711791817813272
- CraigSRCareyFAWalkerWSCameronEWPrimary small cell cancer of the esophagusJ Thorac Cardiovasc Surg19951092842887531797
- BriggsJCIbrahimNBOat cell carcinomas of the oesophagus: a clinico-pathological study of 23 casesHistopathology1983722612776133829
- CasasFFerrerFFarrúsBCasalsJBieteAPrimary small cell carcinoma of the esophagus: a review of the literature with emphasis on therapy and prognosisCancer1997808136613729338459
- PantvaidyaGHPrameshCSDeshpandeMSJambhekarNASharmaSDeshpandeRKSmall cell carcinoma of the esophagus: the Tata Memorial Hospital experienceAnn Thorac Surg20027461924192712643374
- BrennerBTangLHKlimstraDSKelsenDPSmall-cell carcinomas of the gastrointestinal tract: a reviewJ Clin Oncol200422132730273915226341
- LvJLiangJWangJPrimary small cell carcinoma of the esophagusJ Thorac Oncol20083121460146519057273
- MengMBZaorskyNGJiangCRadiotherapy and chemotherapy are associated with improved outcomes over surgery and chemotherapy in the management of limited-stage small cell esophageal carcinomaRadiother Oncol2013106331732223498325
- TakuboKNakamuraKSawabeMPrimary undifferentiated small cell carcinoma of the esophagusHum Pathol199930221622110029452
- MaruDMKhuranaHRashidARetrospective study of clinicopathologic features and prognosis of high-grade neuroendocrine carcinoma of the esophagusAm J Surg Pathol20083291404141118670347
- GamlielZKrasnaMJMultimodality treatment of esophageal cancerSurg Clin North Am20058562163015927656
- SamsonDJSeidenfeldJSimonGRAmerican College of Chest PhysiciansEvidence for management of small cell lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition)Chest20071323 Suppl314S323S17873177
- SgambatoACasaluceFMaionePMedical treatment of small cell lung cancer: state of the art and new developmentExpert Opin Pharmacother201314152019203123901936
- SasajimaKHayashiNYamashitaKOndaMTakuboKOat cell carcinoma of the esophagus with multiple differentiationJ Clin Gastroenterol19881066676712852698
- WalkerSJSteelACullenMHMatthewsHRTreatment of oesophageal small cell carcinoma by combined chemotherapy and surgical resection: report of two cases and review of published casesThorax19894497517522555933
- MoriMMatsukumaAAdachiYSmall cell carcinoma of the esophagusCancer19896335645732536291
- MutoINishimakiTAizawaKSuzukiTTanakaOHatakeyamaKPrimary small cell carcinoma of the esophagus: report of a caseSurg Today19952598308338555704
- CasasFFarrúsBDanielsMSix-year follow-up of primary small cell carcinoma of the esophagus showing a complete response: a case reportJpn J Clin Oncol19962631801848656561
- NishimakiTSuzukiTNakagawaSWatanabeKAizawaKHatakeyamaKTumor spread and outcome of treatment in primary esophageal small cell carcinomaJ Surg Oncol19976421301349047250
- PoyntonARWalshTNKellyAHarneyMStuartRDalyPAHennessyTPSmall cell carcinoma of the oesophagusEur J Surg Oncol19972365095129484920
- ShimizuKTakiyamaWMandaiKTanadaMKawabuchiYHeikeYUndifferentiated carcinoma with lymphoid infiltration of the esophagus: a case reportJpn J Clin Oncol1999291049449710645805
- MitaniMKuwabaraYShinodaNSatoAFujiiYLong-term survivors after the resection of limited esophageal small cell carcinomaDis Esophagus200013325926111206646
- MakinoHTajiriTOndaMEffectiveness of preoperative chemotherapy using carboplatin (CBDCA) and surgery against an esophageal small cell carcinomaDis Esophagus200215323724112444997
- YamamotoJOhshimaKIkedaSIwashitaAKikuchiMPrimary esophageal small cell carcinoma with concomitant invasive squamous cell carcinoma or carcinoma in situHum Pathol200334111108111514652811
- FurihataMOnoYFujimoriTEsophageal small cell carcinoma effectively treated by cisplatin and irinotecanEsophagus2006326164
- YunJPZhangMFHouJHPrimary small cell carcinoma of the esophagus: clinicopathological and immunohistochemical features of 21 casesBMC Cancer200773817335582
- KuGYMinskyBDRuschVWBainsMKelsenDPIlsonDHSmall-cell carcinoma of the esophagus and gastroesophageal junction: review of the Memorial Sloan-Kettering experienceAnn Oncol200819353353717947223
- ChinKBabaSHosakaHIrinotecan plus cisplatin for therapy of small-cell carcinoma of the esophagus: report of 12 cases from single institution experienceJpn J Clin Oncol200838642643118519543
- BibeauFChateauMCGuiuMSmall cell carcinoma with concomitant adenocarcinoma arising in a Barrett’s oesophagus: report of a case with a favourable behaviourVirchows Arch2008452110310718008084
- TeradaTMaruoHEsophageal combined carcinomas: Immunohoistochemical and molecular genetic studiesWorld J Gastroenterol201218131545155122509088
- LiJChenXShenYA rare collision tumor of squamous carcinoma and small cell carcinoma in esophagus involved with separate lymph nodes: a case reportJ Thorac Dis201355E203E20624255793
- KukarMGromanAMalhotraUSmall cell carcinoma of the esophagus: a SEER database analysisAnn Surg Oncol201320134239424423943025
- VosBRozemaTMillerRCSmall cell carcinoma of the esophagus: a multicentre Rare Cancer Network studyDis Esophagus201124425826421073624
- FushimiHKikuiMMorinoHHistologic changes in small cell lung carcinoma after treatmentCancer19967722782838625235
- HageRElbersJRBrutel de la RivièreAvan den BoschJMSurgery for combined type small cell lung carcinomaThorax19985364504539713442
- WangSYMaoWMDuXHXuYPZhangSZThe 2002 AJCC TNM classification is a better predictor of primary small cell esophageal carcinoma outcome than the VALSG staging systemChin J Cancer201332634235223114087
- HoKJHerreraGAJonesJMAlexanderCBSmall cell carcinoma of the esophagus: evidence for a unified histogenesisHum Pathol19841554604686327495
- ZhuYQiuBLiuHPrimary small cell carcinoma of the esophagus: review of 64 cases from a single institutionDis Esophagus201427215215823639106
- BabakoohiSFuPYangMLindenPADowlatiACombined SCLC clinical and pathologic characteristicsClin Lung Cancer201314211311923010092