Abstract
Background
The purpose of this study was to assess the 12-month outcomes associated with naturalistic antipsychotic treatment of patients participating in the Schizophrenia Outpatient Health Outcomes (SOHO) study.
Methods
SOHO is a 3-year, prospective, observational study of the health outcomes associated with antipsychotic treatment in 10 European countries. The study included over 10,000 outpatients who were initiating or changing their antipsychotic medication. Medication use pattern, change in symptom severity, social functioning, and health-related quality of life were assessed, as well as rates of response, remission, treatment discontinuation, adverse events, and hospitalization.
Results
Clinical Global Impression-Severity for Schizophrenia (CGI-SCH) and quality of life scores improved in all treatment cohorts. There were greater improvements in the CGI-SCH overall symptom score and in the CGI-SCH positive, negative, cognitive, and depressive symptom scores in the olanzapine and clozapine cohorts compared with other treatment cohorts. Changes were associated with an improvement in quality of life. Patients treated with olanzapine, quetiapine, and clozapine had better tolerability per extrapyramidal symptoms and sexual-related dysfunction measures compared with patients receiving risperidone, amisulpride, or typicals. Patients treated with olanzapine had greater weight gain than patients in all other treatment cohorts.
Conclusion
Patients initiated on olanzapine and clozapine tend to have better outcomes at 12 months than patients initiated on other antipsychotics in routine outpatient clinical practice. Results should be interpreted conservatively due to the nonrandomized study design.
Introduction
Although antipsychotics remain the cornerstone of the treatment of schizophrenia, the relative effectiveness of different antipsychotics in routine clinical practice is still a topic of debate. Most of the current knowledge about the effects of antipsychotic drugs originates from randomized clinical trials, which have formed the evidence base for current expert guidelines and recommendations for the treatment of schizophrenia.Citation1–Citation4 However, randomized clinical trials have inherent design limitations and cannot fully reflect the use and impact of antipsychotic medications in actual clinical practice. Most randomized clinical trials are of short duration,Citation5 involve selected samples of patients,Citation6,Citation7 focus on clinical outcomes instead of quality of life or social functioning,Citation8 and impose stringent treatment regimens that limit the generalizability of the results.Citation9–Citation11
Recent meta-analyses of randomized clinical trials comparing the effects of antipsychoticsCitation12,Citation13 have shown that there are in fact relevant differences in the outcomes of various antipsychotic treatments. In these reviews, Leucht et al suggest that some second-generation antipsychotics may be more efficacious than others, but that in tailoring drug treatment to the individual patient, efficacy superiorities must be weighed against large differences in treatment-emergent adverse events and cost. How these differences translate into routine clinical practice is not well understood.
The European Schizophrenia Outpatient Health Outcomes (SOHO) study is a large, 3-year, prospective, observational study of the outcomes of antipsychotic treatment for schizophrenia in the outpatient setting that provides a valuable base for comparing the effects of antipsychotics in routine clinical practice. To date, the published results of the SOHO study have focused on reporting the 6-month and 3-year outcomes. However, there has not yet been a paper that reports comprehensively the course of treatment outcomes for the first 12 months of the SOHO study. One year is a timeframe usually employed for planning the delivery of health care services and is often used for the development of economic decision-making models. Thus, reporting the 12-month results of SOHO may provide valuable data to help clinicians, administrators, and policy decision makers to make informed decisions in the treatment of patients with schizophrenia in usual care settings. We report here the results at 12 months of the antipsychotic treatment prescriptions started when patients were recruited into the SOHO study. We present data on a wide range of outcomes including response, remission, treatment maintenance, hospitalization, and treatment tolerability.
Patients and methods
Study design
The SOHO study was a 3-year, international, prospective, observational, non-interventional study conducted in 10 European countries (Denmark, France, Germany, Greece, Ireland, Italy, the Netherlands, Portugal, Spain, and the UK) and recruited 10,972 patients between September 1, 2000 and December 31, 2001. The study was approved in all countries at the site, regional, or national level, depending on the country regulations and participating sites in each of the countries. Patient informed consent followed country regulations. All patients gave at least oral informed consent, and written informed consent was obtained from patients in Denmark, Italy, Portugal, Spain, Ireland, and the UK. The design and baseline findings of the SOHO study and the 6-month results have been reported elsewhere.Citation14–Citation17
Patients participating in the study were adults (aged ≥18 years) who, at the baseline visit, initiated or changed antipsychotic medication for the treatment of schizophrenia in an outpatient, ambulatory, or community setting, irrespective of the reason for medication change. Patients were included regardless of whether the new antipsychotic drug substituted a previous medication or was an addition to existing treatment, and regardless of the reason for the treatment change. Thus, patients in the SOHO study could be prescribed more than one antipsychotic drug at the baseline visit.
Because the SOHO study had a specific focus on olanzapine, the study design included oversampling of patients starting olanzapine and aimed to provide two patient cohorts of approximately equal size, ie, those who initiated therapy with or changed to olanzapine and those who initiated therapy with or changed to a nonolanzapine antipsychotic.
Each participating psychiatrist was asked to enrol approximately 10 patients, with equal numbers in each of the two patient cohorts. No minimum number of patients per psychiatrist was required and the enrolment period was purposely long. Investigators were instructed to make treatment decisions independent of the study and prior to evaluation of eligibility for inclusion based on entry criteria and the structure of enrolment. Effort was made to avoid any interference with clinical practice. A total of 1096 psychiatrists mostly working in public (46.9%) or combined public and private (37.2%) practices participated.
