Abstract
Translating pharmacogenetics to clinical practice has been particularly challenging in the context of pain, due to the complexity of this multifaceted phenotype and the overall subjective nature of pain perception and response to analgesia. Overall, numerous genes involved with the pharmacokinetics and dynamics of opioids response are candidate genes in the context of opioid analgesia. The clinical relevance of CYP2D6 genotyping to predict analgesic outcomes is still relatively unknown; the two extremes in CYP2D6 genotype (ultrarapid and poor metabolism) seem to predict pain response and/or adverse effects. Overall, the level of evidence linking genetic variability (CYP2D6 and CYP3A4) to oxycodone response and phenotype (altered biotransformation of oxycodone into oxymorphone and overall clearance of oxycodone and oxymorphone) is strong; however, there has been no randomized clinical trial on the benefits of genetic testing prior to oxycodone therapy. On the other hand, predicting the analgesic response to morphine based on pharmacogenetic testing is more complex; though there was hope that simple genetic testing would allow tailoring morphine doses to provide optimal analgesia, this is unlikely to occur. A variety of polymorphisms clearly influence pain perception and behavior in response to pain. However, the response to analgesics also differs depending on the pain modality and the potential for repeated noxious stimuli, the opioid prescribed, and even its route of administration.
Introduction
Recent developments in genomic research have opened vast opportunities to expand and improve our understanding of how genetic variability affects response to prescribed medication. The ultimate goal of pharmacogenomic research is to offer “tailored personalized medicine” to improve the efficacy of medication as well as patient safety by helping predict the risk of adverse outcomes. Although numerous hurdles have limited the creation and implementation of pharmacogenetic testing, several pharmacogenetic tests have been recently developed,Citation1 and the US Food and Drug Administration (FDA)Citation2 and the European Medicines Agency have approved several drug label modifications to contain pharmacogenetic information.Citation3 Furthermore, in the last year, the Clinical Pharmacogenetics Implementation ConsortiumCitation4 has published guidelines for warfarin,Citation5 clopidogrel,Citation6 and thiopurine dosingCitation7 based on pharmacogenetic testing, and the guidelines for codeine therapy in the context of CYP2D6 genotype are being published these days.Citation8
Pain perception is one of the most complex quantifiable traits because it encompasses several phenotypes involving the peripheral and central nervous systems, and as a complex trait it is expected to have a polygenic nature shaped by environmental factors such as trauma, lifestyle, and stress. In addition, an important characteristic in determining the pain phenotype is the wide interindividual pharmacologic range in response to drugs. Therefore, not surprisingly, translating pharmacogenetics to clinical practice has been particularly challenging in the context of pain, due to the complexity of this multifaceted phenotype and the overall subjective nature of pain perception and response to analgesia. Yet with a growing body of evidence demonstrating a strong association between severe acute pain and the risk for persistent pain, identifying individuals with an increased vulnerability to pain, including genetic factors, may allow to substantially improve clinical outcomes.Citation9 This overview will present an outline of some genetic variants involved in pain and analgesic responses, bearing in mind the interplay between pharmacokinetic (eg, the CYP450 family of enzymesCitation10) and pharmacodynamic (eg, the well-studied μ-opioid receptor) effects. It will review patient-specific considerations in the clinical setting of opioids for acute pain, including postoperative pain, opioids for labor analgesia, and the response to opioids for chronic pain. Finally, the clinical utility of pharmacogenomic testing in pain management and the future of personalized medicine in this context will be reviewed.
Interindividual variability in pain sensitivity
Clinicians and pain providers are well aware of the large and unpredictable interindividual variability in pain perception and sensitivity to analgesia.Citation11,Citation12 Twin and volunteer studies have demonstrated a significant heritability for experimental pain responses,Citation13,Citation14 and recent genomic and pharmacogenetic research has considered numerous candidate genes as suitable targets for the study of the genetic and inheritable basis of pain and/or response to analgesic drugs.Citation15
The “genetic architecture of human pain perception” has been proposed to include rare deleterious genetic variants and more common genetic polymorphisms as mediators of human pain perception and clinical pain phenotypes.Citation16 An extremely rare pain phenotype characterized by a total absence of pain perception (“congenital insensitivity to pain”) with no associated neuropathy has been associated with the mutations in the gene SCN9A, encoding the α-subunit of the voltage-gated sodium channel NaV1.7.Citation17,Citation18 This discovery has already opened directions for novel generations of therapeutic agents blocking NaV1.7,Citation19,Citation20 with the hope that these drugs may provide selective and safe analgesia/anesthesia. Another clinical phenotype resulting from loss-of-function mutations of NaV1.7 termed “congenital indifference to pain,” refers to individuals who actually recognize painful stimuli but lack the affective-motivational component of pain perception, do not show withdrawal responses, and often die in childhood.Citation21 Along the same line, it has also been proposed from an evolutionary standpoint that individuals experiencing severe pain may in fact not be disfavored, as they are likely to have an increased capacity to sense essentially all environmental stimuli and increase their ability to detect and avoid environmental threats. With that in mind, lower pain threshold is commonly associated with the ability to detect a wide variety of nonnoxious sensory stimuli, and may represent a beneficial adaptive mechanism. This has been suggested as an explanation for sex-dependent differences in pain sensitivity, resulting from evolutionary pain-modulation processes, which afford women a greater sense of awareness of potential environmental threats to offer heightened protection to their offspring.Citation22
In the era of opioid therapy, pharmacogenomic studies to guide opioid-based analgesic regimens are flourishing. Among the numerous candidate genes that have been considered important in opioid response, the CYP family of enzymes, the μ-opioid receptor gene (OPRM1, p.118 A/G), the catechol-O-methyltransferase gene (COMT, Val158Met), several variants of the ATP-binding cassette, and subfamily B member 1 gene (ABCB1) have been extensively reviewed. However, most drug effects are determined by the interaction of several polymorphisms that influence the pharmacokinetics and pharmacodynamics of medications, including inherited differences in drug targets (eg, receptors) and drug disposition (eg, drug-metabolizing enzymes and transporters). This interplay may result in polygenic determinants that involve numerous potential combinations of drug-metabolism, drug-transporters and drug-receptor genotypes with corresponding drug-response phenotypes yielding a wide-range of therapeutic indexes (efficacy/toxicity ratios) for a given drug.
Genetic variants of CYP family of enzymes and opioid metabolism
Altogether, 20%–25% of clinically used drugs are influenced by genetic variants of enzymes.Citation23 Cytochrome P450 enzymes (CYPs) play a major role, as these are responsible for about 80% of phase I metabolism.Citation24 CYP2D6 metabolizes approximately 25% of frequently used drugs, eg, β-blockers, antiarrhythmics, antidepressants, neuroleptics, and analgesics.Citation25,Citation26 Four metabolic phenotypes are characterized; poor (PM), intermediate (IM), extensive (EM), and ultrarapid (UM) metabolizers. Critical base changes or deletions result in more than 80 distinct CYP2D6 allelic variants, explaining the wide spectrum of metabolic diversity within populations.Citation27 A comprehensive list of all known cytochrome alleles is displayed at the website of the CYP Allele Nomenclature Committee (http://www.imm.ki.se/CYPalleles). Relevant polymorphisms resulting in nonfunctional alleles are single base exchanges (CYP2D6*4 [rs3892097], CYP2D6*7 [rs5030867], CYP2D6*8 [rs5030865]) or deletions (CYP2D6*3 [rs35742686], CYP2D6*6 [rs5030655]) within the cytochrome P450 2D6 gene locus. Deletion of the entire CYP2D6 gene (CYP2D6*5) also results in the absence of CYP2D6 protein production. Subjects with these homozygous PM-associated variants are at increased risk for potentially severe adverse side effects due to drug concentrations exceeding the therapeutic level (ie, tricyclic antidepressants, antiarrhythmics) or for therapeutic failure due to poor metabolism of a prodrug (ie, codeine, tramadol) into its active metabolite. In contrast, duplication or multiduplication of the CYP2D6 gene is related to the UM phenotype and increased enzyme activity resulting in rapid decline of respective plasmatic drug concentrations. Thus, therapeutic effects cannot be obtained in UM at conventional doses of an active drug.Citation28
The distribution of different CYP2D6 phenotypes within specific cohorts varies depending on geographic region and individuals’ ethnicity;Citation13 up to 7%–10% of Caucasians are categorized as PMs. In a study screening 1060 individuals within 52 worldwide-distributed populations,Citation29 a greater variation of CYP2D6 within populations than between groups thereof was found. When comparing allelic distribution among different ethnicities, the CYP2D6*4 allele is frequently found in Caucasians (in the order of 20% allelic frequency) and represents more than 75% of the mutant CYP2D6 alleles, while it is extremely rare among Chinese individuals. Other alleles such as the CYP2D6*10, resulting in an IM phenotype, are particularly frequent among Asian individuals, and so are the CYP2D6*45 and CYP2D6*46 alleles among individuals of black African origin. In a middle European population, 3%–5% are UMs, whereas in Scandinavia this figure decreases to 1%–2%; however, it increases for subjects from the Mediterranean (10%–12%), Saudi Arabia (21%) and Ethiopia (29%).Citation23 Of particular clinical relevance, the UM phenotype is the second most common type in North Africa, the Middle East, Oceania, and the EMs being the most common. Prodrugs that rely on CPY2D6 metabolism are likely to reach higher-than-expected plasmatic concentrations of their active metabolite in UMs. Conversely, 7%–10% of Caucasians, those carrying the PM phenotype, are at risk for higher-than-expected drug plasma concentrations of a parent drug, because of delayed or absent CYP2D6 metabolism.
