
Abstract
WHO has confirmed that COVID-19 disease is a pandemic on March 11, 2020. The disease is caused by a new virus called SARS-CoV-2. Since, the pandemic was announced around 18,854,287 cases and 708,639 deaths were reported as of August 7, 2020. This review aimed to explore the etiology, pathogenesis, manifestation and complication. The phylogenetic study showed that SARS-CoV-2 is a single-stranded RNA virus. The virus is very contagious and has rapidly spread globally. Its unique structure called S glycoproteins help the virus enters in and cause infection in the body. Children’s body reacts against SARS-CoV-2 infections through the involvement of innate and adaptive immune system. The clinical manifestation in children is not specific and not determined. However, fever and cough have mostly been profiled. Though the severe condition is rarely reported in children compared with adults, life-threatening complications, and death associated with COVID-19 disease have been documented. Underlying chronic pulmonary disease, cardiovascular disease, immunosuppression, and obesity significantly contribute to the complications.
Background
In the history of Human beings, there have been different pandemics, such as Cholera, bubonic plague, smallpox, and influenza.Citation1 In the 21st century, most of the pandemics were caused by either coronavirus or influenza virus.Citation2 The cause for the current COVID-19 pandemic is also coronavirus. The pandemic is causing a global health and socio-economic crisis and is the major problem encountered after the second global war that lasted from 1939 to 1945. Following its first report in December 2019, SARS-CoV-2 almost reached all over the world.Citation3 It was at the beginning identified as an outbreak of cases of pneumonia with an unexplained cause in China. It was first informed to the World Health Organization (WHO) in December 2019.Citation4
The World Health Organization (WHO) stated Coronavirus disease 2019 as a pandemic on March 11, 2020. The etiology for Coronavirus disease 2019 is a newly identified virus called SARS-CoV-2.Citation5 Individuals infected with the virus can transmit to a healthy person mainly through droplets discharged from the nose and mouth.Citation6 So far, no one has identified specific vaccination or medicine for the disease.Citation7 According to the latest data, around 18,854,287 COVID-19 confirmed cases and 708,639 associated deaths of all ages have been reported from 215 countries as of August 7,2020.Citation8
At the earlier outsets of Covid-19 pandemics, children were believed to have mild COVID-19.Citation9 However, at later time children seriously affected with COVID-19 have appeared to be seen.Citation10 One study in USA reported nearly 5.7% of pediatric patients have been admitted in hospitals.Citation11 Another study conducted among children admitted in ICU in USA showed that nearly 69% of children were critically ill and 38% who were in ICU required ventilation.Citation12 Infants appeared to be affected more seriously than older children. Nearly 11% of infants had serious cases compared to 3% of ages 16 and older.Citation13
In contrast to adults, fewer children were reported to encounter critical illness and admission. Earlier data from china reported nearly 2.4% children with COVID-19 were aged 19 or younger. Besides, only 0.2% pediatrics encountered life threatening complication in contrast with 6.1% overall.Citation11 Similarly, other studies from the USA supported the risk of life threatening complication in children is lower than adults. Hospitalization rate appeared to rise as the age increases. Among children less than 19 years old, only 2–3% of them were hospitalized when more than 31% of patients older than 85 years were hospitalized.Citation14 Furthermore, about 6% of children have been reported to have a critical illness, compared to 18.5% of adults.Citation15 The age-specific fatality ratio appeared to rise from 0.1% in children aged ≤19 years to approximately 80% in adults aged ≥60 years.Citation16 Following treatment children typically recovered within 3 to 4 days.Citation11
Different studies have attempted to characterize the manifestation of COVID-19 disease in children.Citation17 However, the clinical presentation of COVID-19 exclusively in children has not yet been extensively studied. Even the available study showed contradicting findings. For instance, a study from China suggests that children with COVID-19 might have different symptoms than adults.Citation13 On the contrary, another study reported that COVID-19 has similar manifestation both in children and adults.Citation18 This contradicting finding showed how far extensive research is required to enrich the body of knowledge regarding COVID-19 characteristics in children. Thus, this review of existing literature was conducted with the hope to provide an insight into the disease in children. Hence, readers can refer to this review to increase their awareness.
