
Abstract
Malignant fibrous histiocytoma (MFH) is the most common soft-tissue sarcoma in late adult life. Unfortunately, advanced MFH has a poor prognosis due to a lack of effective drugs. We present here a case of advanced MFH with partial response to apatinib, a new potent oral small-molecule tyrosine kinase inhibitor targeting the intracellular domain of vascular endothelial growth factor receptor 2 (VEGFR-2). To the best of our knowledge, this is the first case report using apatinib for MFH. Quantitative polymerase chain reaction analysis revealed high expression of VEGFR-2 mRNA, suggesting that apatinib leads to clinical response by inhibiting VEGFR-2 tyrosine kinase activity and the crucial role of VEGFR-2 for MFH. Apatinib could be a new option for the treatment of MFH. Further studies are needed to optimize the treatment.
Introduction
Malignant fibrous histiocytoma (MFH), originated from mesenchymal cells, is the most common soft-tissue sarcoma (STS) in late adult life. It frequently occurs in deep soft tissues of the extremities (70%).Citation1
Standard treatment guidelines for MFH do not exist currently. Surgical management remains the main treatment. Unfortunately, approximately 40% of patients will develop local recurrences or distant metastases.Citation2 The 5-year survival rate is 10%–30% if MFH is only treated locally.Citation3 Radiotherapy and chemotherapy in adjuvant settings has only limited effectiveness.Citation4 For advanced MFH, the prognosis of MFH remains very poor, even with combined, multimodal therapy. There is an urgent need for novel effective agents.
Apatinib (Hengrui Pharmaceutical Co., Ltd, Shanghai, People’s Republic of China) is a novel oral small-molecule tyrosine kinase inhibitor (TKI) targeting the intracellular domain of vascular endothelial growth factor receptor-2 (VEGFR-2). It has shown a survival benefit in gastric cancer in a Phase III trial and non-small-cell lung cancer in a Phase II trial and is currently being studied in multiple tumor types. Because of low side effects and improved outcomes, apatinib has demonstrated a substantial potential to be a new therapeutic option in a variety of tumor types.Citation5
We here report a case of MFH on the right forearm with partial response (PR) to apatinib. To the best of our knowledge, this is the first case of MFH that responded to apatinib.
Case report
In May 2013, a 78-year-old male came to our hospital with an irregular soft-tissue mass on the right forearm over 1 year, with an area of approximately 6.0 cm × 5.0 cm.
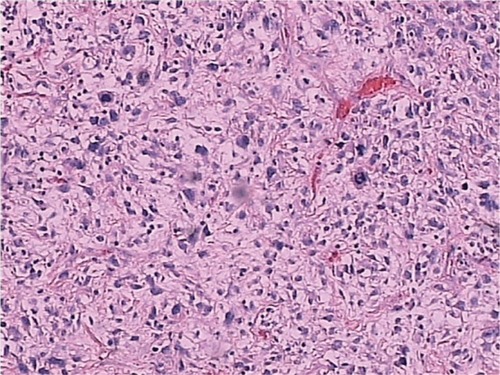
The biopsy from the lesions was taken, and histopathologic examination revealed MFH. The presence of distal metastases was ruled out by chest and abdominal computed tomography (CT) at that time. However, the patients did not receive surgical excision until December 23, 2013, for personal reasons. The mass was found between skin and fascia at operation, with a volume of 5 cm × 4 cm × 3 cm. However, complete resection was not achieved because of nerve infiltration. The postoperative pathology revealed positive surgical margins on the edge of the skin and the basal layer of epithelium. Pathology diagnosis confirmed MFH (mostly myxofibrosarcoma, some pleomorphic forms; ) with immunophenotype: Vimentim(3+), AAT(2+), AE1/AE3(−), CD34(3+), SMA(−), Bcl2(±), S100(−), Desmin(−), LCA(−), ALK(−), CD30(−), β-catenin(+), CD68(+).
Figure 1 Hematoxylin and eosin staining of a tumor section (x200).
The patient was then referred to a radiation oncologist to receive a total of 60 Gy of intensity modulation radiated therapy.
One year after the operation, chest CT (December 10, 2014) revealed multiple lung nodules, considering the possibility of metastases. Whole-body positron emission tomography (PET)/CT further confirmed multiple lung metastases with increased glucose metabolism without local recurrence and metastases in other parts of the body. The patient refused to receive cytotoxic chemotherapy, instead opting for some traditional Chinese medicine because of old age and poor performance status (PS). One month later (November 10, 2014), chest CT revealed increased metastases.
Quantitative polymerase chain reaction of VEGFR-2 mRNA and gene sequencing of EGFR and KRAS were then performed, and the results revealed high expression of VEGFR-2 mRNA, wild-type EGFR, and wild-type KRAS.