The varied and unpredictable analgesic profiles of codeine, dihydrocodeine, hydrocodone, oxycodone, and tramadol are predominantly explained by CYP2D6 and CYP3A4 metabolism. In recent years, there have been several reports associating CYP2D6 genotypes and near misses or fatal outcomes after opioid use.Citation30–Citation33 Adding to the complexity of the metabolic pathway of one drug, adverse outcomes have been noted as a result of multiple drug therapies interacting at the same CYP.Citation34
Codeine
Codeine is a prodrug with a low affinity and low intrinsic activity at the μ-opioid receptor (200 times and 50 times less than morphine, respectively).Citation35 It is classified as a weak opioid (World Health Organization class II), as it is a less potent μ-opioid receptor agonist than morphine. Codeine was initially prescribed because of the belief that this weak opioid is safe and would not result in adverse outcomes. For that reason, codeine has been considered a safe alternative to other opioids for outpatient pain management, and is still available in some countries as an over-the-counter medication, either alone or in combination with paracetamol (acetaminophen). Current use of codeine includes pediatric patientsCitation36 and treatment of postoperative pain, although large-scale evidence on efficacy is sparse and has been challenged by a recent meta-analysis.Citation37
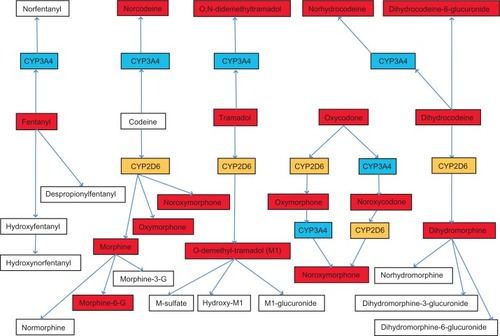
Codeine is a prodrug, and requires O-demethylation catalyzed by CYP2D6 to be converted into morphine and become analgesic; this metabolic pathway accounts for 10% of codeine clearance (). The conversion of codeine into norcodeine by CYP3A4 and into codeine-6-glucuronide by glucuronidation represents approximately 80% of codeine clearance. Morphine is further metabolized into morphine-6-glucuronide (M6G) and morphine-3-glucuronide; both morphine and M6G display opioid activity.
Figure 1 CYP metabolism involved in opioid clearance.
The clinical relevance of CYP2D6 genotyping to predict analgesic outcomes is still relatively unknown. In a recent pilot study, the relationship between CYP2D6 genotype, post-cesarean pain scores, codeine consumption, and side effects were evaluated.Citation38 The two extremes in CYP2D6 genotype seemed to predict pain response and/or adverse effects.
Individuals with an UM phenotype carry a risk for respiratory depression with codeine, particularly if CYP3A4 activity is inhibited by concomitant use of antibiotics or in the context of kidney dysfunction.Citation30 Several reports of fatalities after codeine prescription in pediatric cases with UM have been published in recent years: a 2-year-old boy died due to codeine overdose after a minor surgical procedure,Citation39 and a 29-month-old child of North African descent suffered major hypoxic brain injury following a dose of acetaminophen and codeine 2 days after an uneventful anesthetic for tonsillectomy.Citation40 By account of ethnic affiliation, the risk of this child of carrying a CYP2D6 gene duplication is increased about threefold compared to Caucasian subjects.Citation40
Perhaps the most striking report is that of the death of a breast-fed 13-day-old neonate following a morphine overdose because his mother was taking codeine after childbirth. This resulted in a recent FDA warning on codeine use in nursing mothers.Citation41 Toxic blood levels of morphine or its active metabolite M6G may arise in mothers and neonates that are CYP2D6 ultrarapid or extensive metabolizers. The mother was categorized as a CYP2D6 ultrarapid metabolizer and her breast milk had a morphine concentration of 87 ng/mL, the typical range being 1.9–20.5 ng/mL at doses of 60 mg codeine every 6 hours. The infant was categorized as a CYP2D6 extensive metabolizer (extensively metabolizing the prodrug codeine to morphine), and postmortem toxicology tests using gas-chromatography mass spectrometry revealed blood concentrations of morphine at 70 ng/mL. Sixty mg codeine/day for treatment of postpartum pain normally results in maximum morphine plasma concentrations of 2.2 ng/mL in breast-fed neonates.Citation42 In contrast, neonates prescribed morphine for analgesia displayed serum morphine concentrations of 10–12 ng/mL.Citation43 In a quantitative modeling study simulating the risk for neonates according to CYP2D6 genotypes, repeated codeine administration in a breast-feeding mother demonstrated that toxic plasma levels of morphine could be reached in 4 days.Citation44 The authors concluded that unmonitored use of codeine for postlabor pain in breast-feeding mothers should not be considered a safe practice.
Codeine and morphine clearance in breast-feeding mothers and their relation to CYP2D6 genotypes have been extensively commented on and evaluated.Citation43,Citation45–Citation47 Since 2007, the FDA has required manufacturers of prescription codeine products to state in the “Precautions” section of the drug label the risks of prescribing codeine to breast-feeding mothers.Citation48
An FDA-approved genetic test (AmpliChip CYP450: Roche Diagnostics, Palo Alto, CA) is commercially available to test genetic variants of CYP2D6.Citation49 Overall, the level of evidence linking gene variation (CYP2D6) to phenotype (increased biotransformation of codeine into morphine) is significant; however, there is no randomized clinical trial assessing the benefits of genetic testing prior to codeine therapy at large. In addition, while insufficient morphine formation from codeine resulting in failure of analgesia can currently be well predicted, extremely high morphine formation still requires the effort of combining genotyping with phenotyping.Citation50 Finally, the Clinical Pharmacogenetics Implementation Consortium has just published guidelines based on a focused review and interpretation of the literature by experts in the field ().Citation8
Table 1 Codeine therapy recommendations based on CYP2D6 phenotype
Dihydrocodeine
Dihydrocodeine, a semisynthetic opioid, undergoes similar metabolic pathways as its analog codeine. CYP2D6 catalyses O-demethylation to dihydromorphine, an active metabolite with an opioid receptor activity comparable to that of morphine. CYP3A4 catalyzes N-demethylation to nordihydrocodeine and nordihydromorphine.Citation26 Studies to evaluate CYP2D6 metabolism utilize quinidine to inhibit CYP2D6 metabolism, thus resulting in a PM phenotype; plasma concentrations of dihydromorphine were reduced three- to fourfold, and urinary excretion of dihydromorphine was decreased from 0.91% to 0.28% in the first 12 hours in quinidine-induced poor metabolizers.Citation51 Pain thresholds, however, were not different after a single dose of dihydrocodeine along with quinidine, suggesting that this metabolic pathway and biotransformation of dihydrocodeine into dihydromorphine may not be clinically important for analgesia.Citation51,Citation52
Hydrocodone
Hydrocodone is a synthetic opioid analog to dihydrocodeine. The production of the active metabolite hydromorphone from hydrocodone is reduced in CYP2D6 PMs.Citation53 In vitro studies show that the O-demethylation of hydrocodone is predominantly catalyzed by CYP2D6 and to a lesser extent by an unknown low-affinity cytochrome P450 enzyme.Citation54 Norhydrocodone formation is attributed in part to CYP3A4, and approximately 40% of the clearance of hydrocodone is via non-CYP pathways. In a volunteer trial, CYP2D6 EMs and PMs were equally responsive to oral hydrocodone, and quinidine had no consistent effect on their responses, even though quinidine abolished the preexisting metabolic differences in hydromorphone production, as measured in urine.Citation55
A recent case-report of a fatal hydrocodone overdose in a child demonstrated the effect of CYP2D6 genotype on hydrocodone clearance and highlights the complex interplay between pharmacogenetic factors and drug–drug interactions.Citation56 The child had a PM CYP2D6 phenotype and was treated with clarithromycin, a potent inhibitor of CYP3A4, for an ear infection. The concomitant medication resulted in a substantial reduction in hydrocodone clearance. The combination of reduced clearance with an inhibited CYP3A4 and a PM phenotype contributed to this fatal overdose. Overall, data regarding pain management and hydrocodone is sparse, and there is no recommendation for pharmacogenetic testing to improve hydrocodone’s efficacy and safety profile.
Tramadol
Tramadol, a synthetic analog of codeine and morphine, consists of two enantiomers, both of which contribute to analgesic activity via different mechanisms. (+)-Tramadol and the main metabolite (+)-O-demethyl-tramadol (M1) are agonists of the μ-opioid receptor. (+)-O-demethyl-tramadol’s affinity for μ-opioid receptors is approximately 200 times greater than that of the parent compound.Citation57 (+)-O-demethyl-tramadol is metabolized by CYP2D6, therefore the CYP2D6 genotype will influence the response to tramadol.Citation58–Citation65 (+)-Tramadol inhibits serotonin reuptake and (−)-tramadol inhibits nor-epinephrine reuptake, enhancing inhibitory effects on pain transmission in the spinal cord.