Basics of Etiology
There have been seven corona virus species infecting human being. In 1965s the first coronavirus that infect human being was recognized. The seventh type of newly identified coronavirus is known as SARS-CoV-2.Citation19 Coronaviruses are single-stranded, positive-sense, enveloped, RNA viruses with a crown-like appearance. Genera of corona viruses have been categorized into four: Deltacoronavirus (deltaCoV), Gammacoronavirus (gammaCoV), Alphacoronavirus (alphaCoV), and Betacoronavirus (betaCoV).Citation20 Coronaviruses are involved in human. They can infect, gastrointestinal, respiratory, central nervous system, and hepatic of human and vertebrate’s diseases.Citation21
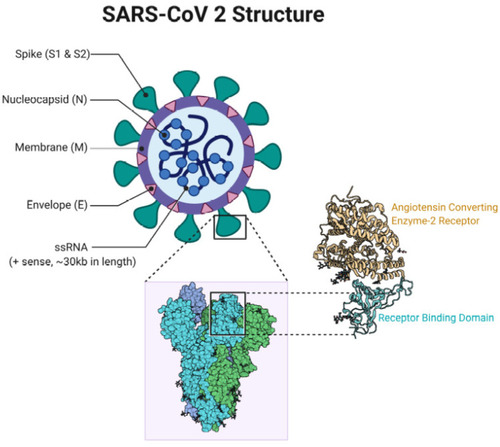
SARS-CoV-2 goes to βCoVs, however SARS-CoV-2 is different from other viruses belonging to βCoVs.Citation22 Bats and rodents have been suspected as the source of βCoVs . The virus has four main structural proteins, namely core nucleocapsid (N) protein, envelope (E), membrane (M) glycoprotein, and spike (S) glycoprotein.Citation23 (see ). Among them, S proteins (S1 and S2 subunits) has the most important function in viral attachment, fusion, and entry into cells.Citation24
Figure 1 SARS-CoV-2 structure.
Pathogenesis
Mucous membranes of the respiratory tract are the way through which SARS-CoV-2 might get to the lung. From the lung, the virus enters into the blood circulation and reach different organs.Citation25 SARS‐CoV‐2 may use angiotensin‐converting enzyme 2 (ACE2) as a host cell receptor to get in and cause infection in humans. This receptor is found widely in various organs, such as the gastrointestinal tract, the lung, heart, and kidney. These organs are targets of SARS-CoV-2.Citation26 Pathophysiology mechanisms of SARS-CoV-2 have been linked to the function of the nonstructural proteins and structural proteins.
