
Abstract
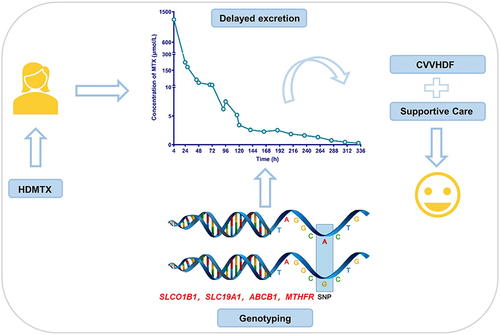
High-dose methotrexate (HDMTX) is a pivotal component of the chemotherapeutic regimens of osteosarcoma. However, the use of HDMTX is limited by an increased risk of dose-dependent toxicity. It is thought that the plasma levels and therapy-related toxicity of MTX could be associated with single nucleotide polymorphisms (SNPs) within MTX metabolism pathway genes. Here, we report a case of a paediatric osteosarcoma girl with delayed MTX excretion who was successfully managed using supportive measures and continuous veno-venous haemodiafiltration. We further identified the cause that could account for delayed elimination by genotyping analysis. The results showed that variations have been found in SLCO1B1, SLC19A1, ABCB1 and MTHFR, all those were reported to have a strong association with delayed elimination of MTX in clinical studies. After comprehensive consideration of genotype and clinical phenotype, the second course of HDMTX was administered to this patient at a half reduced dose. We also performed a literature review to summarize the pharmacogenetic factors that influence HDMTX pharmacokinetics or MTX-related adverse effects in osteosarcoma patients. It is suggested that the potential risk of delayed MTX elimination is worthy of clinical attention, and the implementation of genotyping should be considered to ensure therapeutic safety.
Graphical Abstract
Introduction
Osteosarcoma (OS) is the most common malignant bone tumour and mostly affects teenagers.Citation1 High-dose methotrexate (HDMTX) combined with doxorubicin and cisplatin is the “gold standard” chemotherapy for osteosarcoma.Citation2 Unfortunately, because the dose of HDMTX (8–12 g/m2) is dozens of times more than the common dose, patients receiving this strategy often suffer from significant toxicities of the kidneys, the liver and gastrointestinal tract as well.Citation3 Therefore, supportive measures, including folate supplementation, fluid hyperhydration, and urine alkalization before and during MTX treatment, are used to facilitate renal elimination to reduce HDMTX-related toxicities.Citation4 Nevertheless, there is still considerable interpatient variability in the clearance of HDMTX, with severe delayed MTX excretion seen from 0.86 to 1.8% in youths with OS.Citation5 Factors including age, hydration status and the concurrent use of nephrotoxic agents are shown to influence MTX clearance.Citation6 Furthermore, recent pharmacogenetic studies have investigated the effects of several genes and polymorphisms on MTX clearance,Citation7,Citation8 which may help us to better understand the pharmacokinetic variability and improve patient outcomes.
Here, we report a case of paediatric osteosarcoma in whom delayed MTX excretion was successfully managed using continuous veno-venous haemodiafiltration (CVVHDF) and supportive measures. Most importantly, polymorphisms in genes encoding transporter proteins or folate pathway genes partially account for delayed MTX excretion. According to the pharmacogenetic results, a reduced MTX dose (6 g/m2) was optimized for the second course of chemotherapy and completed uneventfully.