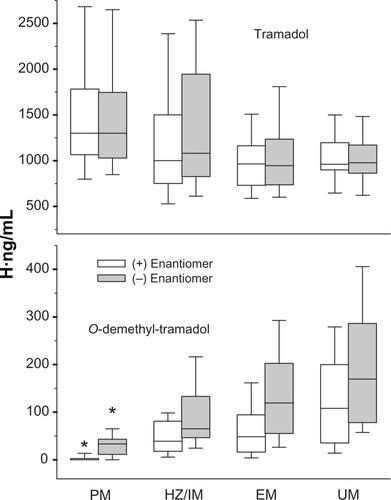
Clinical studies have demonstrated that response rates to tramadol are significantly lower in PM compared to EM individuals.Citation63 In a postoperative study evaluating the efficacy of tramadol, plasma concentrations of the enantiomers tramadol and O-demethyl-tramadol were measured 30, 90, and 180 minutes after tramadol was given.Citation64 Variability of O-demethyl-tramadol concentrations was correlated with CYP2D6 genotype (). Concomitant use of CYP2D6 inhibitors further contributed to variability of tramadol metabolism. Poor efficacy of tramadol analgesia with the need for rescue medication was increased fourfold in PMs. Intoxication or adverse effects after tramadol analgesia in individuals with CYP2D6 duplication have also been reported. Dizziness resulting in hospitalization, respiratory depression requiring naloxone, and a near-fatal cardiotoxicity following tramadol were reported in individuals that were genotyped and found to be UMs.Citation31,Citation66,Citation67
Figure 2 Concentrations of tramadol and enantiomers in different CYP2D6 genotypes. Adapted with permission from Macmillan Publishers Ltd: Stamer et al. Clin Pharmacol Ther. 2007; 82:41–47.Citation64
Some similarities with codeine were found with regards to lactating mothers and O-demethyl-tramadol transfer in breast milk.Citation68 In women treated with tramadol 50 or 100 mg four to six times daily, the calculated mean O-demethyl-tramadol concentration in milk was 1187 nmol/L for EMs and 602 nmol/L for PMs, which are close to measured values reported in a pharmacokinetic modeling study.Citation69 Mean estimates of relative infant dose of tramadol in EM mothers were 2.16%, in PM mothers 2.6%, and of O-demethyl-tramadol 0.93% and 0.47%, respectively.Citation68 Since none of the infant dose in tramadol equivalents was higher than the generally suggested 10% limit, maternal tramadol administration is considered safe, although the authors did recommend caution in individual infants.Citation68
In addition to CYP2D6, the organic cation transporter OCT1 also contributes to the pharmacokinetics of O-demethyl-tramadol. OCT1 is most abundantly expressed in the liver and mediates the cellular uptake of this active tramadol metabolite.Citation70 The O-demethyl-tramadol uptake in vitro is 2.4-fold higher in OCT1-overexpressing cells than in control cells. In vivo common genetic polymorphisms of this transporter resulting in reduced or absent OCT1 activity were correlated with higher plasma concentrations of O-demethyl-tramadol and a prolonged opioid-induced miosis. These data suggest that OCT1 activity is related to hepatic reuptake of O-demethyl-tramadol before glucuronidation and elimination.Citation70,Citation71 More work has to be done in this field to understand the complex interplay between CYP2D6 genotypes, the influence of OCT1, and other candidate genes.
Oxycodone
Oxycodone is a semisynthetic opioid agonist and is widely used as an analgesic for both acute and chronic pain. Both oxycodone and oxymorphone, one of its metabolites, are potent analgesics used for chronic pain. Since the introduction of controlled-release oxycodone in 1995, annual prescriptions of oxycodone have steadily increased several-fold.Citation72 Oxy-codone undergoes metabolism in the liver through four different metabolic pathways catalyzed by CYP3A4 and CYP2D6 (). N-demethylation of oxycodone by CYP3A4 into noroxycodone is quantitatively the most important metabolic route (45% ± 21%), while a smaller fraction (11% ± 6%) of oxycodone is O-demethylated to oxymorphone by CYP2D6.Citation73 The resulting metabolites, when compared to morphine, have different affinities for the μ-opioid receptor,Citation74 from highest to lowest: oxymorphone > morphine > noroxymorphone > oxycodone > noroxycodone. The importance of an intact CYP3A4 pathway for oxycodone clearance has been emphasized in numerous pharmacokinetic studies.Citation73,Citation75–Citation80 Many drugs,Citation79–Citation86 as well as grapefruit juice intake,Citation87 have been shown to interfere with this pathway. Noroxymorphone is a metabolite of noroxycodone and oxymorphone that is a potent μ-agonist when administered intrathecally, but that lacks analgesic activity after systemic administration, probably because of an a priori poor blood–brain barrier penetration.Citation88 Early studies describing the impact of CYP2D6 metabolism (phenotype) on clinical outcomes of oxycodone (analgesia and side effects) have demonstrated a weaker effect in PMs.Citation89,Citation90 Anecdotic cases of adverse effects after oxycodone in CYP2D6 PMs have been reported.Citation91
Despite its widespread and increasing use for pain management and postoperative analgesia, evidence related to the pharmacogenetic influence of CYP3A4 and CYP2D6 on the clinical response (analgesic and side-effect profile) of oxycodone or oxymorphone is particularly scarce. Oxycodone analgesia and side effects were evaluated in ten healthy Caucasian volunteers (all men) phenotyped and genotyped for CYP2D6.Citation92 Experimental pain tests were performed in a five-arm crossover, randomized, double-blinded, placebo-controlled manner, with oral oxycodone 0.2 mg/kg. Differences in analgesia were found with increased analgesic effects in UMs; conversely, PMs had a two- to twentyfold reduction of analgesia compared to EMs. Notable differences in the incidence of spontaneously reported adverse reactions after oxycodone were reported by 2/2 UM, in comparison to only 1/6 EM and no toxicity reported in IM and PM (0/2). Importantly, CYP3A4 blockade, such as that which occurs with itraconazole, increased the analgesic efficacy of oxycodone as well as the toxicity of oxycodone, especially in CYP2D6 UMs. These findings are consistent with reports of life-threatening events in ultrarapid metabolizers receiving codeine.Citation30,Citation39,Citation41
The effects of itraconazole, an inhibitor of the CYP3A4-mediated N-demethylation of oxycodone, were evaluated after administration of oxycodone (0.1 mg IV and 10 mg orally) in eleven healthy Caucasian subjects.Citation86 Itraconazole affected the metabolism of oxycodone to a greater extent when oxycodone was given orally. As a result, dose adjustments of oral oxycodone may be necessary in CYP3A4 poor metabolizers to avoid opioid-related adverse effects.
Another report on the effect of oxycodone analgesia according to CYP2D6 genotype evaluated 33 healthy Caucasian volunteers undergoing nociceptive tests (five experimental modalities) in a placebo-controlled double-blinded study.Citation93 All subjects were evaluated after receiving either placebo or 20 mg oxycodone orally during two separate study sessions in a randomized fashion. Subjects were classified into two groups (rather than the four possible genotypic groups based on allelic function): intermediate, extensive, and ultrarapid metabolizers were pooled into a composite group (called “EM”); and poor metabolizers (PM) were analyzed separately according to CYP2D6 genotype and pharmacokinetic assays. Oxycodone resulted in marked analgesia to all pain modalities in all subjects, with a difference in the extent of analgesia depending on the pain modality. The analgesic effect of oxycodone was less pronounced in the 16 PM subjects, mainly due to a marked increase in analgesia in EM subjects occurring 1–2 hours after the oxycodone dose. The results indicate that oxycodone metabolism to oxymorphone contributes to the analgesic effect but is not responsible for all of its effect.
A follow-up study by the same authors investigated the pharmacogenetic effect of CYP2D6 on oxycodone for postoperative analgesia.Citation94 A total of 270 Caucasian patients undergoing surgery received postoperative analgesia with intravenous oxycodone via IV patient-controlled analgesia (PCA) for 24 hours. There was no difference in overall oxycodone consumption, pain ratings, or side effects between genotype groups despite a significant difference in plasma concentrations. The mean oxymorphone/oxycodone ratio was substantially higher in EM compared to PM subjects. One of the shortcomings of this study is that no genetic test for the UM status was performed, and possibly individuals might have been misclassified to the EM group. Furthermore, pain scores and analgesic consumption were low, and a differentiation of genotypes might not have been possible due to overall low analgesic needs. In another recent study in Caucasian cancer patients managed with oral oxycodone, oxymorphone/oxycodone ratios differed between genotypes. However, this did not translate into any measurable difference in clinical outcomes (pain intensity, nausea, tiredness, or cognitive function).Citation95
Overall, the level of evidence linking genetic variability (CYP2D6 and CYP3A4) to phenotype (altered biotransformation of oxycodone into oxymorphone and overall clearance of oxycodone and oxymorphone) is strong; however, there has been no randomized clinical trial on the benefits of genetic testing prior to oxycodone therapy. There is also no warning on the oxycodone label cautioning against prescription of oxycodone in CYP2D6 UMs or in patients taking CYP3A4 inhibitors concomitantly. Given the widespread use and potential abuse of oxycodone prescription, further studies should certainly investigate this phenotype/genotype association.
