
Abstract
Purpose
To explore patterns in the purchase of prescription and over-the-counter (OTC) oral antihistamines (OAHs) and intranasal corticosteroids (INCSs) by patients, from pharmacies in different geographical regions of Australia.
Patients and methods
Retrospective observational study using a database containing anonymous pharmacy transaction data from 20.0% of the pharmacies in Australia that link doctor prescriptions and OTC information. Pharmacy purchases of at least one prescription or OTC rhinitis treatment during 2013 and 2014 were assessed.
Results
In total, 4,247,193 prescription and OTC rhinitis treatments were purchased from 909 pharmacies over 12 months. Of treatments purchased, 75.9% were OAHs and 16.6% were INCSs. OTC purchases of both treatments exceeded purchases through prescription. OTC OAHs purchasing patterns were seasonal and almost identical in the Australian Capital Territory, Victoria, Western Australia, South Australia, and New South Wales, and similar seasonal patterns for OTC INCSs were noted in most regions except for South Australia and Tasmania. Prescription purchasing patterns of both OAHs and INCSs remained unchanged throughout the year in most regions.
Conclusion
This large-scale retrospective observational study identified seasonal purchasing patterns of OTC and prescription OAHs and INCSs in a real-world setting. It highlighted that seasonality only affects OTC purchasing patterns of OAHs and INCSs across Australia and that practitioner prescribing remains unchanged, suggesting that it is only for persistent disease.
Introduction
Rhinitis is an umbrella term that encompasses a collection of disorders of the nose resulting from inflammation and/or dysfunction of the nasal mucosa. It is characterized by one or more of the following nasal symptoms: anterior or posterior rhinorrhea, sneezing, nasal congestion, and/or itching.Citation1 Rhinitis is classified as allergic rhinitis (AR) or non-allergic rhinitis (NAR), but some types of rhinitis can have both AR and NAR components (known as “mixed rhinitis” [MR]).Citation2 Regardless of the type of rhinitis, untreated or uncontrolled symptoms can have a significant negative impact on patient’s quality of life, including impairments in work productivity, school performance, social interactions, and sleep.Citation3,Citation4 Rhinitis is a significant cause of morbidity and poses a substantial economic and health burden to individuals and society.Citation5,Citation6
AR is the most prevalent form of rhinitis affecting 10%–40% of the global population and its prevalence is increasing in children and adults.Citation3,Citation5 In Australia, AR affects 17% of the population and is predicted to increase in prevalence by 70% in the next 35 years.Citation7 In 2007–2008, AR rates were the highest in Australian Capital Territory (ACT), Western Australia (WA), Victoria (VIC), and South Australia (SA). New South Wales (NSW) and Queensland (QLD) had rates significantly lower than the overall rate for Australia.Citation8 In contrast, estimates of the prevalence of NAR and MR in Australia have yet to be determined. International studies have reported that the ratio of AR to pure NAR is 3:1,Citation9 and data suggest that 44%–87% of patients with AR may have MR.Citation10,Citation11
Traditionally, AR was classified based on the timing of allergen exposure into either seasonal (relating to AR caused by outdoor allergens, such as pollens and molds) or perennial (relating to AR caused by indoor allergens, such as house dust mites, molds, and animal dander). A revised system, proposed in the 2001 Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines, classifies AR into either intermittent or persistent according to the duration of symptoms, and either mild or moderate-to-severe based on the severity of symptoms and their impact on quality of life.Citation12 The ARIA system is appropriate for use in Australia, as in certain regions of Australia: 1) pollens and molds may be perennial allergens; 2) even patients allergic to “seasonal” allergens may have symptoms for most of the year as the pollen season can be difficult to define, particularly in QLD; and 3) most patients are sensitized to multiple allergens and thus symptoms may be present throughout the year.Citation13
In Australia, the most troublesome pollens tend to be airborne pollens produced by Northern Hemisphere grasses, trees, and flowering weed species. Grass pollens from temperate grasses, such as perennial ryegrass, timothy, and subtropical grasses including Bermuda (couch) and Bahia are clinically important seasonal allergens that can trigger AR in some individuals.Citation14,Citation15 Small wind-distributed pollens from trees (including cypress, silver birch, English oak, and Murray pine) and weeds (including ragweed, parthenium weed, pellitory weed, and Paterson’s curse) are more likely to trigger AR. Owing to geographical variability in climate, subtropical grasses have different pollination seasons across Australia. Moreover, VIC has higher peak pollen counts than many other regions of Australia because of the impact of springtime northerly winds that carry pollen from grasslands north of its border.Citation16