Data collection
Data collection occurred during routine outpatient visits and was targeted for baseline, 3 and 6 months post-baseline, and every 6 months thereafter. For each data collection target, investigators were allowed to collect data up to one month before or after the target month. Patients who were not seen during the normal course of care within one assessment interval were not excluded from subsequent data collection. The data collected were similar to those collected in routine clinical practice, including patient demographics, medical resource use, functional status, clinical status, medication use, tolerability, patient-reported and physician-reported adherence, sexual functioning, alcohol and substance abuse, and quality of life.
Data assessment and analysis
Patients were classified into seven treatment cohorts according to the antipsychotic started at baseline, ie, olanzapine, risperidone, quetiapine, amisulpride, clozapine, oral typical antipsychotic, and depot typical antipsychotic, regardless of whether they were still receiving that medication at any further visit. Patients who started more than one antipsychotic at the baseline visit were not included in the analyses. However, patients could be taking more than one antipsychotic if they maintained treatment with an antipsychotic that they were taking before baseline, or added a new antipsychotic after baseline. A total of 9608 patients were included in the analysis. Of these, the proportion of patients evaluated at 12 months was 84% (4344/5204) for patients who started olanzapine at baseline, 86% (1596/1863) for patients who started risperidone, 83% (627/760) for patients who started quetiapine, 76% (243/319) for patients who started amisulpride, 92% (289/316) for patients who started clozapine, 86% (579/676) for patients who started an oral typical, and 87% (407/470) for patients who started a depot typical.
Response
Clinical severity at baseline and response to treatment was assessed using a scale based on the Clinical Global Impression (CGI)Citation18 that evaluated positive, negative, cognitive, depressive, and overall symptoms on the day of assessment. This was validated as the Clinical Global Impression-Severity for Schizophrenia (CGI-SCH).Citation19 Scores range from 0 (normal, not ill) to 6 (among the most severely ill).
Response was defined as a decrease (improvement) from baseline of two points in CGI-SCH overall (scale 0–6) if the initial value is 4, 5, or 6; or one point if the initial value is 1, 2, or 3, at least once at either 3, 6, or 12 months. Patients with a score of 0 at baseline were excluded from the analysis of response. Patients who stopped taking their baseline medication before responding were classified as nonresponders.
Quality of life was assessed using the EuroQol-5 Dimensions (EQ-5D), a patient self-rated, generic, health-related quality of life instrument.Citation20 The EQ-5D is composed of two parts, ie, five questions that assess quality of life in different domains (mobility, self-care, usual activities, pain, and anxiety/depression) and a visual analog scale (EQ-5D VAS) where patients self-rate their overall health on a scale of 0–100, with 0 representing the lowest possible health and 100 the best possible health. Social functioning was assessed using single-item questions that asked whether the patient was involved in any social interactions in the previous 4 weeks (socially active), in a relationship with a spouse or partner, or was exhibiting verbal or physical hostile or aggressive behaviors.
Remission
Remission was defined as a score of 2 (mild severity) or less on a scale of 0–6 on the CGI-SCH overall severity score, the CGI-SCH positive symptoms score, the CGI-SCH negative symptoms score and the CGI-SCH cognitive symptoms score, and maintained for two consecutive visits.Citation21
Antipsychotic dose
To enable a comparison of the doses between the cohorts, doses for typical antipsychotics were transformed into olanzapine or haloperidol depot equivalents following a recent consensus which included most typical antipsychotics.Citation22 However, some medications with equivalences not reported have not been included in the analysis of the dose. Olanzapine 20 mg was used as the reference for the equivalency estimates of oral and long-acting injectable agents. Injectable haloperidol 5 mg was used as the reference for short-acting injectable agents.
Treatment discontinuation
Treatment discontinuation was defined as stopping the antipsychotic medication started at baseline. If a new treatment was added but the baseline antipsychotic was continued, discontinuation was not considered to have occurred. If a patient did not participate in a visit before switching, he/she was censored (not discontinued) at this visit. The time to discontinuation of treatment was expressed in months, from baseline to the first visit at which the patient discontinued. If a patient discontinued the treatment between two visits, the change was imputed at the mid-point. Survival curves for time to discontinuation over 12 months were constructed using unadjusted Kaplan-Meier estimates. A sensitivity analysis was conducted in which patients not participating in a visit were considered to have discontinued (not censored).
Cox regression models were used to compare the time to medication discontinuation between treatment groups. Since differences among the medication groups could exist at baseline (“selection bias”), the models included the characteristics of the patients at the baseline assessment to address variations that could have affected treatment group differences. Only those variables that remained after performing a stepwise model reduction were kept.
Treatment group comparisons in the changes in CGI-SCH scale scores from baseline over time were made using a mixed model (SAS version 9.0) including the same fixed covariates as for the time to discontinuation, plus baseline CGI-SCH score and time. Time was classified into months (3, 6, and 12 months). The correlation of repeated measures within each patient was modeled with the use of a random intercept and an unstructured covariance matrix. Treatment group comparisons for response at any time during follow-up were conducted using a logistic regression analysis taking into account baseline covariates.
