
Abstract
Purpose
To assess the efficacy of pemetrexed plus platinum doublet chemotherapy as first-line treatment for advanced nonsquamous non-small-cell lung cancer (NSCLC) through a trial-level meta-analysis.
Methods
Trials published between 1990 and 2015 were identified by an electronic search of public databases (Medline, Embase, and Cochrane Library). All clinical studies were independently identified by two authors. Demographic data, treatment regimens, objective response rate (ORR), progression-free survival (PFS), and overall survival (OS) were extracted and analyzed using comprehensive meta-analysis software (version 2.0).
Results
A total of 2,551 patients with advanced nonsquamous NSCLC from ten trials were included for analysis: 1,565 patients were treated with pemetrexed plus platinum doublet chemotherapy and 986 with platinum plus other first-line chemotherapy. Pooled ORR for pemetrexed plus platinum chemotherapy was 37.8% (95% confidence interval [CI]: 31.7%–44.3%), with median PFS and OS of 5.7 and 16.05 months, respectively. When compared to other platinum-based doublet chemotherapies, the use of pemetrexed plus platinum chemotherapy significantly improved OS (hazard ratio [HR] =0.86, 95% CI: 0.77–0.97, P=0.01) but not PFS (HR =0.90, 95% CI: 0.80–1.01, P=0.084) in advanced nonsquamous NSCLC patients.
Conclusion
Pemetrexed plus platinum doublet regimen is an efficacious treatment for advanced nonsquamous NSCLC patients. Our findings support the use of pemetrexed plus platinum doublet regimen as first-line treatment in advanced nonsquamous NSCLC patients because of its potential survival benefits.
Introduction
Lung cancer is the most common cause of cancer death worldwide.Citation1 Non-small-cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer cases, and approximately two-thirds of NSCLC patients are diagnosed with advanced disease, which cannot be successfully treated by surgery.Citation2 Currently, platinum combined with a third-generation agent (docetaxel, paclitaxel, gemcitabine, vinorelbine, and pemetrexed) is the standard treatment option for advanced NSCLC.Citation3–Citation6 However, NSCLC is a heterogeneous disease with respect to tumor histology, and those subtypes can be broadly categorized as squamous and nonsquamous. Recent clinical research related to histology has shown important differences within the population of patients with NSCLC.Citation7 In 2008, Scagliotti et alCitation8,Citation9 conducted a Phase III trial comparing first-line treatment using pemetrexed plus cisplatin with gemcitabine plus cisplatin and found that pemetrexed significantly improved overall survival (OS) in patients with nonsquamous histology (hazard ratio [HR] =0.81, 95% confidence interval [CI]: 0.70–0.94). However, in 2009, Gronberg et alCitation10 found that pemetrexed plus carboplatin provided similar OS when compared with gemcitabine plus carboplatin and that there was also no difference in OS when analyzing patients with nonsquamous histology (7.8 versus 7.5 months, P=0.77). As a result, whether pemetrexed plus platinum chemotherapy (PPC) is superior to other platinum-based doublet chemotherapy as first-line chemotherapy for advanced nonsquamous NSCLC patients remains unknown. To our best knowledge, there are no systematic review specially investigating the efficacy of PPC as first-line treatment for advanced nonsquamous NSCLC patients. We thus perform this study of published data to assess the efficacy of PPC in advanced nonsquamous NSCLC and compare the efficacy of PPC with other platinum-based doublet chemotherapy in those patients.
Materials and methods
Study design
We developed a protocol that defined inclusion criteria, search strategy, outcomes of interest, and analysis plan. The reporting of this systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statements.Citation11
Identification and selection of studies
To identify studies for inclusion in our systematic review and meta-analysis, we did a broad search of four databases, including Embase, Medline, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews, from the date of inception of every database to July 2015. The search included the following terms: “lung neoplasms”, “lung carcinoma”, “lung cancer”, “pemetrexed”, “first-line”, “chemotherapy naive”, “prospective study”, and “clinical trials”. Additional references were searched through manual searches of the reference lists and specialist journals. No language restrictions were applied.
To be eligible for inclusion in our systematic review and meta-analysis, study populations (referred to hereafter as cohorts) had to meet all the following criteria: 1) chemotherapy-naïve advanced nonsquamous NSCLC patients; 2) trials investigating the efficacy of PPC or comparing efficacy of PPC with other platinum-based doublet chemotherapy; 3) studies reporting outcomes of interest (ie, objective response rate [ORR], progression-free survival [PFS], and OS); and 4) reports from a prospective trial (ie, randomized controlled trial and nonrandomized clinical trial). If multiple publications of the same trial were retrieved or if there was a case mix between publications, only the most recent publication (and the most informative) was included.
