
Abstract
Background
The emerging dual imperatives of personalized medicine and technologic advances make population screening for preventable conditions resulting from genetic alterations a realistic possibility. Lynch syndrome is a potential screening target due to its prevalence, penetrance, and the availability of well-established, preventive interventions. However, while population screening may lower incidence of preventable conditions, implementation without evidence may lead to unintentional harms. We examined the literature to determine whether evidence exists that screening for Lynch-associated mismatch repair (MMR) gene mutations leads to improved overall survival, cancer-specific survival, or quality of life. Documenting evidence and gaps is critical to implementing genomic approaches in public health and guiding future research.
Materials and methods
Our 2014–2015 systematic review identified studies comparing screening with no screening in the general population, and controlled studies assessing analytic validity of targeted next-generation sequencing, and benefits or harms of interventions or screening. We conducted meta-analyses for the association between early or more frequent colonoscopies and health outcomes.
Results
Twelve studies met our eligibility criteria. No adequate evidence directly addressed the main question or the harms of screening in the general population. Meta-analyses found relative reductions of 68% for colorectal cancer incidence (relative risk: 0.32, 95% confidence interval: 0.23–0.43, three cohort studies, 590 participants) and 78% for all-cause mortality (relative risk: 0.22, 95% confidence interval: 0.09–0.56, three cohort studies, 590 participants) for early or more frequent colonoscopies among family members of people with cancer who also had an associated MMR gene mutation.
Conclusion
Inadequate evidence exists examining harms and benefits of population-based screening for Lynch syndrome. Lack of evidence highlights the need for data that directly compare benefits and harms.
Introduction
Advances in DNA sequencing and the gradual emergence of preventive interventions for certain genetic diseases have spurred growing interest in population-based genomic screening as a possible public health intervention.Citation1,Citation2 Recent calls to screen women in the general US population for BRCA1/2 mutations are an example.Citation3 It is presumed that such screening could minimize morbidity and mortality related to preventable conditions by identifying individuals who harbor unidentified genetic mutations that lead to a high risk for these conditions. Indeed, despite the absence of systematic investigation of the harms and benefits associated with genetic screening in asymptomatic populations, several groups and commercial efforts are already beginning to screen the general adult population for genetic mutations.Citation4–Citation7 Lynch syndrome is often included in such screening programs because of its nontrivial prevalence and high penetrance (50%–80% of family members of those diagnosed with cancer who carry such mutations will develop colorectal cancer [CRC] without preventive measures), and because interventions with well-documented efficacy are available. Lynch syndrome, also called hereditary nonpolyposis CRC, is associated with an increased risk of multiple cancers, including colorectal, endometrial, ovarian, stomach, small intestine, and skin.Citation8 Mutations in the MMR genes (MLH1, MSH2, MSH6, and PMS2) associated with Lynch syndrome occur in an estimated one out of every 440 people and are associated with a range of penetrance estimates (generated from studying family members of MMR mutation carriers diagnosed with cancer): 50%–80% risk of colon cancer and 40%–60% risk of endometrial cancer.Citation8–Citation10 Clinical modalities, such as frequent screening colonoscopies to remove polyps, gynecological screenings, and prophylactic surgery, are currently used and considered effective preventive measures for people with a personal or family history of Lynch-associated cancers and MMR gene mutations.Citation10–Citation12
To date, relevant systematic reviews have focused on screening individuals at high risk due to a family or personal medical history of cancer, but have not examined the evidence for net benefits of screening asymptomatic adults.Citation12,Citation13 For example, in 2009, the Center for Disease Control’s Evaluation of Genomic Applications in Practice and Prevention (EGAPP) Working Group completed a systematic review of the net benefits of performing molecular screening of tumors for evidence of Lynch syndrome in individuals newly diagnosed with CRC. They found sufficient evidence to recommend tumor screening, given the potential benefits for identifying at-risk relatives through cascade germline testing, but the focus on newly diagnosed cancer patients leaves unanswered questions for the larger asymptomatic adult population.Citation12 While there is robust literature and evidence about the benefits of screening symptomatic populations, an asymptomatic population may experience different harms or benefits and may have different penetrance rates than those with a personal or family history of cancer. Before implementing population screening efforts, it is important to understand the evidence of harms and benefits specific to the target population.
