
Abstract
Background
We sought to determine whether catheter ablation of atrial fibrillation (AF) is associated with reduced occurrence of ischemic cerebrovascular events.
Methods and results
Using routinely collected hospital data, ablation patients were matched to two control cohorts via direct and propensity score matching. A total of 4,991 ablation patients were matched 1:1 to general AF controls with no ablation, and 5,407 ablation patients were similarly matched to controls who underwent cardioversion. Yearly rates of ischemic stroke or transient ischemic attack (stroke/TIA) before and after an index date were compared between cohorts. Index date was defined as the first ablation, the first cardioversion, or the second AF event in the general AF cohort. Matched populations had very similar demographic and comorbidity profiles, including nearly identical CHA2DS2-VASc risk distribution (p-values 0.6948 and 0.8152 vs general AF and cardioversion cohorts). Statistical models of stroke/TIA risk in the preindex period showed no difference in annual event rates between cohorts (mean±standard error 0.30% ± 0.08% ablation vs 0.28% ± 0.07% general AF, p=0.8292; 0.37% ± 0.09% ablation vs 0.42% ± 0.08% cardioversion, p=0.5198). Postindex models showed significantly lower annual rates of stroke/TIA in ablation patients compared with each control group over 5 years (0.64% ± 0.11% ablation vs 1.84% ± 0.23% general AF, p<0.0001; 0.82% ± 0.15% ablation vs 1.37% ± 0.18% cardioversion, p=0.0222).
Conclusion
Matching resulted in cohorts having the same baseline risks and rates of ischemic cerebrovascular events. After the index date, there were significantly lower yearly event rates in the ablation cohort. These results suggest the divergence in outcome rates stems from variance in the treatment pathways beginning at the index date.
Introduction
Stroke is the second most common cause of death worldwide,Citation1 and its risk is increased five times with atrial fibrillation (AF).Citation2 While catheter ablation reduces the burden of AF compared with drug therapy,Citation3,Citation4 it is not known whether this results in reduced stroke risk.Citation5 Large randomized trials on this subject – Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial and Early Treatment of Atrial Fibrillation for Stroke Prevention Trial – will not report for several years. Several retrospective cohort design studies have addressed the same question but are limited by potential confounding due to unmeasured risks.Citation6–Citation10
We sought to overcome this key limitation by examining trends over time within the same populations. Using routinely collected data, we examined rates of ischemic stroke or transient ischemic attack (stroke/TIA) in patients undergoing ablation and two matched control cohorts with AF, one having undergone direct current cardioversion. Comparing stroke/TIA rates across cohorts and over time, we hypothesized that there would be a difference in temporal trends after the intervention date.
Methods
Data source
The data source for this study was an anonymized dataset of predefined variables created from the Hospital Episode Statistics (HES) data warehouse, including records from 1996 to 2013. HES contains details of all hospital admissions, outpatient appointments, and accident and emergency attendances at National Health Service hospitals in England. HES records include clinical diagnoses and procedures; patient demographics; and administrative information from inpatient visits since 1989, outpatient visits since 2003, and accident and emergency visits since 2007. The records used for this study included all patients with a diagnosis of AF International Classification of Diseases, tenth edition (ICD-10 code I48) recorded at any time prior to the end of 2013.
Patient selection
Patients included in the analysis population for this study were required to have at least one AF diagnosis (ICD-10 code I48) during or after 2008 to ensure capture of contemporary treatments. Patients with a record of AF prior to April 2005 were excluded to eliminate patients known to have very long-standing AF. In addition, patients were excluded for diagnoses or procedures denoting evidence of valvular heart disease, atrioventricular node ablation, pacemaker, implantable cardioverter defibrillator, or any operation on the heart conduction system at or prior to the cohort-specific index date (Table S1).
Cohort selection
From the selected patients, a pulmonary vein ablation (PVA) treatment cohort was defined as those patients who had an AF ablation incorporating percutaneous transluminal pulmonary vein isolation (ICD-10 procedure code K621) as their primary procedure, simultaneously with a primary AF diagnosis. Exclusions for this cohort included any additional catheter or surgical ablation of the heart prior to the index PVA (Table S1). A general AF control cohort was defined as those patients with at least two hospital records and no catheter or surgical ablation of the heart at any time. Additionally, a cardioversion control cohort was defined as the subset of the general AF control cohort with a record of direct current cardioversion (ICD-10 procedure code X501 or X502) simultaneously with a primary AF diagnosis.