The replication process of SARS-CoV-2 follows five steps: (i) binding to receptor, (ii) fusion in to host cell, (iii) RNA translation, (iv) viral maturation, and (v) bud out.Citation27 The spike protein of coronavirus, S1 substructure facilitates the virus attachment with receptors whereas S2 substructure help cell membrane integration.Citation28 After the virus binds with the host cell, S protein will undergo conformational change by a host cell serine protease called TMPRSS2 which leads to viral entry through the process of endocytosis.Citation29 Following the viral entry into the cells, the viral RNA genome is released into the cytoplasm. Then from the released RNA structural proteins and polyproteins will be synthesized, finally the reproduced virus will be released out.Citation30
Viral entry and cell infection stimulate the body’s immune reaction. In response to the antigen, the inflammatory process is initiated by antigen-presenting cells. After the antigen (virus) is presented, T cells will identify the virus.Citation31 In reaction to antigen presentation, both cell mediated and antibody mediated immune responses will be stimulated. The immune response is mediated by T lymphocytes and B lymphocytes. T helper cells (i.e. CD8+ and CD4+) predominantly play the fight against the virus. The CD4+ initiate B lymphocytes to produce antigen-targeted antibodies, while the cytotoxic cells (CD8+) attack viral diseased cells.Citation32
The fact that most infected children experience mild symptoms and have a better prognosis continuous to hold.Citation33,Citation34 Although the reason is not yet clear, several theories have been proposed to explain it. One of the likely reasons is that children are thought to have fewer ACE2 and TMPRSS2 receptors in their nasal tissue than adults. These receptors help the virus entry in to host body. That is the reason why pneumonia and ARDS is not common in kids with COVID-19 compared to adults.Citation35 Another possible explanation is tied to immune response, overzealous pulmonary inflammatory mediators, termed as cytokine storm is rare in children. An exaggerated immune response may end up in extreme inflammation, thereby eventually causing more severe damage. Children, with immature immune systems, appear to be less capable of mounting cytokine storms suggesting why children do not seem to be getting severely ill.Citation36 It has also been suggested that early childhood vaccines provide some protective immunity against SARS-CoV-2 in children. Studies have suggested that, in contrast to adult vaccines can protect children from acquiring COVID-19 disease.Citation37 The overall pathogenesis is indicated in .
Figure 2 Pathogenesis, corona replication.

Clinical Manifestation
Children of all ages can be affected by COVID-19 disease.Citation38 They may show symptoms within 2–14 days after being infected by SARS-CoV-2.Citation39 The symptoms have been reported to be milder than adults.Citation40 Male children constitute a greater proportion than females.Citation41 A study conducted on children with COVID-19 delineated a spectrum of clinical appearances from no symptom to sever condition. The manifestation can be categorized in to five stage depending on the severity of clinical progression: (i) the initial characteristics is no apparent clinical signs, (ii) minor clinical symptoms such as cough, fever, myalgia, fatigue (iii) subclinical pneumonia, (iv) Severe pneumonia characterized with hypoxia, dyspnea and central cyanosis, and (v) Critical stage involving complication like shock, ARDS and multi-organ failure.Citation13 The clinical feature in children is somehow different from adults. The most common symptom is fever, like in adults, but the incidents of productive cough, vomiting, and diarrhea are much higher than in adults.Citation42 Unlike adults, dry cough and phlegm are not the most common symptoms.Citation43 Children rarely progressed to acute respiratory distress syndrome than adults.Citation44
Although children have milder symptoms compared to adults, it is important however to note the clinical feature in children may progress to critical condition.Citation45 COVID-19 in young infants often has an unexplained fever along with mild respiratory symptoms.Citation46 The most frequently profiled symptoms for children are cough and fever.Citation10,Citation11 In a study that evaluated 171 children with confirmed SARS-CoV-2 infection in China, the most common reported symptoms were: fever (41.5%), cough 48.5%), and pharyngeal erythema (46.2%).Citation47 Recently, a systematic review that identified 131 studies comprising 7780 pediatric patients across 26 countries indicated, most common clinical manifestations. They reported that the frequently encountered symptoms are rhinorrhea (20.0%), fever (59.1%), myalgia/fatigue (18.7%), and cough (55.9%).Citation44 Some children presented with mild or often ignored symptoms such as nasal congestion, nausea, abdominal discomfort, diarrhea, vomiting, and abdominal pain.Citation48,Citation49 Rash was also documented as infrequent sign among children with COVID-19. Dyspnea or hypoxemia and, sign and symptoms of multi-organ failure were rarely described.Citation18 Moreover, ARDS and pneumothorax were indicated in children with COVID-19 very rarely.Citation50
