
Abstract
Recurrent respiratory papillomatosis (RRP) is a condition caused by human papillomavirus (HPV), usually HPV types 6 and 11, which is characterized by recurrent papillomas of the respiratory tract, mainly the larynx. Patients usually present between the ages of 2 and 6 years. The initial presenting symptom is progressive dysphonia, followed by stridor and respiratory distress. Treatment consists of repeated microlaryngoscopic procedures to remove the papillomas as there is no cure. The poor availability and accessibility of appropriate healthcare services in developing countries are barriers to the early diagnosis and appropriate management of patients with juvenile-onset recurrent respiratory papillomatosis (JoRRP), requiring many patients to have a tracheostomy. The introduction of prophylactic vaccines that include HPV6 and HPV11 is necessary in order to reduce the incidence of JoRRP.
Introduction
Recurrent respiratory papillomatosis (RRP) is a condition caused by human papillomavirus (HPV) that is characterized by recurrent papillomas of the respiratory tract, mainly the larynx.Citation1 Two clinical presentations of the disease are recognized – juvenile-onset RRP (JoRRP), where the condition occurs under 12 years of age, and adult-onset RRP (AoRRP). JoRRP predominates in sub-Saharan Africa,Citation2–Citation4 in contrast to Europe and South America, where AoRRP predominates.Citation5,Citation6
Epidemiology
The incidence and prevalence of JoRRP in developing countries has been found to be similar to or slightly higher than that in developed countries ().Citation2,Citation7–Citation16 However these data are probably an underestimate as a result of patients not having symptoms severe enough to present, or dying as a result of upper airway obstruction prior to presentation.
Table 1 Incidence and Prevalence of JORRP
Etiology
There are over 180 HPV types.Citation1 HPV types 6 and 11 are responsible for most cases of JoRRP, although other types, including high risk types have also been identified.Citation3–Citation5,Citation9,Citation17–Citation34 Transmission of HPV is believed to occur during birth from the mother as the fetus passes through an infected genital tract. Although a minority of mothers of children with RRP have a history of previous genital condylomata, most have histologic evidence of HPV infection.Citation35 Children whose mothers have a history of genital warts are at greatly elevated relative risk of developing RRP.Citation36 The triad of a firstborn child born by vaginal delivery to a teenage mother was first described by Kashima and has subsequently been found in a number of other studies.Citation4,Citation21,Citation29,Citation37 Primigravid mothers are more likely to have a long second stage of labor with prolonged exposure to HPV in the birth canal, leading to a higher risk of infection in the first-born child.
Clinical Presentation
Patients generally present between the age of 2 and 6 years, with an approximately equal sex distribution.Citation2,Citation4,Citation7,Citation16,Citation30–Citation33,Citation38–Citation40 Patients with HPV11 disease present at a significantly younger age than those with HPV6 disease.Citation2,Citation20,Citation21,Citation27 The initial presenting symptom is progressive dysphonia, followed by stridor and respiratory distress.Citation4,Citation29,Citation30,Citation38–Citation41 Patients may be aphonic with respiratory distress on presentation. Other symptoms may include chronic cough, recurrent upper respiratory tract infections and hemoptysis.Citation30,Citation32 Patients are often misdiagnosed as having asthma, laryngotracheobronchitis, foreign body aspiration or laryngomalacia.Citation3 In developing countries, as a result of the poor availability of healthcare services in general and ENT services in particular,Citation42–Citation44 patients frequently present with upper airway obstruction and a history of hoarseness for many years.Citation3,Citation4,Citation30,Citation40,Citation41,Citation45–Citation51 In a South African study, all patients diagnosed in the private sector had only hoarseness on initial presentation, while 70.1% of patients diagnosed in the public sector also presented with stridor, with 51.9% being in respiratory distress.Citation40 Pulmonary hypertension and cor pulmonale may rarely occur as a result of chronic upper airway obstruction.Citation46,Citation52
The larynx is the most common site of involvement, with the trachea being the most common site of extralaryngeal involvement. Other extralaryngeal sites that may be involved include the oropharynx, nasopharynx, nose, oral cavity, and lung.Citation3 Between 5 and 48% of children with JoRRP develop distal spread.Citation53,Citation54 Pulmonary involvement occurs in 3.3% of patients with JoRRP. The incidence of lung cancer in patients with pulmonary involvement is 16%, with most patients who develop lung cancer having HPV11 disease.Citation55
Diagnosis
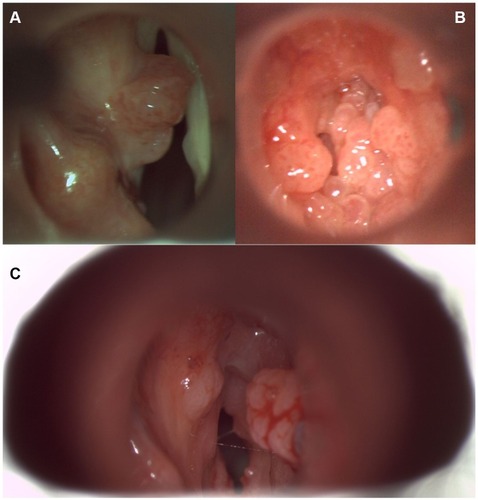
All patients with chronic hoarseness, stridor, and/or respiratory distress should undergo flexible fibreoptic laryngoscopy or direct laryngoscopy and biopsy.Citation56 Unfortunately the expertise and facilities to perform these procedures are not easily accessible in developing countries. The papillomas appears as exophytic, pedunculated masses that can be single or multiple (). In developing countries with a high incidence of tuberculosis, laryngeal tuberculosis may mimic respiratory papillomatosis. Histologically, the papillomas are exophytic finger-like projections of stratified squamous epithelium supported by a connective tissue stroma with abnormal keratinization and basal cell hyperplasia.Citation32,Citation34 Chest imaging by either chest x-ray or CT scan should be performed in patients with RRP, especially those with a clinical presentation suggestive of pulmonary involvement.Citation56
Figure 1 (A-C). Direct laryngoscopy view of laryngeal papillomas.