Adverse events
Tolerability data included extrapyramidal symptoms (dystonia, akathisia, parkinsonism), tardive dyskinesia, prolactin-related sexual dysfunction (loss of libido/impotence, and presence of amenorrhea/galactorrhea/gynecomastia), and weight and body mass index change by antipsychotic treatment cohort at baseline and at each visit thereafter. Extrapyramidal symptoms and tardive dyskinesia were assessed using a four-point scale (1 = not present; 2 = present but does not significantly interfere with patient’s functioning or health-related quality of life; 3 = present and significantly interferes with patient’s functioning or health-related quality of life; 4 = present and outweighs therapeutic effect) and counted as present (rating of 2, 3, or 4) or not present (rating of 1). Body weight was recorded by the clinician at each visit without any standardized procedure (ie, no instructions were given on how to measure weight). The appearance of adverse events for those patients not presenting such events at baseline was assessed by medication cohort. A logistic regression model adjusting for baseline differences was used to test for statistical differences between medication cohorts.
Hospitalization
Differences in frequency of psychiatric hospitalization were described for each of the medication cohorts in the 12 months following baseline.
Results
A total of 9608 patients were included in the baseline analysis, and 8085 (84.1%) were available for analysis at 12 months. shows that approximately half of the patients in the study started olanzapine at baseline (5204/9608, 54%), which is a direct consequence of the study design. The sociodemographic and clinical characteristics of the different cohorts at baseline were similar, except for a few differences (). Patients in the clozapine cohort tended to be younger and have more severe illness (as indicated by higher mean CGI-SCH ratings) than the other cohorts. Baseline functional status was comparable across the treatment cohorts, except for patients in the clozapine cohort, who tended to have lower social functioning.
Table 1 Demographic and clinical characteristics at baseline assessment by treatment cohort
Medication use
Most patients were prescribed treatment with only one antipsychotic after the baseline visit (range 71%–85% across cohorts, ). In general, the mean doses of antipsychotic medication prescribed at baseline remained stable at 12 months, although there was noticeable dose titration with quetiapine and clozapine ().
Table 2 Pharmacological treatment patterns by treatment cohort
Response
shows the improvement in CGI-SCH overall severity scores from baseline to 12 months, by treatment cohort. Although most improvement occurred in the first 3 months after baseline, there was continued improvement during 3 to 12 months in all cohorts. Clinical and social outcomes at 12 months are summarized in . The percentage of patients responding to treatment based on CGI-SCH overall symptom severity ranged from 64% in the olanzapine and clozapine cohorts to 45% in the amisulpride cohort. Patient health-related quality of life (EQ-5D VAS) increased from about 45 at baseline to around 60 at the 12-month visit. Some differences were present among cohorts. Response rates based on CGI-SCH subscales were generally greatest with olanzapine; these ranged from 52% in the quetiapine cohort to 67% in the olanzapine cohort for positive symptoms, from 42% in the depot typical cohort to 61% in the olanzapine cohort for negative symptoms, 40% in the depot typical cohort to 61% in the olanzapine cohort for cognitive symptoms, and 48% in the oral typical cohort to 67% in the olanzapine cohort for depressive symptoms.
Figure 1 CGI-SCH scores over 12 months, by treatment cohort.
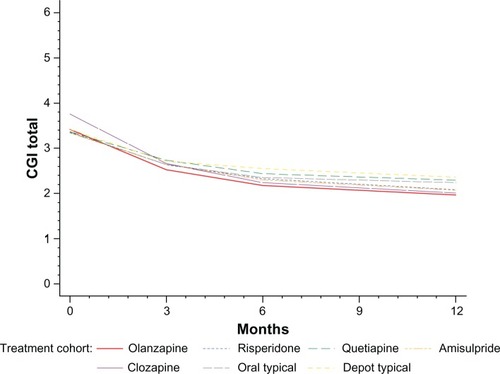
Table 3 Clinical and social outcomes at 12 months
The multivariate models that have been fitted allow the comparison between the treatment cohorts adjusting for the baseline differences that originated in the observational nature of SOHO. shows results of the multivariate analysis for each outcome in each treatment cohort relative to the olanzapine cohort and adjusted for baseline differences between the cohorts. The change in CGI-SCH overall from baseline showed that symptom improvement for patients in the risperidone, quetiapine, and oral and depot typical antipsychotic cohorts was significantly lower than in the olanzapine cohort. Compared with olanzapine, patients in all cohorts, except clozapine, had a significantly lower likelihood of achieving a response in CGI-SCH overall. Patients in all cohorts except the clozapine cohort had a lower increase in EQ-5D VAS at 12 months compared with olanzapine. For CGI-SCH positive symptoms, patients in the risperidone, quetiapine, amisulpride, and oral typical and depot typical antipsychotic cohorts had a significantly lower response than those in the olanzapine cohort (). Compared with olanzapine, also shows that patients in all cohorts except clozapine were less likely to demonstrate a response in CGI-depressive symptoms than those in the olanzapine cohort.
Table 4 Social and clinical outcomes at 12 months: odds ratios from multivariate analysis comparing olanzapine with the other treatment cohorts
Social outcomes
The percentage of patients who were socially active ranged from 52% in the quetiapine cohort to 70% in the olanzapine cohort (). The multivariate models which adjusted for baseline covariates showed that patients in the olanzapine cohort were more likely to be socially active ().