Laboratory Findings
The viral antigen (SARS-CoV-2 nucleic acid) is identified using real-time reverse transcriptase-polymerase chain reaction (RT-PCR). The preferred sample comes from nasopharyngeal swab. The American CDC recommends the swab must be introduced into the nostril and left inside for some seconds. Soon after sample collection, the sample has to be kept in sterile tubes containing 2–3 mL of viral transport media. Samples have to be kept at 2–8°C for about 72 hours after collection.Citation51 The virus can also be detected in stool, sputum, urine, and blood.Citation52
Based on current data, a consistently similar result of laboratory findings has not yet been reported in children. The laboratory result varies with the severity of COVID-19 disease.Citation53 It has been noted that in the early time following the disease onset, either normal or decreased white blood cell count and marginally elevated lymphocyte count have been observed. The majority of patients have normal neutrophil counts.Citation54,Citation55 Severe cases may be accompanied by; increased serum inflammatory markers such as D-dimer, procalcitonin, creatine kinase, and interleukin-6 and progressively decreased lymphocyte.Citation44,Citation56 summarizes the laboratory changes observed in mild and sever cases of COVID-19 in children
Table 1 Summary Laboratory Changes with the Severity of COVID-19
Myoglobin, muscle and hepatic enzymes appeared to rise in kids. Increased CRP and erythrocyte sedimentation rates have also been reported.Citation57 On the other hand, an observational cohort study from China reported that elevated creatine kinase, decreased lymphocytes, leucopenia, and elevated procalcitonin are typical abnormal laboratory results among children with COVID-19.Citation58
The laboratory report in children is somehow different from adults.Citation43 In contrast to adults, the white blood cell counts of children were all normal, with decreased neutrophil counts and increased lymphocyte counts. The value of PCT showed no difference between children and adults, however, an elevated level of CRP and IL-6 was shown in adults, but not in children. Children have higher level of LDH compared to adults.Citation43 The comparison of characteristics of laboratory result in children and adults is summarized in .
Table 2 Comparison of Laboratory Finding Among Adults and Children with COVID-19
Complications
So far, studies reported that children appear to be less affected by this new coronavirus. But the report showed this rare case my cause several life-threatening complications. Children under 18 years of age with COVID-19, 5.7–20% were hospitalized compared 10–33% adults aged 18–64 years. Besides, 0.58–2.0% children were admitted to an ICU compared to 1.4–4.5% adults. Children aged <1 year accounted for the highest percentage 15–62% of hospitalization among pediatric patients with COVID-19.Citation11 A syndrome called pediatric inflammatory multisystem disorder which is associated with COVID-19 has been reported widely. The syndrome appears four to six weeks after infection and manifested by high fever, low blood pressure, and abdominal pain.Citation59 Some children have experienced kidney injury, inflammation in the heart, gastrointestinal symptoms, or excessive blood clotting.Citation60 One study on children with the underlying medical problem has reported that few of them developed failure of two or more organ systems as a result of COVID-19 disease, while many of them developed acute respiratory syndrome and supported with a ventilator.Citation61,Citation62
Risk Factors to Severe Disease
Most infected children have had mild symptoms with no fever or pneumonia, and have an excellent prognosis.Citation63 However; few of them suffer from life-threatening complications. Few studies have tried to show that children with underlying serious conditions appear to be at greatest risk. The most commonly profiled underlying chronic conditions are chronic pulmonary disease, cardiovascular disease, immunosuppression, and obesity. Another conditions that may increase the risk of severe disease are seizure, kidney disease, liver disease, an endocrine disorder, and age less than 1 year.Citation11,Citation64
Conclusion
The current COVID-19 pandemic is a global public health concern. Research is progressing at an unprecedented speed. Our knowledge regarding the disease in children is evolving from time-to-time. Despite fewer children with COVID-19 have been reported, they are more at risk than adults to be infected with the virus. In most cases, clinical manifestation of the disease in children is not clearly specific and often mild or asymptomatic. Severe conditions, such as life-threatening complications and death associated with the disease have rarely been reported. On top of that, the presentation of COVID-19 disease in children is not intensely studied. An intense investigation of the clinical presentation in children is very important.
Ethical Approval
Ethical approval was obtained from the College of Health Science, Mizan Tepi University Ethical Review Board.