Staging
The Derkay staging system is the most commonly used system to stage the disease.Citation57 This system comprises both a functional assessment of clinical features and anatomic assessment of disease distribution. A limitation of this staging system is that, although it is effective for describing the presence of disease, the number of sites involved and the bulkiness of each lesion, it does not distinguish the different degrees of severity within a site.Citation58 A higher anatomical score is associated with a shorter intersurgical interval.Citation16
Disease Course
The clinical behavior of laryngeal papillomatosis is unpredictable. In most patients, the frequency of surgery decreases over time, but in approximately one-third of cases the surgical frequency remains constant or increases.Citation7,Citation16,Citation39,Citation59 Although most patients eventually go into remission, in some the disease persists.Citation32 Patients may have recurrence after many years of remission as the latent viral infection persists in the laryngeal tissue.Citation34 No markers have been identified to predict which patients will go into remission or when this will occur. At least 50% of children with RRP require more than 10 procedures to control their disease, and 7% of patients require more than 100 operations during their lifetime.Citation13 The recurrent and persisting nature of the disease and dysphonia that occurs adversely affects patients’ quality of life.Citation60,Citation61
Disease Aggressiveness
Most studies have found HPV11 disease to be more aggressive than HPV6 disease.Citation20,Citation23–Citation27,Citation29,Citation31,Citation33 HPV typing has therefore been suggested as a possible means of predicting disease aggressiveness.Citation29,Citation31,Citation62 However, younger age at diagnosis has been found to be associated with more aggressive disease, and has also been found to be a more significant marker of disease aggressiveness than HPV type.Citation16,Citation20,Citation21,Citation63
Intratypic variants of high risk HPV types have been shown to have characteristic geographical distribution patterns and to have differing pathogenic potential.Citation64 Intratypic variants of HPV6 and HPV11 have been also been shown to vary by geographic area, but not to be as geographically restricted.Citation65,Citation66 The possible role of intratypic variants in differences in severity of respiratory papillomatosis is unclear but may be a result of combinations of alterations in the viral genome.Citation64 The E5, E6 and E7 open reading frames have generally been found to be conserved across variants, suggesting that they play little role in differences in clinical behavior.Citation64 The activity of the long control region of the genome appears to be associated with disease aggressiveness.Citation64,Citation67
Involvement of multiple levels of the larynx or subglottis at initial laryngoscopy is associated with more severe disease.Citation68 On histology, while the degree of dysplasia has not been found to be associated with more severe disease, the presence of atypical mitoses and mitoses above the basal cell layer of the epithelium have been found to be associated with more severe disease.Citation69
A maternal history of condyloma acuminata may be associated with aggressive RRP.Citation7,Citation21,Citation35
Management
There is no cure and treatment consists of repeated microlaryngoscopic procedures to remove the papillomas until the patient goes into remission. Papilloma removal is either with a cupped forceps, laser (CO2, KTP, or flash dye), microdebrider or coblation, depending on the surgeon’s preference and availability of equipment.Citation56 In developing countries, the use of cold steel instruments to remove the papillomas is often the only means of treating these patients.Citation70,Citation71 The aim of surgery is to remove the papillomas with preservation of the normal laryngeal tissue. The use of a laser or microdebrider is not associated with a longer intersurgical interval.Citation16 Treatment with the microdebrider results in a better voice outcome compared with the CO2 laser.Citation72
Further procedures are usually at set intervals, based on an individual patient’s disease severity.Citation56 Patients in developing countries often need to travel great distances to undergo these procedures, placing a considerable social and economic burden on the family.
