
Abstract
Folate receptor (FR) α expression in normal tissues is restricted to a subpopulation of epithelial cells. In contrast, FRα is overexpressed in epithelial ovarian cancer (EOC) and non-small-cell lung carcinoma. Therefore, FRα is considered a promising therapeutic target for EOC and non-small-cell lung carcinoma. Farletuzumab (MORAb-003) is a humanized monoclonal antibody of immunoglobulin G subtype 1 kappa, targeting human FRα. To date, Phase I/II clinical trials have clearly demonstrated the feasibility and safety of farletuzumab as a treatment option against solid tumors. However, in Phase III clinical trial that was conducted to verify the combined effect of paclitaxel–carboplatin combination therapy and farletuzumab for patients with recurrent EOC, improvement in progression-free survival was not statistically significant. This result might be owing to the fact that the eligibility criteria for these studies did not include FRα expression. The significance of FRα as a predictive/prognostic biomarker remains unclear. In addition, there is currently no established biomarker to predict the response and toxicities among patients receiving farletuzumab therapy. Furthermore, the primary mechanism of action of farletuzumab has not yet been identified. Therefore, further research to identify the mechanism of farletuzumab in tumor suppression is necessary to clarify the full potential of this chemotherapeutic agent.
Introduction
DNA synthesis in cancer cells is highly dependent on folate, whereas folate receptor (FR) α expression in normal tissues is restricted to a subpopulation of epithelial cells.Citation1,Citation2 In contrast, FRα is overexpressed in nearly 90% of epithelial non-mucinous ovarian cancers and has been correlated with tumor stage and grade, chemotherapeutic response, and treatment outcome.Citation3 In addition, FRα expression is retained in recurrent tumors and metastatic lesions.Citation4 Among lung cancers, FRα expression is increased in non-small-cell lung carcinoma (NSCLC)Citation5 and is higher in adenocarcinomas than in squamous cell carcinomas.Citation6 Hence, FRα is considered a promising therapeutic target for epithelial ovarian cancer (EOC)Citation7 and NSCLC.Citation8
Farletuzumab (MORAb-003), a humanized monoclonal antibody of immunoglobulin G subtype 1 kappa that targets human FRα,Citation9 was derived by optimizing the FRα-binding murine antibody LK26, which has high affinity for FRα.Citation10 A profile of farletuzumab is summarized in . Farletuzumab is considered to induce immune-dependent cell death, although no underlying mechanism has yet been clarified.Citation11 Farletuzumab has shown efficacy in both preclinical and clinical studies as a single agent and in combination chemotherapy with minimal drug-specific toxicity.Citation12 However, no improvement in progression-free survival (PFS) was observed in Phase III clinical trials that were conducted to verify the combined effect of cytotoxic drugs and farletuzumab.Citation13 This result might be because the eligibility criteria for these study did not include FRα expression.Citation2 Hence, there is a need for appropriate patient selection based on predictive biomarkers to clarify the potential of FRα expression in the clinical setting. In this review, we describe preclinical and clinical data related to farletuzumab and update recent findings.