The goal of AR management is to achieve optimal symptom control so as to prevent complications and disease progression.Citation6,Citation17 Achieving this goal depends on identifying the triggers and assessing the nature and severity of symptoms. For AR, management strategies include reducing allergen exposure, pharmacotherapy, and immunotherapy.Citation17 ARIA guidelines recommend that pharmacological treatment should consider the severity and duration of the disease, the patient’s preference, and the efficacy, safety, availability, and costs of medications.Citation17 Recommended therapies include intranasal corticosteroids (INCSs), second-generation oral antihistamines (OAHs), oral leukotriene receptor antagonists (LTRAs), and intranasal antihistamines.Citation17,Citation18
All guidelines agree that INCSs are the most effective monotherapy for AR.Citation6,Citation17–Citation19 INCSs are key to the management of moderate-to-severe AR. They have some efficacy on ocular symptomsCitation20 and have been shown to be superior to either OAHs or LTRAs.Citation21,Citation22 The newer INCSs have similar efficacy with excellent safety and tolerability profiles;Citation23 however, several days’ use may be needed to reach maximum response.Citation24 Second-generation OAHs are recommended for mild intermittent AR and have minimal adverse effects.Citation25 Until recently, INCSs were regarded as the most effective treatment option for AR. A new intranasal formulation of a corticosteroid and an antihistamine combined in a single intranasal device has been shown to provide added efficacy and for some patients, that is substantial.Citation26 Of more importance is the convenience factor for patients who use both intranasal antihistamines and INCSs. Although the addition of an OAH to an INCS has been investigated, no additional efficacy above that achieved by INCS monotherapy was demonstrated,Citation27 with most published data confirming no clinical benefits gained by adding oral therapy to intranasal therapy.Citation17
The Allergic Rhinitis in Australia report published in 2011,Citation8 which used pharmaceutical wholesale supply information, found that the wholesale cost to community pharmacies of INCSs and OAHs had almost doubled in the previous 10 years. In 2001, the total wholesale cost of these medications was $107.8 million and in 2010 it was $226.8 million. It was reported that this trend had strengthened over the 10-year period owing largely to increasing availability of over-the-counter (OTC) OAHs. The majority of OAH products available in Australia in 2010 (125 out of 147) had OTC status, making 9 out of 10 OAH products obtainable without consulting a pharmacist or medical practitioner. Of the 12 INCS products available in 2010, 5 had OTC status and 7 had either pharmacist-only (Schedule 3) or prescription-only (Schedule 4) status. Each year monthly wholesale supplies of OAHs started to increase around July and peaked around October to November and monthly wholesale supplies of INCSs started to increase in August, peaking around November.
AR is one of the most underestimated respiratory conditions, by physicians and patients. Its management is frequently complicated by delayed diagnosis and proper treatment because of attempts by patients to self-medicate with a wide range of OTC medications available from pharmacies without the need for doctors’ prescription.Citation13 In Australia, apart from reported patterns and costs of wholesale supplies of rhinitis treatments to pharmacies,Citation8 little is known about the nature or extent of rhinitis treatment purchases from pharmacies, in light of the increasing size of the OTC medicine market and number of people with rhinitis who choose to self-medicate. This study aimed to explore patterns in the purchases of prescription and OTC OAHs and INCSs from pharmacies in different geographical regions of Australia.
Materials and methods
This was a retrospective observational study of a historical cohort conducted with data from a database collected during 2013 and 2014. The study was registered with the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (registration number ENCEPP/SDPP/8507) and approved by the Anonymised Data Ethics Protocols and Transparency (ADEPT) committee (approval reference number ADEPT0215).
Data source
NostraData (https://www.nostradata.com.au/Public/Home/About) provided a suitable dataset of anonymous pharmacy transaction data available from 20% of pharmacies in Australia that links doctor prescriptions and OTC information. Data within this dataset describe the details of valid transactions completed at the pharmacy including name(s) of product(s) purchased, prescription or OTC status, postcode of purchase, and price paid. As the dataset does not contain patient demographic information or longitudinal data, it is, therefore, not possible to track individual patient purchases at different NostraData pharmacies or on different occasions.