Complications as a result of repeated surgical procedures are frequent and include anterior laryngeal synechiae, anterior glottic stenosis, posterior glottic stenosis and granuloma formation.Citation17,Citation73,Citation74 These complications result in abnormal vocal quality in the long term, with a greater number of surgical procedures correlating with a more pathologic voice quality.Citation75 Even if all visible papillomas are removed, the disease recurs as HPV DNA is found in the adjacent uninvolved laryngeal tissue as well as other adjacent anatomic sites.Citation18,Citation34
A tracheostomy may be required for patients with airway obstruction. The presence of a tracheostomy has been associated with spread of the papillomas to the trachea and lower airways,Citation17 but this view is controversial as it is usually patients with the most aggressive disease that undergo tracheostomy and these patients may have developed distal spread regardless of whether or not they had a tracheostomy.Citation56 Tracheostomies are performed more frequently in developing countries as a result of the lack of expertise to manage patients with RRP. Case series from sub-Saharan Africa have reported tracheostomy rates of 20.3% in Kenya,Citation46 42–100% in Nigeria,Citation47–Citation49 47% in Mali,Citation50 and 50.8% in Senegal.Citation70 In a Bangladeshi study, 70% of patients with JoRRP required tracheostomies,Citation45 while studies from Thailand report a tracheostomy rate of 13.3–30%.Citation51,Citation74 This is in comparison to a tracheostomy rate of 0–14% in developed countries.Citation13,Citation24,Citation28,Citation29
Adjuvant Treatment
A number of intralesional and systemic adjuvant treatments have been proposed for RRP, including indole-3 carbinol, mumps vaccine, MMR vaccine, HPV vaccination, interferon-α, bevacizumab, cidofovir, programmed cell death protein 1 (PD-1) inhibitors, celecoxib, and alternative treatments. Unfortunately, many of these adjuvant treatments are unavailable or unaffordable in developing countries. The highly variable nature of the disease makes determining the effectiveness of the various adjuvant treatment options difficult as natural fluctuations occur in the criteria used to determine disease severity.Citation59 The International Pediatric Otolaryngology Group (IPOG) recommends against the use of programmed cell death protein 1 (PD-1), colecoxib and heat shock protein E7.Citation56
Intralesional therapies include cidofovir and bevacizumab. Cidofovir is a cytosine nucleotide analog that blocks the replication of DNA viruses by inhibiting viral DNA polymerase. While uncontrolled and retrospective studies have shown intralesional cidofovir to be effective for RRP with approximately 40–50% of patients achieving remission, a systematic review on adjuvant antiviral therapy for the treatment of RRP identified only one randomized double-blind, placebo-controlled trial of intralesional cidofovir administered at the time of surgical debulking with significant clinical improvements in both the cidofovir and placebo groups and no significant difference between the two groups.Citation76–Citation80
Bevacizumab is a recombinant humanized monoclonal antibody that blocks angiogenesis by binding to and inhibiting the biological activity of human vascular endothelial growth factor A (VEGF‐A).Citation81 Intralesional bevacizumab has been shown to prolong the intersurgical interval in small case series,Citation81 while systemic bevacizumab has been shown to be of benefit in patients with highly aggressive disease and those with pulmonary involvement.Citation82,Citation83
Acyclovir has been found to reduce the mean surgical interval in an uncontrolled study in patients with JoRRP,Citation84 but there are a lack of randomized controlled trials. Although the use of both mumps vaccine and measles, mumps and rubella (MMR) vaccine have been reported in the treatment of RRP,Citation85,Citation86 a randomized controlled trial did not find a significant difference in the recurrence-free remission period in patients who were treated with topical MMR vaccine as compared to those in the control group.Citation87
Pepsin has been detected inside the mucosal cell cytoplasm of 45.5% of children with RRP, suggesting that laryngopharyngeal reflux may be a risk factor for JoRRP, contributing to its development by activating or reactivating latent HPV infection.Citation88 Patients with clinical features suggestive of GERD should therefore be treated with a H2-antagonist or proton pump inhibitor.Citation56
Of the three currently available HPV vaccines, the bivalent vaccine (Cervarix®), quadrivalent vaccine (Gardasil®), and nonavalent vaccine (Gardasil® 9), two (Gardasil® and Gardasil® 9) protect against HPV6 and HPV11. In Australia, a significant decrease in the incidence of JoRRP was found following the introduction of a national vaccination program with the quadrivalent HPV vaccine, probably as a result of the maternal source of exposure to HPV6 and HPV11 being eliminated.Citation89 Given the higher incidence of JoRRP in developing countries, the introduction of these vaccines will likely have a greater impact of the incidence of JoRRP. Unfortunately, less than half of UN member states have introduced the HPV vaccine in their national schedule and these are mostly high income and upper middle-income countries, with most low-income and lower middle-income countries not yet having introduced the vaccine.Citation90 Affordability is a major barrier to the introduction of the vaccine.Citation90 In addition, supply is currently insufficient to fully meet the existing demand.Citation90
Although these are prophylactic vaccines, they have been used as adjunctive therapy for RRP, mainly in adults. A systematic review and meta-analysis found a statistically significant reduction in the mean number of surgical procedures per month after HPV vaccination.Citation91 The proposed mechanisms of action include inhibition of latent HPV infection in the mucosa surrounding the surgical site by the antibody-mediated humoral immune response to the vaccine and activation of the cell-mediated response in the adaptive immune response by vaccination.