Remission
Of the 9079 patients analyzed for remission, a total of 3189 (35.1%) achieved remission over the 12-month period. Remission rate was highest in the clozapine cohort and lowest in the quetiapine cohort; remission was achieved by 1913 (39.1%) olanzapine-treated patients, 594 (33.5%) risperidone-treated patients, 174 (24.4%) quetiapine-treated patients, 74 (25.2%) amisulpride-treated patients, 122 (40.0%) clozapine-treated patients, 194 (29.8%) oral typical-treated patients, and 118 (26.1%) depot typical-treated patients.
The regression analysis demonstrated that the likelihood of achieving remission over the 12-month period was significantly more likely with olanzapine than with any of the other antipsychotics except for clozapine. Compared with olanzapine, the odds ratio of achieving remission was 0.569 (95% CI 0.422–0.768, P = 0.0002) for amisulpride, 1.358 (95% CI 1.045–1.765, P = 0.0219) for clozapine, 0.555 (95% CI 0.437–0.704, P < 0.0001) for depot typical, 0.581 (95% CI 0.476–0.709, P < 0.0001) for oral typical, 0.454 (95% CI 0.372–0.554, P < 0.0001) for quetiapine, and 0.712 (95% CI 0.626–0.810, P < 0.0001) for risperidone.
Treatment discontinuation
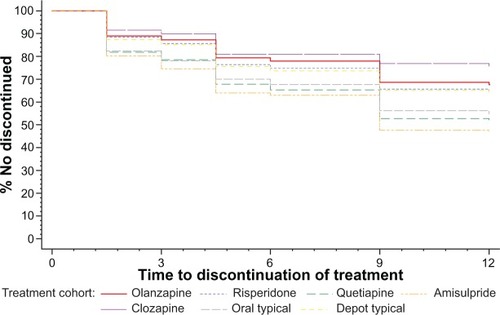
Time to discontinuation by treatment cohort is shown in . The risk of treatment discontinuation at 12 months was lowest and similar for olanzapine and clozapine, slightly higher for risperidone and depot typicals, and highest for quetiapine, amisulpride, and oral typicals. The sensitivity analysis (in which patients not participating in a visit were considered to have discontinued rather than just censored) is shown in ; the rank order of risk of discontinuation with different cohorts remained the same in the sensitivity analysis.
Figure 2 Time to discontinuation over 12 months, by treatment cohort.
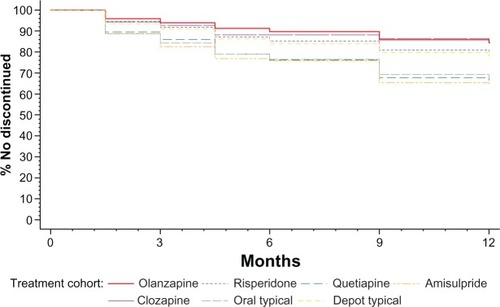
Figure 3 Time to discontinuation over 12 months, by treatment cohort: sensitivity analysis (patients not participating in a visit were considered to have discontinued).
The results of the Cox’s proportional hazards model that analyzed differences in discontinuation rate showed that discontinuation was lowest for olanzapine and clozapine and that all medications except for clozapine had a higher discontinuation rate than olanzapine. Hazards ratios were 1.39 for risperidone (95% CI 1.22–1.59), 2.34 for quetiapine (95% CI 2.00–2.72), 2.39 for amisulpride (95% CI 1.92–2.98), 2.31 for oral typical (95% CI 1.97–2.71), and 1.48 for depot typical (95% CI 1.19–1.84).
Adverse events
Adverse events at 12 months are summarized in . The occurrence of extrapyramidal symptoms at 12 months was least in the olanzapine cohort (8%) and greatest in the depot typical cohort (31%); compared with olanzapine, the likelihood of experiencing extrapyramidal symptoms was increased with all antipsychotics except clozapine and quetiapine. Loss of libido was lowest in the clozapine cohort (17%) and highest in the amisulpride cohort (30%); compared with olanzapine, the likelihood of experiencing loss of libido was increased in patients taking risperidone or typical antipsychotics. Impotence/sexual dysfunction were lowest in the quetiapine cohort (12%) and highest in the amisulpride and oral typical cohorts (22%); compared with olanzapine, impotence/sexual dysfunction was higher with all antipsychotics except for quetiapine. The frequency of gynecomastia and galactorrhea after 12 months of treatment was low in all cohorts; at 12 months gynecomastia ranged from 2% to 5%, and galactorrhea ranged from 1% to 4%. Compared with olanzapine, the likelihood of experiencing amenorrhea was increased in the risperidone, amisulpride, and depot typical antipsychotic cohorts. Mean weight increased during the 12 months of treatment in all treatment cohorts; increases in mean weight from baseline to 12 months ranged from 3.2 kg in the olanzapine cohort to 0.6 kg in the quetiapine cohort. Compared with olanzapine, patients in other cohorts were significantly less likely to experience weight gain, except for clozapine. Clinically significant weight gain (≥7% body weight) from baseline to 12 months occurred in 1379 (28.1%) olanzapine-treated patients, 323 (18.3%) risperidone-treated patients, 109 (15.4%) quetiapine-treated patients, 56 (19.0%) amisulpride-treated patients, 60 (19.6%) clozapine-treated patients, 121 (18.7%) oral typical-treated patients, and 89 (19.7%) depot typical-treated patients. The likelihood of experiencing clinically significant weight gain was higher in the olanzapine cohort than in all other antipsychotic cohorts. At 12 months, the increase in body mass index category across the cohorts ranged from 13% (with quetiapine and depot typicals) to 21% (with olanzapine).