From the pharmacy claims dataset, we assessed pharmacy purchases of at least one prescription or OTC rhinitis treatment (used as a proxy for a diagnosis of rhinitis) during 2013 and 2014. Categories of rhinitis treatments included OAHs, INCSs, intranasal antihistamine and corticosteroid combinations, non-steroidal nasal sprays, LTRAs, eye drops for allergic conjunctivitis, oral corticosteroids, and injectable corticosteroids. A list of drugs included in each therapeutic class and the most representative in terms of prescription and OTC purchases is presented in . As LTRAs alone are likely to be purchased for asthma treatment rather than rhinitis, and individual patients could not be tracked in this dataset, LTRAs were only included as rhinitis therapy for pharmacy transactions without additional asthma/chronic obstructive pulmonary disease treatment. Categories of asthma/chronic obstructive pulmonary disease treatments included short-acting beta2 agonists, inhaled corticosteroids, long-acting beta2 agonists, inhaled corticosteroid/long-acting beta2 agonist combination therapy, short-acting muscarinic antagonists, long-acting muscarinic antagonists, chromones, and theophylline. Patient purchases of oral and systemic corticosteroids (without other rhinitis therapy) were excluded.
Table 1 List of drugs included in each therapeutic class
Data analysis
Data were analyzed using MySQL and Microsoft Excel 2011 software. Descriptive statistics were used to summarize sample characteristics and pharmacy transactions involving purchases of prescription and OTC OAHs and/or INCSs specifically. All pharmacy purchases during the study period were analyzed together and reported as average numbers and percentages per month for each of the following geographical regions: NSW, ACT, QLD, VIC, SA, WA, Tasmania (TAS), and Northern Territory (NT).
Results
Pharmacy transaction data collected from 909 pharmacies during 2013 and 2014 were assessed. Sample characteristics of pharmacy transactions in different geographical regions over 12 months are shown in . Of the 8,334,472 pharmacy transactions assessed, 4,247,193 (51.0%) included rhinitis therapy. Prescription and OTC purchases of OAHs and INCSs in different geographic regions over 12 months are shown in . Of the 4,247,193 prescription and OTC rhinitis treatments purchased over 12 months, 3,222,798 (75.9%) were OAHs and 704,038 (16.6%) were INCSs (). The highest rates of prescription and OTC OAH purchases (in descending order) were in NSW, VIC, and QLD, whereas the highest rates of prescription and OTC INCS purchases were in NSW, VIC, and WA over the 12 months.
Table 2 Sample characteristics of pharmacy transactions in different geographical regions of Australia over 12 months
Table 3 Pharmacy transactions of oral antihistamine and intranasal corticosteroid therapy in different geographical regions of Australia over 12 months
Seasonality in purchasing patterns in different geographical regions
OTC OAHs
Of the 3,222,798 OAHs purchased over 12 months, 2,995,056 (92.9%) were OTC purchases. Seasonal patterns in pharmacy purchases of OTC OAHs in each geographical region are shown in . Almost identical seasonal patterns in purchases were noted in ACT, VIC, WA, SA, and NSW, remaining high from September to November and peaking in October. The highest peak in purchases occurred in the ACT, followed by VIC and WA ().
Figure 1 (A) Seasonal patterns of OTC oral antihistamine purchases in different geographical regions (N=2,995,056). (B) Seasonal patterns of OTC intranasal corticosteroid purchases in different geographical regions (N=456,639).
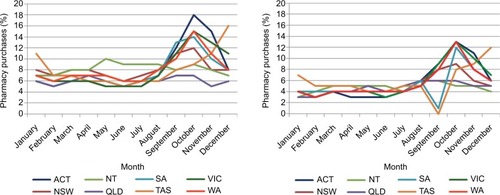
OTC INCSs
Of the 704,038 INCSs purchased over 12 months, 456,639 (64.9%) were OTC purchases. Seasonal patterns in pharmacy purchases of OTC INCSs in each geographical region are shown in . Seasonal patterns in purchases were similar in most regions remaining high from September to November and peaking in October. However, in SA and TAS, purchasing patterns differed from other regions, with purchases dipping in September and peaking in October in SA, and peaking in December in TAS ().