By December 19, 2014, the patient had symptoms of intermittent expectoration and hemoptysis. Chest CT revealed an increased metastasis in the upper lobe of right lung and a significantly increased mass of approximately 9.3 cm in diameter at the lower right parahilar ().
Figure 2 Chest CT images showing metastases before (A and B) and after treatment with apatinib (C, D and E, F, respectively).
Abbreviation: CT, computed tomography.
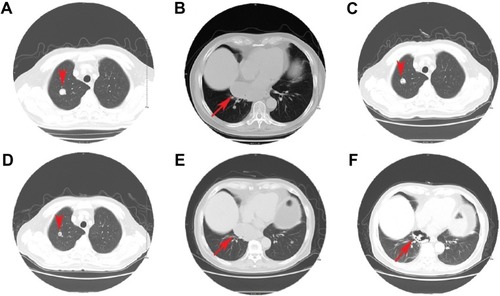
After the patient provided written, informed consent, apatinib was then administered with a dose of 500 mg/d on December 28, 2014. Following 2 months of targeted therapy, symptoms of expectoration reduced significantly and no hemoptysis appeared. Lung metastases were significantly reduced in size with some porosis, which was considered to be a PR (, respectively).
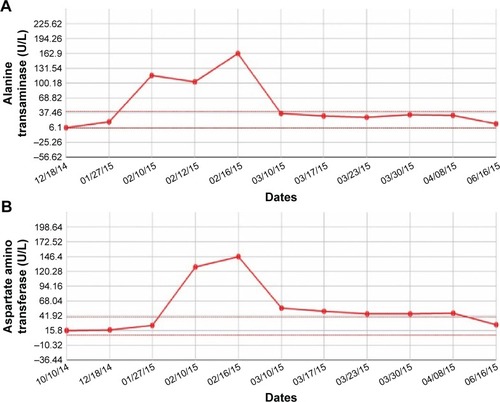
The toxicities the patient experienced were mainly non-hematological toxicities, including skin rash, short-lived elevated alanine transaminase (), and aspartate amino transferase (; grade 2; according to Common Terminology Criteria for Adverse Events v.4.03). No severe toxicities (grades 3–4) and other treatment-related adverse events were reported and detected.
Figure 3 Main toxicities during apatinib treatment.
The patient continued to use apatinib as maintenance therapy. A progression-free survival time of more than 6 months has been achieved and the patient is now still undergoing the apatinib treatment without major toxic effects.
Discussion
MFH is the commonest STS. It usually occurs in late adulthood with a slight predominance in males.Citation6
There are no standard treatment guidelines for MFH. Successful en-bloc resection of the tumor is the principal treatment and is the most important prognostic factor.Citation7 The role of adjuvant chemotherapy and radiation is limited and controversial. Even with en bloc resection (better results than debulking surgery in terms of survival),Citation8 many patients suffered from metastases to lungs, bone, liver, and skin.Citation9
In the advanced stage, the standard treatment is chemotherapy. Regimens are primarily based on doxorubicin and ifosfamide as first-line treatment, either alone or in combination. Approximately 30% of patients treated with doxorubicin-based therapy or ifosfamide-based therapy achieve an objective response.Citation10 The combination of the two drugs could offer a response rate of approximately 30%–59% in patients with STS.Citation11 In a single institution study of 33 patients with STS, approximately 60% of patients treated with dose-intense doxorubicin and ifosfamide achieved an objective response, but 31%–56% of patients suffered from febrile neutropenia.Citation12 However, doxorubicin in combination with ifosfamide did not improve 1-year survival.Citation13
Other chemotherapy options in STS include either gemcitabine monotherapy or docetaxel and gemcitabine combination therapy.Citation14,Citation15 The activity of docetaxel monotherapy is quite limited. In a randomized Phase II study of docetaxel versus doxorubicin in first- and second-line chemotherapy for locally advanced or metastatic STS in Europe, no responses (0%) were seen in the docetaxel therapy arm, compared to the response rate of 30% in doxorubicin therapy arm.Citation14 Response rates of gemcitabine monotherapy in patients with advanced STS were reported to be 3%–20.5%, with median time to progression 1.5–13 months and median overall survival 6–15 months.Citation16–Citation18 Although with limited efficacy, docetaxel may have a synergistic action with gemcitabine when given before gemcitabine. In an open-label Phase II clinical trial with metastatic STS, the overall objective response rates were 16% (gemcitabine-docetaxel) and 8% (gemcitabine), with a response rate of 25% with gemcitabine and 36% with the combination for MFH, indicating that MFH is sensitive to both gemcitabine and the gemcitabine plus docetaxel combination.Citation19 However, combination of gemcitabine with docetaxel is potentially associated with significant toxicity. More than 50% of patients receiving the combination of gemcitabine and docetaxel discontinued treatment within 6 months, despite dose reductions.Citation20
Considering that the prevalence of MFH is highest in late adulthood, and that the toxicities of combined chemotherapy often leads to treatment cessation, MFH requires novel, effective, and safer treatment options, especially for the aged.