Therefore, we conducted a systematic review to evaluate the evidence on benefits and harms associated with screening for Lynch syndrome in the general adult population using targeted next-generation sequencing. We included evidence related to any of the four MMR genes associated with Lynch syndrome. Although specific genes vary in their precise impact on risk (eg, variations exist with regard to the penetrance of CRC and uterine cancer in those with different Lynch-associated gene mutations), we included all four genes in our analyses to increase the breadth and likelihood of identifying relevant studies. Our review is particularly timely due to recent advances in DNA sequencing technology that have driven interest in such screening in the absence of data about benefits and harms. Our overarching question was whether there is direct evidence that screening asymptomatic adults for MMR gene mutations with modern sequencing modalities (ie, massively parallel, also known as “next-generation”, sequencing) leads to improved overall survival, cancer-specific survival, or quality of life.
Materials and methods
We developed an analytic framework and five accompanying questions (Supplementary material 1) to guide the systematic review following procedures used by the US Preventive Services Task Force.Citation14 The analytic framework included five questions. First, our overarching question: Is there direct evidence that screening asymptomatic adults with genetic testing for MMR gene mutations (MLH1, MSH2, PMS2, and MSH6) leads to improved overall survival, cancer-specific survival, or quality of life? Second, what is the accuracy and reliability of targeted next-generation sequencing compared with Sanger sequencing and deletion/duplication testing for detecting mutations in MMR genes in asymptomatic adults? Third, for asymptomatic adults with an MMR gene mutation, and their family members who elect to be tested, does genetic counseling and early introduction of cancer-specific preventive measures reduce the incidence of cancers compared with routine cancer screening? Fourth, do counseling and early detection/preventive measures/interventions improve overall survival, cancer-specific survival, or quality of life for individuals and their family members who test positive for an MMR gene mutation? Fifth, are harms associated with genetic screening for MMR gene mutations using targeted next-generation sequencing or with subsequent interventions?
We present findings from each of these five questions in our results. Anticipating that we were unlikely to find any primary studies directly addressing our overarching question (ie, randomized controlled trials [RCTs] comparing screening with no screening and enrolling adults from the general population), our analytic framework constructed an indirect pathway potentially linking evidence on screening to health outcomes.
Data sources and searches
In May 2014, an experienced evidence-based practice center librarian searched PubMed, EMBASE, CINAHL, and the Cochrane Library for English-language papers published from June 2006 through May 2014 (Table S1, in Supplementary material 2). The 2006 date corresponds to the timing of last searches conducted by other reviews and technology assessments, especially the 2009 EGAPP review.Citation14,Citation15 To identify relevant papers published prior to June 2006, we manually searched reference lists of pertinent reviews and studies.
Study selection
All abstracts and full-text articles were independently reviewed by at least two investigators using prespecified eligibility criteria (Table S2, in Supplementary material 2), with disagreements resolved by group discussion. For our overarching question, we searched for RCTs comparing screening with no screening in asymptomatic adults without previous or current diagnosis of Lynch-associated cancers; however, non-RCTs, cohort studies, and modeling studies were also eligible. Given our anticipation of a limited number of studies of asymptomatic adults without a personal or family history of Lynch syndrome or associated cancers, studies of asymptomatic individuals with a family history were also eligible for inclusion.
Data extraction and risk of bias assessment
For each paper, one investigator identified and extracted relevant data using structured data extraction forms, while a second reviewed for completeness and accuracy. To assess studies’ risk of bias, two independent reviewers used predefined criteria based on established guidance.Citation16–Citation18 We rated the studies as low, medium, high, or unclear risk of bias.Citation17 For studies addressing analytic validity, we assessed risk of bias using the QUADAS-2.Citation19 Disagreements were resolved through group discussion. Tables S3–S14 (in Supplementary material 2) provide details of risk of bias assessment criteria and outcomes. Data extraction and assessment occurred between May 2014 and November 2015.