Speech Therapy
Most patients have poor voice quality that can vary from mild hoarseness to aphonia, which can persist into adulthood.Citation75,Citation92 While formal voice evaluation and therapy may be of value in the management of patients,Citation56 these services are often not available in developing countries.Citation42–Citation44
Conclusions
JoRRP is a condition that initially presents with hoarseness but can result in life-threatening upper airway obstruction. Treatment requires repeated surgical procedures. A significant limiting factor in the early diagnosis and treatment of children with JoRRP in developing countries is the availability and accessibility of healthcare services in general, and ENT services in particular. The introduction of prophylactic vaccines that include HPV6 and HPV11 is necessary in order to reduce the incidence of JoRRP.
Disclosure
The author reports no conflicts of interest in this work.
References
- Seedat RY, Combrinck CE, Burt FJ. HPV associated with recurrent respiratory papillomatosis. Future Virol. 2013;8(5):477–492. doi:10.2217/fvl.13.31
- Seedat RY, Schall R. Age of diagnosis, incidence and prevalence of recurrent respiratory papillomatosis-A South African perspective. Clin Otolaryngol. 2018;43(2):533–537. doi:10.1111/coa.1301629054106
- Ilboudo M, Zohoncon TM, Traore IMA, et al. Implication of low risk human papillomaviruses, HPV6 and HPV11 in laryngeal papillomatosis in Burkina Faso. Am J Otolaryngol - Head Neck Med Surg. 2019;40(3):368–371. doi:10.1016/j.amjoto.2019.02.003
- Matinhira N, Soko ND, Bandason T, et al. Human papillomavirus types causing recurrent respiratory papillomatosis in Zimbabwe. Int J Pediatr Otorhinolaryngol. 2019;116:147–152. doi:10.1016/j.ijporl.2018.10.03630554686
- Sanchez GI, Jaramillo R, Cuello G, et al. Human papillomavirus genotype detection in recurrent respiratory papillomatosis (RRP) in Colombia. Head Neck. 2013;35(2):229–234. doi:10.1002/hed.2295322367608
- San Giorgi MRM, van den Heuvel ER, Tjon Pian Gi REA, et al. Age of onset of recurrent respiratory papillomatosis: a distribution analysis. Clin Otolaryngol. 2016;41(5):448–453. doi:10.1111/coa.1256526460806
- Silverberg MJ, Thorsen P, Lindeberg H, Ahdieh-Grant L, Shah KV. Clinical course of recurrent respiratory papillomatosis in Danish children. Arch Otolaryngol Head Neck Surg. 2004;130(6):711–716. doi:10.1001/archotol.130.6.71115210551
- Novakovic D, Cheng ATL, Cope DH, Brotherton JML. Estimating the prevalence of and treatment patterns for juvenile onset recurrent respiratory papillomatosis in Australia pre-vaccination: a pilot study. Sex Health. 2010;7(3):253–261. doi:10.1071/SH0914220719212
- Ushikai M, Fujiyoshi T, Kono M, et al. Detection and cloning of human papillomavirus DNA associated with recurrent respiratory papillomatosis in Thailand. Jpn J Cancer Res. 1994;85(7):699–703. doi:10.1111/j.1349-7006.1994.tb02417.x8071111
- Bomholt A. Juvenile laryngeal papillomatosis. An epidemiological study from the Copenhagen region. Acta Otolaryngol. 1988;105(3–4):367–371. doi:10.3109/000164888090970203389122
- Lindeberg H, Elbrønd O. Laryngeal papillomas: the epidemiology in a Danish subpopulation 1965-1984. Clin Otolaryngol Allied Sci. 1990;15(2):125–131. doi:10.1111/j.1365-2273.1990.tb00444.x2350888
- Omland T, Akre H, Vårdal M, Brøndbo K. Epidemiological aspects of recurrent respiratory papillomatosis: a population-based study. Laryngoscope. 2012;122(7):1595–1599. doi:10.1002/lary.2332722565595
- Derkay CS. Task force on recurrent respiratory papillomas: a preliminary report. Arch Otolaryngol - Head Neck Surg. 1995;121(12):1386–1391. doi:10.1001/archotol.1995.018901200440087488368
- Armstrong LR, Preston EJ, Reichert M, et al. Incidence and prevalence of recurrent respiratory papillomatosis among children in Atlanta and Seattle. Clin Infect Dis. 2000;31(1):107–109. doi:10.1086/31391410913405
- Marsico M, Mehta V, Chastek B, Liaw K-L, Derkay C. Estimating the incidence and prevalence of juvenile-onset recurrent respiratory papillomatosis in publicly and privately insured claims databases in the United States. Sex Transm Dis. 2014;41(5):300–305. doi:10.1097/OLQ.000000000000011524722383