Table 1 Profile of farletuzumab
Preclinical data on farletuzumab
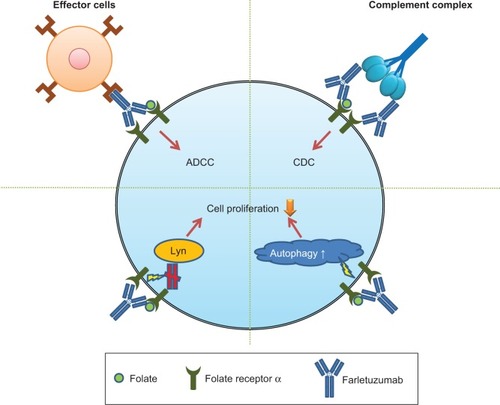
An in vitro study found that farletuzumab did not inhibit binding of folic acid and antifolates to FRα and that it had no significant effect on cell growth or folate uptake via FRα.Citation14 The proposed mechanism of farletuzumab-induced cell toxicity shown in suggests that farletuzumab inhibits FRα-dependent cell growth in a dose-dependent manner and exhibits tumor cytotoxicity through complement-dependent cytotoxicity (CDC) and antibody-dependent cellular cytotoxicity.Citation9 Farletuzumab has also been shown to inhibit the interaction between cytoplasmic tyrosine kinase Lyn and membrane-signaling complexes; this results in a reduction in the growth of these cells.Citation15 A recent preclinical study,Citation16 which found that farletuzumab inhibited tumor growth via induction of autophagy-associated cell death, demonstrated this inhibitory effect in three-dimensional in vitro models and showed that farletuzumab reduced tumor cell proliferation but had no significant effect on apoptosis, suggesting that blockade of FRα by farletuzumab induced sustained autophagy and suppressed cell proliferation.
Figure 1 Schema of the mechanism of farletuzumab-induced cell toxicity.
Abbreviations: ADCC, antibody-dependent cellular cytotoxicity; CDC, complement-dependent cytotoxicity.
Clinical data on ovarian cancer
Among gynecological malignancies, EOC is the most difficult to cure.Citation17,Citation18 The standard treatment for advanced EOC is maximum tumor debulking and systemic chemotherapy.Citation19,Citation20 Although >80% of patients respond to paclitaxel–carboplatin combination therapy, most will relapse.Citation21 Because the prognosis of advanced EOC remains poor, new agents are urgently needed to improve treatment outcome.Citation22 Toward this goal, farletuzumab is currently among the most promising drugs for EOC, as evidenced in several clinical trials.
Phase I studies
MORAb-003-001(NCT00428766)
In this Phase I dose-escalation study,Citation23 farletuzumab was intravenously administered to 25 patients with platinum-refractory or platinum-resistant EOC to assess the safety of weekly administration of 12.5–400 mg/m2 on days 1, 8, 15, and 22 and to determine the maximum tolerated dose. Drug efficacy was assessed using Response Evaluation Criteria in Solid Tumors (RECIST) and by monitoring serum cancer antigen (CA) 125 levels and evaluating pharmacokinetics of the drug. Because there was no dose-limiting toxicity, which is defined by the occurrence of grade ≥3 treatment-related adverse events (AEs), maximum tolerated dose was not determined. Therefore, a recommended dosage was not determined in this study. Given that 400 mg/m2 substantially corresponds to a weight-based dosing of 10–12 mg/kg, a dosage of 2.5–10 mg/kg was adopted in a Phase II clinical trial.
Although AEs were generally mild, grade 1/2 treatment-related AEs were observed in 20 patients (80.0%); however, there were no severe (grade ≥3) treatment-related AEs. The most common treatment-related AEs and drug hypersensitivity AEs are shown in . Drug hypersensitivity reactions were mild and managed with antipyretics and/or antihistamines. Efficacy was assessed at 4 weeks after cessation of treatment. No objective responses were observed. Of the 24 surviving patients who were included in this trial, stable disease was observed in nine (36%) and disease progression was observed in 15 (60%), while decreased CA125 levels were observed in four (17%). A population pharmacokinetic analysis revealed that body weight was the only investigated covariate, which explained inter-patient variability in disease clearance and central volume of distribution.Citation24
MORAb-003-005 (NCT01004380)
This Phase I studyCitation25 evaluated the safety of combination therapy with farletuzumab, carboplatin, and pegylated liposomal doxorubicin (PLD) in subjects with platinum-sensitive EOC. In this study, 15 patients who relapsed after >6 months after the completion of first- or second-line platinum-based chemotherapy were enrolled. All patients received six cycles of carboplatin (area under the curve [AUC] of 5–6) and PLD (30 mg/m2) on day 1 of every 4-week combination treatment cycle. The patients also received weekly intravenous injections of farletuzumab at 2.5 mg/kg. Following the completion of car-boplatin/PLD/farletuzumab therapy, maintenance treatment with 7.5 mg/kg farletuzumab was administered triweekly until disease progression. Among this cohort, there were no severe AEs, although anemia was observed in 14 (93%) patients; moreover, fatigue and hand–foot syndrome were observed in eight patients (53%). No increase in the incidence of side effects associated with the combination of farletuzumab and cytotoxic drugs was observed. Further clinical trials on the efficacy of this regimen are expected.