Data synthesis and analysis
We qualitatively synthesized findings for each question by summarizing the characteristics and results of included studies in tabular and narrative format. Meta-analyses were conducted using Stata® version 11 (Stata Press, College Station, TX, USA) when we identified three or more studies making the same comparison and reporting similar outcomes. We used random effects models with the inverse-variance weighted method (DerSimonian and Laird) to estimate relative risks (RRs).Citation20 For all quantitative syntheses, the χ2 and I2 statistics were calculated to assess statistical heterogeneity in effects between studies.Citation21,Citation22
We graded the strength of evidence as high, moderate, low, or insufficient based on an established approach that incorporates four key domains: risk of bias, consistency, directness, and precision.Citation23,Citation24 Tables S15–S23 (in Supplementary material 2) detail our strength of evidence assessments, which were determined by group consensus.
Results
Of 2,147 abstracts and 120 full papers reviewed, 12 studies met our eligibility criteria () – one modeling study addressed our overarching question;Citation25 two studies addressed analytic validity;Citation26,Citation27 six studies addressed the impact of early or more frequent colonoscopiesCitation28–Citation30 or gynecological screenings or prophylactic surgeryCitation31–Citation33 on cancer incidence or survival; and five studies addressed harms of screening and interventions.Citation30,Citation31,Citation34–Citation36 describes the characteristics and outcomes of each of our included studies.
Figure 1 Summary of searches and study selection.
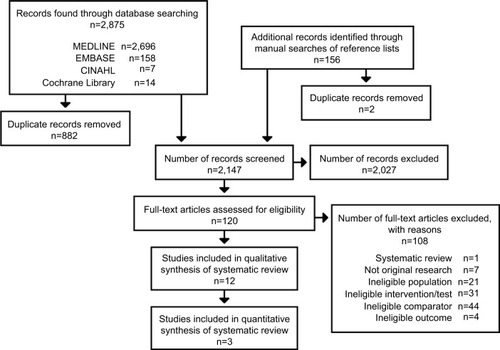
Table 1 Characteristics and main results of included studies
Included studies, other than those examining analytic validity, used prospective cohort,Citation29,Citation30 retrospective cohort,Citation28,Citation31–Citation33 and modeling designs.Citation25,Citation34–Citation36 No included studies were controlled trials. Both analytic validity studies were cross-sectional comparisons between next-generation and Sanger sequencing.Citation26,Citation27 We found no eligible studies reporting on quality of life, overdiagnosis, false-positive test results, disease-specific distress or anxiety, burden of responsibility associated with communicating positive test results with family, false-negative test results, or loss of insurance or inability to be insured.
Question 1: overarching question
The only included study for our overarching question was a cost-effectiveness analysis with a simulation framework integrating models of colorectal and endometrial cancers with a five-generation family history model to predict health and economic outcomes.Citation25 The study modeled 20 primary screening strategies for a simulated population of 100,000 people representative of the US population. The 20 screening strategies started at different ages (20, 25, 30, 35, or 40 years) and different thresholds for risk of carrying one of the four MMR mutations (based on PREMM126 model: 0%, 2.5%, 5%, or 10%).Citation37
The 20 hypothetical screening strategies yielded anywhere from 0.41 to 4.07 life-years saved per carrier exposed to screening; a strategy of universal screening starting at age 20 resulted in the greatest gain. However, universal screening (using no risk threshold) was not cost-effective. As the model increased the risk threshold for genetic testing, fewer people received primary genetic screening, and quality-adjusted life-years (QALYs) gained per 100,000 simulated individuals decreased while cost-effectiveness steadily improved ().
Some study strengths included using the validated Archimedes model and some inputs from a systematic review conducted for EGAPP.Citation15 Key limitations of the study included the lack of available inputs from the general asymptomatic population, using a risk prediction model developed from and validated for people referred for genetic testing and individuals with CRC (rather than the general population), limited use of sensitivity analyses to explore the potential impact of variation in uncertain inputs, not including other cancers for the probands (besides colorectal or endometrial) that occur more frequently in people with Lynch syndrome, and omission of indirect costs. In light of these limitations, many of which bias the results in favor of the intervention, we rated the study as high risk of bias for the clinical effectiveness assessment of universal screening and for all of the models using the PREMM risk prediction (Table S3, in Supplementary material 2). However, we rated the risk of bias as medium for the universal screening cost-effectiveness assessment (noting that the intervention was not found to be cost-effective). We graded the strength of evidence as insufficient (Table S15, in Supplementary material 2).
