
Abstract
Background
Pharmacogenomics research is currently revolutionizing treatment optimization by discovering molecular markers. Medicines are the cornerstone of treatment for both acute and chronic diseases. Pharmacogenomics associated treatment response varies from 20% to 95%, resulting in from lack of efficacy to serious toxicity. Pharmacogenomics has emerged as a useful tool for therapy optimization and plays a bigger role in clinical care going forward. However, in Africa, in particular in Ethiopia, such studies are scanty and not generalizing. Therefore, the objective of this review was to outline such studies, generating comprehensive evidence and identify studied variants’ association with treatment responses in Ethiopian patients.
Methods
The Joanna Briggs Institute’s updated 2020 methodological guidelines for conducting and guidance for scoping reviews were used. We meticulously adhered to the systemic review reporting items checklist and scoping review meta-analyses extension.
Results
Two hundred twenty-nine possibly relevant studies were searched. These include: 64, 54, 21, 48 and 42 from PubMed, Scopus, Google Scholar, EMBASE, and manual search, respectively. Seventy-seven duplicate studies were removed. Thirty-nine papers were rejected with justification, whereas 58 studies were qualified for full-text screening. Finally 19 studies were examined. The primary pharmacogene that was found to have a significant influence on the pharmacokinetics of efavirenz was CYP2B6. Drug-induced liver injury has frequently identified toxicity among studied medications.
Conclusion and Future Perspectives
Pharmacogenomics studies in Ethiopian populations are less abundant. The studies conducted focused on infectious diseases, specifically on HAART commonly efavirenz and backbone first-line anti-tuberculosis drugs. There is a high need for further pharmacogenomics research to verify the discrepancies among the studies and for guiding precision medicine. Systematic review and meta-analysis are also recommended for pooled effects of different parameters in pharmacogenomics studies.
Background
Scientific evidence identified inter-individual variabilities in treatment response due to genetics. Recently, there has been a global upsurge in the application of precision medicine in a variety of medical sectors.Citation1–3 Pharmacogenomics research currently holds the promise of revolutionizing in identifying molecular markers associated with treatment response and optimize therapy.Citation4,Citation5 Medicines are the cornerstone of treatment for both acute and chronic diseases. However, patients’ response to medication treatment varies because of their genetic make-up greatly ranging from 20% to 95% experiencing from lack of efficacy to adverse drug reactions (ADRs) or serious toxicity.Citation4,Citation6,Citation7 Given that genetic variants (polymorphisms) account for this variability. Pharmacogenomics has emerged as a useful tool for therapy optimization and is expected to play a bigger role in clinical care going forward.Citation2,Citation6 Precision medicine refers to a therapeutic strategy that considers a patient’s genetics, behavior, surroundings, and way of life.Citation2 Pharmacogenomics offer opportunities to researchers and physicians from the most molecular to the most clinical. Knowledge in computational biology, physiology, endocrinology, molecular biology, human genetics, bioinformatics, genomics, epidemiology, statistics, pharmacology, toxicology, and internal medicine are all relevant to the study of pharmacogenetics and pharmacogenomics.Citation8 Consequently, pharmacogenomics knowledge of a drug’s molecular effects is useful for both drug development and customized therapy.Citation9 Although pharmacogenetics and pharmacogenomics are different, nowadays, they are used interchangeably for the sake of simplicity.Citation2,Citation10
A Synopsis of Pharmacogenetics and Pharmacogenomics’ Distinctions
It was suggested that pharmacogenetics is back about 510 B.C when Pythagoras was in southern Italy, in Croton, the first to identify some of the dangers, but not other. Individuals who eat the fava beans, hemolytic anemia was an adverse effect in individuals with insufficient glucose-6-phosphate dehydrogenase. Some contend that the field of current pharmacogenetics began with Snyder’s 1932 study on the “phenylthiourea nontaster” phenotype, which is inherited as an autosomal recessive trait. Others still related to its origin a few decades back because of the human genome project.Citation9 Drug response is a trait that can range from potentially fatal ADRs to an equally severe ineffectiveness of treatment. The enquiry of pharmacogenetics and pharmacogenomics delves into the impact of genetics on individual variations in medicine’s response. The fast progress in both genomics and molecular pharmacology led to the evolution of this specialty. Pharmacogenetics research was first primarily concerned with monogenic features, which frequently involved genetic variation in metabolic drug states. Additionally, pharmacogenomics is integrated into the drug regulation and drug development process and moves beyond the “translational interface” into health sectors more significantly.Citation11