The advances in understanding the molecular mechanisms of malignancies have led to the development of targeted treatment options. Targeted TKIs represent a major treatment of choice. Several potential TKIs have been reported to be effective in the treatment of MFH, including sunitinib, sorafenib, and pazopanib.Citation21–Citation25 Moreover, preclinical data evidenced that imatinib could reduce tumor growth of MFH that express PDGFRs and c-Kit.Citation26 However, no case has been reported for apatinib in the treatment of MFH.
Apatinib is a novel oral small-molecule protein tyrosine kinase (RTK) inhibitor that selectively targets VEGFR-2, the primary VEGF family receptor driving angiogenesis.Citation27 VEGFR-2 binds all VEGF-A isoforms, VEGF-C and VEGF-D. The binding of VEGF-A to VEGFR-2 could induce a cascade of different signaling pathways such as PLC-γ-Raf kinase-MEK-MAP kinase and PI3K-AKT pathways, eventually causing cellular proliferation and endothelial-cell survival. A number of clinical trials have confirmed the efficacy of blockage of VEGFR-2 to be a promising strategy for inhibiting angiogenesis.Citation28 Apatinib has shown a survival benefit in gastric cancer in a Phase III trial and in a non-small-cell lung cancer in a Phase II trial in China, with a manageable toxicity profile.Citation5
In the Phase I study of apatinib, dose escalation was conducted in patients aged between 18 and 70 years. Hypertension and hand–foot syndrome were the two dose-limiting toxicities noted at dose level of 1,000 mg. Maximum tolerated dose was determined to be 850 mg once daily. The recommended dose of 750 mg once daily was well tolerated. The most frequently observed drug-related adverse events were hypertension (69.5%), proteinuria (47.8%), and hand–foot syndrome (45.6%).Citation29
In this case, the patient with MFH did not receive en bloc resection because of nerve infiltration. Although radiotherapy was performed, multiple lung metastases developed 1 year after the surgery. Because of old age and poor PS, the patient refused to accept any toxic chemotherapy, and apatinib monotherapy was then used to control the disease successfully with a PR.
Gene expression analysis revealed high expression of VEGFR-2 mRNA, suggesting that apatinib led to clinical response by inhibiting VEGFR-2 tyrosine kinase activity and the crucial role of VEGFR-2 for MFH. The administration of apatinib resulted in well-tolerated toxic profiles.
Conclusion
In conclusion, apatinib may provide an additional option for the treatment of MFH especially for the aged and patient with poor PS. Nevertheless, further large-scale prospective studies are required to improve the treatment of angiosarcoma.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
This case report was approved by the Medical Ethics Committee of the Navy General Hospital. Written informed consent was obtained from the patient for publication of this case report and accompanying images. The authors thank the patient for his participation and his agreement to publication of the report.
Disclosure
The authors report no conflicts of interest in this work.