Data extraction
Two investigators screened the titles and abstracts of potentially relevant studies. We retrieved the full text of relevant studies for further review by the same two reviewers. A third senior investigator resolved any discrepancies between reviewers. If reviewers suspected an overlap of cohorts in a report, they contacted the corresponding author for clarification; we excluded studies with a clear overlap.
The same pair of reviewers extracted study details independently, using a standardized pilot-tested form. A third investigator reviewed all data entries. We extracted the following data: author, study design, study period, median age, interventions (chemotherapy regimens and dose), sample size, and outcomes of interest. We defined outcomes of interest as ORR, PFS, and OS. The quality of reports of clinical trials was assessed and calculated using the 5-item Jadad scale including randomization, double-blinding, and withdrawals as previously described.Citation12
Statistical analysis
We prespecified the analysis plan in the protocol. We analyzed all patients who started PPC, regardless of their adherence to treatment. We calculated event rates of outcome (the proportion of patients who developed outcomes of interest) from the included cohorts for PPC groups. We pooled log-transformed event rates with DerSimonian and Laird random-effect models according to heterogeneity among studies.Citation13 We also pooled the overall HR for OS and PFS. A statistical test with a P-value <0.05 was considered significant. To measure overall heterogeneity across the included cohorts, we calculated the I2 statistic, with I2>50% indicating high heterogeneity. If heterogeneity existed, data were analyzed using a random-effects model. In the absence of heterogeneity, a fixed-effects model was used. We did all statistical analyses with comprehensive meta-analysis software version 2.0 (Biostat, Englewood, NJ, USA).
Results
Search results
A total of 319 potentially relevant studies were retrieved electronically, 309 of which were excluded for the reasons shown in . Six cohorts from six trialsCitation14–Citation19 assessing the efficacy of PPC in patients with nonsquamous histology and four randomized controlled trials (RCTs)Citation8,Citation10,Citation20,Citation21 comparing PPC with other platinum-based doublet chemotherapy were included in the meta-analysis. The baseline characteristics of each trial are presented in . The quality of four RCTs was approximately assessed according to Jadad scale. Four of the included trials did not mention the blinding of allocation clearly in the randomization process and thus had Jadad scores of 3. Overall, a total of 1,565 patients with advanced nonsquamous NSCLC receiving PPC and 986 with other platinum-based doublet chemotherapy were included; the pooled median PFS and OS were 5.7 and 16.05 months, respectively. A total of 680 patients from seven trials receiving PPC as first-line chemotherapy were included for ORR analysis. The pooled overall response rate was 37.8% (95% CI: 31.7%–44.3%, ). There was significant heterogeneity between the trials (I2=56.9%, P=0.031), and the pooled overall response was performed using a random-effects model. All of the four RCTs reported OS data. The pooled results demonstrated that PPC significantly improved OS in comparison with other platinum-based doublet chemotherapy treatments (0.86, 95% CI: 0.77–0.97, P=0.01, ) using a fixed-effects model (I2=0%, P=0.65). Two of four RCTs reported PFS data. The pooled hazard ratio for PFS demonstrated that PPC tends to improve PFS by giving HR 0.90 (95% CI: 0.80–1.01, P=0.084, ), compared with other platinum-based doublet chemotherapy in advanced nonsquamous NSCLC patients. There was no significant heterogeneity between trials (I2=0%, P=0.95), and the pooled HR for PFS was performed by using fixed-effects model.
Figure 1 Studies eligible for inclusion in the meta-analysis.
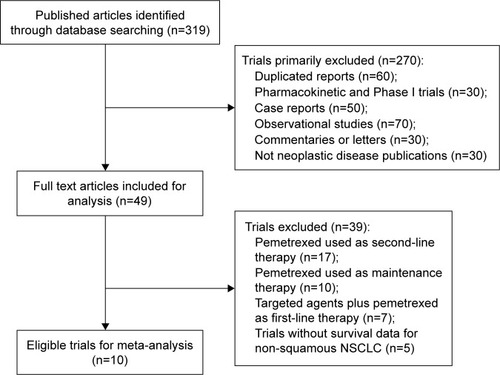
Figure 2 Random-effects model of ORR (95% CI) for pemetrexed plus platinum doublet chemotherapy.
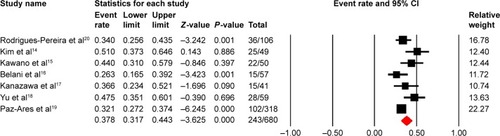
Figure 3 Fixed-effects model of HR (95% CI) of OS associated with PEM plus platinum versus other platinum-based chemotherapy.