Baseline definitions and data conventions
The index date (time zero) was defined as the date of the first PVA, the first cardioversion, and the second hospital record of any type in the dataset, for the PVA, cardioversion, and general AF cohorts, respectively.
Baseline risk factors were defined via diagnosis and procedure codes observed within 3 years prior to a patient’s index date (Table S1). Risk factors included diagnoses of previous stroke or TIA, hypertension, diabetes mellitus, heart failure, peripheral vascular disease, coronary artery disease, sleep apnea, hemorrhagic stroke, cardiomyopathy, obesity, other arrhythmias or conduction disorders, chronic kidney disease, COPD, hyperlipidemia, and pulmonary disease, as well as procedures for coronary artery bypass graft and percutaneous coronary intervention. CHADS2 and CHA2DS2-VASc scoresCitation11,Citation12 for stroke risk were also calculated.
Cohort matching
In order to reduce selection bias and create cohorts of patients that were clinically well matched with respect to available risk information, a combination of propensity and direct matching was used to match ablation patients in a 1:1 ratio with patients in the general AF control cohort, and separately to patients in the cardioversion cohort.
Propensity scores, defined as the patients’ probabilities of having PVA treatment based on their individual characteristics at or prior to their index date, were calculated separately for each control cohort from logistic regression models. Potential predictors in the propensity models included all baseline risk factors, as previously defined, with stepwise selection used to retain only those conditions that significantly impacted treatment cohort. The resulting propensity scores summarize patients’ probabilities of being in the ablation cohort vs each control cohort given their unique baseline comorbidity profile.
The two sets of propensity score, one for each control group, were used simultaneously with additional metrics to match ablation patients with general AF controls and separately with cardioversion controls. A SAS macro called gmatch, developed by the Mayo Clinic Biomedical Statistics and Informatics Division, was used to match patients in a 1:1 ratio on age, sex, year of index date, time from AF diagnosis to index date, and the resulting comorbidity-based propensity scores.Citation13
Stroke endpoints
The primary outcomes of interest were occurrence of ischemic stroke/TIA (ICD-10 diagnosis codes I63-I64x, G45) within 1-year intervals over equal time spans before and after a patient’s index date. The pre- and postindex analysis interval for each patient was equal to their follow-up from index date to last visit. Hospital and specialty care records were assumed to be comprehensive for all patients within this interval.
Binary stroke/TIA endpoints were created for each patient, for each year of their analysis interval, to indicate the occurrence of ischemic stroke or TIA events within the year. Patients with a stroke/TIA in a postindex year for which they did not have complete follow-up were included for that year to avoid bias from stroke mortality. Counts of patients with stroke/TIA and event rates for each year of follow-up were summarized by analysis cohort.
Statistical modeling
Generalized estimating equations with binary distributions and log link functions were utilized to model stroke/TIA event rates by year for each set of matched cohorts. Repeated measures methodology with unstructured correlation was used to account for the lack of statistical independence among multiple endpoints for each patient.
Separate models were utilized to test for the impact of PVA treatment on stroke risk in the preindex period and the postindex period due to the expectation that treatment would change the pattern or slope of stroke/TIA rates over time. Two preindex models, one for each pair of matched analysis cohorts, were constructed to test the assumption that baseline stroke risks were similar in the risk-matched cohorts. They included cohort and year as predictors, with year as a categorical variable, and cohort–year interaction included only if significant at a level of α =0.05. Two similar postindex models were constructed to test whether the stroke risk patterns over time were similar or different after divergence in AF treatment pathways.
All statistical analyses in this study were performed using SAS software, Version 9.2 (SAS Institute, Inc., Cary, NC, USA). All data used to perform this analysis were deidentified and accessed in compliance with the Health Insurance Portability and Accountability Act. As a retrospective analysis of a deidentified database, the research was exempt from Independent Review Board review under 45 Code of Federal Regulations 46.101(b)(4).