- Campisi P, Hawkes M, Simpson K. The epidemiology of juvenile onset recurrent respiratory papillomatosis derived from a population level national database. Laryngoscope. 2010;120(6):1233–1245. doi:10.1002/lary.2090120513045
- Soldatski IL, Onufrieva EK, Steklov AM, Schepin NV. Tracheal, bronchial, and pulmonary papillomatosis in children. Laryngoscope. 2005;115(10):1848–1854. doi:10.1097/01.mlg.0000173155.57491.2a16222208
- Pignatari S, Smith EM, Gray SD, Shive C, Turek LP. Detection of human papillomavirus infection in diseased and nondiseased sites of the respiratory tract in recurrent respiratory papillomatosis patients by DNA hybridization. Ann Otol Rhinol Laryngol. 1992;101(5):408–412. doi:10.1177/0003489492101005061315130
- Komloš KF, Kocjan BJ, Košorok P, et al. Tumor-specific and gender-specific pre-vaccination distribution of human papillomavirus types 6 and 11 in anogenital warts and laryngeal papillomas: a study on 574 tissue specimens. J Med Virol. 2012;84(8):1233–1241. doi:10.1002/jmv.2331822711351
- Buchinsky FJ, Donfack J, Derkay CS, et al. Age of child, more than HPV type, is associated with clinical course in recurrent respiratory papillomatosis. PLoS One. 2008;3(5):e2263. doi:10.1371/journal.pone.000226318509465
- Buchinsky FJ, Valentino WL, Ruszkay N, et al. Age at diagnosis, but not HPV type, is strongly associated with clinical course in recurrent respiratory papillomatosis. PLoS One. 2019;14(6):e0216697. doi:10.1371/journal.pone.021669731194767
- Kocjan BJ, Gale N, Hocevar Boltezar I, et al. Identical human papillomavirus (HPV) genomic variants persist in recurrent respiratory papillomatosis for up to 22 years. J Infect Dis. 2012. doi:10.1093/infdis/jis733
- Rimell FL, Shoemaker DL, Pou AM, Jordan JA, Post JC, Ehrlich GD. Pediatric respiratory papillomatosis: prognostic role of viral typing and cofactors. Laryngoscope. 1997;107(7):915–918. doi:10.1097/00005537-199707000-000159217130
- Carvalho CM, Huot L, Charlois A-L, Khalfallah SA, Chapuis F, Froehlich P. Prognostic factors of recurrent respiratory papillomatosis from a registry of 72 patients. Acta Otolaryngol. 2009;129(4):462–470. doi:10.1080/0001648090273798619235575
- Shehata BM, Otto KJ, Sobol SE, et al. E6 and E7 oncogene expression by human papilloma virus (HPV) and the aggressive behavior of recurrent laryngeal papillomatosis (RLP). Pediatr Dev Pathol. 2008;11(2):118–121. doi:10.2350/06-09-0160.117990904
- Maloney EM, Unger ER, Tucker RA, et al. Longitudinal measures of human papillomavirus 6 and 11 viral loads and antibody response in children with recurrent respiratory papillomatosis. Arch Otolaryngol Head Neck Surg. 2006;132(7):711–715. doi:10.1001/archotol.132.7.71116847177
- Draganov P, Todorov S, Todorov I, Karchev T, Kalvatchev Z. Identification of HPV DNA in patients with juvenile-onset recurrent respiratory papillomatosis using SYBR Green real-time PCR. Int J Pediatr Otorhinolaryngol. 2006;70(3):469–473. doi:10.1016/j.ijporl.2005.07.01816137771
- Hartley C, Hamilton J, Birzgalis AR, Farrington WT. Recurrent respiratory papillomatosis–the Manchester experience, 1974-1992. J Laryngol Otol. 1994;108(3):226–229. doi:10.1017/S00222151001263508169504
- Wiatrak BJ, Wiatrak DW, Broker TR, Lewis L. Recurrent respiratory papillomatosis: a longitudinal study comparing severity associated with human papilloma viral types 6 and 11 and other risk factors in a large pediatric population. Laryngoscope. 2004;114(11Pt 2 Suppl 104):1–23. doi:10.1097/01.mlg.000148224.83491.0f
- Padayachee A, Prescott CA. Relationship between the clinical course and HPV typing of recurrent laryngeal papillomatosis. The Red Cross War Memorial Children’s Hospital experience 1982-1988. Int J Pediatr Otorhinolaryngol. 1993;26(2):141–147. doi:10.1016/0165-5876(93)90019-Y8383099
- Rabah R, Lancaster WD, Thomas R, Gregoire L. Human papillomavirus-11-associated recurrent respiratory papillomatosis is more aggressive than human papillomavirus-6-associated disease. Pediatr Dev Pathol. 2001;4(1):68–72. doi:10.1007/s10024001010511200493
- Somers GR, Tabrizi SN, Borg AJ, Garland SM, Chow CW. Juvenile laryngeal papillomatosis in a pediatric population: a clinicopathologic study. Pediatr Pathol Lab Med. 1997;17(1):53–64. doi:10.1080/155138197091683469050060