Although the concept of pharmacogenetics was founded in 1950’s by Arno Motulsky and his colleagues,Citation12,Citation13 the term was coined for the first time in 1959 by Friedrich Vogel.Citation2,Citation14 The study of pharmacogenomics focuses on how a person’s genetic makeup influences how their body responds to medications. The phrase refers to the area where genetics and pharmacology converge, and it originated from molecular pharmacology and genomics.Citation11,Citation15 Pharmacogenomics offers hope that medications may eventually be customized to each person’s unique genetic makeup.Citation15
Pharmacogenomics is the enquiry of differences in Deoxyribonucleic acid (DNA) and ribonucleic acid properties in relation to medicines’ response, whereas the impact of differences in DNA sequence on medication response is known as pharmacogenetics. Within the field of precision medicine, pharmacogenomics examines how genetic differences impact how medicines are processed and respond. More precisely, pharmacogenetics uses genetic, epigenetic, and nutrigenetic methods to examine the effects of changes in one or a few genes on medication responsiveness.Citation2,Citation16
Applying pharmacogenetics to the full genome, pharmacogenomics studies the relationships between individual genes and medications. Pharmacogenetics studies the effects of genetic variations on pharmacological action, dose, and use in individuals. Pharmacogenetics investigation can determine which patient is responsive before medication is administered, which is the foundation of precision medicine. Genetic variations affecting drug transporter proteins and liver enzymes (the cytochrome P450 group) are of particular interest in the field of pharmacogenetics. Similarly, genetic variations affecting drug pharmacodynamic profiles, such as variations in receptor protein expressions, are of particular interest. Pharmacogenomics, on the other hand, is associated with the entire genome rather than just a single gene’s SNP. It is the study of all the genes in an organism, both expressed and non-expressed, in every physiological state.Citation17
Pharmacogenomics, beyond academic research contexts, is becoming more widely accepted as a tool for being informed by objective evidence medicine management. Pharmacogenomics tests are used to predict the efficacy and possible negative effects of pharmacological prescriptions. However, research in pharmacogenomics in African continent is not keeping up with global norms. Researchers throughout Africa must have access to infrastructural assistance and information sharing in order to integrate pharmacogenomics into clinical practice. The application of pharmacogenomics necessitates digital storage and quick, safe access to information for authorized users. Pharmacogenomics data is frequently integrated with electronic healthcare record systems,Citation2 which are very poor in Africa, particularly in Ethiopia. Due to genetic, environmental, and illness heterogeneity, different people respond differently to medicines. Genetic variations can alter a drug’s pharmacokinetics and pharmacodynamics, which in turn can alter the drug’s response by influencing the drug target’s function as well as local and systemic drug exposure. Many pharmacogenomics indicators that have been shown to improve therapeutic outcomes.Citation18
Many of the inter-individual differences in therapeutic efficacy and adverse effect risk are due to variations in the genes encoding proteins implicated in immunological or pharmacological responses to medications. The number of genetic variants important for medication action is substantially more than previously believed, and given the tremendous advancements in genetic analysis technology, a true personalized drug response prediction necessitates consideration of millions of rare mutations.Citation19
As more people undertake acute or long-term therapeutic interventions, ADRs are emerging as a significant global health concern. In affluent nations, ADRs rank in the top ten causes of illness and death. Pharmacogenomics is accountable in 20–95% of variability in medication response and plays a major part in the frequency and severity of ADRs.Citation7 Pharmacogenomics profiles have been established for around 50% of currently available medications. These profiles can be used for preemptive genotyping and provide clinical benefits for patients, such as increased efficacy and less ADRs.Citation6
Research on pharmacogenomics in Africa over the previous 20 years has produced a wealth of information regarding variant alleles that affect plasma exposure variability in patients and the effectiveness of treatment outcomes from drugs used to treat malaria, TB, and HIV.Citation1,Citation20 Widespread pharmacogenetics research in several African nations will greatly improve patient care and maximize treatment success of HIV, TB, and malaria on the continent.Citation7,Citation20 Similarly in Ethiopia, even though a few research were conducted on TB and HIV in the capital Addis Ababa, Pharmacogenomics data utilization and knowledge are at its infant stage.Citation7,Citation21
To the greatest of reviewers’ knowledge, there is no thorough investigation conducted in Ethiopia either by scoping or systematic reviews to investigate the pharmacogenetics and pharmacogenomics associated impacts. Scoping review is a useful method for outlining the body of existing literature and identifying topics that may require more researches.Citation22 Therefore, the objective of this review was to outline main study areas, to generate comprehensive evidence and identify studied variants’ association with treatment responses in Ethiopian patients.