Methadone
Methadone is a synthetic opioid best known for its use in the treatment of opioid dependence and is considered a second-line option in the setting of neuropathic pain in cancer patients.Citation96,Citation97 Methadone occurs in R- and S-enantiomeric forms, with essentially all of its activity due to R-methadone. Both enantiomers bind to the noncompetitive site of the N-methyl-d-aspartate receptor;Citation26 however, R-methadone (levomethadone) is a tenfold stronger μ-opioid receptor agonist than S-methadone.Citation98 S-methadone on the other hand seems to be related to side effects (eg, increased QTc intervals in the electrocardiogram).Citation99 The N-methyl-d-aspartate antagonistic effect explains the popularity of methadone as second-line opioid, and its place in opioid switching when conventional opioids fail to provide satisfactory pain relief.Citation100 With regard to methadone metabolism, a great variation in plasma concentration of the different enantiomers has been shown. CYP3A4 and CYP2B6 are the major CYP isoforms involved in methadone metabolism, with CYP2D6 only contributing in a negligible manner, with close to no impact on methadone dosage requirements.Citation101–Citation104 ABCB1 genetic polymorphisms do contribute slightly to the interindividual variability of methadone kinetics.Citation102,Citation103,Citation105,Citation106 CYP2B6 activity is clearly associated with altered pharmacokinetics, clinical outcome and adverse effects.Citation107–Citation110 Methadone should be carefully administered in patients using CYP3A inhibitorsCitation104 or drugs inhibiting CYP2B6.Citation110
OPRM1 polymorphism, pain perception, and opioid analgesia
Among the numerous candidate genes that have been considered important in opioid response, the μ-opioid receptor gene (OPRM1) is probably the best studied. A common polymorphism of OPRM1 is a single nucleotide substitution at position 118, with an adenine substitution by a guanine (A118G) reported to occur with an allelic frequency of 10%–30% among Caucasians,Citation111 a higher prevalence among Asians,Citation112 and a lower one in African–Americans.Citation113 The major interest for this particular polymorphism is due to its pharmacological and physiological consequences; however, the exact mechanism by which the altered receptor influences opioid analgesia is still unresolved. In vitro studies have suggested that A118G polymorphism affects receptor binding characteristicsCitation114,Citation115 or messenger RNA expression levels;Citation116 however, under some experimental conditions, there was no effect on functionCitation117 or expression levels.Citation118 In a recent humanized mouse model exploring signal transduction pathways that mediate opioid pharmacology, sensory neurons expressing the 118GG gene displayed reduced morphine (but not fentanyl) potency and efficacy compared with the 118AA version. This suggests that the genetic effect is at least at the level of the sensory neurons.Citation119
Experimental pain
Individuals carrying the variant receptor gene (G118) could show differences in some of the functions mediated by β-endorphin action and exogenous opioids. Human volunteers (male and female) carrying a G118 allele exhibited lower sensitivity to pressure pain (ie, higher tolerance threshold to pressure pain) compared with A118 homozygotes.Citation120 However, the association between genotype and pain perception is not that simple; a significant interaction between sex and genotype for heat-pain ratings at 49°C was identified, indicating that the variant G118 allele was associated with lower pain ratings among men but higher pain ratings among women. A study in a Han Chinese cohort of healthy female volunteers demonstrated that pressure-pain threshold is influenced by another polymorphism of OPRM1 (IVS2 + A31G) but not the A118G polymorphism.Citation121 Other studies assessing the influence of genetic variants on experimental pain demonstrated no effect of OPRM1 A118G genotype on pain processingCitation122 or lower pain-tolerance thresholds to single electrical nerve stimulation in individuals carrying the G118 allele.Citation123 It has been determined that the effect size of various determinants for experimental pain perception is greatest for heat sensitization by capsaicin, followed by gender (higher pain sensitivity in women) and a more modest effect size for genetic determinants.Citation33 Therefore, cautious interpretation of experimental pain tests should take into account ethnicity (population admixture), the noxious stimulus, and gender, as well as possible linkage disequilibrium with other polymorphisms that may represent the true functional genetic variant.
Neuraxial opioids for labor analgesia
Using the up–down sequential allocation model to identify differences in analgesic requirement according to OPRM1 genotype in women requesting neuraxial analgesia early in labor, women carrying the G118 allele required substantially lower doses of spinal fentanyl, with a 1.5-fold difference compared to wild types.Citation124 This finding was replicated with a different pharmacological study design using random-dose allocation, with a twofold difference between genetic groups.Citation124 Of note, cervical dilatation at the time of analgesia request was significantly less in 118 AA women than that in women carrying one or two variant alleles (118 AG or 118 GG). The finding of lower analgesic requirements at a more advanced stage in labor is consistent with the principle that women carrying the G118 allele may have higher pain tolerance that allows them to wait longer before requesting epidural analgesia. Therefore, according to our findings, genotyping may help in improving labor analgesia, because 30% of Caucasian women (and probably a vast majority of Asian women) may in fact require significantly lower doses of spinal fentanyl during labor. On the other hand, the duration of spinal fentanyl analgesia does not appear to be influenced by A118G genotype,Citation125 suggesting that this SNP may influence spinal fentanyl potency without affecting the duration of analgesic action. Using the same methodology, a recent study demonstrated a similar pharmacogenetic association, although with a more modest effect, with lower dose requirement for epidural sufentanil in women carrying the variant G allele.Citation126
Spinal and systemic morphine for postoperative analgesia
The effect of the A118G polymorphism of OPRM1 on postcesarean analgesia after spinal and IV morphine was also evaluated in three recent studies with variable outcomes.Citation125,Citation127,Citation128 One study found no differences in the duration of spinal morphine analgesia, the need for analgesic supplementation or the incidence of nausea according to A118G genotype; however, pruritus was less frequent in carriers of the G118 allele during the first 24 hours.Citation125 In Asian women, however, with a slightly different analgesic regimen, G118 carriers exhibited increased 24-hour postoperative consumption of morphine via IV PCA.Citation127 In a multiple regression analysis, the most important factor contributing to morphine usage was maximum pain score, followed by ethnicity and A118G polymorphism.Citation129 After correction for genotype, ethnicity was still a significant contributing factor, with Indian women reporting higher pain scores and using higher doses of IV morphine.
Although the analysis and interpretation of specific allelic combination of multiple SNPs is often challenging,Citation130,Citation131 morphine consumption via IV PCA for management of acute postoperative pain, in the nonobstetric context, has been shown to be higher in patients carrying the G118 allele.Citation132–Citation135 The effect may be modest and not clinically relevant.
Overall, inconsistent findings across studies investigating opioid analgesia according to OPRM1 genotype may be due to the fact that spinal and systemic opioid pharmacokinetics and pharmacodynamics may be different; enhanced analgesia in response to spinal fentanyl in the presence of the G118 allele may not exist in response to IV fentanyl or other opioids via the IV route. Or one could speculate that human spinal cord receptor function and signal transduction is selectively more altered by the G118 variant than supraspinal receptors. Another potential explanation and factor to bear in mind is the different nature of the nociceptive stimulus in labor (predominantly a visceral component in early labor) versus other painful syndromes.
Systemic fentanyl for postoperative analgesia
Recent studies evaluating postoperative IV consumption of fentanyl according to A118G polymorphism of OPRM1 after surgery in various Asian cohorts revealed lower fentanyl requirements in A118G-homozygous individuals ().Citation136–Citation139 Potential explanations for these varying findings are that labor pain is different from that tested by experimental models of pain or that experienced in other clinical settings (postoperative or chronic pain), or that the response to systemic administration of fentanyl, rather than spinal, is affected differently by OPRM1 genotype. Alternatively, it may be that other factors, including ethnicity, influence the effect of genetic variants of OPRM1.