Prescription OAHs
Of the 3,222,798 OAHs purchased over 12 months, 227,742 (7.1%) were prescription purchases. Seasonal patterns in pharmacy purchases of prescription OAHs in each geographical region are shown in . With the exception of SA, rates of pharmacy purchases of prescription OAHs were low and stable in most regions throughout the 12 months, with a higher rate of purchases in QLD.
Figure 2 (A) Seasonal patterns of prescription oral antihistamine purchases in different geographical regions (N=267,742). (B) Seasonal patterns of prescription intranasal corticosteroid purchases in different geographical regions (N=247,399).
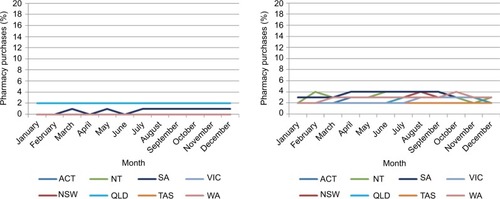
Prescription INCSs
Of the 704,038 INCSs purchased over 12 months, 247,399 (35.1%) were prescription purchases. Seasonal patterns in pharmacy purchases of prescription INCSs in each geographical region are shown in . In most regions, patterns in purchases of prescription INCSs, generally, remained stable throughout the 12 months.
Seasonality of purchasing patterns across Australia
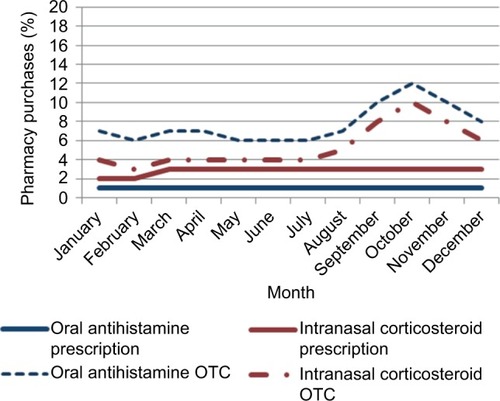
Seasonal patterns in pharmacy purchases of prescription and OTC OAHs and INCSs across Australia are shown in . Seasonal purchasing patterns across Australia of prescription INCS and OAHs were similar and remained stable throughout the 12 months, but differed from those of OTC INCSs and OAHs, remaining high from September to December, and peaking in October ().
Figure 3 Seasonal purchasing patterns of oral antihistamines (N=3,222,798) and intranasal corticosteroids (N=704,038) across Australia.
Discussion
This study is the first to provide a unique “snapshot” of seasonal patterns in purchases of OAHs and INCSs from community pharmacies in different geographical regions of Australia, using prescription and OTC information. It provides valid pharmacy transaction data on rhinitis treatment purchases for patients in a real-world setting. Of the OTC and prescription treatments purchased, 75.9% were OAHs, and 16.6% were INCSs. The highest rates of prescription and OTC OAH purchases (in descending order) were in NSW, VIC, and QLD, whereas the highest rates of prescription and OTC INCS purchases were in NSW, VIC, and WA over the 12 months. OTC purchases of both treatments exceeded purchases through prescription. Similarities and differences were identified in seasonal purchasing patterns of prescription and OTC treatments across various regions. The seasonality of purchasing patterns across Australia of both OTC OAHs and INCSs indicates that most instances of seasonal disease are managed by OTC treatments while the stable purchasing patterns of prescription OAHs and INCSs represent unchanged prescribing behavior for those with persistent disease.
Few published studies have explored patterns of rhinitis treatment purchases from community pharmacies using prescription and OTC information. Research in this area has primarily focused on examining wholesaler supply patterns of rhinitis therapy,Citation8 investigating demographics and medication use, and evaluating clinical and humanistic outcomes of individuals suffering with symptoms of rhinitis who visit the pharmacy, using self-report questionnaire-based surveys without validation of the accuracy of the recording of symptoms and treatments.Citation28–Citation31 Therefore, exploring patterns in pharmacy purchases of OAHs and INCSs using valid prescription and OTC information was considered important, given the increasing size of the OTC medicine market, the number of people with rhinitis who choose to self-medicate, the quality use of medicines in achieving optimal patient outcomes, and the paucity of data about OTC and prescription treatment purchases for rhinitis symptoms in the primary care setting.