Case Summary
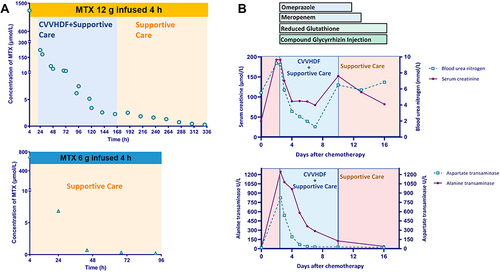
A 12-year-old girl was diagnosed with osteosarcoma of the right proximal femur and received chemotherapy in our department of haematology and oncology. Her laboratory test results, including the indicators of liver and kidney function, were all in the normal range. Her first course of HDMTX was administered at 12 g/m2. Six hours before MTX infusion, she was intravenously hydrated with 500–1000 mL/m2 of 5% glucose together with 5 mL/kg of 5% NaHCO3 solution. MTX was dissolved in 500 mL of D5W and infused over 4 hours. After this MTX infusion, she was hydrated with the same fluid to a total of 3000–4000 mL/m2 per day during the first 48 hours. Her 4-hour MTX level was 1270.08 μmol/L. Her 24-hour and 28-hour MTX levels were 224.64 and 181.4 μmol/L, respectively (). Thus, leucovorin was immediately escalated to 200 mg/m2 and administered every 6 hours. The girl developed acute kidney injury (AKI) with an increasing serum creatinine level of 197 μmol/L (). She also suffered from acute liver failure with prothrombin activity less than 40%, an increased ALT and AST levels (1247 U/L and 823 U/L, respectively, ). She was recommended to be transferred to pediatric intensive care unit (PICU) for CVVHDF management. Furthermore, repeated blood routine tests showed that the number of white blood cells, the proportion of neutrophils and the PCT levels were significantly higher than normal. The patient developed a fever, so bacteremia was considered, and meropenem was used to protect against infection. During CVVHDF, omeprazole was given to protect the stomach, atomolan and compound glycyrrhizin were administered to protect the liver, and leucovorin rescue was continued at a dose that was administered according to the MTX concentration. After a total of 5 days for CVVHDF, serum ALT and AST levels were decreased to 285 U/L and 30 U/L, respectively, and the serum creatinine level was 79.9 μmol/L (). The MTX concentration was decreased to 2.28 μmol/L. Then the patient was transferred back to the general ward for further treatment. Over the following hospital days, her MTX level decreased very slowly and finally reached to 0.28 μmol/L after 14 days of high-dose leucovor in rescue (). Another two days later, indicators of liver and kidney function returned to normal.
Figure 1 Time course of plasma methotrexate concentrations (A) and medications and liver/renal function (B).
To identify the cause that could account for delayed elimination and to explore a suitable dosage strategy for the next chemotherapy of MTX, we selected the following candidate genetic variants, rs1051296 in SLC19A1; rs4149056 and rs11045879 in SLCO1B1; rs1045642, rs2032582 and rs1128503 in ABCB1; rs717620 in ABCC2; rs1801131 and rs1801133 in MTHFR, for genotyping by real-time PCR. As shown in , variations have been found in SLCO1B1, SLC19A1, ABCB1 and MTHFR, all of which were reported to have a strong association with delayed elimination of MTX in clinical studies.
Table 1 Genotype of the Targeted SNPs
After comprehensive consideration of genotype and clinical phenotype, the second course of HDMTX was administered to this patient at a half reduced dose (6 g/m2). The 4-hour and 24-hour MTX levels were 699.84 and 6.84 μmol/L, respectively. Continuous leucovorin rescue was performed according to the MTX concentration. After 3 days, the MTX level was decreased to 0.22 μmol/L (). Following recovery, she proceeded to chemotherapy comprising of cisplatin (60 mg/m2·d) and epirubicin (37.5 mg/m2·d) and completed the course uneventfully.
Discussion
Although HDMTX (8–12 g/m2) has been shown to be the most effective single agent in the neoadjuvant therapy of OS, delayed excretion of MTX can result in life-threatening toxicity that may lead to treatment cessation, irreversible organ damage, and even death. As it excreted primarily by renal route, the precipitation of MTX or its relatively insoluble metabolites in the renal tubules might be one of the most likely mechanisms for acute nephrotoxicity and then result in delayed excretion.Citation9 More important, delayed MTX excretion may occur in the absence of any predisposing factor.Citation6 In this case, the girl suffered from “severe” delayed excretion (C24h >50 μmol/L) and acute liver and kidney injury. She was successfully managed using supportive cares and CVVHDF.