Table 2 OPRM1 genotype and fentanyl requirement
In a Japanese cohort of healthy individuals undergoing surgery, a baseline preoperative cold pressor test was better tolerated in 118 AA individuals, and the response to fentanyl was enhanced in these subjects; however, there was no difference in pain ratings or fentanyl consumption during the first 24 hours after surgery.Citation138 Women, on the other hand, required more fentanyl postoperatively than men. Another polymorphism of the OPRM1 gene (IVS3 + A8449G SNP in intron 3), present in 22% of individuals in this cohort, did alter the clinical effect of fentanyl, with a modest reduction of total postoperative IV PCA use of fentanyl in carriers of the minor G allele of this SNP. A study in Han Chinese patients undergoing laparoscopic abdominal surgery concluded that individuals carrying the G118 allele have a shorter time to awakening and extubation, and experience reduced analgesic efficacy of fentanyl with no clinically significant changes in respiratory depression.Citation139 In another study in a Han Chinese cohort of women undergoing elective hysterectomies, pain thresholds after electric stimulation did not differ between genotypic groups; however, there was a difference for pain tolerance with this experimental model of pain. Pain-tolerance threshold was lower in women carrying the minor G118 allele, and there was no difference in postoperative pain scores; however, IV PCA fentanyl consumption was higher in women carrying the G118 allele.Citation136 The same authors did not find an association between A118G genotype and the incidence of nausea and vomiting caused by fentanyl for postoperative pain.Citation140
Finally, subjects carrying the G118 allele complained of more severe pain during shock-wave lithotripsy, despite self-administration of higher doses of alfentanil, reaching higher plasma alfentanil concentrations. This indicates that carriers of the minor G118 allele may experience impaired analgesia in response to alfentanil.Citation141 The advantage of this model of clinical pain and anesthetic protocol resides in the fact that patients received only alfentanil, and therefore pharmacokinetic/dynamic interactions resulting from concomitant medications are unlikely to have confounded the findings.
Morphine for cancer pain
Screening for A118G genotype in a cohort of cancer patients on oral morphine initially revealed that individuals homozygous for the G118 allele required higher morphine doses for adequate pain control.Citation142 In addition, combining this genotype with other gene variants (ABCB1 or COMT) seemed to confirm an association of these polymorphisms with morphine requirements.Citation143,Citation144 However, subsequent larger trials did not confirm that oral morphine consumption for chronic pain (eg, cancer pain) could be reliably predicted by A118G genotype.Citation145,Citation146 In particular, a large European multicenter study found no association between 112 SNPs in 25 candidate genes, including OPRM1 and COMT, and opioid dose (morphine, oxycodone, or fentanyl primarily) in a cohort of 2294 cancer patients.Citation145 While no joint combined allelic combination was evaluated, this trial does fail to validate associations related to opioid efficacy reported in several previous association studies, and with the current body of knowledge argues against including pharmacogenetic testing for improvements in clinical decision-making for opioid prescription.
COMT gene, pain and opioid analgesia
Among the usual candidate genes proposed, the Val158Met polymorphism of the catechol-O-methyltransferase (COMT) gene that regulates the metabolism of dopamine and noradrenaline may be identified as potentially inferring an increased risk for the development of chronic pain disorders,Citation147 acute postoperative pain,Citation36,Citation135 chronic postsurgical pain,Citation148 and opioid-induced hyperalgesia.Citation149 High COMT activity, as found with the Val158 allele, is associated with improved dopaminergic transmission and has been suggested to confer an advantage in the processing of aversive stimuli or stressful conditions (warrior strategy), while Met158 alleles may be associated with an advantage in memory and attention tasks (worrier strategy).Citation150 Individuals homozygous for the Met158 allele display increased pain sensitivity, and there are findings of lower μ-opioid system activation during sustained pain.Citation151–Citation153 The interplay between COMT inhibition and pain sensitivity mediated by β2 and β3 adrenergic receptor modulation has been highlighted,Citation154 and response to propranolol for management of temporomandibular pain has been shown to be predicted by COMT haplotype.Citation155 In a recent study evaluating repeated thermal-pain stimulation before and after a single opiate dose in a Caucasian cohort, the Val158Met genotype did not influence the reaction to the initial noxious stimulus or the analgesic response to intravenous remifentanil administration.Citation149 However, after repeated heat stimulation and post-remifentanil administration, pain ratings in Met158 individuals were significantly higher, suggesting that initial pain response is not influenced by COMT and that differences may become apparent only after endogenous pain modulation is challenged. The increased pain sensitivity in Met158 individuals following remifentanil could result from reduced efficacy of endogenous pain modulation and/or increased susceptibility to opioid-induced hyperalgesia. The suggestion that the effect of COMT genotype on pain processing becomes apparent only when the pain modulation is challenged, such as occurs after repeated pain stimulation, was confirmed in a functional magnetic resonance imaging study investigating brain responses to thermal pain stimuli.Citation156
The future of personalized medicine
Contrasting results in human genetic studies of pain sensitivity have been shown to occur with each of the usual polymorphisms assessed.Citation157,Citation158 This illustrates the challenges in evaluating a genotype–phenotype association when the underlying genetic susceptibility is clearly polygenic, and genotyping of allelic combinations should be done concomitantly.Citation48 The phenotype is indeed complex in itself, representing subjective and multifactorial pain perception experiences and/or responses to pain-modulating drugs. Numerous candidate genes as well as elaborate models have been suggested for the study of the genetic component of pain. Nonetheless, due to the inherent complexity in the study of pain, involving different nociceptive modalities, gender differences, limitations in extrapolating data from animal models to human perception, interethnic and environmental differences in addition to the obvious polygenic nature of pain, it is the design and execution of large clinical studies analyzing multiple haplotypes simultaneously that remains the true challenge to date. Meanwhile, genome-wide association studies in the context of acute postoperative pain are being published,Citation159 and researchers are already actively working on gene therapies for chronic pain.Citation160–Citation162
Conclusion
To improve clinical outcomes based on pharmacogenetic testing in the context of pain therapies, genotyping of CYP isozymes is likely to become strongly recommended. The individual pharmacokinetic profile and possible drug–drug interactions with potentially devastating outcomes for opioids relying on CYP2D6 and CYP3A4 metabolism are well-recognized major variables influencing the pharmacotherapy of pain. On the other hand, predicting the analgesic response to morphine based on pharmacogenetic testing is more complex; though there was hope that simple genetic testing would allow tailoring morphine doses to provide optimal analgesia, this is unlikely to occur. Different polymorphisms clearly influence pain perception and behavior in response to pain. However, the response to analgesics also differs depending on the pain modality and the potential for repeated noxious stimuli, the opioid prescribed, and even its route of administration.
Acknowledgements
Ruth Landau is the recipient of Swiss National Foundation Research grant SNF 3200B0-114129 that funded in part the OPRM1 genetic research conducted in Switzerland. Pascal H Vuilleumier is the recipient of Swiss National Foundation Research grant SPUM 33CM30-1241117.
Disclosure
The authors declare no conflicts of interest.
References
- FlockhartDASkaarTBerlinDSKleinTENguyenATClinically available pharmacogenomics testsClin Pharmacol Ther20098610911319369936
- FruehFWAmurSMummaneniPPharmacogenomic biomarker information in drug labels approved by the United States food and drug administration: prevalence of related drug usePharmacotherapy20082899299818657016
- SimSCIngelman-SundbergMPharmacogenomic biomarkers: new tools in current and future drug therapyTrends Pharmacol Sci201132728121185092