Table 5 Appearance of adverse events during the 12 months of follow-up
Hospitalization
Hospitalization in the different medication cohorts during the 12 months following baseline ranged from 13%–24%; hospitalization occurred in 607 (13%) olanzapine-treated patients, and in 240 (14%) risperidone, 137 (20%) quetiapine, 70 (24%) amisulpride, 49 (16%) clozapine, 105 (16%) oral typical, and 79 (18%) depot typical-treated patients. Compared with olanzapine, the odds ratios for hospitalization were higher in the other cohorts except clozapine and risperidone.
Discussion
The SOHO study is the largest prospective observational investigation of the long-term use and outcomes associated with antipsychotic drugs in schizophrenia to have been conducted to date. This analysis of 12-month SOHO data found that the cohorts of patients treated with olanzapine and clozapine tended to have a better clinical course than patients treated with other atypical or typical antipsychotics. Patients receiving olanzapine or clozapine had a higher response rate when using CGI-SCH overall symptom severity and when assessing specific symptom domains, ie, positive, negative, cognitive, and depressive symptoms. In addition, the differences in clinical outcomes were associated with greater improvements in patient health-related quality of life as well as in some aspects of social functioning. Treatment discontinuation, which is considered the best method to assess effectiveness of antipsychotics,Citation23 was also lower. With regard to remission, regression analysis demonstrated that the likelihood of achieving remission over the 12-month period was significantly higher with olanzapine and clozapine than with the other studied antipsychotics.
Current findings of better outcomes with olanzapine and clozapine compared with other antipsychotics are consistent with prior studies comparing different antipsychotic drugs, such as the CATIE study,Citation23 the meta-analyses of randomized controlled trials comparing the effectiveness of antipsychotics conducted by Leucht et al,Citation12,Citation13 and the findings of the large-scale observational study conducted by Tiihonen et al.Citation24 Therefore, these 12-month findings from the SOHO study add to the body of evidence suggesting that there are differences in the outcomes of treatment with various antipsychotics.
In the present study, improvements in clinical outcomes at 12 months were translated into improvements in patient health-related quality of life and social functioning. Quality of life was assessed using the EQ-5D, a generic instrument that has been validated in patients with schizophrenia from the 10 countries included in the SOHO study,Citation25 and which is sensitive enough to pick up differences between patients with varying severities of illness.Citation26 Improvement in quality of life was slightly greater for patients in the olanzapine cohort compared with the risperidone, amisulpride, quetiapine, and typical and depot antipsychotic cohorts. Improvements in quality of life have been noted previously with atypical antipsychotics and are greater than those seen with typical antipsychotics.Citation27,Citation28 We also found evidence of some improvement in social functioning. There were some differences between treatment cohorts in these functional outcomes, and patients treated with typical antipsychotics were found to be less socially active than those treated with olanzapine. Similar findings have been reported previously in a comparison between olanzapine and haloperidol.Citation29
Antipsychotic dose can be of great importance in the interpretation of effectiveness and the prevalence and severity of treatment-emergent adverse events. In general, the dosage range is not only related to optimal efficacy, but can also be related to the prevalence of adverse events. The antipsychotic doses used in the SOHO study are consistent with those from previous long-term and mid-term studies, clinical experience, and pharmacological guidelines for schizophrenia. The mean dose of olanzapine used in SOHO (12.0 mg/day) is similar to that used by other investigatorsCitation30 and appears to be optimal in the treatment of outpatients with schizophrenia.Citation31 The mean dosage used in the risperidone cohort (5.0 mg/day) was also similar to the modal dose (4.8 mg/day) used in a study by Conley and Mahmoud.Citation32 The dose for amisulpride (mean 415 mg/day) is at the lower end of the recommended range (400–800 mg/day),Citation33 and the dose for quetiapine (mean 388 mg/day) is slightly below the recommended dose (400 mg/day);Citation34 in both medications there was an upward dose titration during the course of the study. Although used in clinical practice in a wide range, the mean clozapine dose in the SOHO study (245 mg/day) is lower than that recommended by the manufacturer.Citation35
Antipsychotic discontinuation for any cause is considered a powerful indicator of medication effectiveness in schizophreniaCitation23 because it reflects the medication’s efficacy, safety, and tolerability from both the patient and clinician perspectives. In the CATIE study, olanzapine was the antipsychotic with the lowest rate of all-cause medication discontinuation.Citation23 The risk of treatment discontinuation at 12 months in SOHO was also the lowest and similar for olanzapine and clozapine. However, rates of 12-month antipsychotic treatment maintenance reported here were higher than in CATIECitation23 which might be related to the double-blind design of the CATIE study. Other observational studies also support the higher effectiveness of olanzapine compared with other antipsychotics.Citation24
With regard to treatment-emergent adverse events, the olanzapine, quetiapine, and clozapine cohorts had, at 12 months, the lowest proportion of patients with extrapyramidal symptoms, while the risperidone and oral and depot typical antipsychotic cohorts had the highest proportions. In a meta-analysis of randomized clinical trials, patients treated with olanzapine, quetiapine, risperidone, and sertindole were found to use less antiparkinsonian medication than haloperidol-treated patients.Citation36 Moreover, the higher incidence of extrapyramidal symptoms in the risperidone cohort is also consistent with previous reports showing that risperidone-induced extrapyramidal symptoms are dose-dependent.Citation37
Patients treated with olanzapine, clozapine, and quetiapine were significantly less likely to have sexual dysfunction after 12 months of treatment than those in the other treatment cohorts; these adverse events were much more likely to occur in patients treated with oral typical or depot typical antipsychotics, risperidone, and amisulpride. These findings are in line with other studies reporting that olanzapine is associated with less sexual dysfunction than risperidone or typical antipsychotics,Citation38,Citation39 and that quetiapine is associated with a low incidence of sexual dysfunction.Citation39
The mechanisms underlying sexual dysfunction in antipsychotic-treated patients are poorly understood but may be related to increased prolactin levels, and prolactin levels may be 10 times higher than normal in some patients receiving antipsychotics.Citation40 Elevated prolactin levels are common during treatment with amisulpride and risperidone, whereas olanzapine-, quetiapine-, and clozapine-treated patients experience modest elevations on prolactin levels during chronic administration.Citation41,Citation42 Treatment-emergent sexual dysfunction is distressing for patients and may result in nonadherence with medication, which in turn can result in treatment failure.