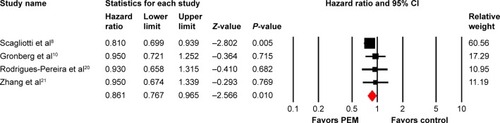
Figure 4 Fixed-effects model of HR (95% CI) of PFS associated with PEM plus platinum versus other platinum-based chemotherapy.
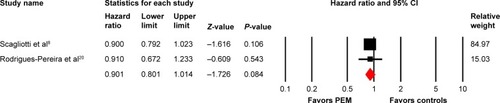
Table 1 Baseline characteristics of ten trials included for meta-analysis
Publication bias
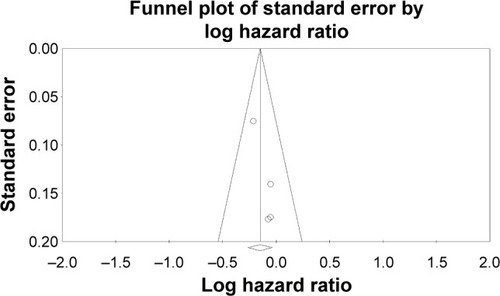
Begg’s funnel plot and Egger’s test were performed to assess the publication bias of literatures. The Begg’s funnel plots did not reveal any evidence of obvious asymmetry (P=0.50 for OS, ). Then, Egger’s test was used to provide statistical evidence of funnel plot symmetry. The results still did not suggest any evidence of publication bias for OS (P=0.05).
Figure 5 Funnel plot of publication bias in the meta-analysis.
Discussion
Many comprehensive and systematic reviews of the literature on PPC have been reported recently and are available for patients with advanced NSCLC.Citation3,Citation22–Citation24 However, to the best of our knowledge, this study is the first meta-analysis specifically focusing on investigating the efficacy of PPC as first-line chemotherapy in advanced nonsquamous NSCLC patients. Our study includes a total of 1,565 patients with advanced nonsquamous NSCLC receiving PPC and 986 with other platinum-based doublet chemotherapy. The pooled results demonstrate that pooled ORR for PPC is 37.8% (95% CI: 31.7%–44.3%), with median PFS and OS of 5.7 and 16.05 months, respectively. In addition, the use of PPC significantly improves OS (HR =0.86, 95% CI: 0.77–0.97, P=0.01) but not PFS (HR =0.90, 95% CI: 0.80–1.01, P=0.084) in advanced nonsquamous NSCLC patients. Based on pooled results, we found that pemetrexed plus platinum doublet regimen is an efficacious treatment for advanced nonsquamous NSCLC patients when compared to other platinum-based doublet chemotherapies. However, the results of our meta-analysis regarding survival data are not solid because of the limited number of RCTs included for analysis. Further RCTs specifically comparing PPC with other platinum-based doublet chemotherapy as first-line chemotherapy in advanced nonsquamous NSCLC patients are still needed.
The pathogenesis of the higher treatment effect of PPC in nonsquamous NSCLC remains unknown. One possible mechanism to explain this effect could be that the expression of thymidylate synthase is higher in squamous NSCLC and lower in nonsquamous NSCLC, leading to lower sensitivity to pemetrexed in the squamous histotype and higher sensitivity in nonsquamous types.Citation25
Our study has several limitations that need to be taken into account. First, all included studies were conducted at major academic institutions among patients with adequate major organ function; thus, the results may not entirely apply to the general patient population in the community or patients with organ dysfunction. Second, this is a meta-analysis at the study level; data are extracted from published clinical trial results, and individual patient information is not available. Therefore, subgroup analyses according to patients’ characteristics are not possible in this analysis. Finally, in the meta-analysis of published studies, publication bias is important because trials with positive results are more likely to be published and trials with null results tend not to be published. Our research detects no publication bias for OS.
Conclusion
In conclusion, pemetrexed plus platinum doublet regimen is an efficacious treatment for advanced nonsquamous NSCLC patients. Our findings support the use of pemetrexed plus platinum doublet regimens as first-line treatment in advanced nonsquamous NSCLC patients because of its potential survival benefits. Further investigation of this regimen as first-line treatment in nonsquamous NSCLC patients is still warranted.
Disclosure
The authors report no conflicts of interest in this work.