- RellingMVKleinTECPIC: Clinical Pharmacogenetics Implementation Consortium of the Pharmacogenomics Research NetworkClin Pharmacol Ther20118946446721270786
- JohnsonJAGongLWhirl-CarrilloMClinical Pharmacogenetics Implementation Consortium Guidelines for CYP2C9 and VKORC1 genotypes and warfarin dosingClin Pharmacol Ther20119062562921900891
- ScottSASangkuhlKGardnerEEClinical Pharmacogenetics Implementation Consortium guidelines for cytochrome P450-452C19 (CYP2C19) genotype and clopidogrel therapyClin Pharmacol Ther20119032833221716271
- RellingMVGardnerEESandbornWJClinical Pharmacogenetics Implementation Consortium guidelines for thiopurine methyltransferase genotype and thiopurine dosingClin Pharmacol Ther20118938739121270794
- CrewsKRGaedigkADunnenbergerHMClinical Pharmacogenetics Implementation Consortium (CPIC) Guidelines for codeine therapy in the context of cytochrome P450 2D6 (CYP2D6) genotypeClin Pharmacol Ther20129132132622205192
- KehletHJensenTSWoolfCJPersistent postsurgical pain: risk factors and preventionLancet20063671618162516698416
- CavallariLJeongHBressARole of cytochrome P450 genotype in the steps toward personalized drug therapyPharmgenomics Pers Med20114123136
- NielsenCSStaudRPriceDDIndividual differences in pain sensitivity: measurement, causation, and consequencesJ Pain20091023123719185545
- SmithHSVariations in opioid responsivenessPain Physician20081123724818354715
- AngstMSPhillipsNGDroverDROpioid pharmacogenomics using a twin study paradigm: methods and procedures for determining familial aggregation and heritabilityTwin Res Hum Genet20101341242520874462
- NielsenCSStubhaugAPriceDDVassendOCzajkowskiNHarrisJRIndividual differences in pain sensitivity: genetic and environmental contributionsPain2008136212917692462
- FoulkesTWoodJNPain genesPloS Genet20084e100008618654615
- DiatchenkoLNackleyAGTchivilevaIEShabalinaSAMaixnerWGenetic architecture of human pain perceptionTrends Genet20072360561318023497
- CoxJJReimannFNicholasAKAn SCN9A channelopathy causes congenital inability to experience painNature200644489489817167479
- NilsenKBNicholasAKWoodsCGMellgrenSINebuchennykhMAaslyJTwo novel SCN9A mutations causing insensitivity to painPain200914315515819304393
- GoldbergYPPriceNNamdariRTreatment of Na(v) 1.7-mediated pain in inherited erythromelalgia using a novel sodium channel blockerPain2012153808522035805
- NguyenHNBregmanHBuchananJLDiscovery and optimization of aminopyrimidinones as potent and state-dependent Nav1.7 antagonistsBioorg Med Chem Lett2012221055106022209205
- GoldbergYPMacFarlaneJMacDonaldMLLoss-of-function mutations in the Nav1.7 gene underlie congenital indifference to pain in multiple human populationsClin Genet20077131131917470132
- FillingimRBKingCDRibeiro-DasilvaMCRahim-WilliamsBRileyJL3rdSex, gender, and pain: a review of recent clinical and experimental findingsJ Pain20091044748519411059
- Ingelman-SundbergMSimSCGomezARodriguez-AntonaCInfluence of cytochrome P450 polymorphisms on drug therapies: pharmacogenetic, pharmacoepigenetic and clinical aspectsPharmacol Ther200711649652618001838
- EichelbaumMIngelman-SundbergMEvansWEPharmacogenomics and individualized drug therapyAnnu Rev Med20065711913716409140
- WangBYangLPZhangXZHuangSQBartlamMZhouSFNew insights into the structural characteristics and functional relevance of the human cytochrome P450 2D6 enzymeDrug Metab Rev20094157364319645588
- ZhouSFPolymorphism of human cytochrome P450 2D6 and its clinical significance: part IIClin Pharmacokinet20094876180419902987
- DalyAKBrockmollerJBrolyFNomenclature for human CYP2D6 allelesPharmacogenetics199661932018807658
- StamerUMZhangLStuberFPersonalized therapy in pain management: where do we stand?Pharmacogenomics20101184386420504256
- SistonenJSajantilaALaoOCoranderJBarbujaniGFuselliSCYP2D6 worldwide genetic variation shows high frequency of altered activity variants and no continental structurePharmacogenet Genomics2007179310117301689
- GascheYDaaliYFathiMCodeine intoxication associated with ultrarapid CYP2D6 metabolismN Engl J Med20043512827283115625333
- StamerUMStuberFMudersTMusshoffFRespiratory depression with tramadol in a patient with renal impairment and CYP2D6 gene duplicationAnesth Analg200810792692918713907
- MogilJSBaileyALSex and gender differences in pain and analgesiaProg Brain Res201018614115721094890
- DoehringAKusenerNFluhrKNeddermeyerTJSchneiderGLotschJEffect sizes in experimental pain produced by gender, genetic variants and sensitization proceduresPloS One20116e1772421423693
- PintoNDolanMEClinically relevant genetic variations in drug metabolizing enzymesCurr Drug Metab20111248749721453273
- ThornCFKleinTEAltmanRBCodeine and morphine pathwayPharmacogenet Genomics20091955655819512957
- LeePJDelaneyPKeoghJSleemanDShortenGDCatecholamine-o-methyltransferase polymorphisms are associated with postoperative pain intensityClin J Pain2011279310120842020
- DerrySMooreRAMcQuayHJSingle dose oral codeine, as a single agent, for acute postoperative pain in adultsCochrane Database Syst Rev20104CD00809920393966
- VanderVaartSBergerHSistonenJCYP2D6 polymorphisms and codeine analgesia in postpartum pain management: a pilot studyTher Drug Monit20113342543221743374
- CiszkowskiCMadadiPPhillipsMSLauwersAEKorenGCodeine, ultrarapid-metabolism genotype, and postoperative deathN Engl J Med200936182782819692698
- VoronovPPrzybyloHJJagannathanNApnea in a child after oral codeine: a genetic variant – an ultra-rapid metabolizerPaediatr Anaesth20071768468717564651
- KorenGCairnsJChitayatDGaedigkALeederSJPharmacogenetics of morphine poisoning in a breastfed neonate of a codeine-prescribed motherLancet200636870416920476
- MenyRGNaumburgEGAlgerLSBrill-MillerJLBrownSCodeine and the breastfed neonateJ Hum Lact199392372408260056
- MadadiPKorenGCairnsJSafety of codeine during breast-feeding: fatal morphine poisoning in the breastfed neonate of a mother prescribed codeineCan Fam Physician200753333517872605
- WillmannSEdgintonANCoboekenKAhrGLippertJRisk to the breast-fed neonate from codeine treatment to the mother: a quantitative mechanistic modeling studyClin Pharmacol Ther20098663464319710640
- LotschJGeisslingerGA critical appraisal of human genotyping for pain therapyTrends Pharmacol Sci20103131231720483491
- MadadiPRossCJHaydenMRPharmacogenetics of neonatal opioid toxicity following maternal use of codeine during breastfeeding: a case-control studyClin Pharmacol Ther200985313518719619
- MadadiPShiraziFWalterFGKorenGEstablishing causality of CNS depression in breastfed infants following maternal codeine usePaediatr Drugs20081039940418998750
- LotschJFluhrKNeddermayerTDoehringAGeisslingerGThe consequence of concomitantly present functional genetic variants for the identification of functional genotype-phenotype associations in painClin Pharmacol Ther200985253018548001
- de LeonJSusceMTMurray-CarmichaelEThe AmpliChip CYP450 genotyping test: integrating a new clinical toolMol Diagn Ther20061013515116771600
- LotschJRohrbacherMSchmidtHDoehringABrockmollerJGeisslingerGCan extremely low or high morphine formation from codeine be predicted prior to therapy initiation?Pain200914411912419395173
- Wilder-SmithCHHufschmidEThormannWThe visceral and somatic antinociceptive effects of dihydrocodeine and its metabolite, dihydromorphine. A cross-over study with extensive and quinidine-induced poor metabolizersBr J Clin Pharmacol1998455755819663813
- WebbJARostami-HodjeganAAbdul-ManapRHofmannUMikusGKamaliFContribution of dihydrocodeine and dihydro-morphine to analgesia following dihydrocodeine administration in man: a PK-PD modelling analysisBr J Clin Pharmacol200152354311453888
- OttonSVSchadelMCheungSWKaplanHLBustoUESellersEMCYP2D6 phenotype determines the metabolic conversion of hydrocodone to hydromorphoneClin Pharmacol Ther1993544634727693389
- HutchinsonMRMenelaouAFosterDJCollerJKSomogyiAACYP2D6 and CYP3A4 involvement in the primary oxidative metabolism of hydrocodone by human liver microsomesBr J Clin Pharmacol20045728729714998425
- KaplanHLBustoUEBaylonGJInhibition of cytochrome P450 2D6 metabolism of hydrocodone to hydromorphone does not importantly affect abuse liabilityJ Pharmacol Exp Ther19972811031089103485
- MadadiPHildebrandtDGongIYFatal hydrocodone overdose in a child: pharmacogenetics and drug interactionsPediatrics2010126e986e98920837591
- GrondSSablotzkiAClinical pharmacology of tramadolClin Pharmacokinet20044387992315509185
- EnggaardTPPoulsenLArendt-NielsenLBrosenKOssigJSindrupSHThe analgesic effect of tramadol after intravenous injection in healthy volunteers in relation to CYP2D6Anesth Analg200610214615016368820
- Garcia-QuetglasEAzanzaJRSadabaBMunozMJGilICampaneroMAPharmacokinetics of tramadol enantiomers and their respective phase I metabolites in relation to CYP2D6 phenotypePharmacol Res20075512213017175164