Rates of obesity in schizophrenia are a cause for concern because they are higher than in the general population.Citation43 Weight gain, as an adverse event of treatment with antipsychotic medications, is an important problem because it may contribute to the increased risk for obesity-associated problems,Citation44,Citation45 and may also affect adherence to medication.Citation46 A meta-analysis of 81 studies revealed that among the antipsychotic agents examined, clozapine and olanzapine were associated with the greatest increase in weight at 10 weeks.Citation47
The results from the present study confirm previous findings that many antipsychotics, both typical and atypical agents, are associated with weight gain. Consistently with the meta-analysis reported above, the increases in weight were significantly greater in the olanzapine cohort than in the other treatment cohorts, except clozapine.
The mechanisms underlying antipsychotic treatment-emergent weight gain are unclear, but may be caused by a number of factors, including effects on neurotransmission (such as dopamine, serotonin, or histamine), interactions with hormones, and several environmental factors.Citation45,Citation48 Some patients may have a genetic predisposition to antipsychotic treatment-emergent weight gain.Citation48
There is little information on how the results from one region of the world generalize to other areas. There is some evidence that the course of schizophrenia varies among regions of the world.Citation49 However, it is not clear if medication effects or differences also vary in the different countries. Luckily, studies with very similar or exact designs as the SOHO study have been conducted in different continents (eg, Intercontinental-SOHO)Citation50 and in Japan.Citation51 The results of those studies are largely consistent. For example, the baseline characteristics of the patients initiated on olanzapine in the SOHO study appear similar to those of the outpatients in the Japanese study in terms of average age (40.0 ± 13.4 and 38.3 ± 13.9 years, respectively), gender (41.1% and 49.6% female), or CGI-SCH global severity in the moderately ill range (3.4 ± 1.0 and 3.0 ± 1.0). In addition, treatment outcomes for outpatients on the core outcome domains in the Japanese study were similar to those observed in the European SOHO study. For example, the percent of patients remaining on treatment for 1 year was 63.8% for the outpatients in the Japanese study and only slightly higher in this study; functional improvement on the EQ-5D VAS score from baseline to endpoint was similar for SOHO participants (change from 45.7 to 65.2) and the outpatient participants in the Japanese study (change from 45.3 to 65.3); percent of participants working for pay at endpoint was almost identical for participants in SOHO (20.3%) and the outpatients in the Japanese study (20.5%).Citation52
Limitations
SOHO is an observational study and several aspects of the study design are worthy of discussion. Firstly, approximately half of the patients started therapy with olanzapine due to the study design (oversampling of the olanzapine cohort). This does not change the observational nature of the study nor does it influence the interpretation of the results because the statistical analysis adjusts for the different sizes of the treatment cohorts. Secondly, assignment to treatment cohort was not random, in that psychiatrists decided which drug to initiate in which patients and at what dose. Importantly, this led to the presence of baseline differences between cohorts. The multivariate analysis employed adjusted for all observed baseline differences between cohorts. Previous research has found that when observational studies have appropriate designs and analysis strategies, comparisons of the findings of randomized controlled trials and observational studies reveal no major differences in the effects of treatments.Citation53,Citation54 An important limitation of the SOHO study is that the assessment by participating psychiatrists was not blind and this could lead to outcome bias in favor of the olanzapine cohort, especially given that the company that produces olanzapine is supporting the study. However, as reported previously, differences between treatment cohorts in physician-rated clinical status (CGI) are accompanied by differences in health-related quality of life, which is a patient self-reported measure and thus observer bias does not seem to have a relevant effect in the SOHO study.Citation54 Finally, in the search for simplicity of assessment, several dimensions of social functioning and the presence of adverse events were measured using single-item questions and may, therefore, have lower sensitivity and precision than specific instruments used to measure adverse events, such as the Simpson-Angus Scale for extrapyramidal symptomsCitation55 or the Abnormal Involuntary Movement Scale.Citation18
The SOHO study has several strengths worth mentioning. Due to its large size, powerful statistical techniques can be used to control for confounding factors. There was a high retention rate in the study, much higher than that seen in randomized controlled trials, where high dropout rates may limit the drawing of firm conclusions. This high retention rate may partly be due to the treatment flexibility allowed, such that physicians could change a patient’s medication and/or dosage as deemed necessary while patients continued to be evaluated. Additionally, there were no protocol-defined clinical reasons to discontinue patients from SOHO. These methodological differences may help to explain why we find differential clinical responses between antipsychotic medications that are not present in randomized clinical trials. Despite the treatment flexibility allowed, we found that at 12 months, the majority of patients were still on the same medication they had started at baseline. Furthermore, we used several outcome measures to represent fully the characteristics of the course of schizophrenia, including response short-term treatment outcomes and remission for long-term treatment outcomes.