Acknowledgment
I would like to forward my heartfelt gratitude to my colleague Mrs. Bethelihem Abebe for her support in each step of my review. I would also like to extend my sincere thanks for Dr. Gizelle Arnold for her help in editing the English language.
Disclosure
The author reports no conflicts of interest in this work.
Additional information
Funding
References
- MPH online. Outbreak: 10 of the worst pandemics in history [Internet]. 2020 [cited Jun 4, 2020] Available from: https://www.mphonline.org/worst-pandemics-in-history/. Accessed 828, 2020.
- How does COVID-19 compare to past pandemics? Gavi, the vaccine alliance [internet]. [cited Jul 27, 2020] Available from: https://www.gavi.org/vaccineswork/how-does-covid-19-compare-past-pandemics. Accessed 828, 2020.
- Coronavirus disease COVID-19 pandemic. UNDP [Internet]. [cited Jul 27, 2020] Available from: https://www.undp.org/content/undp/en/home/coronavirus.html. Accessed 828, 2020.
- How Coronavirus Spreads. CDC [Internet]. [cited Jul 27, 2020] Available from: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fabout%2Findex.html. Accessed 828, 2020.
- WHO Director-General’s opening remarks at the media briefing on COVID-19–11 March 2020 [Internet]. [cited Jul 27, 2020] Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020. Accessed 828, 2020.
- Santarpia JL, Rivera DN, Herrera V, et al. Transmission potential of SARS-CoV-2 in viral shedding observed at the University of Nebraska Medical center. medRxiv. 2020;03(23):20039446.
- World Health Organization. Coronavirus [Internet]. 2020 [cited Jun 4, 2020] Available from: https://www.who.int/health-topics/coronavirus#tab=tab_1. Accessed 828, 2020.
- World health organization. WHO Coronavirus Disease (COVID-19) Dashboard [Internet]. 2020 [cited Jun 10, 2020] Available from: https://covid19.who.int/. Accessed 828, 2020.
- World health organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19) [Internet]. 2020 [cited Jun 4, 2020] Available from: https://www.who.int/publications-detail/report-of-the-who-china-joint-mission-on-coronavirus-disease-2019-(covid-19). Accessed 828, 2020.
- Parri N, Lenge M, Buonsenso D. Coronavirus Infection in Pediatric Emergency Departments (CONFIDENCE) research group. Children with covid-19 in pediatric emergency departments in Italy. N Engl J Med. 2020;383(2):187–190. doi:10.1056/NEJMc200761732356945
- Bialek S, Gierke R, Hughes M, McNamara LA, Pilishvili T, Skoff T, CDC COVID-19 Response Team. Coronavirus disease 2019 in children — United States, February 12–April 2, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(14):422–426. doi:10.15585/mmwr.mm6914e432271728
- Study: 38% of kids in ICU with COVID-19 needed ventilation. CIDRAP [Internet]. [cited Jul 27, 2020] Available from: https://www.cidrap.umn.edu/news-perspective/2020/05/study-38-kids-icu-covid-19-needed-ventilation. Accessed 828, 2020.
- Dong Y, Mo X, Hu Y, et al. Epidemiological characteristics of 2143 pediatric patients with 2019 coronavirus disease in China. Pediatrics. 2020 Available from https://pediatrics.aappublications.org/content/early/2020/03/16/peds.2020-0702.1.
- Bialek S, Boundy E, Bowen V, et al. Severe outcomes among patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(12):343–346. doi:10.15585/mmwr.mm6912e232214079
- Jenco M. COVID-19 less severe in children than adults: study/American Academy of Pediatrics [Internet]. 2020 [cited Jul 27, 2020] Available from: https://www.aappublications.org/news/2020/03/16/coronavirus031620. Accessed 828, 2020.