Methods
The Joanna Briggs Institute’s updated 2020 methodological guidelines for conducting scoping and guidance for scoping reviews were used in this review.Citation23–25 The draft protocol was developed by the principal author and reviewed by the second co-author, and as a result, few amendments were made. We meticulously adhered to the systemic review reporting items checklist and scoping review meta-analyses extension.Citation25
The Scoping Review Question
To ascertain whether our main research questions were eligible, we employed the Population, Concept, and Context (PCC) framework created by the Joanna Briggs Institute. The following were the primary research questions addressed: What are the relevant genomic markers from pharmacogenomics and pharmacogenetics studies that can help Ethiopian patients receive precision medicine, and what are the clinical consequences of these findings? Furthermore, what research in the fields of pharmacogenomics and pharmacogenetics is lacking?
Eligibility Criteria
The following criteria were used to determine which studies to be included: research with patients; any type of study, including original, review, and grey literature articles; and only studies published in English. No limitations on publication years or ages. Studies lacking pharmacogenes, medications, and markers were excluded.
Data Sources and Searching Strategies
PubMed, MEDLINE through PubMed, Scopus, EMBASE, and Google Scholar were systematically searched without language, publication status or date restrictions. Manual search, as a supplemental approach, was also employed to identify additional primary studies. Searching medical subject heading terms used were: “Pharmacogenetic”, OR “pharmacogenomics”, OR “human”, OR “humans”, OR “patients”, OR “gene”, OR “-genetics”, “pharmacokinetics”, OR “genomics”, OR “pharmacodynamics”, OR “GWAS”, OR “-kinetics”, OR “-dynamics”, OR “precision medicine”, OR “mutations”, OR “Ethiopia” OR/AND “Ethiopian” and “population”.
Study Selection and Reliability
Two expert reviewers who have conducted systematic reviews carried out our initial searches. These reviewers individually screened the titles, abstracts, and entire texts. A disagreement between the two reviewers about whether or not to include certain articles was settled by consensus. A second reviewer was blinded to the first reviewer’s selections while choosing papers and gathering data.
Data Charting (Extraction)
The lead author extracted the data, and the second reviewer confirmed it. A consensus was achieved regarding the outcomes. After deliberation, the third reviewer decided how to handle disagreements. From every study, we took out the following information: initial author name, year of publication, age in year, study type, patient category, research region, primary genes or chromosomes found, alleles, variants, and single nucleotide polymorphisms (SNPs). The clinical consequences of the key findings and related medications are summurized in table.
Table 1 Summary of Extracted Data and the Main Outcomes
Predicated on the scoping review methodology framework,Citation24,Citation25 we included a narrative, graphs, and a tabulation of our findings. First, the breadth and distribution of the research included in the review were analyzed numerically in a basic manner. Next, thematic content analysis was used to present the research findings from the literature. The themes that arose from the study’s conclusions or findings then guided the organization of our narrative content.
Result
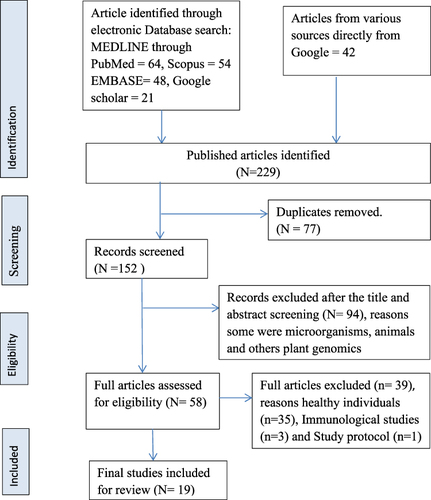
Two hundred twenty-nine candidate studies were found from the first search, including 64 from PubMed, 54 from Scopus, 21 from Google Scholar (advanced searching), 48 from EMBASE, and 42 articles that were found manually. There were 152 studies after removal of duplicate studies. A total of fifty-eight studies qualified for full-text screening. On further screening 39 studies excluded because of reasons described in PRISMA-ScR study flow chart see . No scoping review, meta-analysis and grey literature were found in the area. Although 5 conference reports were identified, there was no single report that fulfils the criteria. Finally, 19 full articles were reviewed.Citation26–44
Figure 1 Flow diagram for study selection.
Characteristics of Included Studies
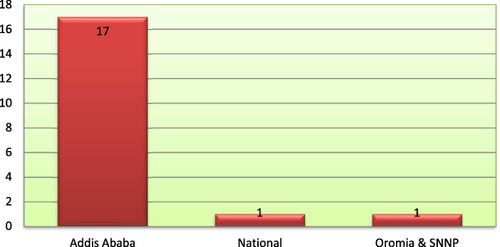
Most studies, 89.47%, were conducted in Addis Ababa, and almost all are prospective cohort studies in their types. The main findings, their clinical implications and pertinent extracted data were tabulated in .
Figure 2 Distributions of research undertaken in Ethiopia on pharmacogenomics by study area.
After filtering, the only research that remained was the pharmacogenetics and pharmacogenomics studies done on Ethiopian inhabitants and diaspora. depicts pharmacogenetics, and pharmacogenomics conducted on Ethiopian patients.