Conclusion
This analysis of 12-month data from the large observational SOHO study found that outpatients with schizophrenia who required initiation or a change in their antipsychotic for clinical reasons showed a marked improvement in symptoms, that translated into improvements in their health-related quality of life and in some dimensions of social functioning. The cohorts of patients treated with olanzapine and clozapine tended to have a better clinical course than patients treated with other atypical or typical antipsychotics.
Acknowledgments
The authors thank Sarah Smith for her assistance in editing the paper.
Disclosure
The SOHO study was funded by Eli Lilly and Company. JMH has received economic compensation for his participation on the SOHO advisory board and has acted as consultant or speaker for Astra-Zeneca, Eli Lilly and Lundbeck. JB conducted the statistical analysis of the SOHO study under a contract of Fundació Sant Joan de Déu with Eli Lilly and Company. DN and HA-S are employees of Eli Lilly and Company.
References
- American Psychiatric AssociationPractice guidelines for the treatment of patients with schizophreniaAm J Psychiatry2001154163
- Expert Consensus PanelsThe Expert Consensus Guideline Series: treatment of schizophrenia 1999J Clin Psychiatry199960Suppl 11182
- LehmanAFSteinwachsDMTranslating research into practice: The Schizophrenia Patient Outcomes Research Team (PORT) treatment recommendationsSchizophr Bull1998241109502542
- National Institute for Clinical ExcellenceTechnology appraisal. Guidance No. 43. Guidance on the use of newer (atypical) antipsychotic drugs for the treatment of schizophreniaLondonNICE2002 Available from: http://www.nice.org.uk/nicemedia/live/11786/43628/43628.pdfAccessed July 7, 2011
- ThornlyBAdamsCContent and quality of 2000 controlled trials in schizophrenia over 50 yearsBMJ1998317118111849794850
- HoferAHummerMHuberRKurzMWalchTFleischhackerWWSelection bias in clinical trials with antipsychoticsJ Clin Psychopharmacol20002069970211106145
- RobinsonDWoernerMGPollackSLernersGSubject selection biases in clinical trials: data from a multicenter schizophrenia treatment studyJ Clin Psychopharmacol1996161701768690832
- GeddesJFreemantleNHarrisonPBebbingtonPAtypical antipsychotics in the treatment of schizophrenia: systematic overview and meta-regression analysisBMJ20003211371137611099280
- SchoolerNRTollefsonGDTranPVGheuensJGrebbJAComments on article by Tran and colleagues, ‘Double-blind comparison of olanzapine versus risperidone in treatment of schizophrenia and other psychotic disorders’J Clin Psychopharmacol1998181741799555605
- KasperSKufferleBComments on ‘Double-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disorders’ by Trans and AssociatesJ Clin Psychopharmacol1998183533569690709
- KapurSRemingtonGAtypical antipsychotics: new directions and new challenges in the treatment of schizophreniaAnn Rev Med20015250351711160792
- LeuchtSKomossaKRummel-KlugeCA meta-analysis of head-to-head comparisons of second-generation antipsychotics in the treatment of schizophreniaAm J Psychiatry200916615216319015230
- LeuchtSCorvesCArbterDEngelRRLiCDavisJMSecond-generation versus first-generation antipsychotic drugs for schizophrenia: a meta-analysisLancet20093739657314119058842
- HaroJMEdgellETJonesPBfor SOHO Study Group. The European Schizophrenia Outpatient Health Outcome (SOHO) Study: rationale, methods and recruitmentActa Psychiatr Scand200310722223212580830
- HaroJMEdgellETFrewerPfor SOHO Study GroupThe European Schizophrenia Outpatient Health Outcomes Study: baseline findings across country and treatmentActa Psychiatr Scand2003107Suppl 41619
- HaroJMEdgellENovickDEffectiveness of antipsychotic treatment for schizophrenia: 6-months results of the pan-European Schizophrenia Outpatient Health Outcomes (SOHO) studyActa Psychiatr Scand200511122023115701107
- LambertMHaroJMNovickDOlanzapine versus other antipsychotics in actual outpatient settings: six months tolerability results from the European Schizophrenia Outpatient Health Outcomes (SOHO) studyActa Psychiatr Scand200511123224315701108
- GuyWECDEU Assessment Manual for Psychopharmacology: Revised EditionWashington, DCUS Department of Health, Education, and Welfare1976
- HaroJMKamathSAOchoaSfor the SOHO Study GroupThe Clinical Global Impression-Schizophrenia scale: a simple instrument to measure the diversity of symptoms present in schizophreniaActa Psychiatr Scand2003107Suppl 4161623
- WilliamsAEuroQol – a new facility for the measurement of health-related quality of lifeHealth Policy19901619920810109801