This study showed that 75.9% of purchased treatments were OAHs and 16.6% were INCSs. Our results are consistent with those from a 2001 longitudinal community pharmacy-based study in the UK, which found that of the patient reported treatments obtained for AR symptoms, over 70% were OAHs and 14% were INCSs.Citation31 Williams and Scadding reported similar findings upon survey completion of a random sample of French, German, and UK population.Citation32 The Allergic Rhinitis in Australia report also found that three times as many OAHs than INCSs were supplied to pharmacies in 2010.Citation8
This study also showed that 92.9% of OAHs purchases were OTC purchases. OAHs are recommended for mild intermittent AR symptoms, and are effective in relieving sneezing, itching, and rhinorrhea, yet often fail to relieve nasal congestion, which is often the most troublesome symptom.Citation6,Citation17,Citation19 In NAR, second-generation OAHs are of no benefit as histamine release has not been seen in NAR.Citation2 Furthermore, AR can sometimes copresent in association with other types of rhinitis (MR) leading to increased severity requiring INCS treatment.Citation6,Citation19 It is, therefore, likely that a proportion of OTC OAH purchases may not be appropriate first-line treatment according to ARIA guidelines. This not only puts the person with rhinitis at risk of future adverse outcomes due to sub-optimal disease management, but also places the pharmacist at a risk of failure to identify sub optimal treatment and intervene appropriately.
In Australia, although the majority of second-generation OAHs are available OTC (Schedule 2), first-generation sedating OAHs have Schedule 3 status (Pharmacist Only Medicine), requiring pharmacist counseling and advice. Although it is not possible to determine whether patients self-selected OAHs with or without seeking pharmacist advice prior to purchasing them in this study, these findings have wide implications for pharmacy. Over 60% of rhinitis patients are known to self-medicate, often with inappropriate medication, leading to poorly controlled symptoms and sub optimal management.Citation30,Citation31 Moreover, many people who initially present during the pollen season can still have symptoms 6 months later, suggesting that much AR that appears initially to be intermittent is in fact persistent in nature.Citation31 Our study results support the need for new tools and strategies for primary health care providers, which take into account patients’ perception of symptoms and the effect of ongoing treatment. These tools and strategies should aim at facilitating the application of clinical guidelines in practice and quality use of medicines so that rhinitis can be better managed in the primary care setting.
In our study, a greater number of prescription and OTC OAHs were purchased in NSW, VIC, and QLD compared with other regions over 12 months. A possible explanation for this finding is that a greater number of NostraData pharmacies were located in these regions, and hence were able to capture a greater proportion of purchases of OAHs, which represent the most commonly used treatment for AR.Citation17,Citation19 Furthermore, OTC OAH and INCS purchases were found to exceed those of prescription OAHs and INCSs. This is not surprising, since most OAHs and INCSs on the market for the management of rhinitis are now available from Australian pharmacies, without the need for doctor’s prescription.
This study also explored seasonal patterns in purchases of OAHs and INCSs in different geographical areas of Australia. Seasonal patterns in prescription purchases of both treatments were similar and stable in most regions, indicating that pre-scribing patterns were unaffected by geographical variability in climate and pollination seasons, but were influenced by treatment requirements for persistent symptoms throughout the year. In contrast, the similar and fluctuating seasonal purchasing patterns of OTC OAHs in the ACT, VIC, WA, SA, and NSW indicate these regions share common clinically relevant seasonal aeroallergens despite geographical variability in climate and temperature. Seasonal purchasing patterns of OTC INCSs were similar in most regions, with patterns differing in the southern states of SA and TAS from August to December. This finding could be explained by the fact that, during the time of the study, these states may have experienced a longer winter resulting in a delayed pollination season and/or that they may have undergone weather changes in temperature and humidity, thus triggering nasal symptoms in patients with NAR or MR. As global temperatures increase, it is anticipated that allergen seasons may become longer and subtropical grasses and weeds will become more important allergens in regions with temperate climates.Citation15
A key contribution of our study has been the identification of seasonal pharmacy purchasing patterns across Australia of both prescription and OTC OAHs and INCSs. The seasonality in pharmacy purchasing pattern of OTC OAHs appears to be consistent with the seasonality in pharmaceutical whole-sale supply pattern of OAHsCitation8 and with the ARIA guidelines for the treatment of mild intermittent (seasonal) AR.Citation18 The overall seasonal pattern and peak in pharmacy purchases of OTC INCSs seems to mimic that of OTC OAHs, suggesting that INCSs are being appropriately used for the treatment of moderate-to-severe intermittent (seasonal) AR based on the latest AR guidelines.Citation18 It is well recognized that AR is often regarded by patients as a background noise, a nuisance, and a trivial disease as it is not life-threatening. For those reasons, AR is frequently self-managed by patients with OTC treatments from community pharmacies, and the pharmacist, therefore, represents the first-point of contact for advice on appropriate medication.Citation33–Citation36 A population survey in 2010 found that 63% of Australian patients with AR visited a pharmacist for advice on AR treatment.Citation37 The purchasing pattern of prescription INCSs, however, appears to be unaffected by seasonal changes and represents ongoing treatment requirements for those with moderate-to-severe persistent rhinitis.Citation17 Studies have shown that most patients who visit a doctor for their AR have moderate-severe persistent disease,Citation38 with most patients first visiting their doctor when AR symptoms become “intolerable”.Citation34 Similarly, the stable purchasing pattern of prescription OAHs is unaffected by seasonal changes and represents unchanged prescribing behavior for those with persistent disease.