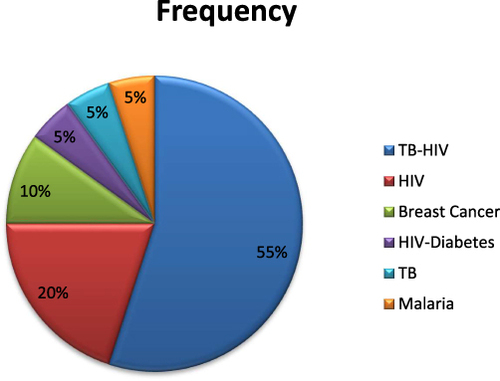
On our systematic research, we found that about 58 studies on human population more than half of them were conducted on healthy individuals. Most of the research is done on infectious disease in particular of tuberculosis co infected with human immune virus. We found two studies on breast cancer and only a single study on malaria as shown in .
Figure 3 Frequency distribution of diseases category.
Discussion
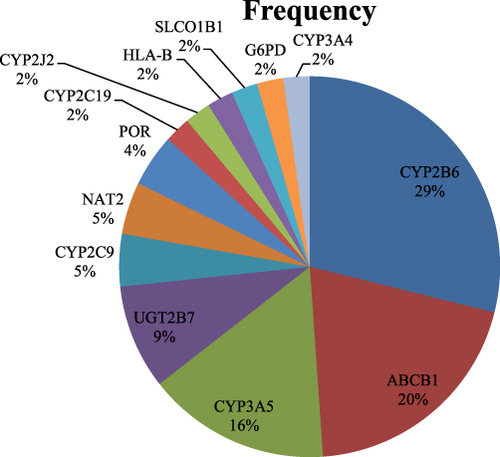
Currently, pharmacogenomics, the foundation for precision medicine, is the major area of research to manage and treat patients better. In certain industrialized nations, they have become the cornerstones of healthcare. Nonetheless, pharmacogenomics research and clinical application is still in their infancy in Africa, specifically in Ethiopia. Therefore, to provide thorough evidence, we have gathered pertinent Ethiopian pharmacogenetic and pharmacogenomics studies for this review. We found that the largest percentage of cytochrome P450 isozymes, together with three-quarters of all the genes examined, were included in our review. Among which, CYP2B6 is the primary gene responsible for 29% of the metabolism of efavirenz, a popular antiretroviral non-nucleoside transcriptase inhibitor. In , the primary pharmacogenes found in the Ethiopian patients under study are displayed. This review also identified many pharmacogenes or drug-metabolizing enzymes, along with their alleles and variants, in accordance with identifications from quality control and global research. These summarized data validate existing markers and augment pharmacogenomics that holds the promise of revolutionizing clinical research and enhancing healthcare in sub-Saharan Africa. In addition, the importance of the variety of the African genome is emphasized, as are the prospects for pharmacogenomics research, which will make it possible to identify new genetic pathways.Citation45
Figure 4 The major genes identified among Ethiopian patients.
The genes found out in Ethiopian patients are in line with 28 genes identified by quality control studies (CYP3A4, CYP2B6, CYP2C9, CYP2C8, CYP3A5, CYP2D6, CYP2C19, CYP2E1, CYP4F2, GSTM1, NAT1, SLC22A2, NAT2, SLC15A2, SLCO1B1, SLCO2B1, UGT2B7, UGT1A1, UGT2B15, and UGT2B17) by consensus confirmation, verified the existence of 108 or more variant pharmacogenetic alleles.Citation46
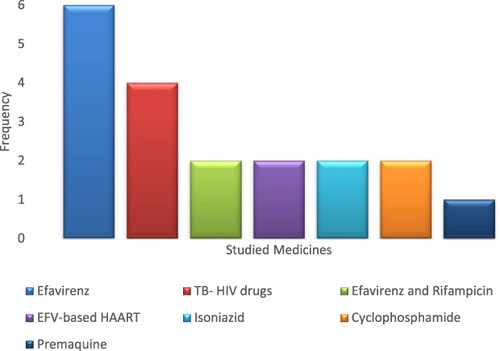
The medications that are most frequently studied are isoniazid, efavirenz, rifampicin, and other very effective anti-retroviral medications combined with an anti-tuberculosis regimen. High variability between patients was discovered in terms of pharmacogene expression, pharmacokinetic characteristics, and adverse drug events. Drugs that were used to treat tuberculosis combined with antiretrovirals caused a serious medicine-induced liver injury (DILI). Hematologic toxicity, neurotoxicity, and a little deficit of glucose-6-phosphoglucose dehydrogenase, which may result in hemolytic anemia, were the other toxicities that were reported. presents the medications under investigation that have been linked to the aforementioned toxicities.