- KirchheinerJKeulenJTBauerSRootsIBrockmollerJEffects of the CYP2D6 gene duplication on the pharmacokinetics and pharmacodynamics of tramadolJ Clin Psychopharmacol200828788318204346
- PedersenRSDamkierPBrosenKTramadol as a new probe for cytochrome P450 2D6 phenotyping: a population studyClin Pharmacol Ther20057745846715961977
- PedersenRSDamkierPBrosenKEnantioselective pharmacokinetics of tramadol in CYP2D6 extensive and poor metabolizersEur J Clin Pharmacol20066251352116763825
- StamerUMLehnenKHothkerFImpact of CYP2D6 genotype on postoperative tramadol analgesiaPain200310523123814499440
- StamerUMMusshoffFKobilayMMadeaBHoeftAStuberFConcentrations of tramadol and O-desmethyl-tramadol enantiomers in different CYP2D6 genotypesClin Pharmacol Ther200782414717361124
- WangGZhangHHeFFangXEffect of the CYP2D6*10 C188T polymorphism on postoperative tramadol analgesia in a Chinese populationEur J Clin Pharmacol20066292793116960721
- EichhornABarthJChronic dizziness in a pain patient – pharmacogenomic identification of tramadol as cause [German]Rehabilitation (Stuttg)20104939339521140323
- ElkalioubieAAllorgeDRobriquetLNear-fatal tramadol cardiotoxicity in a CYP2D6 ultrarapid metabolizerEur J Clin Pharmacol20116785585821691803
- SalmanSSySKIlettKFPage-SharpMPaechMJPopulation pharmacokinetic modeling of tramadol and its O-desmethyl metabolite in plasma and breast milkEur J Clin Pharmacol20116789990821394525
- IlettKFPaechMJPage-SharpMUse of a sparse sampling study design to assess transfer of tramadol and its O-desmethyl metabolite into transitional breast milkBr J Clin Pharmacol20086566166618294329
- TzvetkovMVSaadatmandARLotschJTegederIStinglJCBrockmollerJGenetically polymorphic OCT1: another piece in the puzzle of the variable pharmacokinetics and pharmacodynamics of the opioidergic drug tramadolClin Pharmacol Ther20119014315021562485
- LehtonenPStenTAitioOGlucuronidation of racemic O-desmethyl-tramadol, the active metabolite of tramadolEur J Pharm Sci20104152353020797434
- OlkkolaKTHagelbergNMOxycodone: new “old” drugCurr Opin Anaesthesiol20092245946219369865
- LalovicBKharaschEHofferCRislerLLiu-ChenLYShenDDPharmacokinetics and pharmacodynamics of oral oxycodone in healthy human subjects: role of circulating active metabolitesClin Pharmacol Ther20067946147916678548
- SamerCFDaaliYWagnerMThe effects of CYP2D6 and CYP3A activities on the pharmacokinetics of immediate release oxycodoneBr J Pharmacol201016090791820590587
- GronlundJSaariTIHagelbergNMNeuvonenPJLaineKOlkkolaKTEffect of inhibition of cytochrome P450 enzymes 2D6 and 3A4 on the pharmacokinetics of intravenous oxycodone: a randomized, three-phase, crossover, placebo-controlled studyClin Drug Investig201131143153
- GronlundJSaariTIHagelbergNMNeuvonenPJOlkkolaKTLaineKExposure to oral oxycodone is increased by concomitant inhibition of CYP2D6 and 3A4 pathways, but not by inhibition of CYP2D6 aloneBr J Clin Pharmacol201070788720642550
- KummerOHammannFMoserCSchallerODreweJKrahenbuhlSEffect of the inhibition of CYP3A4 or CYP2D6 on the pharmacokinetics and pharmacodynamics of oxycodoneEur J Clin Pharmacol201167637120857093
- LiukasAHagelbergNMKuusniemiKNeuvonenPJOlkkolaKTInhibition of cytochrome P450 3A by clarithromycin uniformly affects the pharmacokinetics and pharmacodynamics of oxycodone in young and elderly volunteersJ Clin Psychopharmacol20113130230821508859
- NieminenTHHagelbergNMSaariTIOxycodone concentrations are greatly increased by the concomitant use of ritonavir or lopinavir/ritonavirEur J Clin Pharmacol20106697798520697700
- NieminenTHHagelbergNMSaariTIRifampin greatly reduces the plasma concentrations of intravenous and oral oxycodoneAnesthesiology20091101371137819417618
- GronlundJSaariTHagelbergNEffect of telithromycin on the pharmacokinetics and pharmacodynamics of oral oxycodoneJ Clin Pharmacol20105010110819755414
- GronlundJSaariTIHagelbergNNeuvonenPJOlkkolaKTLaineKMiconazole oral gel increases exposure to oral oxycodone by inhibition of CYP2D6 and CYP3A4Antimicrob Agents Chemother2011551063106721173180
- HagelbergNMNieminenTHSaariTIVoriconazole drastically increases exposure to oral oxycodoneEur J Clin Pharmacol20096526327118836708
- HagelbergNMNieminenTHSaariTIInteraction of oxycodone and voriconazole – a case series of patients with cancer pain supports the findings of randomised controlled studies with healthy subjectsEur J Clin Pharmacol20116786386421221959
- NieminenTHHagelbergNMSaariTISt John’s wort greatly reduces the concentrations of oral oxycodoneEur J Pain20101485485920106684
- SaariTIGronlundJHagelbergNMEffects of itraconazole on the pharmacokinetics and pharmacodynamics of intravenously and orally administered oxycodoneEur J Clin Pharmacol20106638739720076952
- NieminenTHHagelbergNMSaariTIGrapefruit juice enhances the exposure to oral oxycodoneBasic Clin Pharmacol Toxicol201010778278820406214
- LembergKKSiiskonenAOKontinenVKYli-KauhaluomaJTKalsoEAPharmacological characterization of noroxymorphone as a new opioid for spinal analgesiaAnesth Analg200810646347018227301
- MaddocksISomogyiAAbbottFHayballPParkerDAttenuation of morphine-induced delirium in palliative care by substitution with infusion of oxycodoneJ Pain Symptom Manage1996121821898803381
- HeiskanenTOlkkolaKTKalsoEEffects of blocking CYP2D6 on the pharmacokinetics and pharmacodynamics of oxycodoneClin Pharmacol Ther1998646036119871425
- SusceMTMurray-CarmichaelEde LeonJResponse to hydrocodone, codeine and oxycodone in a CYP2D6 poor metabolizerProg Neuropsychopharmacol Biol Psychiatry2006301356135816631290
- SamerCFDaaliYWagnerMGenetic polymorphisms and drug interactions modulating CYP2D6 and CYP3A activities have a major effect on oxycodone analgesic efficacy and safetyBr J Pharmacol201016091993020590588
- ZwislerSTEnggaardTPNoehr-JensenLThe hypoalgesic effect of oxycodone in human experimental pain models in relation to the CYP2D6 oxidation polymorphismBasic Clin Pharmacol Toxicol200910433534419281600
- ZwislerSTEnggaardTPMikkelsenSBrosenKSindrupSHImpact of the CYP2D6 genotype on post-operative intravenous oxycodone analgesiaActa Anaesthesiol Scand20105423224019719813
- AndreassenTNEftedalIKlepstadPDo CYP2D6 genotypes reflect oxycodone requirements for cancer patients treated for cancer pain? A cross-sectional multicentre studyEur J Clin Pharmacol201268556421735164
- FareedACasarellaJAmarRVayalapalliSDrexlerKMethadone maintenance dosing guideline for opioid dependence, a literature reviewJ Addict Dis20102911420390694
- ShaiovaLBergerABlindermanCDConsensus guideline on parenteral methadone use in pain and palliative carePalliat Support Care2008616517618501052
- FredheimOMMoksnesKBorchgrevinkPCKaasaSDaleOClinical pharmacology of methadone for painActa Anaesthesiol Scand20085287988918331375
- AnsermotNAlbayrakOSchlapferJSubstitution of (R,S)-methadone by (R)-methadone: impact on QTc intervalArch Intern Med201017052953620308640
- QuigleyCOpioid switching to improve pain relief and drug tolerabilityCochrane Database Syst Rev20043CD00484715266542
- CollerJKJoergensenCFosterDJLack of influence of CYP2D6 genotype on the clearance of (R)-, (S)- and racemic-methadoneInt J Clin Pharmacol Ther20074541041717725248
- CrettolSDeglonJJBessonJABCB1 and cytochrome P450 genotypes and phenotypes: influence on methadone plasma levels and response to treatmentClin Pharmacol Ther20068066868117178267
- FonsecaFde la TorreRDiazLContribution of cytochrome P450 and ABCB1 genetic variability on methadone pharmacokinetics, dose requirements, and responsePloS One20116e1952721589866
- ShiranMRLennardMSIqbalMZContribution of the activities of CYP3A, CYP2D6, CYP1A2 and other potential covariates to the disposition of methadone in patients undergoing methadone maintenance treatmentBr J Clin Pharmacol200967293719133059
- CollerJKBarrattDTDahlenKLoennechenMHSomogyiAAABCB1 genetic variability and methadone dosage requirements in opioid-dependent individualsClin Pharmacol Ther20068068269017178268
- LevranOO”HaraKPelesEABCB1 (MDR1) genetic variants are associated with methadone doses required for effective treatment of heroin dependenceHum Mol Genet2008172219222718424454
- BuntenHLiangWJPounderDSeneviratneCOsseltonMDCYP2B6 and OPRM1 gene variations predict methadone-related deathsAddict Biol20111614214421158011
- BuntenHLiangWJPounderDJSeneviratneCOsseltonDOPRM1 and CYP2B6 gene variants as risk factors in methadone-related deathsClin Pharmacol Ther20108838338920668445
- LevranOPelesEHamonSRandesiMAdelsonMKreekMJCYP2B6 SNPs are associated with methadone dose required for effective treatment of opioid addictionAddict Biol Epub July 25, 2011
- WangSCHoIKTsouHHCYP2B6 polymorphisms influence the plasma concentration and clearance of the methadone S-enantiomerJ Clin Psychopharmacol20113146346921694616
- LandauRCahanaASmileyRMAntonarakisSEBlouinJLGenetic variability of mu-opioid receptor in an obstetric populationAnesthesiology20041001030103315087647
- TanECTanCHKarupathivanUYapEPMu opioid receptor gene polymorphisms and heroin dependence in Asian populationsNeuroreport20031456957212657887