Strengths and limitations of this study
This large dataset included pharmacy transaction data from 909 Australian community pharmacies and information on 4,247,193 rhinitis treatments for “real-life” patients with or without additional respiratory disease in 2013 and 2014. Data related to rhinitis therapy underwent rigorous quality assurance procedures prior to statistical analyses. As the dataset used prescription and OTC information, rather than patient-reported outcomes, it provided a unique insight into prescribing and self-medication behavior, and the significant burden posed on community pharmacy to address the needs of people with rhinitis symptoms. The sample of pharmacy transactions involving OAH and INCS treatments is representative of the Australian population as a whole, based on the latest published data of pharmaceutical wholesale supply of OAHs and INCSs to community pharmacies.Citation8 Finally, another strength of the study is its observational nature, which allowed a “snapshot” of the current state of rhinitis treatment purchases via prescription and OTC supply in Australia. This approach provides insight into prescriber behavior and patient purchasing behavior that would have be difficult to obtain through other approaches, such as surveys, which can misrepresent patient and prescriber behavior.
The limitations of the study were associated with the cross-sectional design, variation in the number of pharmacies in each geographical region and lack of patient demographic data. In addition, we used prescription and OTC purchases of rhinitis therapy as a proxy for a rhinitis diagnosis. Although there is a possibility that prescription and OTC purchases of treatment classified as rhinitis therapy could be used for another indication, the marked seasonality in pharmacy purchases of OTC INCS and OAH treatments observed in our study provides evidence to support the use of rhinitis therapy as a proxy for a diagnosis of intermittent (seasonal) AR. Furthermore, in this study it was not possible to check whether therapies purchased together in the dataset were all destined to the same patient nor was it possible to document purchases or rhinitis therapy from pharmacies outside NostraData coverage.
Conclusion
This large-scale retrospective observational study identified seasonal purchasing patterns of OTC and prescription OAHs and INCSs in a real-world setting across Australia. It highlighted that seasonality only affects OTC purchasing patterns of OAHs and INCSs, confirming that spring is the worst time for nasal allergies and that practitioner prescribing remains unchanged, suggesting that it is only for those with persistent (perennial) disease.
Acknowledgments
The abstract of this paper was presented at the Respiratory Effectiveness Group 2016 Annual Summit as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in The Journal of Thoracic Disease (Vol. 8, Supplement 5, 5 July 2016). http://jtd.ame-groups.com/article/view/8504.