- Novel CP. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2020;41(2):145–151.32064853
- Ludvigsson JF. Systematic Review of COVID-19 in Children Shows Milder Cases and a Better Prognosis Than Adults [Internet]. Vol. 109 Acta Paediatrica, International Journal of Paediatrics. Blackwell Publishing Ltd; 2020:1088–1095. Available from https://onlinelibrary.wiley.com/doi/full/10.1111/apa.15270.
- Zimmermann P, Curtis N. Coronavirus Infections in Children Including COVID-19: An Overview of the Epidemiology, Clinical Features, Diagnosis, Treatment and Prevention Options in Children [Internet]. Vol. 39 Pediatric Infectious Disease Journal. Lippincott Williams and Wilkins; 2020:355–368. Available from https://pubmed.ncbi.nlm.nih.gov/32310621/.
- Coronavirus. Human coronavirus types | CDC [internet]. [cited May 29, 2020] Available from: https://www.cdc.gov/coronavirus/types.html. Accessed 828, 2020.
- Chan JFW, To KKW, Tse H, Jin DY, Yuen KY. Interspecies transmission and emergence of novel viruses: lessons from bats and birds [internet]. Trends Microbiol. 2013;21:544–555. doi:10.1016/j.tim.2013.05.00523770275
- Chen Y, Liu Q, Guo D. Emerging coronaviruses: genome structure, replication, and pathogenesis. J Med Virol. 2020; 92(4):418–423. doi:10.1002/jmv.2568131967327
- Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa200101731978945
- Lai MMC, Cavanagh D. The Molecular Biology of Coronaviruses. Academic Press; 1997:1–100. Available from https://linkinghub.elsevier.com/retrieve/pii/S0065352708602869.
- He Y, Zhou Y, Liu S, et al. Receptor-binding domain of SARS-CoV spike protein induces highly potent neutralizing antibodies: implication for developing subunit vaccine. Biochem Biophys Res Commun. 2004;324(2):773–781. doi:10.1016/j.bbrc.2004.09.10615474494
- Letko M, Munster V. Functional assessment of cell entry and receptor usage for lineage B β-coronaviruses, including 2019-nCoV. Nat Microbiol. 2020.
- Hamming I, Timens W, Bulthuis MLC, Lely AT, Navis GJ, van Goor H. Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. J Pathol. 2004;203(2):631–637.15141377
- Bosch BJ, van der Zee R, de Haan CAM, Rottier PJM. The coronavirus spike protein is a class i virus fusion protein: structural and functional characterization of the fusion core complex. J Virol. 2003;77(16):8801–8811. doi:10.1128/JVI.77.16.8801-8811.200312885899
- Yan R, Zhang Y, Li Y, Xia L, Guo Y, Zhou Q. Structural basis for the recognition of SARS-CoV-2 by full-length human ACE2. Science (80-). 2020;367(6485):1444–1448. doi:10.1126/science.abb2762
- Zhou P, Lou YX, Wang XG, et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature. 2020;579(7798):270–273. doi:10.1038/s41586-020-2012-732015507
- de Wilde AH, Snijder EJ, Kikkert M, van Hemert MJ. Host factors in coronavirus replication In: Trip R,Tompkins S, editors. Roles of Host Gene and Non-coding RNA Expression in Virus Infection Current Topics in Microbiology and Immunology, vol 419. Cham: Springer. doi:10.1007/82_2017_25.
- Liu J, Wu P, Gao F, et al. Novel immunodominant peptide presentation strategy: a featured HLA-A*2402-restricted cytotoxic T-lymphocyte epitope stabilized by intrachain hydrogen bonds from severe acute respiratory syndrome coronavirus nucleocapsid protein. J Virol. 2010;84(22):11849–11857. doi:10.1128/JVI.01464-1020844028
- Cecere TE, Todd SM, LeRoith T. Regulatory T cells in arterivirus and coronavirus infections: do they protect against disease or enhance it? Viruses. 2012;4(5):833–846. doi:10.3390/v405083322754651
- Wu Z, Jama JM. 2020 undefined. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese. jamanetwork.com [Internet]. [cited Jul 30, 2020] Available from: https://jamanetwork.com/journals/jama/article-abstract/2762130. Accessed 828, 2020.