Results
A total of 1,409,106 patients had a diagnosis of AF, of which 6,356 met all inclusion and exclusion criteria for the PVA cohort. An additional 81,189 patients met the criteria for the cardioversion cohort, and 1,312,339 patients met the criteria for the general AF cohort. These cohorts formed the eligible populations from which matched pairs of PVA and cardioversion patients, and separately matched pairs of PVA and general AF patients, were chosen.
Matched populations
Of the 6,356 patients in the PVA cohort, 4,991 patients were matched to an equal number of general AF controls, and 5,407 patients were separately matched to cardioversion controls. CHADS2 and CHA2DS2-VASc risk score profiles were nearly identical between the two cohorts in each match (p-values 0.5588 and 0.6948, respectively, for PVA vs general AF; p-values 0.7428 and 0.8152 for PVA vs cardioversion). Age and sex distributions were also similar between cohorts, with the majority of patients 45–75 years of age and approximately 70% male. Since an AF diagnosis was required in 2008 or later and the data were only complete through 2013, most patients had index dates between 2008 and 2013, with nearly half of them in 2012 or 2013 ().
Table 1 Baseline patient characteristics
The time from first AF diagnosis to index date was similar in the matched PVA vs general AF controls, as this requirement was added to the matching algorithm to ensure that controls were not matched prior to their first AF diagnosis (means: 15 months). The matched PVA vs cardioversion controls were less similar since this timing was not a matching requirement, resulting in the PVA cohort having AF of longer duration than the cardioversion control cohort (means: 21 months PVA, 5 months cardioversion; )
The average length of available follow-up after index through the end of the 2013 was over 2 years for all cohorts, with median durations close to 2 years (). The number of patients with sufficient follow-up through their last visit record to be included in each year of the statistical models is shown by cohort and year in . In addition, this table shows the number of patients who dropped out of the analysis population for each year due to having a record of death in a hospital setting or due to reaching the end of 2013. Deaths in a hospital setting after index were consistently higher in the control cohorts than in the PVA cohorts.
Table 2 Sample sizes and reasons for loss to follow-up by year
Endpoint summary
In the PVA vs general AF matched cohorts, unadjusted stroke/TIA rates were similar between the cohorts in the year immediately prior to their index date, and both cohorts had increased stroke/TIA rates in the index year compared with prior years (). The increase in stroke rates during the index year was due in part to strokes occurring on the index date, which was a visit to the hospital system (including outpatient specialist visits). The stroke rates on this single day were 0.74% in the general AF cohort and 0.26% in the PVA cohort, leaving 1.02% and 0.39% stroke rates, respectively, occurring in the remainder of the first year. After the index date, the general AF cohort had consistently higher stroke/TIA rates than the PVA cohort, rising steadily through 4 years postindex, while the rate in the PVA cohort steadily decreased until the rate was nearly nine times as high in the general AF control cohort. Stroke/TIA rates were then similar in the fifth year, at which time the combined population had decreased to just 469 patients.
Figure 1 Yearly observed stroke rates in matched cohorts. (A) PVA vs matched general AF cohorts; (B) PVA vs matched cardioversion cohorts.
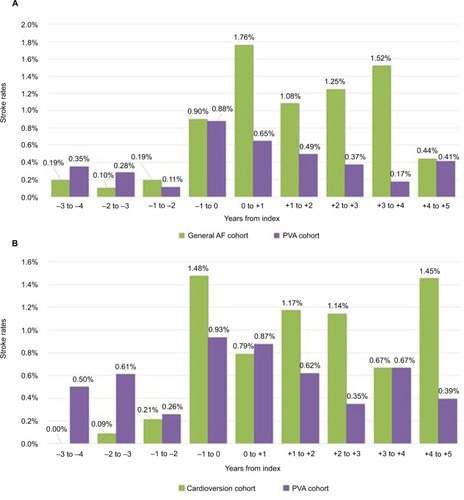
The PVA vs cardioversion control matched cohorts showed a pattern similar to the first match, although somewhat less regular (). Some notable differences were the higher stroke/TIA rates in this PVA cohort 1–4 years prior to the index date, and the higher stroke/TIA rates in the cardioversion control cohort for the year immediately prior to the index date. The index date accounted for 0.13% of the strokes in the cardioversion control cohort and 0.36% in the PVA cohort within the first year after treatment, leaving 0.66% and 0.51% rates, respectively, for the remainder of the first year. Since the cardioversion controls had a shorter duration of preceding AF, their higher stroke/TIA rate in the year before index suggests that a number of these events may have triggered the initial AF diagnosis.