Figure 5 Studied drugs distributions in association with identified genes.
Our genetic diversity exceeds that of many larger geographic locations on a worldwide scale, as we Ethiopians continuously demonstrate with our substantial degree of cultural and linguistic diversity.Citation47 Therefore, owning to 20–95% pharmacogenomics variabilityCitation4 in drug response and toxicity especial consideration should be given as far as severity of ADRs and efficacy are concerned. Among Ethiopians, a wide range of DILI which is 11.6%–30% found out similar patients might be associated with this genetic variability.Citation27,Citation28,Citation34,Citation47 Higher incidence of cyclophosphamide toxicity hematologic grade 3 or 4 (51%) largely appeared as neurotoxicity (50.2%) also needs due clinicians’ attention for breast cancer Ethiopian patients. We discovered that research on pediatric patients from Ethiopia is extremely lacking. In order to prevent ADRs, special consideration should be given to special population like women, elderly patients, and children due to their distinct physiological and pathological conditions complemented with pharmacogenomics features may impacts differently than any other population. Additionally, due to the pharmacogenomics differences among African continent populations, particularly Ethiopians, when extrapolating findings from clinical trials conducted in Caucasians to other populations, caution should be taken.
According to two investigations in Ethiopian health professionals to assess their knowledge and attitude, huge gap was found, although professionals have good attitude toward pharmacogenomics.Citation7,Citation21 The current review also come up with very few research that was done in Ethiopia and no practical startup of pharmacogenomics was here in Ethiopia. Ethiopian data/studies on elite athlete genetics, high altitude adaptation, milk consumption, tuberculosis, and drug metabolizing enzymes for the discovery of novel genes and greatest asset for the world have been incorporated. This is because Ethiopians have the highest genetic variability, which makes it easier to identify novel variants.Citation48
The main allele that was found in most of Ethiopian study participants was CYP2B6*6 and associated with low EFV concentration,Citation26,Citation37 whereas patients who express CYP2B1*1 alleles was found to have insignificant pharmacokinetics impact and inconsistency.Citation32 CYP2D6, CYP2C9, CYP2C19, and CYP3A4/5 are the most significant CYPs involved in the metabolism of common medications. Although, there are variations in age, sex, circadian rhythm, and ethnicity, these four CYP genes encode the enzymes that are in charge of 60–80% of the medications that are currently prescribed.Citation49 The current review finding is in line with such scientific known facts except CYP2D6. We also found many discrepancies among the study results in Ethiopia.Citation39,Citation40,Citation50 The effect of CYP2B6 on EFV pharmacokinetic parameters, its major metabolites, the effect of CYP2J2 on cyclophosphamide,Citation39 and different percent findings of DILI are among the most common.Citation27,Citation28,Citation34
Patients with HLA-B57:03 and HLA-B57:02 variant alleles are more likely to experience cholestatic liver injury and mild DILI, respectively, as a result of anti-TB and ARV medication-induced liver injury which is similar to a study done by Qihui Shao et al.Citation51 HLA molecules or HLA antigens are encoded by the human major histocompatibility complex (MHC), commonly referred to as the HLA gene complex. It is separated into three subgroups: Class I, Class II, and Class III, and is found on chromosome 6, which has more than 200 genes. CD8+ T cells are able to identify class I MHC molecules, which are made up of the HLA-A, HLA-B, and HLA-C genes. CD4+ T cells detect class II MHC molecules, which include HLA-DRA, HLA-DRB1, HLA-DPB1, HLA-DQB1, and HLA-DPA1. Complement components, tumor necrosis factor (TNF), heat shock protein 70 (HSP70), and the 21 hydroxylase gene (CYP21A and CYP21B) are mostly encoded by class III MHC.Citation51
Despite the great genetic diversity of Ethiopian populations, there is currently a dearth of genetic data on them. Pharmacogenomics research has the potential to completely change how diseases are treated, and thus Ethiopian communities stand to gain from its ability to pinpoint prospective responders, minimize medicines’ side effects, and optimize medication dosage.Citation52 Inadequate training and education of pharmacogenomics for healthcare providers; non-specific biomarkers of medicines efficacy and toxicity; cost-effectiveness; administrative issues in health organizations; and a lack of regulation for the widespread use of pharmacogenomics in clinical settings are the main obstacles that Ethiopians face in attempting to prevent ADRs through the routine use of pharmacogenomics procedures.Citation7 Providing individualized therapies is essential in preventing ADRs and optimizing efficacy because of different ethnic communities within the same country.