Question 2: analytic validity
Two studies met eligibility criteria for our analytic validity question.Citation26,Citation27 Both compared the performance of next-generation sequencing technologies with traditional Sanger sequencing (the reference standard). Hansen et alCitation26 tested 55 DNA samples for deleterious variants in the four MMR mutations, 39 of which were previously known to carry a deleterious mutation. Sixteen of the samples were previously uncharacterized, only evaluated as a test of the workflow, and did not contribute to characterization of the sensitivity/specificity of next-generation sequencing as a diagnostic test. Pritchard et alCitation27 tested 82 samples for mutations in genes classically implicated in Lynch syndrome. We extracted data on samples relevant to our review to calculate sensitivity and thus included the following: 23 from patients with known mutations in Lynch-associated genes or other familial colon cancers, and six public samples from a sequencing consortium. Nineteen samples from patients without any family history of cancer were evaluated for purposes of addressing specificity ().
Both studies reported high sensitivity and specificity for next-generation sequencing of Lynch-associated genes. The included studies reported sensitivities and specificities of 95%–100% and 89%–99.4%, respectively (). We rated both studies as low risk of bias (Tables S4 and S5, in Supplementary material 2) and graded the strength of evidence as high for both sensitivity and specificity (Tables S16 and S17, in Supplementary material 2).
Questions 3 and 4: cancer incidence and survival
Early or more frequent colonoscopy
Three studies examined the potential benefits of early or more frequent colonoscopies (with polypectomy, as needed) for adult family members with an MMR gene mutation (). Participants were identified either through testing subsequent to a first-degree relative’s cancer diagnosisCitation29,Citation30 or through confirmation mutation testing, being in the line of descent and having offspring with a proven mutation, or being in the line of descent and presenting clinically with a Lynch-associated tumor before age 50.Citation28 The included controls were individuals who had an identified MMR gene mutation,Citation29,Citation30 or who were identified or presumed to have a mutation based on familial and clinical indicationsCitation28 and failed to undergo recommended colonoscopy screening. Two studies tested for both MLH1 and MSH2;Citation29,Citation30 one included only MSH2.Citation28 Two were prospective cohort studies,Citation29,Citation30 and one was a retrospective cohort.Citation28 All three reported CRC incidence and overall survival, and one reported cancer-specific survival.Citation29
Overall, the three studies reported lower rates of CRC for those undergoing colonoscopy and polypectomy than for the control group. Our meta-analysis found a relative reduction of almost 70% in CRC incidence (RR: 0.32, 95% confidence interval [CI]: 0.23–0.43, I2: 7.7%) (Supplementary material 3). Additionally, Stupart et alCitation29 reported that cancers diagnosed in individuals who underwent colonoscopies were more likely to be early stage (Duke’s A/B) than late stage (Duke’s C/D), and late-stage cancers were more likely in unscreened individuals ().
Our meta-analysis showed that early or more frequent colonoscopies were associated with a significant reduction in all-cause mortality (RR: 0.22, 95% CI: 0.09–0.56; I2: 77.0%) (Supplementary material 4). Although each study found a statistically significant reduction in all-cause mortality, the analysis revealed considerable statistical heterogeneity. Our analysis, stratified by study design, identified differences in design as the possible cause of the heterogeneity, with the retrospective cohort studyCitation28 finding a greater effect size than the prospective studies. One study reported cancer-specific survival and found CRC to be the cause of death for 2% of those undergoing colonoscopies as compared with 12% of controls (RR: 0.19, 95% CI: 0.026–0.61) ().Citation29 We rated the risk of bias as low,Citation29 medium,Citation30 and high (due to risk of selection and survivor biases)Citation28 (Tables S7, S10, and S12, in Supplementary material 2). We graded the strength of evidence of the effects of colonoscopy on both CRC incidence and overall survival as moderate and the strength of evidence for cancer-specific survival as low (Tables S18, S21, and S22, respectively, in Supplementary material 2).