The pharmacokinetics of HDMTX showed large individual variability. A reduced effective blood volume or the concurrent use of nephrotoxic agents were known to be related to the development of delayed MTX excretion.Citation10 However, the patient had no signs of decreased blood volume and did not receive any nephrotoxic agent. Before administration, her renal function was normal, and her hydration status was standard. The reason for delayed MTX excretion is worth exploring. Recently, growing evidence suggested that genetic variants of metabolic enzymesCitation11,Citation12 or transportersCitation13,Citation14 involved in MTX elimination could provide a mechanistic explanation for the variability of its pharmacokinetics. Furthermore, these variants might be potential predictors for personalized pharmacotherapy. Therefore, we focused on the pharmacogenomics of MTX to illustrate the causes of delayed MTX elimination.
Generally, pharmacogenetic studies have identified various genes that contribute to the vast interindividual variation in MTX pharmacokinetics and are mainly involved in transporter genes (SLCO1B1, SLC19A1, ABCB1, and ABCC2) or folate pathway genes (MTHFR, MTR, MTRR, and DHFR). However, those studies that focused on OS patients were very limited. We first searched PubMed with a combination of the keywords “pharmacogenetic” AND “methotrexate” AND “osteosarcoma”; the information of these studies is summarized and presented in . Of those genes, the SNPs on ABCG2,Citation7 ABCB1, ABCC3,Citation15 and SLCO1B1Citation16 were associated with MTX-PK parameters. Other genetic variants, such as MTHFR (rs1801133), RFC1 (rs1051266), GSTP1 (rs1695), and MTR (rs1805087) were shown to be associated with an increased risk of HDMTX-related adverse effects.Citation17–23 In addition, rs4148416 in ABCC3 and three SNPs in ABCB1, rs4148737, rs1128503 and rs10276036 were associated with overall survival.Citation24
Table 2 Pharmacogenetic Literatures Information of HD-MTX in OS
Interestingly, SLCO1B1 was considered to be the only gene that reliably demonstrates an effect on MTX pharmacokinetics in a recent systematic review.Citation25 Notably, rs4149081 and rs11045879 in SLCO1B1 have been strongly associated for the first time with MTX clearance.Citation26,Citation27 The rs11045879 variant was found in this patient, which may partially account for the delayed excretion. However, one study showed variants in SLCO1B1 explained up to 10% of the interpatient variability in the clearance of HDMTX.Citation26 Hence, other MTX transporters could be of interest. Among them, the most studied was SLC19A1. Overall, SLC19A1 is an important transporter responsible for folate homeostasis and the uptake of endogenous reduced folates and anti-folate xenobiotics including MTX.Citation28 In Chinese children with acute lymphoblastic leukaemia, delayed elimination of MTX was more frequent in rs1051296 mutant carriers than in wild-type patients.Citation29 This girl carried a heterozygous variant of SLC19A1, increasing the risk of delayed elimination. On the other hand, pumping out MTX from the cell was mediated by highly polymorphic ABC (specifically the ABCB1, ABCC2, ABCC4 and ABCG2) transporters.Citation30 Polymorphisms in these genes have been studied in early studies, however, the results are inconsistent.Citation7,Citation21 This girl has two heterozygous mutations in rs1045642 and rs2032582 in ABCB1, which might lead to a decrease in MTX clearance.Citation8
In addition, the girl carried a T variant of rs1801133 in MTHFR. MTHFR is responsible for the conversion of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate. It has been confirmed that reduced MTHFR expression is related to MTX-induced toxicity in patients with leukaemia.Citation31 Furthermore, both SNPs of MTHFR C677T (rs1801133) and MTHFR A1298C (rs1801131) have been suggested to be accompanied by decreased enzyme activity.Citation32 Some studies found that the T allele in rs1801133 was associated with decreased elimination of MTX, while few studies found a clinically significant association between MTX elimination and rs1801131.Citation33,Citation34 Therefore, we hypothesized that carrying with the T allele may aggravate the plasma MTX level and increase the risk of adverse effects in this case.