Disclosure
A Simon Carney is a consultant for Olympus and Smith and Nephew and has received honoraria from MEDA Pharmaceuticals. David B Price has board membership with Aerocrine, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, Meda, Mundipharma, Napp, Novartis, and Teva Pharmaceuticals; consultancy agreements with Almirall, Amgen, AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Meda, Mundipharma, Napp, Novartis, Pfizer, Teva Pharmaceuticals, and Theravance; grants and unrestricted funding for investigator-initiated studies (conducted through Observational and Pragmatic Research Institute Pte Ltd) from UK National Health Service, British Lung Foundation, Aerocrine, AKL Research and Development Ltd, AstraZeneca, Boehringer Ingelheim, Chiesi, Meda, Mundipharma, Napp, Novartis, Pfizer, Respiratory Effectiveness Group, Takeda, Teva Pharmaceuticals, Zentiva, and Theravance; payment for lectures/speaking engagements from Almirall, AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Meda, Merck, Mundipharma, Novartis, Pfizer, Skyepharma, Takeda, and Teva Pharmaceuticals; payment for manuscript preparation from Mundipharma and Teva Pharmaceuticals; payment for the development of educational materials from Novartis and Mundipharma; payment for travel/accommodation/meeting expenses from Aerocrine, Boehringer Ingelheim, Mundipharma, Napp, Novartis, Teva Pharmaceuticals, and AstraZeneca; funding for patient enrolment or completion of research from Chiesi, Teva Pharmaceuticals, Zentiva, and Novartis; stock/stock options from AKL Research and Development Ltd, which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd, UK, and 74% of Observational and Pragmatic Research Institute Pte Ltd, Singapore; and is peer reviewer for grant committees of the Medical Research Council, Efficacy and Mechanism Evaluation programme, and Health Technology Assessment. Pete Smith has received honoraria from AstraZeneca, GlaxoSmithKline, MEDA Pharmaceuticals, and Mundipharma. Richard Harvey is a consultant for Medtronic, Neilmed, and Olympus, he has received honoraria from Sequiris and grant support from MEDA Pharmaceuticals, Neilmed and Stallergenes.
Vicky Kritikos has received honoraria from AstraZeneca, GlaxoSmithKline, and Pfizer.
Sinthia Bosnic-Anticevich has received honoraria from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Mundipharma, and TEVA Pharmaceuticals for her contribution to advisory boards/key international expert forum. Alice Durieux was an employee of Observational and Pragmatic Research Institute, which has conducted paid research in respiratory disease on behalf of UK National Health Service, British Lung Foundation, Aerocrine, AKL Research and Development Ltd, AstraZeneca, Boehringer Ingelheim, Chiesi, MEDA Pharmaceuticals, Mundipharma, Napp, Novartis, Pfizer, Respiratory Effectiveness Group, Takeda, TEVA Pharmaceuticals, Theravance, and Zentiva. The other authors report no conflicts of interest in this work.
References
- SettipaneRAKalinerMANonallergic rhinitisAm J Rhinol Allergy201327Suppl 1485123406601
- ScarupaMDKalinerMANonallergic rhinitis, with a focus on vasomotor rhinitisWorld Allergy Organ J200923202523282951
- NathanRAThe burden of allergic rhinitisAllergy Asthma Proc20072813917390749
- MelzerEOFarrarJRSennettCFindings from an online survey assessing the burden and management of seasonal allergic rhinoconjunctivitis in US patientsJ Allergy Clin Immunol Pract201753779789.e627914815
- MeltzerEOBuksteinDAThe economic impact of allergic rhinitis and current guidelines for treatmentAnn Allergy Asthma Immunol2011106Supp 21216
- SeidmanMDSchwartzSRBonnerJRClinical practice guideline: allergic rhinitisOtolaryngol Head Neck Surg20151521SS1S43
- Australian Institute of Health and WelfareAustralia’s health 20142014 Available from: http://www.aihw.gov.au/publication-detail/?id=60129547205Accessed November, 2016
- Australian Institute of Health and WelfareAllergic rhinitis (‘hay fever’) in Australia2011 Available from: http://www.aihw.gov.au/publication-detail/?id=10737420595Accessed November, 2016
- SettipaneRARhinitis: a dose of epidemiological realityAllergy Asthma Proc200324314715412866316
- SettipaneRACharnockDREpidemiology of rhinitis: allergic and nonallergicClin Allergy Immunol200719233417153005
- SettipaneRADemographics and epidemiology of allergic and nonallergic rhinitisAllergy Asthma Proc200122418518911552666