Gynecological screening and/or prophylactic surgery
We included three retrospective cohort studies. Two studies examined incidence of and survival from gynecological cancers in adult family members with an MMR gene mutation who had undergone gynecological screening.Citation32,Citation33 A third study examined the effect of prophylactic gynecological surgery in women with an MMR mutation identified from hereditary-cancer registries.Citation31 Specific screening and surgical interventions examined varied for each study (). Controls were individuals with identified MMR mutationsCitation31,Citation33 or who were known or presumed to have a mutation based on familial and clinical indicationsCitation32 and who did not undergo gynecological screeningCitation32,Citation33 or surgery.Citation31 Two studies examined MLHI, MSH2, and MSH6 carriers;Citation31,Citation33 one included only MSH2 carriers.Citation32 All three studies examined cancer survival and incidence of endometrial cancer; two also examined incidence of ovarian cancer.Citation31,Citation32
Two studies found that gynecological screening had little effect on cancer incidence or survival, while the third study found prophylactic surgery to be effectiveCitation31 (). Schmeler et alCitation31 found that no woman who had undergone prophylactic hysterectomy subsequently had endometrial cancer, compared with 33% of the control group’s women (prevented fraction of potential new cancers: 100%, 95% CI: 90%–100%). Similarly, no one who had undergone bilateral salpingo-oophorectomy at the time of their hysterectomy was subsequently diagnosed with ovarian cancer, whereas 5% of the control group’s women developed ovarian cancer (prevented fraction of potential new cancers: 100%, 95% CI: –62%–100%). Three participants in the surgery group died (from colon, brain, and bladder cancer, respectively), while 22 died in the control group. Of these 22, 17 died from various cancers, one from cardiac disease, and four from causes unknown.
We rated the study of prophylactic surgeryCitation31 as having a medium risk of bias, and the two papers on gynecological screening as having high risk of biasCitation32,Citation33 (due to selection bias and risk of confounding). The strength of evidence ratings for endometrial cancer and ovarian cancer incidence were low and insufficient, respectively, for both gynecological screening and surgery (Tables S19 and S20, in Supplementary material 2). Additionally, we graded the strength of evidence of both cancer-specific and overall survival following screenings or surgery as insufficient (Tables S21 and S22, in Supplementary material 2).
Question 5: harms of screening and interventions
Complications due to surgery
One study reported the death of a control group patient due to a pulmonary embolism after a successful colectomy.Citation30 Another study reported complications of ureteral injury, ureterovaginal fistula, and ureteroenteral fistula in a woman who had prophylactic abdominal hysterectomy with salpingo-oophorectomy and a prior history of rectal carcinoma treated by rectosigmoid resection with colostomy and creation of a Hartmann’s pouch.Citation31
Costs
Three modeling studies presented somewhat relevant data on costs of preventive interventions for people with Lynch syndrome or testing relatives of people known to have Lynch syndrome (). Yang et alCitation35 modeled cost-effectiveness for a theoretical population of women with Lynch syndrome at age 30, comparing prophylactic surgery (hysterectomy and bilateral salpingo-oophorectomy) with two forms of surveillance (annual gynecological screening and annual gynecological exam), to predict endometrial or ovarian cancer outcomes.Citation35 The authors found that risk-reducing surgery led to the lowest costs and highest number of QALYs ($23,224 per patient for 25.71 QALYs for surgery, compared with $68,392 for 25.17 QALYs for annual screening, and $100,484 for 24.60 QALYs for annual exam). A second study by Breheny et alCitation34 presented a decision analysis for asymptomatic first-degree relatives of known Lynch mutation carriers.Citation34 Using life expectancy and costs of surveillance and surgery in Western Australia for individuals aged 25–70 years, they found a net savings and one CRC-free year gained when comparing relatives who are tested to relatives who are not tested but have increased colonoscopy and gynecological surveillance. However, when comparing testing to a control group with population surveillance only, they found eight CRC-free years gained at an overall net cost.Citation34 In the final study, Vasen et alCitation36 modeled the cost-effectiveness of increased colonoscopy surveillance for male Lynch syndrome mutation carriers.Citation36 They found cost savings and a 7-year increased life expectancy for those receiving surveillance versus no surveillance. We graded the strength of evidence of these studies as insufficient given the medium risk of bias, the reliance on various evidence sources and assumptions, and the lack of reporting on precision estimates (Table S23, in Supplementary material 2).