- U.S. State and Local Public Health Laboratories Reporting to CDC. CDC [internet]. [cited Jul 30, 2020] Available from: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/covidview/04102020/labs-regions.html. Accessed 828, 2020.
- Saheb Sharif-Askari N, Saheb Sharif-Askari F, Alabed M, et al. Airways expression of SARS-CoV-2 receptor, ACE2, and TMPRSS2 is lower in children than adults and increases with smoking and COPD. Mol Ther Methods Clin Dev. 2020;18:1–6. doi:10.1016/j.omtm.2020.05.01332537478
- Schouten LR, van Kaam AH, Kohse F, et al. Age-dependent differences in pulmonary host responses in ARDS: a prospective observational cohort study. Ann Intensive Care. 2019;9(1):55. doi:10.1186/s13613-019-0529-431089908
- Sidiq KR, Sabir DK, Ali SM, Kodzius R. Does early childhood vaccination protect against COVID-19? Front Mol Biosci. 2020;7:120. doi10.3389/fmolb.2020.0012032582766
- Dong Y, Mo X, Hu Y, et al. Epidemiology of COVID-19 among children in China. Pediatrics. 2020;145(6):e20200702. doi:10.1542/peds.2020-070232179660
- Center for Disease Control and Prevention. Symptoms of Coronavirus. CDC [internet]. 2020 [cited May 26, 2020] Available from: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fcoronavirus%2F2019-ncov%2Fabout%2Fsymptoms.html. Accessed 828, 2020.
- Du W, Yu J, Wang H, et al. Clinical characteristics of COVID-19 in children compared with adults in Shandong Province, China. Infection. 2020;1.
- Jin J-M, Bai P, He W, et al. Gender differences in patients with COVID-19: focus on severity and mortality [internet]. Front Public Health. 2020;8:152. doi:10.3389/fpubh.2020.0015232411652
- How COVID-19 Affects Children Compared to Adults [Internet]. [cited Jul 30, 2020] Available from: https://www.healthline.com/health-news/how-covid-19-affects-children-compared-to-adults. Accessed 828, 2020.
- Du W, Yu J, Wang H, et al. Clinical characteristics of COVID-19 in children compared with adults in Shandong Province, China. Infection. 2020;48(3):445–452. doi:10.1007/s15010-020-01427-232301099
- Hoang A, Chorath K, Moreira A, et al. COVID-19 in 7780 pediatric patients: a systematic review. EClinicalMedicine. 2020;24:100433. doi:10.1016/j.eclinm.2020.10043332766542
- Panahi L 1, Amiri M. 2 SP 3. clinical characteristics of COVID-19 infection in newborns and pediatrics: a systematic review - PubMed. Arch Acad Emerg Med. 2020;8(1). Available from https://pubmed.ncbi.nlm.nih.gov/32440661/.
- Feld L, Belfer J, Kabra R, et al. A case series of the 2019 novel Coronavirus (SARS-CoV-2) in 3 febrile infants in New York. Pediatrics. 2020;146(1):e20201056. doi:10.1542/peds.2020-105632404431
- Lu X, Zhang L, Du H, et al. SARS-CoV-2 infection in children [internet]. N Engl J Med. 2020;382(17):1663–1665. doi:10.1056/NEJMc200507332187458
- Garazzino S, Montagnani C, Donà D, et al. Multicentre Italian study of SARS-CoV-2 infection in children and adolescents, preliminary data as at 10 April 2020. Eurosurveillance. 2020;25(18):2000600. doi:10.2807/1560-7917.ES.2020.25.18.2000600
- Hong H, Wang Y, Chung HT, Chen CJ. Clinical characteristics of novel coronavirus disease 2019 (COVID-19) in newborns, infants and children. Pediatr Neonatol.2020;61:131–132. doi:10.1016/j.pedneo.2020.03.00132199864
- Chen N, Zhou M, Dong X, et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. Lancet. 2020;395(10223):507–513. doi:10.1016/S0140-6736(20)30211-732007143
- Prevention C for DC and. Interim guidelines for clinical specimens for COVID-19 | CDC. [Internet] 2020 [cited May 27, 2020] Available from: https://www.cdc.gov/coronavirus/2019-nCoV/lab/guidelines-clinical-specimens.html. Accessed 828, 2020.