Based on the genotype results of this patient and previous literatures,Citation35 we speculate that genetic polymorphisms in the transporters and folate pathways at least partially account for delayed MTX elimination. We consider that implementation of genotyping before HDMTX chemotherapy may help predict MTX treatment response. However, it is worth noting that the pharmacogenetics of MTX are still at the bench level. There is a lack of a definite quantified association between each genetic polymorphism and the efficacy or adverse effects of HDMTX. Therefore, only one pharmacogenetic variant alone may not have sufficient predictive power. A panel consisting of multiple genes should be considered in the clinic.
Here, we describe a valuable case of delayed MTX elimination, possibly attributed to genetic mutations in transporters (SLCO1B1, SLC19A1 and ABCB1) and the folate pathway (MTHFR). The potential risk of delayed MTX elimination is worthy of clinical attention, and the implementation of genotyping should be considered to ensure therapeutic safety.
Abbreviations
HDMTX, high-dose methotrexate; MTX, methotrexate; SNPs, single nucleotide polymorphisms; SLCO1B1, solute carrier organic anion transporter family member 1B1; SLC19A1, solute carrier family 19 member 1; ABCB1, ATP binding cassette subfamily B member 1; MTHFR, methylenetetrahydrofolate reductase; OS, osteosarcoma; CVVHDF, continuous veno-venous haemodiafiltration; D5W, dextrose 5% water solution; AKI, acute kidney injury; ALT, alanine aminotransferase; AST, aspartate aminotransferase; PICU, pediatric intensive care unit; PCT, proealcitonin; PCR, polymerase chain reaction; ABCC2, ATP binding cassette subfamily C member 2; MTR, 5-methyltetrahydrofolate-homocysteine methyltransferase; MTRR, 5-methyltetrahydrofolate-homocysteine methyltransferase reductase; DHFR, dihydrofolate reductase; ABCG2, ATP binding cassette subfamily G member 2; ABCC3, ATP binding cassette subfamily C member 3; PK, pharmacokinetics; RFC1, reduced folate carrier protein 1; GSTP1, glutathione S-transferase pi 1; ABC, ATP binding cassette family; ABCC4, ATP binding cassette subfamily C member 4.
Patient Consent Statement
Written informed consent was obtained from the patient’s mother for the publication of this case report. The study was approved by the Ethics Committee of Children’s Hospital of Nanjing Medical University (202203007-1).
Disclosure
Yue-Tao Zhao is a visiting graduate student from China Pharmaceutical University. The authors declare no other conflicts of interest in this work.
Acknowledgments
This research was supported by the Nanjing Medical Science and Technique Development Foundation (QRX 17074) and the Specially Appointed Medical Expert Project of the Jiangsu Commission of Health (2019). This study was also supported by the Scientific Research Support Foundation for Young Scholars at the Children’s Hospital of Nanjing Medical University (2020).
References
- Belayneh R, Fourman MS, Bhogal S, et al. Update on osteosarcoma. Curr Oncol Rep. 2021;23(6):71. doi:10.1007/s11912-021-01053-7
- Isakoff MS, Bielack SS, Meltzer P, et al. Osteosarcoma, current treatment and a collaborative pathway to success. J Clin Oncol. 2015;33(27):3029–3035. doi:10.1200/JCO.2014.59.4895
- Abe K, MAEDA-MINAMI A, Ishizu T, et al. Risk factors for hepatic toxicity of high-dose methotrexate in patients with osteosarcoma. Anticancer Res. 2022;42(2):1043–1050. doi:10.21873/anticanres.15565
- Brown P, Inaba H, Annesley C, et al. Pediatric acute lymphoblastic leukemia, version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2020;18(1):81–112.