Discussion
Overall, we found little evidence to inform an assessment of the harms and benefits of screening asymptomatic adults without a personal or family history of Lynch-associated cancers for Lynch syndrome with targeted next-generation sequencing. The vast majority of papers exploring the effectiveness of interventions studied individuals already diagnosed with cancer or their family members. Of the 12 included studies, three were modeling studies and two examined analytic validity. The remaining seven examined the effects of early or more frequent colonoscopies or gynecological screenings and surgeries on cancer incidence and mortality among individuals already diagnosed with cancer or their family members. The 12 studies focused on Lynch-associated colorectal and gynecological cancers. In spite of the fact that Lynch syndrome, like many genetic conditions, is pleiotropic, which raises unique concerns regarding returning results and explaining implications and medical interventions,Citation38 we found no evidence about screening measures for other Lynch-associated cancers, such as skin cancers, hepatobiliary cancer or transitional cell carcinomas of the renal pelvis or ureter.
In population-based screening programs, asymptomatic individuals face potential harms that are distinct from those faced by individuals with symptoms and their relatives, such as overdiagnosis (identifying mutations that would never have caused a problem) leading to anxiety and unnecessary treatment, or misinterpreting the meaning of negative results for Lynch-associated mutations (giving false reassurance that routine CRC screening is unnecessary for them).Citation39 Further complicating population-based interventions, current penetrance estimates for Lynch-associated mutations (and other Mendelian conditions) are based on families with a high incidence of the disorder in question; penetrance of mutations found in the general population is likely lower than that estimated in published studies. Despite these potential differences in harms for asymptomatic individuals, we found an absence of evidence on harms of screening the general population for Lynch syndrome. Our initial inclusion/exclusion criteria comprised a broad range of potential harms, from overdiagnosis and overtreatment to misinterpretation of negative or uncertain results and increased cost (Table S2, in Supplementary material 2). Despite the breadth of our search, we found only three modeling studies examining cost and two studies that briefly described complications postintervention.
Misinterpretation of results and subsequent overtreatment is a major potential harm of genomic screening of an asymptomatic population. Any time individuals undergo genetic sequencing, numerous variants of uncertain significance are generated. In screening asymptomatic populations, the probability that any given variant of uncertain significance represents an actual deleterious Lynch variant is very low. This reality necessitates an extremely rigorous variant classification and reporting scheme to avoid reporting a large number of false positives that would commit a vast number of individuals to unnecessary surveillance.Citation40
Limitations
We did not include uncontrolled studies that evaluated the benefits or harms of relevant interventions. To be eligible, studies were required to have a comparator group. The studies included in our review were not designed or adequately powered to assess complications of colonoscopy or other interventions. Although we found limited evidence that met our inclusion criteria, other bodies of literature have described harms from the preventive interventions in our review. For example, serious harms including perforations, hemorrhage, diverticulitis, cardiovascular events, severe abdominal pain, and death are estimated to occur in 2.8 per 1,000 screening colonoscopies (95% CI: 1.5–5.2 per 1,000 procedures).Citation41 Furthermore, we identified a number of non-comparative studies addressing psychosocial harms and the short- and long-term impacts of predictive testing that did not meet our eligibility criteria.Citation42–Citation44 Most authors, however, acknowledge methodological limitations in these studies as well as selection biases inherent in self-referred, motivated study populations.
Conclusion
In summary, there are increasing calls to implement genomic screening at the population level, and Lynch syndrome is an appealing candidate for such programs. Overall, however, our systematic review shows that there is inadequate evidence examining the potential harms and benefits of such population-based screening. The need for rigorous investigation is especially compelling at present given the large uncontrolled experiment that is currently being conducted by multiple groups, including commercial efforts, which are embarking upon such screening without a sufficient underlying evidence base. Some research projects are beginning to explore the impact of genomic testing in asymptomatic populations without a personal or family history of cancer, but clearly more research is needed before we can begin to understand the implications of how genomic screening may differ from testing in symptomatic patients and their relatives, and what benefits and harms it may entail when broadly applied to asymptomatic populations.