Of the patients with stroke occurring on their index date, only a single PVA patient had another stroke in a subsequent year. This patient was represented in both matched populations and had a record of a second stroke in the second analysis year. No control patients in either the matched cardioversion cohort or the matched general AF cohort had strokes at index and also in a subsequent year. In addition, no patients with stroke occurring on their index date died in a hospital setting at any time through 2013.
Statistical modeling results
In both matched populations, statistical models of patient risk for stroke/TIA in the preindex time frame show similar event rates between cohorts (p=0.8292 for PVA vs general AF and 0.5198 for PVA vs cardioversion; ). The similar preindex event rates indicate that cohort matching was successful in creating cohorts with similar baseline stroke risks.
Table 3 Repeated measures logistic regression model resultsTable Footnotea
Postindex model results are also consistent between the two matched populations, but these models show a significantly lower risk of stroke/TIA events in PVA patients vs matched control groups over 5 years postindex (p<0.0001 for PVA vs general AF and 0.0222 for PVA vs cardioversion). Adjusted mean rates in PVA patients were 60% of the rates in matched cardioversion controls and 35% of the rates in general AF matches (0.82% PVA vs 1.37% cardioversion, p=0.0222; 0.64% PVA vs 1.84% general AF; p<0.0001). The large difference in postindex event rates and similar preindex rates suggests a divergence in outcomes stemming from the difference in treatment pathways beginning at the index date.
Discussion
In this very large population, matching resulted in almost identical CHA2DS2-VASc scores and stroke/TIA rates between cohorts prior to the index date. After the index date – on which ablation or cardioversion occurred – the adjusted rate of stroke/TIA was significantly lower in ablation patients than in either the cardioversion or the general AF control cohorts (40% and 65% lower, respectively). Repeated measures methodology, which observes the same patients before and after intervention, has not previously been utilized to determine whether catheter ablation of AF reduces stroke risk. The similarity in stroke risk between cohorts prior to the index date suggests that confounding by unmeasured variables is not responsible for subsequent differences, while the divergence following the index date suggests a treatment effect beginning on that date.
No studies have prospectively tested whether the superiority of catheter ablation over antiarrhythmic drugs in restoring sinus rhythmCitation3,Citation4 results in a lower risk of stroke/TIA. Investigators have reported stroke/TIA rates <1%/year among patients with CHA2DS2-VASc scores ≥2 and discontinued anticoagulation following AF ablation.Citation14–Citation17 Registry data have also shown that patients who maintain sinus rhythm following ablation have stroke/TIA rates similar to age- and sex-matched patients with no AF history.Citation18 Large randomized trials – Catheter Ablation vs Antiarrhythmic Drug Therapy for Atrial Fibrillation Trial and Early Treatment of Atrial Fibrillation for Stroke Prevention Trial – are not expected to be completed until 2018–2019. Two retrospective cohort studies, each with 4,212 PVA patients, used age and sex matching,Citation6 and CHADS2 score matching,Citation7 to show that stroke/TIA risk in the PVA patients was similar to patients without AF, and significantly lower than in patients with AF but without intervention. Two subsequent papers used propensity matching to compare populations of over 800 matched PVA and AF control pairs each, resulting in PVA groups with significantly lower stroke/TIA rates.Citation8,Citation9 Propensity matching was also used to show a significantly lower stroke/TIA rate in 12,122 PVA patients compared with AF patients who had undergone cardioversion.Citation10
While matching technologies can greatly reduce bias, they are still limited by the possibility of confounding due to unmeasured variables. The key strength of this study is the unique combination of tight matching and repeated measures methodology used to overcome this limitation. The tight matching of patient stroke risks ensures that stroke rates are similar among cohorts at baseline, while repeated measures methodology examines the effect of intervention over time in the same patients. Together, these provide confidence that the drop in stroke rates for the PVA cohorts after index is a consequence of treatment.