References
- Abou-JaoudeMEl AliMMalignant fibrous histiocytoma: a case report and literature reviewInt Surg200994319620020187510
- WeitzJAntonescuCRBrennanMFLocalized extremity soft tissue sarcoma: improved knowledge with unchanged survival over timeJ Clin Oncol200321142719272512860950
- BacciGAvellaMPicciPThe effectiveness of chemotherapy in localized malignant fibrous histiocytoma (MFH) of bone: the Rizzoli Institute experience with 66 patients treated with surgery alone or surgery + adjuvant or neoadjuvant chemotherapyChemioterapia1988764064132851393
- EfeTHeyseTJSchoferMDFuchs-WinkelmannSRexinPSchmittJMalignant fibrous histiocytoma of the distal femur after an arthroscopic anterior cruciate ligament reconstruction: a case report and a review of the literatureBMC Cancer20101026420529315
- ScottAJMessersmithWAJimenoAApatinib: a promising oral antiangiogenic agent in the treatment of multiple solid tumorsDrugs Today (Barc)201551422322926020064
- PobirciDDBogdanFPobirciOPetcuCARoscaEStudy of malignant fibrous histiocytoma: clinical, statistic and histopatological interrelationRom J Morphol Embryol2011521 Suppl38538821424079
- TengHXinghaiYWeiHHuangQXiaoJZhangCMalignant fibrous histiocytoma of the spine: a series of 13 clinical case reports and review of 17 published casesSpine (Phila Pa 1976)20113622E1453E146221343863
- KawaharaNTomitaKMurakamiHDemuraSTotal en bloc spondylectomy for spinal tumors: surgical techniques and related basic backgroundOrthop Clin North Am20094014763vi19064055
- SerenoMMerinoMAguayoCA major response to trabectedin in metastatic malignant fibrous histiocytoma of the vertebra: a case report and review of the literatureTumori2013992e43e4823748828
- KanjeekalSChambersAFungMFVermaSSystemic therapy for advanced uterine sarcoma: a systematic review of the literatureGynecol Oncol200597262463715863170
- WeiZLiLXuXYA case of recurrent malignant fibrous histiocytoma with marked response to combined chemotherapy with gemcitabine and carboplatinArch Med Sci20141051057106025395962
- PatelSRVadhan-RajSBurgessMAResults of two consecutive trials of dose-intensive chemotherapy with doxorubicin and ifosfamide in patients with sarcomasAm J Clin Oncol19982133173219626808
- VermaSYounusJStys-NormanDHaynesAEBlacksteinMMeta-analysis of ifosfamide-based combination chemotherapy in advanced soft tissue sarcomaCancer Treat Rev200834433934718313854
- VerweijJLeeSMRukaWRandomized phase II study of docetaxel versus doxorubicin in first- and second-line chemotherapy for locally advanced or metastatic soft tissue sarcomas in adults: a study of the european organization for research and treatment of cancer soft tissue and bone sarcoma groupJ Clin Oncol200018102081208610811673
- SeddonBScurrMJonesRLA phase II trial to assess the activity of gemcitabine and docetaxel as first line chemotherapy treatment in patients with unresectable leiomyosarcomaClin Sarcoma Res201551325987978
- LookKYSandlerABlessingJALucciJA3rdRosePGPhase II trial of gemcitabine as second-line chemotherapy of uterine leiomyosarcoma: a Gynecologic Oncology Group (GOG) StudyGynecol Oncol200492264464714766260
- HartmannJTOechsleKHuoberJAn open label, non-comparative phase II study of gemcitabine as salvage treatment for patients with pretreated adult type soft tissue sarcomaInvest New Drugs200624324925316133789
- OkunoSRyanLMEdmonsonJHPriebatDABlumRHPhase II trial of gemcitabine in patients with advanced sarcomas (E1797): a trial of the Eastern Cooperative Oncology GroupCancer20039781969197312673725
- MakiRGWathenJKPatelSRRandomized phase II study of gemcitabine and docetaxel compared with gemcitabine alone in patients with metastatic soft tissue sarcomas: results of sarcoma alliance for research through collaboration study 002 [corrected]J Clin Oncol200725192755276317602081
- MakiRGGemcitabine and docetaxel in metastatic sarcoma: past, present, and futureOncologist2007128999100617766660
- CaspersenCSSosunovAUtkina-SosunovaIRatnerVIStarkovAATenVSAn isolation method for assessment of brain mitochondria function in neonatal mice with hypoxic-ischemic brain injuryDev Neurosci200830531932418349523
- MauriDPanouCValachisAKamposiorasKTsaliLTyrosine kinase inhibitors in treatment of fibrous histiocytomaExp Oncol2009311606119300420
- MakiRGD’AdamoDRKeohanMLPhase II study of sorafenib in patients with metastatic or recurrent sarcomasJ Clin Oncol2009271931333140 doi: 3110.1200/JCO.2008.3120.449519451436
- HeudelPCassierPDerbelOPazopanib for the treatment of soft-tissue sarcomaClin Pharmacol20124657023204874
- RajendraRJonesRLPollackSMTargeted treatment for advanced soft tissue sarcoma: profile of pazopanibOnco Targets Ther2013621722223524973
- IrsanIAkisueTHaraHImatinib mesylate inhibits tumorigenicity of malignant fibrous histiocytoma cells in vivoAnticancer Res2007271A42342917352263
- TianSQuanHXieCYN968D1 is a novel and selective inhibitor of vascular endothelial growth factor receptor-2 tyrosine kinase with potent activity in vitro and in vivoCancer Sci201110271374138021443688
- FontanellaCOngaroEBolzonelloSGuardascioneMFasolaGAprileGClinical advances in the development of novel VEGFR2 inhibitorsAnn Transl Med201521212325568876
- LiJZhaoXChenLSafety and pharmacokinetics of novel selective vascular endothelial growth factor receptor-2 inhibitor YN968D1 in patients with advanced malignanciesBMC Cancer20101052920923544