NCT01049061
This Phase I studyCitation26 assessed the safety and tolerability of farletuzumab among Japanese patients with solid tumors that express FRα. Pharmacokinetic profiles were also examined. Sixteen patients (14 with EOC and two with gastric cancer) were enrolled in this study. Farletuzumab (50, 100, 200, and 400 mg/m2) was intravenously administered weekly until tumor progression. No dose-limiting toxicity was observed among the study participants, and there were no severe AEs. Grade 1/2 infusion-related reactions were observed in 15 (93.8%) patients, and headache was observed in seven (43.8%). Furthermore, nausea and appetite loss were observed in five (31.3%) patients, respectively. Pharmacokinetic profiles in this study were similar to those in previous reports. Together, these results suggest that farletuzumab is also well tolerated by Japanese patients.
Phase II studies
MORAb-003-002 (NCT00318370)
This Phase II study evaluated the efficacy of farletuzumab treatment alone and in combination with chemotherapy, which consists of taxane and platinum, in patients with platinum-sensitive relapsed EOC.Citation27 For six cycles over a 21-day interval, 54 evaluable patients received weekly farletuzumab alone or in combination with chemotherapy, followed by weekly doses of farletuzumab maintenance until disease progression. The primary end points were normalization of CA125 levels and overall response rate. A serologic response (change in CA125) was defined using the modified Gynecologic Cancer Intergroup (GCIG) criteria. Furthermore, the interval of secondary responses was compared with the duration of the first response.
Of the 54 patients enrolled in this study, 47 (87%) received combination chemotherapy. In 38 (70%) patients, CA125 levels normalized after six cycles of combination therapy. Forty-three (80%) patients were evaluated based on RECIST. In these patients, the overall response rate was 70% (complete response, 7%; partial response, 63%). Notably, a second remission that was longer than their first remission was observed in nine (21%) of 44 evaluable patients. Furthermore, the response rate was high among patients with a first progression-free interval of <12 months. The results of this study suggested that farletuzumab combined with standard chemotherapy improves the response rate and progression-free interval in platinum-sensitive EOC patients.
MORAb-003-011 (NCT02289950)
This Phase II global, multicenter, double-blind, randomized, placebo-controlled study is underway to assess the safety and efficacy of farletuzumab in platinum-sensitive subjects in their first relapse with high-grade serous EOC and low CA125 levels. In this trial involving a target enrollment of 210 patients, weekly farletuzumab at a dosage of 5 mg/kg is being compared with a placebo in combination with chemotherapy (carboplatin + paclitaxel or carboplatin + PLD). The primary end point is PFS based on RECIST, and secondary endpoints are overall survival (OS), length of first vs second platinum-free interval, and tumor response.
Phase III studies
MORAb-003-003 (NCT00738699)
This Phase III randomized, placebo-controlled trialCitation28 assessed the efficacy and safety of farletuzumab in combination with weekly paclitaxel in patients with platinum-resistant recurrent or refractory EOC () to determine whether paclitaxel is more efficacious when administered alone or in combination with farletuzumab. The primary end point was 2-year PFS. This study was terminated early after recruiting 417 patients because the study did not meet the prespecified criteria for continuation following interim futility analysis.