- Bouadma L, Lescure FX, Lucet JC, Yazdanpanah Y, Timsit JF. Severe SARS-CoV-2 infections: practical considerations and management strategy for intensivists. Intensive Care Med. 2020;46(4):579–582. doi:10.1007/s00134-020-05967-x32103284
- Henry BM, Benoit SW, de Oliveira MHS, et al. Laboratory abnormalities in children with mild and severe coronavirus disease 2019 (COVID-19): a pooled analysis and review [internet]. Clin Biochem. 2020;81:1. doi:10.1016/j.clinbiochem.2020.05.01232473151
- Wu Q, Xing Y, Shi L, et al. Co-infection and other clinical characteristics of COVID-19 in children. Pediatrics. 2020;6:e20200961. doi:10.1542/peds.2020-0961
- Ma H, Hu J, Tian J, et al. A single-center, retrospective study of COVID-19 features in children: a descriptive investigation. BMC Med. 2020;18(1):123. doi:10.1186/s12916-020-01596-932370747
- Shen K, Yang Y, Wang T, et al. Diagnosis, treatment, and prevention of 2019 novel coronavirus infection in children: experts’ consensus statement [internet]. World J Pediatr. 2020;16:223–231. doi:10.1007/s12519-020-00343-732034659
- Chen ZM, Fu JF, Shu Q, et al. Diagnosis and treatm ent recommendations for pediatric respiratory infection caused by the 2019 novel coronavirus. World J Pediatr. 2020:1–7.32026149
- Qiu H, Wu J, Hong L, Luo Y, Song Q, Chen D. Clinical and epidemiological features of 36 children with coronavirus disease 2019 (COVID-19) in Zhejiang, China: an observational cohort study. Lancet Infect Dis. 2020;20(6):689–696. doi:10.1016/S1473-3099(20)30198-532220650
- Kids can develop severe complications from COVID-19 in rare cases. Science news [Internet]. [cited May 27, 2020] Available from: https://www.sciencenews.org/article/coronavirus-covid-19-kids-complications-inflammation-rare-cases. Accessed 828, 2020.
- COVID-19 in children: What’s behind the recent alerts about MIS-C? Boston children’s discoveries [internet]. [cited May 27, 2020] Available from: https://discoveries.childrenshospital.org/covid-19-complications-children/. Accessed 828, 2020.
- Children face risk for severe complications and death from COVID-19: Most of the children admitted to pediatric intensive care units had underlying conditions – ScienceDaily [Internet]. [cited May 27, 2020] Available from: https://www.sciencedaily.com/releases/2020/05/200511142153.htm. Accessed 828, 2020.
- Shekerdemian LS, Mahmood NR, Wolfe KK, et al. Characteristics and outcomes of children with Coronavirus Disease 2019 (COVID-19) infection admitted to us and Canadian pediatric intensive care units. JAMA Pediatr. 2020. doi:10.1001/jamapediatrics.2020.1948
- Mehta NS, Mytton OT, Mullins EWS, et al. SARS-CoV-2 (COVID-19): what do we know about children? A systematic review. Clin Infect Dis. 2020. doi:10.1093/cid/ciaa556
- Coronavirus Disease 2019 (COVID-19) Treatment Guidelines [Internet]. [cited May 30, 2020] Available from: https://www.covid19treatmentguidelines.nih.gov/. Accessed 828, 2020.
- Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). Treasure Island, FL: StatPearls Publishing; 2020.