Conclusion and Future Perspective
There are few investigations on pharmacogenomics in Ethiopian populations. Studies on infectious diseases were conducted commonly on efavirenz and the first-line anti-tuberculosis medications. The primary discovery of pharmacogene that affects the pharmacokinetics of efavirenz is CYP2B6. Drug-induced liver damage was frequently discovered to be harmful in relation to medicines and genes that were studied. Given Ethiopians’ considerable genetic variability, careful consideration must be given to assessing the efficacy and potential side effects of medications that dictate the importance of precision medicine implementation. Additional pharmacogenomics research will be crucial to confirm the differences between the studies. The pooled impacts of several pharmacogenomics study parameters were also suggested by systematic review and meta-analysis.
Ethical Approval
Ethical approval is not needed for this investigation.
Author Contributions
The corresponding author conceptualized the study and the idea from the inception. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation. Then, all authors critically reviewed the article; gave final approval for the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no conflicts of interest to disclose for this work.
Acknowledgment
The authors are thankful for those who conducted pharmacogenetics and pharmacogenomic studies in Ethiopian population and study participants of each reviewed articles.
Additional information
Funding
References
- Radouani F, Zass L, Hamdi Y, et al. A review of clinical pharmacogenetics Studies in African populations. Per Med. 2020;17(2):155–170. doi:10.2217/pme-2019-0110
- Davis BH, Limdi NA. Translational pharmacogenomics: discovery, evidence synthesis and delivery of race-conscious medicine. Clin Pharmacol Ther. 2021;110(4):909–925. doi:10.1002/cpt.2357
- Khan A, Abbas M, Verma S, et al. Genetic variants and drug efficacy in tuberculosis: A step toward personalized therapy. Glob Med Genet. 2022;9(2):90–96. doi:10.1055/s-0042-1743567
- Ross CJ, Carleton B, Warn DG, Stenton SB, Rassekh SR, Hayden MR. Genotypic approaches to therapy in children: a national active surveillance network (GATC) to study the pharmacogenomics of severe adverse drug reactions in children. Ann N Y Acad Sci. 2007;1110(1):177–192. doi:10.1196/annals.1423.020
- RCoP, and Society BP. Personalised prescribing using pharmacogenomics to improve patient outcomes; 2022.
- Cacabelos R, Naidoo V, Corzo L, Cacabelos N, Carril JC. Genophenotypic factors and pharmacogenomics in adverse drug reactions. Int J Mol Sci. 2021;22(24):13302. doi:10.3390/ijms222413302
- Abdela OA, Bhagavathula AS, Gebreyohannes EA, Tegegn HG. Ethiopian health care professionals’ knowledge, attitude, and interests toward pharmacogenomics. Pharmgen Pers Med. 2017;10:279–285. doi:10.2147/PGPM.S145336
- Nebert DW. Pharmacogenetics and pharmacogenomics: why is this relevant to the clinical geneticist? Clin Genet. 1999;56(4):247–258. doi:10.1034/j.1399-0004.1999.560401.x
- Oh M, Park S, Lee S, et al. DRIM: A web-based system for investigating drug response at the molecular level by condition-specific multi-omics data integration. Front Genet. 2020;11:564792. doi:10.3389/fgene.2020.564792
- Daly AK. Pharmacogenetics: a general review on progress to date. Br Med Bull. 2017;124(1):65–79. doi:10.1093/bmb/ldx035
- Weinshilboum RM, Wang L. Pharmacogenetics and pharmacogenomics: development, science, and translation. Annu Rev Genomics Hum Genet. 2006;7(1):223–245. doi:10.1146/annurev.genom.6.080604.162315
- Marshall A. Laying the foundations for personalized medicines. Nature Biotechnol. 1998;16(S2):6–8. doi:10.1038/5138
- Roden DM, McLeod HL, Relling MV, et al. Pharmacogenomics. Lancet. 2019;394(10197):521–532. doi:10.1016/S0140-6736(19)31276-0
- Malsagova KA, Butkova TV, Kopylov AT, et al. Pharmacogenetic testing: a tool for personalized drug therapy optimization. Pharmaceutics. 2020;12(12):1240. doi:10.3390/pharmaceutics12121240
- Aneesh TPSSM, Jose A, Chandran L, Mary Zachariah S, Zachariah SM. Pharmacogenomics: The right drug to the right person. J Clin Med Res. 2009;1(4):191–194. doi:10.4021/jocmr2009.08.1255
- Russo R, Capasso M, Paolucci P, Iolascon A. Pediatric pharmacogenetic and pharmacogenomic studies: the current state and future perspectives. Eur J Clin Pharmacol. 2011;67(Suppl S1):17–27. doi:10.1007/s00228-010-0931-1
- Sindelar RD. Crommelin RDSaBM. In: Daan JA, editor. Pharmaceutical Biotechnology Fundamentals and Applications. Switzerland Springer Nature; 2019:192–237 p.