Until large randomized trials report, clinicians will need to judge from these data whether catheter ablation of AF reduces the risk of stroke. Previous cohort studies have been consistent in showing a large benefit toward PVA. The current study examines the modern era of PVA with >80% of procedures performed during or after 2010. Its results are consistent with previous studies, but greatly reduce the likelihood of selection bias by demonstrating equal stroke risks between cohorts prior to PVA.
These results, coupled with prior results suggesting that ablation prevents progression of paroxysmal to persistent AFCitation19 and its consequent morbidity and mortality,Citation20,Citation21 raise important questions for clinicians. Current guidelines recommend catheter ablation be performed only in symptomatic patients.Citation22,Citation23 Additionally, they recommend that anticoagulation be continued late after ablation in patients with elevated CHA2DS2-VASc scores.Citation24 These recommendations are potentially impacted by the results of this study.
Limitations
The primary limitation of this study is its reliance on routinely collected data, which may lack the sensitivity and specificity of prospectively collected data. Stroke/TIA rates may be underestimated, but this would be expected to affect all cohorts proportionately. The study could not differentiate types of AF, and thus the benefit of PVA may not be consistent across all stages of AF. Anticoagulation usage was unknown and could vary between groups, although the tight matching on CHADS2 and CHA2DS2-VASc scores minimizes this risk, as does comparison to a cardioversion cohort. In previous studies where anticoagulation data were available, usage was similar between cohorts.Citation8,Citation9 Recent adoption of continued oral anticoagulation at ablation could reduce the postindex stroke rate even further,Citation25 as might newer techniques that improve long-term maintenance of sinus rhythm.Citation26 It is important to note that despite the careful cohort matching combined with methodology that used patients as their own controls over time, residual confounding is still a possibility due to data limitations.
Conclusion
Propensity matching of AF patients with PVA treatment to similar patients with cardioversion or with neither treatment resulted in cohorts with the same baseline rate of stroke/TIA. Following treatment, the stroke/TIA rate was significantly lower in the PVA cohort than in either control cohort.
Acknowledgments
Biosense Webster provided funding for data collection, statistical analysis, and medical writing. The Cardiovascular Biomedical Research Unit, Royal Brompton & Harefield NHS Foundation Trust, supported data analysis, drafting, and revision work of JWEJ, WH, TW, and VM.
Supplementary material
Table S1 Diagnosis or procedure codes
Disclosure
TDH is an employee of CTI Clinical Trial & Consulting Services, Inc., which is a paid consultant to Biosense Webster. JLM is a paid employee of Biosense Webster. VM reports personal fees from Biosense Webster, outside the submitted work. The authors report no other conflicts of interest in this work.
References
- SvennbergEEngdahlJAl-KhaliliFFribergLFrykmanVRosenqvistMMass screening for untreated atrial fibrillation: The STROKESTOP StudyCirculation2015131252176218425910800
- WolfPAAbbottRDKannelWBAtrial fibrillation as an independent risk factor for stroke: the Framingham StudyStroke19912289839881866765
- NoheriaAKumarAWylieJVJrJosephsonMECatheter ablation vs antiarrhythmic drug therapy for atrial fibrillation: a systematic reviewArch Intern Med2008168658158618362249
- WynnGJDasMBonnettLJPanikkerSWongTGuptaDEfficacy of catheter ablation for persistent atrial fibrillation: a systematic review and meta-analysis of evidence from randomized and nonrandomized controlled trialsCirc Arrhythm Electrophysiol20147584185225132078
- HaACHindricksGBirnieDHVermaALong-term oral anticoagulation for patients after successful catheter ablation of atrial fibrillation: is it necessary?Curr Opin Cardiol20153011725389647