Table 2 Characteristics of Phase III trial of farletuzumab for non-mucinous ovarian cancer including primary peritoneal or fallopian tube malignancies
MORAb-003-004 (NCT00849667)
This Phase III randomized, double-blind, placebo-controlled trial compared the efficacy and safety of six cycles of carboplatin and taxane (paclitaxel or docetaxel) with and without weekly farletuzumab in patients with a first platinum-sensitive relapse of EOC (). A total of 1,100 women were randomized to the following three arms: 1.25 mg/kg farletuzumab plus combination therapy, 2.5 mg/kg farletuzumab plus combination therapy, or placebo plus combination therapy. The primary end point was PFS. Secondary end points included OS, GCIG PFS, length of first vs second remission, tumor response, serologic response (CA125), quality of life, resource utilization, and pharmacokinetically assessed drug–drug interactions. The median PFS durations were 9.7, 9.5, and 9.0 months for 2.5 mg/kg farletuzumab, 1.25 mg/kg farletuzumab, and placebo, respectively (hazard ratio, 0.86; 95% confidence interval, 0.70–1.06 for 2.5 mg/kg vs placebo). No significant differences in PFS among the treatment arms were observed. The primary end point of PFS was not met in this study. However, post hoc exploratory analysis revealed a trend toward improved PFS in some patient subsets.Citation13,Citation28
Clinical data on lung cancer
Lung cancer is a leading cause of cancer-related death worldwide.Citation29,Citation30 NSCLC constitutes ~85% of lung cancers, and the median OS of patients with untreated advanced NSCLC is <6 months. Furthermore, the 1-year OS rate is 10% at best.Citation31 Thus, effective treatment for these patients is urgently needed.
A meta-analysis to verify the effectiveness of cytotoxic chemotherapy containing cisplatin for advanced NSCLC showed that platinum-based chemotherapy reduced the risk of mortality in these patients and improved symptom control and quality of life.Citation32 However, the effect of chemotherapy remains insufficient. In recent years, targeted therapies using epidermal growth factor receptor (EGFR) tyrosine kinase inhibitors and anaplastic lymphoma kinase (ALK) inhibitors have continued to attract attention. For example, the EGFR tyrosine kinase inhibitor gefitinib prolonged PFS in patients with NSCLC having EGFR mutations as compared with paclitaxel–carboplatin combination therapy.Citation33 However, EFGR mutations and translocations involving ALK only occur in 13% and 5% of patients with NSCLC, respectively.Citation34 Thus, an alternative therapeutic target is essential for improving the prognosis of patients with advanced NSCLC.
Similar to ovarian cancer, FRα expression is relatively higher in NSCLC tissues than in normal lung tissue. In addition, expression of FRα in lung adenocarcinoma is higher than that in squamous cell carcinoma.Citation5,Citation35,Citation36 Furthermore, some studies have revealed that FOLR1 expression is also relatively higher in lung adenocarcinoma.Citation37–Citation39 These characteristics have become the rationale for developing a targeted therapy that is efficacious against NSCLC with mild AEs. Therefore, farletuzumab is expected to be a new treatment option against NSCLC.
Based on the aforementioned preclinical data and safety profile of farletuzumab in combination with carboplatin–taxane doublet against EOC, a Phase II study involving patients with metastatic adenocarcinoma of the lung with FRα-expressing tumors was conducted.
NCT01218516
This Phase II, double-blind, placebo-controlled study evaluated the efficacy of farletuzumab in patients with FRα-positive metastatic adenocarcinoma of the lung. Importantly, in all patients, FRα expression of resected tumors was confirmed by immunohistochemistry using an antihuman FR monoclonal antibody. The primary end point was PFS, and the secondary end point was OS. Farletuzumab at a dose of 7.5 mg/kg was combined with a platinum-containing doublet in chemonaïve patients. The following platinum-based regimens were allowed: carboplatin (AUC of 6) and paclitaxel (200 mg/m2), carboplatin (AUC of 5) and pemetrexed (500 mg/m2), and cisplatin (75 mg/m2) and pemetrexed (500 mg/m2). Four to six cycles of combination chemotherapy were administered on a triweekly schedule. Patients who achieve objective tumor shrinkage after combination therapy will receive maintenance therapy with a placebo or 7.5 mg/kg of farletuzumab every 3 weeks until documented disease progression. The target enrollment of a total of 130 patients has already been reached. However, the results of this study were not available at the time that this manuscript was submitted for publication. Therefore, at present, the clinical evidence is insufficient to establish the efficacy of farletuzumab for the treatment of NSCLC.