- Pirmohamed M. Personalized pharmacogenomics: predicting efficacy and adverse drug reactions. Annu Rev Genomics Hum Genet. 2014;15(1):349–370. doi:10.1146/annurev-genom-090413-025419
- Lauschke VM, Milani L, Ingelman-Sundberg M. Pharmacogenomic biomarkers for improved drug therapy-recent progress and future developments. AAPS J. 2017;20(1):4. doi:10.1208/s12248-017-0161-x
- Suarez-Kurtz G, Aklillu E, Saito Y, Somogyi AA. Conference report: pharmacogenomics in special populations at WCP2018. Br J Clin Pharmacol. 2019;85(3):467–475. doi:10.1111/bcp.13828
- Admas T, Banjaw A. Healthcare professionals’ knowledge, attitudes and future expectations towards personalized medicine. Per Med. 2021;18(5):483–490. doi:10.2217/pme-2020-0185
- Yow HY, Hamzah S, Abdul Rahim N, Suppiah V. Pharmacogenomics of response to statin treatment and susceptibility to statin-induced adverse drug reactions in Asians: A scoping review. Asian Biomed (Res Rev News). 2023;17(3):95–114. doi:10.2478/abm-2023-0050
- Gc PM, McInerney P, Munn Z, Tricco A, Khalil H. Guidance for the Conduct of JBI Scoping Reviews. In: Edoardo Aromataris ZM, editor. Joanna Briggs Institute Reviewer’s Manual. The Joanna Briggs Institute; 2017.
- Peters MDJ, Marnie C, Tricco AC, et al. Updated methodological guidance for the conduct of scoping reviews. JBI Evid Synth. 2020;18(10):2119–2126. doi:10.11124/JBIES-20-00167
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
- Habtewold A, Amogne W, Makonnen E, et al. Long-term effect of efavirenz autoinduction on plasma/peripheral blood mononuclear cell drug exposure and CD4 count is influenced by UGT2B7 and CYP2B6 genotypes among HIV patients. J Antimicrob Chemother. 2011;66(10):2350–2361. doi:10.1093/jac/dkr304
- Yimer G, Ueda N, Habtewold A, et al. Pharmacogenetic & pharmacokinetic biomarker for efavirenz based ARV and rifampicin based anti-TB drug induced liver injury in TB-HIV infected patients. PLoS One. 2011;6(12):e27810. doi:10.1371/journal.pone.0027810
- Yimer G, Amogne W, Habtewold A, et al. High plasma efavirenz level and CYP2B6*6 are associated with efavirenz-based HAART-induced liver injury in the treatment of naive HIV patients from Ethiopia: A prospective cohort study. Pharmacogenomics J. 2012;12(6):499–506. doi:10.1038/tpj.2011.34
- Habtewold A, Amogne W, Makonnen E, et al. Pharmacogenetic and pharmacokinetic aspects of CYP3A induction by efavirenz in HIV patients. Pharmacogenomics J. 2013;13(6):484–489. doi:10.1038/tpj.2012.46
- Ibrahim M. Pharmacokinetics of isoniazid in Ethiopian children with tuberculosis in relation to the N-acetyltransferase 2 (NAT2) genotype. Afr J Pharm Pharmacol. 2013;7(18):1124–1130. doi:10.5897/AJPP2012.0040
- Ngaimisi E, Habtewold A, Minzi O, et al. Importance of ethnicity, CYP2B6 and ABCB1 genotype for efavirenz pharmacokinetics and treatment outcomes: a parallel-group prospective cohort study in two sub-Saharan Africa populations. PLoS One. 2013;8(7):e67946. doi:10.1371/journal.pone.0067946
- Abiy Habtewold EM, Amogne W, Yimer G, Aderaye G, Leif BJBEA. Is there a need to increase the dose of efavirenz during concomitant rifampicin-based antituberculosis therapy in sub-Saharan Africa? The HIV-TB pharmagene study. Pharmacogenomics. 2015;16(10):1047–1064
- Habtewold A, Aklillu E, Makonnen E, et al. Long-term effect of rifampicin-based anti-tb regimen coadministration on the pharmacokinetic parameters of Efavirenz and 8-Hydroxy-Efavirenz in Ethiopian patients. J Clin Pharmacol. 2016;56(12):1538–1549. doi:10.1002/jcph.756
- Petros Z, Lee MM, Takahashi A, et al. Genome-wide association and replication study of anti-tuberculosis drugs-induced liver toxicity. BMC Genomics. 2016;17(1):755. doi:10.1186/s12864-016-3078-3
- Petros Z, Lee MT, Takahashi A, et al. Genome-Wide association and replication study of hepatotoxicity induced by antiretrovirals alone or with concomitant anti-tuberculosis drugs. OMICS. 2017;21(4):207–216. doi:10.1089/omi.2017.0019
- Petros Z, Kishikawa J, Makonnen E, Yimer G, Habtewold A, Aklillu E. HLA-B(*)57 allele is associated with concomitant anti-tuberculosis and antiretroviral drugs induced liver toxicity in Ethiopians. Front Pharmacol. 2017;8:90. doi:10.3389/fphar.2017.00090
- Habtewold A, Aklillu E, Makonnen E, et al. Population pharmacokinetic model linking plasma and peripheral blood mononuclear cell concentrations of efavirenz and its metabolite, 8-Hydroxy-Efavirenz, in HIV Patients. Antimicrob Agents Chemother. 2017;61(8). doi:10.1128/AAC.00207-17.