References
- JemalABrayFCenterMMFerlayJWardEFormanDGlobal cancer statisticsCA Cancer J Clin2011612699021296855
- BreathnachOSFreidlinBConleyBTwenty-two years of phase III trials for patients with advanced non-small-cell lung cancer: sobering resultsJ Clin Oncol20011961734174211251004
- GenovaCRijavecETruiniAPemetrexed for the treatment of non-small cell lung cancerExpert Opin Pharmacother201314111545155823683110
- FossellaFPereiraJRvon PawelJRandomized, multinational, phase III study of docetaxel plus platinum combinations versus vinorelbine plus cisplatin for advanced non-small-cell lung cancer: the TAX 326 study groupJ Clin Oncol200321163016302412837811
- PallisAGAgelakiSAgelidouAA randomized phase III study of the docetaxel/carboplatin combination versus docetaxel single-agent as second line treatment for patients with advanced/metastatic non-small cell lung cancerBMC Cancer20101063321092076
- GaoGJiangJLiangXA meta-analysis of platinum plus gemcitabine or vinorelbine in the treatment of advanced non-small-cell lung cancerLung Cancer200965333934419144444
- RossiARicciardiSMaionePde MarinisFGridelliCPemetrexed in the treatment of advanced non-squamous lung cancerLung Cancer200966214114919577816
- ScagliottiGVParikhPvon PawelJPhase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage non-small-cell lung cancerJ Clin Oncol200826213543355118506025
- ScagliottiGHannaNFossellaFThe differential efficacy of pemetrexed according to NSCLC histology: a review of two Phase III studiesOncologist200914325326319221167
- GronbergBHBremnesRMFlottenOPhase III study by the Norwegian lung cancer study group: pemetrexed plus carboplatin compared with gemcitabine plus carboplatin as first-line chemotherapy in advanced non-small-cell lung cancerJ Clin Oncol200927193217322419433683
- MoherDLiberatiATetzlaffJPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementPLoS Med200967e100009719621072
- MoherDPhamBJonesADoes quality of reports of randomized trials affect estimates of intervention efficacy reported in meta-analyses?Lancet199835291286096139746022
- ZintzarasEIoannidisJPHeterogeneity testing in meta-analysis of genome searchesGenet Epidemiol200528212313715593093
- KimYHHirabayashiMTogashiYPhase II study of carboplatin and pemetrexed in advanced non-squamous, non-small-cell lung cancer: Kyoto Thoracic Oncology Research Group Trial 0902Cancer Chemother Pharmacol201270227127622752216
- KawanoYOhyanagiFYanagitaniNPemetrexed and cisplatin for advanced non-squamous non-small cell lung cancer in Japanese patients: phase II studyAnticancer Res20133383327333323898099
- BelaniCPYamamotoNBondarenkoIMRandomized phase II study of pemetrexed/cisplatin with or without axitinib for non-squamous non-small-cell lung cancerBMC Cancer20141429024766732
- KanazawaKYokouchiHWangXPhase II trial of carboplatin and pemetrexed as first-line chemotherapy for non-squamous non-small cell lung cancer, and correlation between the efficacy/toxicity and genetic polymorphisms associated with pemetrexed metabolism: Hokkaido Lung Cancer Clinical Study Group Trial (HOT) 0902Cancer Chemother Pharmacol20147461149115725294632
- YuHZhangJWuXA phase II randomized trial evaluating gefitinib intercalated with pemetrexed/platinum chemotherapy or pemetrexed/platinum chemotherapy alone in unselected patients with advanced non-squamous non-small cell lung cancerCancer Biol Ther201415783283924755888
- Paz-AresLMezgerJCiuleanuTENecitumumab plus pemetrexed and cisplatin as first-line therapy in patients with stage IV non-squamous non-small-cell lung cancer (INSPIRE): an open-label, randomized, controlled phase 3 studyLancet Oncol201516332833725701171
- Rodrigues-PereiraJKimJHMagallanesMA randomized phase 3 trial comparing pemetrexed/carboplatin and docetaxel/carboplatin as first-line treatment for advanced, nonsquamous non-small cell lung cancerJ Thorac Oncol20116111907191422005471
- ZhangXLuJXuJPemetrexed plus platinum or gemcitabine plus platinum for advanced non-small cell lung cancer: final survival analysis from a multicentre randomized phase II trial in the East Asia region and a meta-analysisRespirology201318113113922882698
- LiXWeiSChenJCritical appraisal of pemetrexed in the treatment of NSCLC and metastatic pulmonary nodulesOnco Targets Ther2014793794524944517
- TomasiniPGreillierLKhobtaNBarlesiFThe place of pemetrexed in the management of non-small-cell lung cancer patientsExpert Rev Anticancer Ther201313325726623477511
- GridelliCMaionePRossiAPemetrexed in advanced non-small cell lung cancerExpert Opin Drug Saf201110231131721261558
- ShihCChenVJGossettLSLY231514, a pyrrolo[2,3-d] pyrimidine-based antifolate that inhibits multiple folate-requiring enzymesCancer Res1997576111611239067281