Discussion
Past clinical trials revealed that farletuzumab exhibited certain antitumor effects with slight side effects, as described earlier. However, the effectiveness of farletuzumab alone for cancer treatment remains insufficient. To realize the actual potential of farletuzumab, appropriate patient selection based on appropriate biomarkers and combination therapy with other agents is important ().
Figure 2 Overview of the future direction to maximize the potential of farletuzumab.
Selecting appropriate patients through biomarker screening will facilitate the improvement of patient outcomes and decrease the degree of toxicity.Citation40 We already confirmed FRα expression of malignant tumors in the clinical setting.Citation41,Citation42 However, the significance of FRα as a predictive/prognostic biomarker remains unclear,Citation2 and the primary mechanism of action of farletuzumab has not yet been identified. The mechanisms of antitumor effects of monoclonal antibody therapy are believed to involve direct tumor targeting and indirect effects by enhancing immune responses.Citation23 Farletuzumab exhibits tumor cytotoxicity mediated by antibody-dependent cellular cytotoxicity and CDC rather than blocking FRα-mediated folate transport.Citation8 A recent in vitro study showed that farletuzumab enhanced type 2 cell death of tumor cells due to late-stage autophagy.Citation16 Hence, this mechanism may be considered the primary action of farletuzumab.Citation16 However, the effectiveness of farletuzumab to increase autophagy of tumor cells is unpredictable. In other words, there is currently no biomarker to predict the effectiveness of treatment. Therefore, further studies are needed to identify the underlying mechanisms involved in the antitumor effects of farletuzumab.
Proliferation of cancer cells is not necessarily dependent on a single pathway. When cancer cells are exposed to an anticancer agent, they acquire resistance through a variety of bypass pathways. In lung cancer, interactions between FRα expression and other molecular characteristics including EGFR mutation and ALK rearrangement, which are targets for treatment of lung cancer, are unclear. Hence, additional research to further elucidate the molecular biological mechanisms of the folate-related pathway is necessary. Bronte et alCitation43 suggested that combination therapy, consisting of farletuzumab and pemetrexed, may have a synergic effect because both drugs target the folate pathway. However, worsening of AEs remains a concern.Citation8 From the viewpoint of side effects, anticancer drugs, targeting molecules that are not associated with the folate pathway, for use in combination with farletuzumab are preferred. To this end, the combined effect of docetaxel and farletuzumab was confirmed in a recent in vitro study.Citation16 Based on these outcomes, future clinical applications for treating EOC and NSCLC are expected.
Conclusion
Phase I/II clinical trials clearly demonstrated the feasibility and safety of farletuzumab as a treatment option against solid tumors. In contrast, a Phase III clinical trial that was conducted to verify the effect of paclitaxel–carboplatin therapy combined with farletuzumab for patients with recurrent EOC found that improvement in PFS was not statistically significant, which might be due to the fact that the eligibility criteria for this study did not include FRα expression. The significance of FRα as a predictive/prognostic biomarker remains unclear. In addition, at present, there is no biomarker to predict the response and toxicities of patients treated with farletuzumab. Furthermore, the primary mechanism of action of farletuzumab has not yet been identified. Therefore, further research to discern the underlying mechanism of farletuzumab in tumor suppression is necessary to clarify the full potential of this chemotherapeutic agent.
Disclosure
The authors report no conflicts of interest and received no financial support associated with this article.