- Widemann BC, Balis FM, Kempf-Bielack B, et al. High-dose methotrexate-induced nephrotoxicity in patients with osteosarcoma. Cancer. 2004;100(10):2222–2232. doi:10.1002/cncr.20255
- Lee KM, Lee HW, Kim SY, et al. Two pediatric osteosarcoma cases with delayed methotrexate excretion, its clinical course and management. Cancer Res Treat. 2011;43(1):67–70. doi:10.4143/crt.2011.43.1.67
- Lui G, Treluyer J-M, Fresneau B, et al. A pharmacokinetic and pharmacogenetic analysis of osteosarcoma patients treated with high-dose methotrexate, data from the OS2006/Sarcoma-09 Trial. J Clin Pharmacol. 2018;58(12):1541–1549. doi:10.1002/jcph.1252
- Esmaili MA, Kazemi A, Faranoush M, et al. Polymorphisms within methotrexate pathway genes, relationship between plasma methotrexate levels, toxicity experienced and outcome in pediatric acute lymphoblastic leukemia. Iran J Basic Med Sci. 2020;23(6):800–809. doi:10.22038/ijbms.2020.41754.9858
- Buchen S, Ngampolo D, Melton RG, et al. Carboxypeptidase G2 rescue in patients with methotrexate intoxication and renal failure. Br J Cancer. 2005;92(3):480–487. doi:10.1038/sj.bjc.6602337
- Misaka KO, Suga Y, Staub Y, et al. Risk factors for delayed elimination of methotrexate in children, adolescents and young adults with osteosarcoma. In Vivo. 2020;34(6):3459–3465. doi:10.21873/invivo.12185
- Frikha R, Elloumi M, Rebai T, et al. MTHFR 677T-1298C haplotype in acute lymphoblastic leukemia, impact on methotrexate therapy. J Oncol Pharm Pract;2021. 10781552211017193. doi:10.1177/10781552211017193
- Yazicioglu B, Kaya Z, Güntekin Ergün S, et al. Influence of folate-related gene polymorphisms on high-dose methotrexate-related Toxicity and prognosis in Turkish children with acute lymphoblastic leukemia. Turk J Haematol. 2017;34(2):143–150. doi:10.4274/tjh.2016.0007
- Yang L, Wu H, Gelder TV, et al. SLCO1B1 rs4149056 genetic polymorphism predicting methotrexate toxicity in Chinese patients with non-Hodgkin lymphoma. Pharmacogenomics. 2017;18(17):1557–1562. doi:10.2217/pgs-2017-0110
- Han J, Liu L, Meng L, et al. Effect of Polymorphisms of ABCB1 and MTHFR on methotrexate-related toxicities in adults with hematological malignancies. Front Oncol. 2021;11:759805. doi:10.3389/fonc.2021.759805
- Hegyi M, Arany A, Semsei AF, et al. Pharmacogenetic analysis of high-dose methotrexate treatment in children with osteosarcoma. Oncotarget. 2017;8(6):9388–9398. doi:10.18632/oncotarget.11543
- Goricar K, Kovač V, Jazbec J, et al. Influence of the folate pathway and transporter polymorphisms on methotrexate treatment outcome in osteosarcoma. Pharmacogenet Genomics. 2014;24(10):514–521. doi:10.1097/FPC.0000000000000083
- Lambrecht L, Sleurs C, Labarque V, et al. The role of the MTHFR C677T polymorphism in methotrexate-induced toxicity in pediatric osteosarcoma patients. Pharmacogenomics. 2017;18(8):787–795. doi:10.2217/pgs-2017-0013
- Hattinger CM, Biason P, Iacoboni E, et al. Candidate germline polymorphisms of genes belonging to the pathways of four drugs used in osteosarcoma standard chemotherapy associated with risk, survival and toxicity in non-metastatic high-grade osteosarcoma. Oncotarget. 2016;7(38):61970–61987. doi:10.18632/oncotarget.11486
- Jabeen S, Holmboe L, Alnæs GIG, et al. Impact of genetic variants of RFC1, DHFR and MTHFR in osteosarcoma patients treated with high-dose methotrexate. Pharmacogenomics J. 2015;15(5):385–390. doi:10.1038/tpj.2015.11
- Hagleitner MM, Coenen MJH, Aplenc R, et al. The role of the MTHFR 677C>T polymorphism in methotrexate-induced liver toxicity: a meta-analysis in patients with cancer. Pharmacogenomics J. 2014;14(2):115–119. doi:10.1038/tpj.2013.19
- Windsor RE, Strauss SJ, Kallis C, et al. Germline genetic polymorphisms may influence chemotherapy response and disease outcome in osteosarcoma, a pilot study. Cancer. 2012;118(7):1856–1867. doi:10.1002/cncr.26472
- Patino-Garcia A, Zalacaín M, Marrodán L, et al. Methotrexate in pediatric osteosarcoma, response and toxicity in relation to genetic polymorphisms and dihydrofolate reductase and reduced folate carrier 1 expression. J Pediatr. 2009;154(5):688–693. doi:10.1016/j.jpeds.2008.11.030
- Muller J, Kralovánszky J, Adleff V, et al. Toxic encephalopathy and delayed MTX clearance after high-dose methotrexate therapy in a child homozygous for the MTHFR C677T polymorphism. Anticancer Res. 2008;28(5B):3051–3054.