Acknowledgments
Research reported in this publication was supported by the National Institutes of Health through the National Human Genome Research Institute under Award Numbers P50HG004488 (all authors, except DP) and U01HG006487 (GEH and JPE), the National Heart, Lung, and Blood Institute under Award Number HL105493 (GC-S), and the US Department of Health and Human Services through the Health Resources and Services Administration under Award Number 5-D33-HP25771 (DP). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. All authors participated in the conception and design of the systematic review, the analysis of the data, and the drafting and revising of the manuscript. The review’s literature searches were conducted by Christiane Voisin, MLS. Additional data analysis support was received from Roberta Wines, Gabriel Lázaro-Muñoz, Alexi McHugh, and Malika Roman Isler. We also thank the two anonymous reviewers for their helpful comments and suggestions to improve this manuscript.
Disclosure
The authors report no other conflicts of interest in this work.
References
- EvansJPBergJSOlshanAFMagnusonTRimerBKWe screen newborns, don’t we?: realizing the promise of public health genomicsGenet Med201315533233423470837
- GuttmacherAECollinsFSKhouryMJMcCabeLLMcCabeERPopulation screening in the age of genomic medicineN Engl J Med20033481505812510043
- Levy-LahadELahadAKingMCPrecision medicine meets public health: population screening for BRCA1 and BRCA2J Natl Cancer Inst2015107142025550384
- Million Veteran Program (MVP) Available from: http://www.research.va.gov/mvp/Accessed November 11, 2015
- The 100,000 Genomes Project Available from: http://www.genomic-sengland.co.uk/about-genomics-england/Accessed November 4, 2015
- RayTCompanies Begin Subsidizing Color Genomics’ Breast, Ovarian Cancer Testing for EmployeesGenomeWeb2015 Available from: https://www.genomeweb.com/molecular-diagnostics/companies-begin-subsidizing-color-genomics-breast-ovarian-cancer-testingAccessed December 2, 2016
- HelgerMGeisinger Begins Returning Clinically Actionable Exome Sequencing Results to PatientsGenomeWeb2015
- KohlmannWGruberSBLynch syndromePagonRAAdamMPArdingerHHGeneReviews®Seattle, WAUniversity of Washington1993
- ChenSWangWLeeSPrediction of germline mutations and cancer risk in the Lynch syndromeJAMA2006296121479148717003396
- LindorNMPetersenGMHadleyDWRecommendations for the care of individuals with an inherited predisposition to Lynch syndrome: a systematic reviewJAMA2006296121507151717003399
- VasenHFBlancoIAktan-CollanKRevised guidelines for the clinical management of Lynch syndrome (HNPCC): recommendations by a group of European expertsGut201362681282323408351
- Recommendations from the EGAPP Working Group: genetic testing strategies in newly diagnosed individuals with colorectal cancer aimed at reducing morbidity and mortality from Lynch syndrome in relativesGenet Med2009111354119125126
- MoyerVARisk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: US Preventive Services Task Force recommendation statementAnn Intern Med2014160427128124366376
- US Preventive Services Task Force Procedure Manual Available from: https://www.uspreventiveservicestaskforce.org/Page/Name/methods-and-processes?Accessed December 2, 2016
- PalomakiGEMcClainMRMelilloSHampelHLThibodeauSNEGAPP supplementary evidence review: DNA testing strategies aimed at reducing morbidity and mortality from Lynch syndromeGenet Med2009111426519125127
- Agency for Healthcare Research and QualityMethods Guide for Effectiveness and Comparative Effectiveness ReviewsRockville, MDAgency for Healthcare Research and Quality2014
- ViswanathanMAnsariMTBerkmanNDAssessing the Risk of Bias of Individual Studies in Systematic Reviews of Health Care InterventionsRockville, MDAHRQ Publication No. 12-EHC047-EF2012
- Agency for Healthcare Research and QualityMethods Guide for Medical Test ReviewsRockville, MDAgency for Healthcare Research and Quality2012
- WhitingPFRutjesAWWestwoodMEQUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studiesAnn Intern Med2011155852953622007046
- SuttonAJAbramsKRJonesDRMethods for Meta-Analysis in Medical Research (Wiley Series in Probability and Statistics – Applied Probability and Statistics Section)London, UKWiley2000