References
- KelemenLEThe role of folate receptor alpha in cancer development, progression and treatment: cause, consequence or innocent bystander?Int J Cancer2006119224325016453285
- LedermannJACanevariSThigpenTTargeting the folate receptor: diagnostic and therapeutic approaches to personalize cancer treatmentsAnn Oncol201526102034204326063635
- ChenYLChangMCHuangCYSerous ovarian carcinoma patients with high alpha-folate receptor had reducing survival and cytotoxic chemo-responseMol Oncol20126336036922265591
- KalliKRObergALKeeneyGLFolate receptor alpha as a tumor target in epithelial ovarian cancerGynecol Oncol2008108361962618222534
- IwakiriSSonobeMNagaiSHirataTWadaHMiyaharaRExpression status of folate receptor alpha is significantly correlated with prognosis in non-small-cell lung cancersAnn Surg Oncol200815388989918181001
- O’ShannessyDJYuGSmaleRFolate receptor alpha expression in lung cancer: diagnostic and prognostic significanceOncotarget20123441442522547449
- MarchettiCPalaiaIGiorginiMTargeted drug delivery via folate receptors in recurrent ovarian cancer: a reviewOnco Targets Ther201471223123625031539
- ShiHGuoJLiCWangZA current review of folate receptor alpha as a potential tumor target in non-small-cell lung cancerDrug Des Devel Ther2015949894996
- EbelWRouthierELFoleyBPreclinical evaluation of MORAb-003, a humanized monoclonal antibody antagonizing folate receptor-alphaCancer Immun20077617346028
- ThomasAMaltzmanJHassanRFarletuzumab in lung cancerLung Cancer2013801151823357463
- LinJSpidelJLMaddageCJThe antitumor activity of the human FOLR1-specific monoclonal antibody, farletuzumab, in an ovarian cancer mouse model is mediated by antibody-dependent cellular cytotoxicityCancer Biol Ther201314111032103824025360
- SpannuthWASoodAKColemanRLFarletuzumab in epithelial ovarian carcinomaExpert Opin Biol Ther201010343143720092424
- VergoteIArmstrongDScambiaGPhase III double-blind, placebo-controlled study of weekly farletuzumab with carboplatin/taxane in subjects with platinum-sensitive ovarian cancer in first relapseInt J Gynecol Cancer2013238 Suppl 111
- KamenBASmithAKFarletuzumab, an anti-folate receptor alpha antibody, does not block binding of folate or anti-folates to receptor nor does it alter the potency of anti-folates in vitroCancer Chemother Pharmacol201270111312022644798
- MiottiSBagnoliMTomassettiAColnaghiMICanevariSInteraction of folate receptor with signaling molecules lyn and G(alpha)(i-3) in detergent-resistant complexes from the ovary carcinoma cell line IGROV1J Cell Sci2000113Pt 234935710633085
- WenYGraybillWSPrevisRAImmunotherapy targeting folate receptor induces cell death associated with autophagy in ovarian cancerClin Cancer Res201521244845925416196
- ArmstrongDKBradyMFIntraperitoneal therapy for ovarian cancer: a treatment ready for prime timeJ Clin Oncol200624284531453317008690
- SatoSItamochiHOvarian cancer and drug resistanceCurr Obstet Gynecol Rep2015411825
- SatoSItamochiHNeoadjuvant chemotherapy in advanced ovarian cancer: latest results and place in therapyTher Adv Med Oncol20146629330425364394
- CannistraSACancer of the ovaryN Engl J Med2004351242519252915590954
- JelovacDArmstrongDKRole of farletuzumab in epithelial ovarian carcinomaCurr Pharm Des201218253812381522591419
- KudlowitzDTeplinskyEMuggiaFIntegrating targeted drugs with taxanes and platinums: opportunities and challengesTransl Cancer Res201541127136
- KonnerJABell-McGuinnKMSabbatiniPFarletuzumab, a humanized monoclonal antibody against folate receptor alpha, in epithelial ovarian cancer: a phase I studyClin Cancer Res201016215288529520855460