- CrowleyJJOslinDWPatkarAAA genetic association study of the mu opioid receptor and severe opioid dependencePsychiatr Genet20031316917312960749
- KroslakTLaforgeKSGianottiRJHoANielsenDAKreekMJThe single nucleotide polymorphism A118G alters functional properties of the human mu opioid receptorJ Neurochem2007103778717877633
- BondCLaForgeKSTianMSingle-nucleotide polymorphism in the human mu opioid receptor gene alters beta-endorphin binding and activity: possible implications for opiate addictionProc Natl Acad Sci U S A199895960896139689128
- ZhangYWangDJohnsonADPappACSadeeWAllelic expression imbalance of human mu opioid receptor (OPRM1) caused by variant A118GJ Biol Chem2005280326183262416046395
- BeyerAKochTSchroderHSchulzSHolltVEffect of the A118G polymorphism on binding affinity, potency and agonist-mediated endocytosis, desensitization, and resensitization of the human mu-opioid receptorJ Neurochem20048955356015086512
- OertelBGKettnerMScholichKA common human micro-opioid receptor genetic variant diminishes the receptor signaling efficacy in brain regions processing the sensory information of painJ Biol Chem20092846530653519116204
- MahmoudSThorsellASommerWHPharmacological consequence of the A118G mu opioid receptor polymorphism on morphine- and fentanyl-mediated modulation of Ca(2) channels in humanized mouse sensory neuronsAnesthesiology20111151054106221926562
- FillingimRBKaplanLStaudRThe A118G single nucleotide polymorphism of the mu-opioid receptor gene (OPRM1) is associated with pressure pain sensitivity in humansJ Pain2005615916715772909
- HuangCJLiuHFSuNYAssociation between human opioid receptor genes polymorphisms and pressure pain sensitivity in femalesAnaesthesia2008631288129519032295
- VossenHKenisGRuttenBvan OsJHermensHLousbergRThe genetic influence on the cortical processing of experimental pain and the moderating effect of pain statusPloS One20105e1364121049025
- ZwislerSTEnggaardTPNoehr-JensenLThe antinociceptive effect and adverse drug reactions of oxycodone in human experimental pain in relation to genetic variations in the OPRM1 and ABCB1 genesFundam Clin Pharmacol20102451752419845769
- LandauRKernCColumbMOSmileyRMBlouinJLGenetic variability of the mu-opioid receptor influences intrathecal fentanyl analgesia requirements in laboring womenPain200813951418403122
- WongCAMcCarthyRJBlouinJLandauRObservational study of the effect of mu-opioid receptor genetic polymorphism on intrathecal opioid labor analgesia and post-cesarean delivery analgesiaInt J Obstet Anesth20101924625320171873
- CamorciaMCapognaGStirparoSBerrittaCBlouinJLLandauREffect of mu-opioid receptor A118G polymorphism on the ED50 of epidural sufentanil for labor analgesiaInt J Obstet Anesth201221404422153130
- SiaATLimYLimECA118G single nucleotide polymorphism of human mu-opioid receptor gene influences pain perception and patient-controlled intravenous morphine consumption after intrathecal morphine for postcesarean analgesiaAnesthesiology200810952052618719451
- TanECLimYTeoYYGohRLawHYSiaATEthnic differences in pain perception and patient-controlled analgesia usage for postoperative painJ Pain2008984985518550441
- TanECLimECTeoYYLimYLawHYSiaATEthnicity and OPRM variant independently predict pain perception and patient-controlled analgesia usage for post-operative painMol Pain200953219545447
- LandauROne size does not fit all: genetic variability of mu-opioid receptor and postoperative morphine consumptionAnesthesiology200610523523716871054
- LandauROrtnerCCarvalhoBChallenges in interpreting joined allelic combinations of OPRM1 and COMT genesAnesth Analg201111343221788333
- ChouWYWangCHLiuPHLiuCCTsengCCJawanBHuman opioid receptor A118G polymorphism affects intravenous patient-controlled analgesia morphine consumption after total abdominal hysterectomyAnesthesiology200610533433716871067
- ChouWYYangLCLuHFAssociation of mu-opioid receptor gene polymorphism (A118G) with variations in morphine consumption for analgesia after total knee arthroplastyActa Anaesthesiol Scand20065078779216879459
- CoulbaultLBeaussierMVerstuyftCEnvironmental and genetic factors associated with morphine response in the postoperative periodClin Pharmacol Ther20067931632416580900
- KolesnikovYGabovitsBLevinAVoikoEVeskeACombined catechol-O-methyltransferase and mu-opioid receptor gene polymorphisms affect morphine postoperative analgesia and central side effectsAnesth Analg201111244845321127283
- ZhangWChangYZKanQCAssociation of human micro-opioid receptor gene polymorphism A118G with fentanyl analgesia consumption in Chinese gynaecological patientsAnaesthesia20106513013520003118
- FukudaKHayashidaMIkedaKKoukitaYIchinoheTKanekoYDiversity of opioid requirements for postoperative pain control following oral surgery – is it affected by polymorphism of the mu-opioid receptor?Anesth Prog20105714514921174568
- FukudaKHayashidaMIdeSAssociation between OPRM1 gene polymorphisms and fentanyl sensitivity in patients undergoing painful cosmetic surgeryPain200914719420119783098
- WuWDWangYFangYMZhouHYPolymorphism of the micro-opioid receptor gene (OPRM1 118 A > G) affects fentanyl-induced analgesia during anesthesia and recoveryMol Diagn Ther20091333133719791836
- ZhangWYuanJJKanQCZhangLRChangYZWangZYStudy of the OPRM1 A118G genetic polymorphism associated with postoperative nausea and vomiting induced by fentanyl intravenous analgesiaMinerva Anestesiol201177333921150856
- GinosarYDavidsonEMMerozYBlotnickSShachamMCaracoYMu-opioid receptor (A118G) single-nucleotide polymorphism affects alfentanil requirements for extracorporeal shock wave lithotripsy: a pharmacokinetic-pharmacodynamic studyBr J Anaesth200910342042719605407
- KlepstadPRakvagTTKaasaSThe 118 A > G polymorphism in the human mu–opioid receptor gene may increase morphine requirements in patients with pain caused by malignant diseaseActa Anaesthesiol Scand2004481232123915504181
- CampaDGioiaATomeiAPoliPBaraleRAssociation of ABCB1/MDR1 and OPRM1 gene polymorphisms with morphine pain reliefClin Pharmacol Ther20088355956617898703
- Reyes-GibbyCCSheteSRakvagTExploring joint effects of genes and the clinical efficacy of morphine for cancer pain: OPRM1 and COMT genePain2007130253017156920
- KlepstadPFladvadTSkorpenFInfluence from genetic variability on opioid use for cancer pain: a European genetic association study of 2294 cancer pain patientsPain20111521139114521398039
- LotschJvon HentigNFreynhagenRCross-sectional analysis of the influence of currently known pharmacogenetic modulators on opioid therapy in outpatient pain centersPharmacogenet Genomics20091942943619514130
- BelferISegallSCOMT genetic variants and painDrugs Today (Barc)20114745746721695287
- HickeyOTNugentNFBurkeSMHafeezPMudrakouskiALShortenGDPersistent pain after mastectomy with reconstructionJ Clin Anesth20112348248821911195
- JensenKBLonsdorfTBSchallingMKosekEIngvarMIncreased sensitivity to thermal pain following a single opiate dose is influenced by the COMT val(158)met polymorphismPloS One20094e601619547755
- SteinDJNewmanTKSavitzJRamesarRWarriors versus worriers: the role of COMT gene variantsCNS Spectr20061174574817008817
- DiatchenkoLNackleyAGSladeGDCatechol-O-methyltransferase gene polymorphisms are associated with multiple pain-evoking stimuliPain200612521622416837133
- ZubietaJKHeitzegMMSmithYRCOMT val158 met genotype affects mu-opioid neurotransmitter responses to a pain stressorScience20032991240124312595695
- AndersenSSkorpenFVariation in the COMT gene: implications for pain perception and pain treatmentPharmacogenomics20091066968419374521
- NackleyAGTanKSFechoKFloodPDiatchenkoLMaixnerWCatechol-O-methyltransferase inhibition increases pain sensitivity through activation of both beta2- and beta3-adrenergic receptorsPain200712819920817084978
- TchivilevaIELimPFSmithSBEffect of catechol-O-methyltransferase polymorphism on response to propranolol therapy in chronic musculoskeletal pain: a randomized, double-blind, placebo-controlled, crossover pilot studyPharmacogenet Genomics20102023924820216107
- LoggiaMLJensenKGollubRLWasanADEdwardsRRKongJThe catechol-O-methyltransferase (COMT) val158 met polymorphism affects brain responses to repeated painful stimuliPloS One20116e2776422132136
- WalterCLotschJMeta-analysis of the relevance of the OPRM1 118A > G genetic variant for pain treatmentPain200914627027519683391
- KimHClarkDDionneRAGenetic contributions to clinical pain and analgesia: avoiding pitfalls in genetic researchJ Pain20091066369319559388
- KimHRamsayELeeHWahlSDionneRAGenome-wide association study of acute post-surgical pain in humansPharmacogenomics20091017117919207018
- WolfeDWechuckJKriskyDMataMFinkDJA clinical trial of gene therapy for chronic painPain Med2009101325133019818042
- GloriosoJCFinkDJGene therapy for pain: introduction to the special issueGene Ther20091645345419357693
- FinkDJWechuckJMataMGene therapy for pain: results of a phase I clinical trialAnn Neurol20117020721221796661