- Caronia D, Patiño-Garcia A, Peréz-Martínez A, et al. Effect of ABCB1 and ABCC3 polymorphisms on osteosarcoma survival after chemotherapy, a pharmacogenetic study. PLoS One. 2011;6(10):e26091. doi:10.1371/journal.pone.0026091
- Taylor ZL, Vang J, Lopez-Lopez E, et al. Systematic review of pharmacogenetic factors that influence high-dose methotrexate pharmacokinetics in pediatric malignancies. Cancers (Basel). 2021;13(11):2837. doi:10.3390/cancers13112837
- Trevino LR, Shimasaki N, Yang W, et al. Germline genetic variation in an organic anion transporter polypeptide associated with methotrexate pharmacokinetics and clinical effects. J Clin Oncol. 2009;27(35):5972–5978. doi:10.1200/JCO.2008.20.4156
- Ramsey LB, Panetta JC, Smith C, et al. Genome-wide study of methotrexate clearance replicates SLCO1B1. Blood. 2013;121(6):898–904. doi:10.1182/blood-2012-08-452839
- Uhlen M, Fagerberg L, Hallström BM, et al. Proteomics. Tissue-based map of the human proteome. Science. 2015;347(6220):1260419. doi:10.1126/science.1260419
- Wang SM, Sun LL, Zeng WX, et al. Effects of a microRNA binding site polymorphism in SLC19A1 on methotrexate concentrations in Chinese children with acute lymphoblastic leukemia. Med Oncol. 2014;31(7):62. doi:10.1007/s12032-014-0062-0
- Mikkelsen TS, Thorn CF, Yang JJ, et al. PharmGKB summary, methotrexate pathway. Pharmacogenet Genomics. 2011;21(10):679–686. doi:10.1097/FPC.0b013e328343dd93
- Chae H, Kim M, Choi SH, et al. Influence of plasma methotrexate level and MTHFR genotype in Korean paediatric patients with acute lymphoblastic leukaemia. J Chemother. 2020;32(5):251–259. doi:10.1080/1120009X.2020.1764280
- Chiusolo P, Giammarco S, Bellesi S, et al. The role of MTHFR and RFC1 polymorphisms on toxicity and outcome of adult patients with hematological malignancies treated with high-dose methotrexate followed by leucovorin rescue. Cancer Chemother Pharmacol. 2012;69(3):691–696. doi:10.1007/s00280-011-1751-4
- Mahmoud LB, Mdhaffar M, Frikha R, et al. Use of MTHFR C677T polymorphism and plasma pharmacokinetics to predict methotrexate toxicity in patients with acute lymphoblastic leukemia. Adv Clin Exp Med. 2018;27(8):1061–1068. doi:10.17219/acem/69802
- Choi YJ, Park H, Lee JS, et al. Methotrexate elimination and toxicity: MTHFR 677C>T polymorphism in patients with primary CNS lymphoma treated with high-dose methotrexate. Hematol Oncol. 2017;35(4):504–509. doi:10.1002/hon.2363
- Hu YH, Zhou L, Wang SS, et al. Methotrexate disposition in pediatric patients with acute lymphoblastic leukemia, what have we learnt from the genetic variants of drug transporters. Curr Pharm Des. 2019;25(6):627–634. doi:10.2174/1381612825666190329141003