- FarrellCSchweizerCWustnerJPopulation pharmacokinetics of farletuzumab, a humanized monoclonal antibody against folate receptor alpha, in epithelial ovarian cancerCancer Chemother Pharmacol201270572773422955257
- KimKHJelovacDArmstrongDKPhase 1b safety study of farletuzumab, carboplatin and pegylated liposomal doxorubicin in patients with platinum-sensitive epithelial ovarian cancerGynecol Oncol2016140221021426644263
- SasakiYMiwaKYamashitaKA phase I study of farletuzumab, a humanized anti-folate receptor alpha monoclonal antibody, in patients with solid tumorsInvest New Drugs201533233234025380636
- ArmstrongDKWhiteAJWeilSCPhillipsMColemanRLFarletuzumab (a monoclonal antibody against folate receptor alpha) in relapsed platinum-sensitive ovarian cancerGynecol Oncol2013129345245823474348
- WaltersCLArendRCArmstrongDKNaumannRWAlvarezRDFolate and folate receptor alpha antagonists mechanism of action in ovarian cancerGynecol Oncol2013131249349823863359
- GoldstrawPCrowleyJChanskyKThe IASLC Lung Cancer Staging Project: proposals for the revision of the TNM stage groupings in the forthcoming (seventh) edition of the TNM Classification of malignant tumoursJ Thorac Oncol20072870671417762336
- JemalASiegelRXuJWardECancer statistics, 2010CA Cancer J Clin201060527730020610543
- SchillerJHHarringtonDBelaniCPComparison of four chemotherapy regimens for advanced non-small-cell lung cancerN Engl J Med20023462929811784875
- Non-small Cell Lung Cancer Collaborative GroupChemotherapy in non-small cell lung cancer: a meta-analysis using updated data on individual patients from 52 randomised clinical trialsBMJ199531170108999097580546
- MokTSWuYLThongprasertSGefitinib or carboplatin-paclitaxel in pulmonary adenocarcinomaN Engl J Med20093611094795719692680
- SequistLVHeistRSShawATImplementing multiplexed genotyping of non-small-cell lung cancers into routine clinical practiceAnn Oncol201122122616262422071650
- FranklinWAWaintrubMEdwardsDNew anti-lung-cancer antibody cluster 12 reacts with human folate receptors present on adenocarcinomaInt J Cancer Suppl1994889958194901
- NunezMIBehrensCWoodsDMHigh expression of folate receptor alpha in lung cancer correlates with adenocarcinoma histology and EGFR [corrected] mutationJ Thorac Oncol20127583384022729036
- KikuchiTDaigoYKatagiriTExpression profiles of non-small cell lung cancers on cDNA microarrays: identification of genes for prediction of lymph-node metastasis and sensitivity to anti-cancer drugsOncogene200322142192220512687021
- GarberMETroyanskayaOGSchluensKDiversity of gene expression in adenocarcinoma of the lungProc Natl Acad Sci U S A20019824137841378911707590
- BhattacharjeeARichardsWGStauntonJClassification of human lung carcinomas by mRNA expression profiling reveals distinct adenocarcinoma subclassesProc Natl Acad Sci U S A20019824137901379511707567
- LeamonCPLovejoyCDNguyenBPatient selection and targeted treatment in the management of platinum-resistant ovarian cancerPharmgenomics Pers Med2013611312524109193
- MaurerAHElsingaPFantiSNguyenBOyenWJWeberWAImaging the folate receptor on cancer cells with 99mTc-etarfolatide: properties, clinical use, and future potential of folate receptor imagingJ Nucl Med201455570170424732155
- KimMHKimWHKimCGKimDWSynthesis and evaluation of (99m)Tc-labeled folate-tripeptide conjugate as a folate receptor-targeted imaging agent in a tumor-bearing mouse modelNucl Med Mol Imaging201549320020726279693
- BronteGLo VulloFPerniceGFarletuzumab for NSCLC: exploiting a well-known metabolic pathway for a new therapeutic strategyExpert Opin Investig Drugs2015241125132