- Lo E, Zhong D, Raya B, et al. Prevalence and distribution of G6PD deficiency: implication for the use of primaquine in malaria treatment in Ethiopia. Malar J. 2019;18(1):340. doi:10.1186/s12936-019-2981-x
- Ahmed JH, Makonnen E, Yimer G, et al. CYP2J2(*)7 Genotype Predicts Risk of Chemotherapy-Induced Hematologic Toxicity and Reduced Relative Dose Intensity in Ethiopian Breast Cancer Patients. Front Pharmacol. 2019;10:481. doi:10.3389/fphar.2019.00481
- Ahmed JH, Makonnen E, Bisaso RK, et al. Population Pharmacokinetic, Pharmacogenetic, and Pharmacodynamic Analysis of Cyclophosphamide in Ethiopian Breast Cancer Patients. Front Pharmacol. 2020;11:406. doi:10.3389/fphar.2020.00406
- Aklillu E, Zumla A, Habtewold A, et al. Early or deferred initiation of efavirenz during rifampicin-based TB therapy has no significant effect on CYP3A induction in TB-HIV infected patients. Br J Pharmacol. 2021;178(16):3294–3308. doi:10.1111/bph.15309
- Mugusi S, Habtewold A, Ngaimisi E, et al. Impact of Population and Pharmacogenetics Variations on Efavirenz Pharmacokinetics and Immunologic Outcomes During Anti-Tuberculosis Co-Therapy: a Parallel Prospective Cohort Study in Two Sub-Sahara African Populations. Front Pharmacol. 2020;11:26. doi:10.3389/fphar.2020.00026
- Chala A, Tadesse BT, Chaka TE, et al. Predictors of Efavirenz Plasma Exposure, Auto-Induction Profile, and Effect of Pharmacogenetic Variations among HIV-Infected Children in Ethiopia: a Prospective Cohort Study. J Pers Med. 2021;11(12):1303. doi:10.3390/jpm11121303
- Tadesse WT, Mlugu EM, Shibeshi W, Degu WA, Engidawork E, Aklillu E. CYP3A and CYP2B6 Genotype Predicts Glucose Metabolism Disorder among HIV Patients on Long-Term Efavirenz-Based ART: a Case-Control Study. J Pers Med. 2022;12(7):1087. doi:10.3390/jpm12071087
- Matimba A, Dhoro M, Dandara C. Is there a role of pharmacogenomics in Africa. Glob Health Epidemiol Genom. 2016;1(e9).
- Zhou Y, Ingelman‐Sundberg M, Lauschke VM. Worldwide distribution of Cytochrome P450 Alleles: A meta-analysis of population-scale sequencing projects. Clin Pharmacol Ther 2017;102(4):688–700. doi:10.1002/cpt.690
- Hellenthal G, Bird N, Morris S. Structure and ancestry patterns of Ethiopians in genome-wide autosomal DNA. Hum Mol Genet. 2021;30(R1):R42–R48. doi:10.1093/hmg/ddab019
- Lopez S, Tarekegn A, Band G, et al. Evidence of the interplay of genetics and culture in Ethiopia. Nat Commun. 2021;12(1):3581. doi:10.1038/s41467-021-23712-w
- Cacabelos R, Cacabelos N, Carril JC. The role of pharmacogenomics in adverse drug reactions. Expert Rev Clin Pharmacol. 2019;12(5):407–442. doi:10.1080/17512433.2019.1597706
- Zhang F, Finkelstein J. Inconsistency in race and ethnic classification in pharmacogenetics studies and its potential clinical implications. Pharmg Pers Med. 2019;12:107–123. doi:10.2147/PGPM.S207449
- Shao Q, Mao X, Zhou Z, Huai C, Li Z. Research progress of pharmacogenomics in drug-induced liver injury. Front Pharmacol. 2021;12:735260. doi:10.3389/fphar.2021.735260
- Pirmohamed M. Pharmacogenomics: current status and future perspectives. Nat Rev Genet. 2023;24(6):350–362. doi:10.1038/s41576-022-00572-8