- Seedat RY, Thukane M, Jansen AC, Rossouw I, Goedhals D, Burt FJ. HPV types causing juvenile recurrent laryngeal papillomatosis in South Africa. Int J Pediatr Otorhinolaryngol. 2010;74(3):255–259. doi:10.1016/j.ijporl.2009.11.01620018386
- Abramson AL, Steinberg BM, Winkler B. Laryngeal papillomatosis: clinical, histopathologic and molecular studies. Laryngoscope. 1987;97(6):678–685. doi:10.1288/00005537-198706000-000053035299
- Gerein V, Schmandt S, Babkina N, Barysik N, Coerdt W, Pfister H. Human papilloma virus (HPV)-associated gynecological alteration in mothers of children with recurrent respiratory papillomatosis during long-term observation. Cancer Detect Prev. 2007;31(4):276–281. doi:10.1016/j.cdp.2007.07.00417935912
- Silverberg MJ, Thorsen P, Lindeberg H, Grant LA, Shah KV. Condyloma in pregnancy is strongly predictive of juvenile-onset recurrent respiratory papillomatosis. Obstet Gynecol. 2003;101(4):645–652. doi:10.1016/s0029-7844(02)03081-812681865
- Kashima HK, Shah F, Lyles A, et al. A comparison of risk factors in juvenile-onset and adult-onset recurrent respiratory papillomatosis. Laryngoscope. 1992;102(1):9–13. doi:10.1288/00005537-199201000-000021309932
- Reyes LM, Aguilar JL, Villamor P, et al. Clinical and sociodemographic characteristics associated with disease severity in juvenile recurrent respiratory papillomatosis: a study of 104 patients in a tertiary care pediatric hospital. Int J Pediatr Otorhinolaryngol. 2018;108:63–66. doi:10.1016/j.ijporl.2018.02.02529605367
- Hawkes M, Campisi P, Zafar R, et al. Time course of juvenile onset recurrent respiratory papillomatosis caused by human papillomavirus. Pediatr Infect Dis J. 2008;27(2):149–154. doi:10.1097/INF.0b013e318159833e18174855
- Seedat RY. The incidence and prevalence of juvenile-onset recurrent respiratory papillomatosis in the Free State province of South Africa and Lesotho. Int J Pediatr Otorhinolaryngol. 2014;78(12):2113–2115. doi:10.1016/j.ijporl.2014.09.01725300480
- Maïga S, Ndiaye C, Diouf M, et al. Laryngeal papillomatosis in Senegal: a ten-year experience. Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135(3):221–224. doi:10.1016/j.anorl.2018.01.00229396224
- Mulwafu W, Ensink R, Kuper H, Fagan J. Survey of ENT services in sub-Saharan Africa: little progress between 2009 and 2015. Glob Health Action. 2017;10(1):1289736. doi:10.1080/16549716.2017.128973628485648
- Peer S, Vial I, Numanoglu A, Fagan JJ. What is the availability of services for paediatric ENT surgery and paediatric surgery in Africa? Eur Ann Otorhinolaryngol Head Neck Dis. 2018;135(5):S79–S83. doi:10.1016/j.anorl.2018.07.00530143398
- Wagner R, Fagan J. Survey of otolaryngology services in Central America: need for a comprehensive intervention. Otolaryngol Head Neck Surg. 2013;149(5):674–678. doi:10.1177/019459981350597224057675
- Majumder SMKA, Ibrahim MF, Huda QKKMN, Bhattacharjee N, Amin MN. Recurrent respiratory papillomatosis: a study of 24 cases. Bangladesh Med Res Counc Bull. 1999;25(2):46–50.11026935
- Muriithi CM Recurrent respiratory papillomatosis at Kenyatta National Hospital, Nairobi-Kenya A ten year retrospective study between January 1990-December 1999. [dissertation]. Nairobi: University of Nairobi; 2001.
- Fasunla AJ, Lasisi OA. Diagnostic challenges of laryngeal papillomatosis and its implications among children in developing country. Int J Pediatr Otorhinolaryngol. 2009;73(4):593–595. doi:10.1016/j.ijporl.2008.12.00919157575
- Orji FT, Okorafor IA, Akpeh JO. Experience with recurrent respiratory papillomatosis in a developing country: impact of tracheostomy. World J Surg. 2012;37(2):339–343. doi:10.1007/s00268-012-1839-y
- Adoga AA, Nimkur LT, Adoga AS. Recurrent respiratory papillomatosis in Jos, Nigeria: clinical presentation, management and outcome. East Cent African J Surg. 2008;13(2):105–108.
- Timbo SK, Konipo-Togola F, Mohamed AA, Keita MA, Sacko HB, Traore L. Papillomatose laryngée au Mali. À propos de 19 cas colligés à l’hôpital Gabriel-Touré de Bamako. Bull Soc Pathol Exot. 2002;95(1):31–33.12012961
- Intakorn P, Sonsuwan N. Human papillomatosis genotyping and severity in patients with recurrent respiratory papillomatosis. J Med Assoc Thai. 2014;97(Suppl 6):S136–S141.