- BousquetJVan CauwenbergePKhaltaevNAllergic rhinitis and its impact on asthmaJ Allergy Clin Immunol20011085 SupplS147S33411707753
- WallsRSHeddleRJTangMLKBasgerBJSolleyGOYeoGTOptimising the management of allergic rhinitis: an Australian perspectiveMed J Aust20051821283315651945
- DaviesJMGrass pollen allergens globally: the contribution of subtropical grasses to burden of allergic respiratory diseasesClin Exp Allergy201444679080124684550
- BeggsPJAdaptation to impacts of climate change on aeroallergens and allergic respiratory diseasesInt J Environ Res Public Health2010783006302120948943
- Australian Society of Clinical Immunology and Allergy: Pollen allergy2015 Available from: http://www.allergy.org.auAccessed November, 2016
- BousquetJKhaltaevNCruzAAAllergic rhinitis and its impact on asthma (ARIA) 2008 update (in collaboration with the World Health Organization, GA(2)LEN and AllerGen)Allergy200863Supp 86816018331513
- BrozekJLBousquetJBaena-CagnaniCEAllergic rhinitis and its impact on asthma (ARIA) guidelines: 2010 revisionJ Allergy Clin Immunol2010126346647620816182
- ScaddingGKDurhamSRMirakianRBSACI guidelines for the management of allergic and non-allergic rhinitisClin Exp Allergy2008381194218081563
- BieloryLChunYBieloryBPCanonicaGWImpact of mometasone furoate nasal spray on individual ocular symptoms of allergic rhinitis: a meta-analysisAllergy201166568669521261661
- WeinerJMAbramsonMJPuyRMIntranasal corticosteroids versus oral H1 receptor antagonists in allergic rhinitis: systematic review of randomised controlled trialsBMJ19983177173162416299848901
- RatnerPHHowlandWCIIIArastuRFluticasone propionate aqueous nasal spray provided significantly greater improvement in daytime and nightime nasal symptoms of seasonal allergic rhinitis compared with montelukastAnn Allergy Asthma Immunol200390553654212775135
- NeilsenLPMygindNDahlRIntranasal corticosteroids for allergic rhinitis: superior relief?Drugs200161111563157911577794
- KlimekLMullolJHellingsPGevaertPMösgesRFokkensWRecent pharmacological developments in the treatment of perennial and persistent allergic rhinitisExp Opin Pharmacother2016175657669
- SimonsFESimonsKJHistamine and H1-antihistamines:celebrating a century of progressJ Allergy Clin Immunol201112861139115022035879
- MeltzerEOWallaceDDykewiczMShneyerLMinimal clinically important difference (MCID) in allergic rhinitis: agency for healthcare research and quality or anchor-based thresholds?J Allergy Clin Immunol Pract20164468268827084419
- BenningerMFarrarJRBlaissMEvaluating approved medications to treat allergic rhinitis in the United States: an evidence-based review of efficacy for nasal symptom classAnn Allergy Asthma Immunol20101041132920143641
- LombardiCMusiccoERastrelliFBettoncelliGPassalacquaGCanonicaGWThe patient with rhinitis in the pharmacy. A cross-sectional study in real lifeAsthma Res Pract201511627965756
- LourencoOCaladoSSa-SousaAFonsecaJEvaluation of allergic rhinitis and asthma control in a Portuguese community pharmacy settingJ Mang Care Pharm2014205513522
- MehuysEGevaertPBrusselleGSelf-medication in persistent rhinitis: overuse of decongestants in half of the patientsJ Allergy Clin Immunol Pract2014231331924811023
- SinclairHBondCLargueGPriceDHannafordPCommunity pharmacy provision of allergic rhinitis treatments: a longitudinal study of patient reported outcomeInt J Pharm Pract200513249256
- WilliamsAScaddingGIs reliance on self-medication and pharmacy care adequate for rhinitis patients?Int J Clin Pract20096319810419125997
- DemolyPAllaertFALecasbleMERASM, a pharmacoepidemiologic survey on management of intermittent allergic rhinitis in every day general practice in FranceAllergy20025754655412028122
- MaurerMZuberbierTUndertreatment of rhinitis symptoms in Europe: findings from a cross-sectional questionnaire surveyAllergy20076291057106317581263
- FromerLMOrtizGRyanSFStoloffSWInsights on allergic rhinitis from the patient perspectiveJ Fam Pract2012612 SupplS16S22
- StormsWMeltzerEONathanRASelnerJCAllergic rhinitis: the patient’s perspectiveJ Allergy Clin Immunol1997996S825S828
- KatelarisCHLaiCKRheeCNasal allergies in the Asia-Pacific population: results from the Allergies in Asia-Pacific surveyAm J Rhinol Allergy201125Suppl 1S3S1522185687
- DemolyPBousquetPJMesbahKBousquetJDevillierPVisual analogue scale in patients treated for allergic rhinitis: an observational prospective study in primary care: asthma and rhinitisClin Exp Allergy201343888188823889242