- HigginsJPThompsonSGQuantifying heterogeneity in a meta-analysisStat Med200221111539155812111919
- HigginsJPThompsonSGDeeksJJAltmanDGMeasuring inconsistency in meta-analysesBMJ2003327741455712958120
- OwensDKLohrKNAtkinsDAHRQ series paper 5: grading the strength of a body of evidence when comparing medical interventions – Agency for Healthcare Research and Quality and the Effective Health-Care ProgramJ Clin Epidemiol201063551352319595577
- BerkmanNDLohrKNAnsariMTGrading the strength of a body of evidence when assessing health care interventions: an EPC updateJ Clin Epidemiol201468111312132425721570
- DinhTARosnerBIAtwoodJCHealth benefits and cost-effectiveness of primary genetic screening for Lynch syndrome in the general populationCancer Prev Res (Phila)20114192221088223
- HansenMFNeckmannULavikLAA massive parallel sequencing workflow for diagnostic genetic testing of mismatch repair genesMol Genet Gen Med201422186200
- PritchardCCSmithCSalipanteSJColoSeq provides comprehensive lynch and polyposis syndrome mutational analysis using massively parallel sequencingJ Mol Diagn201214435736622658618
- StucklessSGreenJSMorgensternMImpact of colonoscopic screening in male and female Lynch syndrome carriers with an MSH2 mutationClin Gen2012825439445
- StupartDAGoldbergPAAlgarURamesarRSurveillance colonoscopy improves survival in a cohort of subjects with a single mismatch repair gene mutationColorectal Dis200911212613019143775
- JarvinenHJAarnioMMustonenHControlled 15-year trial on screening for colorectal cancer in families with hereditary nonpolyposis colorectal cancerGastroenterology2000118582983410784581
- SchmelerKMLynchHTChenLMProphylactic surgery to reduce the risk of gynecologic cancers in the Lynch syndromeN Engl J Med2006354326126916421367
- StucklessSGreenJDawsonLImpact of gynecological screening in Lynch syndrome carriers with an MSH2 mutationClin Gen2013834359364
- Renkonen-SinisaloLButzowRLeminenALehtovirtaPMecklinJPJarvinenHJSurveillance for endometrial cancer in hereditary nonpolyposis colorectal cancer syndromeInt J Cancer2007120482182417096354
- BrehenyNGeelhoedEGoldblattJEeHO’LearyPEconomic evaluation of the familial cancer programme in Western Australia: predictive genetic testing for familial adenomatous polyposis and hereditary non-polyposis colorectal carcinomaCommunity Genet2006929810616612060
- YangKYCaugheyABLittleSECheungMKChenLMA cost-effectiveness analysis of prophylactic surgery versus gynecologic surveillance for women from hereditary non-polyposis colorectal cancer (HNPCC) familiesFam Cancer201110353554321538078
- VasenHFvan BallegooijenMBuskensEA cost-effectiveness analysis of colorectal screening of hereditary nonpolyposis colorectal carcinoma gene carriersCancer1998829163216379576281
- KastrinosFSteyerbergEWMercadoRThe PREMM(1,2,6) model predicts risk of MLH1, MSH2, and MSH6 germline mutations based on cancer historyGastroenterology20111401738120727894
- KocarnikJMFullertonSMReturning pleiotropic results from genetic testing to patients and research participantsJAMA2014311879579624481117
- PrinceAEBergJSEvansJPJonasDEHendersonGGenomic screening of the general adult population: key concepts for assessing net benefit with systematic evidence reviewsGenet Med201517644144325232850
- AdamsMCEvansJPHendersonGEBergJSInvestigatorsGThe promise and peril of genomic screening in the general populationGenet Med201618659359926540154
- WhitlockEPLinJSLilesEBeilTLFuRScreening for colorectal cancer: a targeted, updated systematic review for the US Preventive Services Task ForceAnn Intern Med2008149963865818838718
- BleikerEMEsplenMJMeiserBPetersenHVPatenaudeAF100 years Lynch syndrome: what have we learned about psychosocial issues?Fam Cancer201312232533923670341
- SieASPrinsJBSpruijtLKetsCMHoogerbruggeNCan we test for hereditary cancer at 18 years when we start surveillance at 25? Patient reported outcomesFam Cancer201312467568223604858
- CollinsVRMeiserBUkoumunneOCGaffCSt JohnDJHallidayJLThe impact of predictive genetic testing for hereditary nonpolyposis colorectal cancer: three years after testingGenet Med20079529029717505206