- Grobbelaar J, Seedat RY, Brown S, Claassen AJ. Pulmonary hypertension due to recurrent juvenile laryngeal papillomatosis. Int J Pediatr Otorhinolaryngol. 2005;69(9):1279–1282. doi:10.1016/j.ijporl.2005.03.01916061114
- Armstrong LR, Derkay CS, Reeves WC. Initial results from the national registry for juvenile-onset recurrent respiratory papillomatosis. RRP task force. Arch Otolaryngol Head Neck Surg. 1999;125(7):743–748. doi:10.1001/archotol.125.7.74310406310
- Lindeberg H, Elbrønd O. Laryngeal papillomas: clinical aspects in a series of 231 patients. Clin Otolaryngol. 1989;14(4):333–342. doi:10.1111/j.1365-2273.1989.tb00381.x2805372
- Gélinas J-F, Manoukian J, Côté A. Lung involvement in juvenile onset recurrent respiratory papillomatosis: a systematic review of the literature. Int J Pediatr Otorhinolaryngol. 2008;72(4):433–452. doi:10.1016/j.ijporl.2007.12.00318281102
- Lawlor C, Balakrishnan K, Bottero S, et al. International Pediatric Otolaryngology Group (IPOG): juvenile-onset recurrent respiratory papillomatosis consensus recommendations. Int J Pediatr Otorhinolaryngol. 2020;128:109697. doi:10.1016/j.ijporl.2019.10969731698245
- Suter-Montano T, Montaño E, Martínez C, Plascencia T, Sepulveda MT, Rodríguez M. Adult recurrent respirator papillomatosis: a new therapeutic approach with pegylated interferon alpha 2a (Peg-IFNα-2a) and GM-CSF. Otolaryngol Head Neck Surg. 2013;148(2):253–260. doi:10.1177/019459981246622623124924
- Lee AS, Rosen CA. Efficacy of cidofovir injection for the treatment of recurrent respiratory papillomatosis. J Voice. 2004;18(4):551–556. doi:10.1016/j.jvoice.2003.07.00715567056
- Ongkasuwan J, Friedman EM. Juvenile recurrent respiratory papilloma: variable intersurgical intervals. Laryngoscope. 2012;122(12):2844–2849. doi:10.1002/lary.2353422847877
- Montaño-Velázquez BB, Nolasco-Renero J, Parada-Bañuelos JE, et al. Quality of life of young patients with recurrent respiratory papillomatosis. J Laryngol Otol. 2017;131(5):425–428. doi:10.1017/S002221511700035428193306
- Chadha NK, Allegro J, Barton M, Hawkes M, Harlock H, Campisi P. The quality of life and health utility burden of recurrent respiratory papillomatosis in children. Otolaryngol Head Neck Surg. 2010;143(5):685–690. doi:10.1016/j.otohns.2010.08.00520974340
- Combrinck CE, Seedat RY, Burt FJ. FRET-based detection and genotyping of HPV-6 and HPV-11 causing recurrent respiratory papillomatosis. J Virol Methods. 2013;189:271–276. doi:10.1016/j.jviromet.2013.01.02523473839
- Cuello G, Sánchez GI, Jaramillo R, et al. Clinical characteristics and HPV type in recurrent respiratory papillomatosis in Colombia. Salud Publica Mex. 2013;55(4):416–420. doi:10.21149/spm.v55i4.722624165718
- Gáll T, Kis A, Tatár TZ, Kardos G, Gergely L, Szarka K. Genomic differences in the background of different severity in juvenile-onset respiratory papillomatoses associated with human papillomavirus type 11. Med Microbiol Immunol. 2013;202(5):353–363. doi:10.1007/s00430-013-0297-y23649705
- Jelen MM, Chen Z, Kocjan BJ, et al. Global genomic diversity of human papillomavirus 6 based on 724 isolates and 190 complete genome sequences. J Virol. 2014;88(13):7307–7316. doi:10.1128/JVI.00621-1424741079
- Jelen MM, Chen Z, Kocjan BJ, et al. Global genomic diversity of human papillomavirus 11 based on 433 isolates and 78 complete genome sequences. J Virol. 2016;90(11):5503–5513. doi:10.1128/JVI.03149-1527030261
- Seedat RY, Combrinck CE, Bester PA, Lee J-Y, Burt FJ. Determination of the complete genome and functional analysis of HPV6 isolate VBD19/10 from a patient with aggressive recurrent respiratory papillomatosis. Epidemiol Infect. 2016;144(10):2128–2135. doi:10.1017/S095026881600038826931553
- Moreddu E, Lambert E, Kacmarynski D, Nicollas R, Triglia J-M, Smith RJ. Risk factors for severity of juvenile-onset recurrent respiratory papillomatosis at first endoscopy. Eur Ann Otorhinolaryngol Head Neck Dis. 2019;136(1):25–28. doi:10.1016/j.anorl.2018.11.00730503689
- El Achkar VNR, Duarte A, Carlos R, et al. Histopathological features of juvenile‐onset laryngeal papillomatosis related to severity. Head Neck. 2019;41(5):1412–1417. doi:10.1002/hed.2560230623508
- Malick N, Cheikh NI, Arnaud IOF, et al. Laryngeal papillomatosis in children. Oto-Rhino-Laryngologie Française. 2008;94:379–381.
- Aliyu MK, Abimiku SL, Babagana MA, Musa E. Recurrent respiratory papillomatosis: management outcome at national ear care centre, Kaduna. Borno Med J. 2010;7(2):5–7.