- BunchTJCrandallBGWeissJPPatients treated with catheter ablation for atrial fibrillation have long-term rates of death, stroke, and dementia similar to patients without atrial fibrillationJ Cardiovasc Electrophysiol201122883984521410581
- BunchTJMayHTBairTLAtrial fibrillation ablation patients have long-term stroke rates similar to patients without atrial fibrillation regardless of CHADS2 scoreHeart Rhythm20131091272127723835257
- ReynoldsMRGunnarssonCLHunterTDHealth outcomes with catheter ablation or antiarrhythmic drug therapy in atrial fibrillation: results of a propensity-matched analysisCirc Cardiovasc Qual Outcomes20125217118122373904
- ChangCHLinJWChiuFCCaffreyJLWuLCLaiMSEffect of radiofrequency catheter ablation for atrial fibrillation on morbidity and mortality: a nationwide cohort study and propensity score analysisCirc Arrhythm Electrophysiol201471768224446025
- NoseworthyPAKapaSDeshmukhAJRisk of stroke after catheter ablation versus cardioversion for atrial fibrillation: a propensity-matched study of 24,244 patientsHeart Rhythm20151261154116125708883
- GageBFWatermanADShannonWBoechlerMRichMWRadfordMJValidation of clinical classification schemes for predicting stroke: results from the national registry of atrial fibrillationJAMA2001285222864287011401607
- LipGYNieuwlaatRPistersRLaneDACrijnsHJRefining clinical risk stratification for predicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heart survey on atrial fibrillationChest2010137226327219762550
- Mayo Clinic [homepage on the Internet]Gmatch macro developed by Erik Bergstralh and Jon Kosanke2003 Available from: http://www.mayo.edu/research/departments-divisions/department-health-sciences-research/division-biomedical-statistics-informatics/software/locally-written-sas-macrosAccessed January 31, 2016
- WinkleRAMeadRHEngelGKongMHPatrawalaRADiscontinuing anticoagulation following successful atrial fibrillation ablation in patients with prior strokesJ Interv Card Electrophysiol201338314715324101149
- SaadEBd’AvilaACostaIPVery low risk of thromboembolic events in patients undergoing successful catheter ablation of atrial fibrillation with a CHADS2 score ≤3: a long-term outcome studyCirc Arrhythm Electrophysiol20114561562121841192
- RileyMPZadoEHutchinsonMDRisk of stroke or transient ischemic attack after atrial fibrillation ablation with oral anticoagulant use guided by ECG monitoring and pulse assessmentJ Cardiovasc Electrophysiol201425659159624533561
- ThemistoclakisSCorradoAMarchlinskiFEThe risk of thromboembolism and need for oral anticoagulation after successful atrial fibrillation ablationJ Am Coll Cardiol201055873574320170810
- HunterRJMcCreadyJDiabIMaintenance of sinus rhythm with an ablation strategy in patients with atrial fibrillation is associated with a lower risk of stroke and deathHeart2012981485321930724
- ProiettiRHadjisAAlTurkiAA systematic review on the progression of paroxysmal to persistent atrial fibrillation. Shedding new light on the effects of catheter ablationJACC Clin Electrophysiol201513105115
- SteinbergBAHellkampASLokhnyginaYHigher risk of death and stroke in patients with persistent vs. paroxysmal atrial fibrillation: results from the ROCKET-AF TrialEur Heart J201536528829625209598
- GlotzerTVDaoudEGWyseDGThe relationship between daily atrial tachyarrhythmia burden from implantable device diagnostics and stroke risk: the TRENDS studyCirc Arrhythm Electrophysiol20092547448019843914
- CammAJLipGYDe CaterinaR2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm AssociationEur Heart J201233212719274722922413
- JanuaryCTWannLSAlpertJS2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm SocietyCirculation2014130232071210424682348
- CalkinsHKuckKHCappatoR2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial designEuropace201214452860622389422
- Di BiaseLBurkhardtJDSantangeliPPeriprocedural stroke and bleeding complications in patients undergoing catheter ablation of atrial fibrillation with different anticoagulation management: results from the Role of Coumadin in Preventing Thromboembolism in Atrial Fibrillation (AF) Patients Undergoing Catheter Ablation (COMPARE) randomized trialCirculation2014129252638264424744272
- DuytschaeverMTaghjiPTavernierRTowards durable pulmonary vein isolation: we are closing the gapEuropace20151781164116526041871