- Holler T, Allegro J, Chadha NK, et al. Voice outcomes following repeated surgical resection of laryngeal papillomata in children. Otolaryngol Head Neck Surg. 2009;141(4):522–526. doi:10.1016/j.otohns.2009.06.08019786223
- Hermann JS, Pontes P, Weckx LLM, Fujita R, Avelino M, Pignatari SSN. Laryngeal sequelae of recurrent respiratory papillomatosis surgery in children. Rev Assoc Med Bras. 2012;58(2):204–208. doi:10.1016/S0104-4230(12)70181-122569615
- Antarasena S. Clinical study of juvenile laryngeal papilloma. Acta Otolaryngol Suppl. 1988;458:163–166. doi:10.3109/000164888091251233245425
- Ilmarinen T, Nissilä H, Rihkanen H, et al. Clinical features, health-related quality of life, and adult voice in juvenile-onset recurrent respiratory papillomatosis. Laryngoscope. 2011;121(4):846–851. doi:10.1002/lary.2133221400536
- Graupp M, Gugatschka M, Kiesler K, Reckenzaun E, Hammer G, Friedrich G. Experience of 11 years use of cidofovir in recurrent respiratory papillomatosis. Eur Arch Otorhinolaryngol. 2013;270(2):641–646. doi:10.1007/s00405-012-2221-223070260
- Valera F, Maldonato L, Lima J, et al. Efficacy of cidofovir in recurrent juvenile respiratory papillomatosis. Braz J Otorhinolaryngol. 2010;76(6):713–717. doi:10.1590/S1808-8694201000060000821180938
- Derkay C. Cidofovir for recurrent respiratory papillomatosis (RRP): a re-assessment of risks. Int J Pediatr Otorhinolaryngol. 2005;69(11):1465–1467. doi:10.1016/j.ijporl.2005.08.00716174538
- Chadha NK, James A. Adjuvant antiviral therapy for recurrent respiratory papillomatosis. Cochrane Database Syst Rev. 2012;12(1):CD005053. doi:10.1002/14651858.CD005053.pub423235619
- McMurray JS, Connor N, Ford CN. Cidofovir efficacy in recurrent respiratory papillomatosis: a randomized, double-blind, placebo-controlled study. Ann Otol Rhinol Laryngol. 2008;117(7):477–483. doi:10.1177/00034894081170070218700421
- Maturo S, Hartnick CJ. Use of 532-nm pulsed potassium titanyl phosphate laser and adjuvant intralesional bevacizumab for aggressive respiratory papillomatosis in children: initial experience. Arch Otolaryngol Head Neck Surg. 2010;136(6):561–565. doi:10.1001/archoto.2010.8120566906
- Mohr M, Schliemann C, Biermann C, et al. Rapid response to systemic bevacizumab therapy in recurrent respiratory papillomatosis. Oncol Lett. 2014;8(5):1912–1918. doi:10.3892/ol.2014.248625289079
- Zur KB, Fox E. Bevacizumab chemotherapy for management of pulmonary and laryngotracheal papillomatosis in a child. Laryngoscope. 2017;127(7):1538–1542. doi:10.1002/lary.2645027996119
- Mitra S, Das A, Ghosh D, Sengupta A. Postoperative systemic acyclovir in juvenile-onset recurrent respiratory papillomatosis: the outcome. Ear Nose Throat J. 2019;98(1):28–31. doi:10.1177/014556131882331130834790
- Pashley NRT. Can mumps vaccine induce remission in recurrent respiratory papilloma? Arch Otolaryngol Head Neck Surg. 2002;128(7):783–786. doi:10.1001/archotol.128.7.78312117334
- Wang Y, Dai PD, Zhang TY. Experimental research on the therapeutic effect of MMR vaccine to juvenile-onset recurrent respiratory papillomatosis. Eur Arch Oto-Rhino-Laryngol. 2019;276(3):801–803. doi:10.1007/s00405-019-05351-6
- Lei J, Yu W, Yuexin L, Qi C, Xiumin S, Tianyu Z. Topical measles-mumps-rubella vaccine in the treatment of recurrent respiratory papillomatosis: results of a preliminary randomized, controlled trial. Ear Nose Throat J. 2012;91(4):174–175. doi:10.1177/01455613120910041122522357
- Formánek M, Komínek P, Jančatová D, et al. Laryngopharyngeal reflux is a potential risk factor for juvenile-onset recurrent respiratory papillomatosis. Biomed Res Int. 2019;2019:1463896. doi:10.1155/2019/146389630881982
- Novakovic D, Cheng ATL, Zurynski Y, et al. A prospective study of the incidence of juvenile-onset recurrent respiratory papillomatosis after implementation of a national HPV vaccination program. J Infect Dis. 2018;217(2):208–212. doi:10.1093/infdis/jix49829136168
- World Health Organization. Global Market Study: HPV Vaccines; 2019 Available from: https://www.who.int/immunization/programmes_systems/procurement/v3p/platform/module2/WHO_HPV_market_study_public_summary.pdf. Accessed September 30, 2019.
- Rosenberg T, Philipsen BB, Mehlum CS, et al. Therapeutic use of the human papillomavirus vaccine on recurrent respiratory papillomatosis: a systematic review and meta-analysis. J Infect Dis. 2019;219(7):1016–1025. doi:10.1093/infdis/jiy61630358875
- Verma H, Solanki P, James M. Acoustical and perceptual voice profiling of children with recurrent respiratory papillomatosis. J Voice. 2016;30(5):600–605. doi:10.1016/j.jvoice.2015.06.00826474713