- HaroJMAssessment of remission in schizophrenia with the CGI and CGI-SCH scalesActa Psychiatr Scand200811715617970843
- GardnerDMMurphyALO’DonnellHCentorrinoFBaldessariniRJInternational consensus study of antipsychotic dosingAm J Psychiatry201016768669320360319
- LiebermanJAStroupTSMcEvoyJPfor the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) InvestigatorsEffectiveness of antipsychotic drugs in patients with chronic schizophreniaN Engl J Med20053531209122316172203
- TiihonenJWahlbeckKLönnqvistJEffectiveness of antipsychotic treatments in a nationwide cohort of patients in community care after first hospitalisation due to schizophrenia and schizoaffective disorder: observational follow-up studyBMJ200633322416825203
- PrietoLNovickDSacristanJAfor the SOHO Study GroupA Rasch model analysis to test the cross-cultural validity of the Euro-Qol-5D (EQ-5D) in the Schizophrenia Outpatient Health Outcomes (SOHO) studyActa Psychiatr Scand2003107Suppl 4162429
- PrietoLSacristanJAHormaecheaJAGomezJCEuro-Qol-5D (a generic health-related quality of life measure); psychometric validation in a sample of schizophrenic patientsEur Neuropsychopharmacol200212Suppl 3300
- RevickiDAGendusoLAHamiltonSHGanoczyDBeasleyCMOlanzapine versus haloperidol in the treatment of schizophrenia and other psychotic disorders: quality of life and clinical outcomes of a randomized clinical trialQual Life Res1999841742610474283
- RosenheckRCramerJXuWA comparison of clozapine and haloperidol in hospitalised patients with refractory schizophreniaN Engl J Med19973378098159295240
- HamiltonSHEdgellETRevickiDABreierAFunctional outcomes in schizophrenia: a comparison of olanzapine and haloperidol in a European sampleInt Clin Psychopharmacol20001524525510993126
- TollefsonGDBeasleyCMJrTranPVOlanzapine versus haloperidol in the treatment of schizophrenia, schizoaffective and schizophreniform disorders: results of an international collaboration studyAm J Psychiatry19971544574659090331
- McGorryPDKillackeyELambertMElkinsKLambertTSummary Australian and New Zealand Clinical Practice Guidelines for the treatment of schizophreniaAustralas Psychiatry200311113
- ConleyRRMahmoudRA randomized double-blind study of risperidone and olanzapine in the treatment of schizophrenia or schizoaffective disorderAm J Psychiatry200115876577411329400
- CurranMPPerryCMSpotlight on amisulpride in schizophreniaCNS Drugs20021620721111888341
- CutlerAJGoldsteinJMTumasJARelated dosing and switching strategies for quetiapine fumarateClin Ther20022420922211911552
- SpinaEAvenosoAFacciolaGRelationship between plasma concentrations of clozapine and norclozapine and therapeutic response in patients with schizophrenia resistant to conventional neurolepticsPsychopharmacology2000148838910663421
- LeuchtSPitschel-WalzGAbrahamDKisslingWEfficacy and extrapyramidal side-effects of the new antipsychotics olanzapine, quetiapine, risperidone and sertindole compared to conventional antipsychotics and placebo. A meta-analysis of randomized controlled trialsSchizophr Res19993551689988841
- TarsyDBaldessariniRJTaraziFIEffects of newer antipsychotics on extrapyramidal functionCNS Drugs200216234511772117
- TranPVHamiltonSHKuntzAJDouble-blind comparison of olanzapine versus risperidone in the treatment of schizophrenia and other psychotic disordersJ Clin Psychopharmacol1997174074189315992
- BobesJGarc A-PortillaMPRejasJFrequency of sexual dysfunction and other reproductive side-effects in patients with schizophrenia treated with risperidone, olanzapine, quetiapine, or haloperidol: the results of the EIRE studyJ Sex Marital Ther20032912514712623765
- WiechAHaddadPMAntipsychotic-induced hyperprolactinaemia in women: pathophysiology, severity and consequences. Selective literature reviewBr J Psychiatry200318219920412611781
- DavidSRTaylorCCKinonBJBreierAThe effects of olanzapine, risperidone, and haloperidol on plasma prolactin levels in patients with schizophreniaClin Ther2000221085109611048906
- TurronePKapurSSeemanMVFlintAJElevation of prolactin levels by atypical antipsychoticsAm J Psychiatry200215913313511772702
- AronneLJEpidemiology, morbidity, and treatment of overweight and obesityJ Clin Psychiatry200162Suppl 23132211603881
- SussmanNThe implications of weight changes with antipsychotic treatmentJ Clin Psychopharmacol200323Suppl 1S21S2612832946
- McIntyreRSManciniDABasileVSMechanisms of antipsychotic-induced weight gainJ Clin Psychiatry200162Suppl 23232911603882
- AllisonDBMackellJAMcDonnellDDThe impact of weight gain on quality of life among persons with schizophreniaPsychiatr Serv20035456556712663847
- AllisonDBMentoreJLHeoMAntipsychotic-induced weight gain: a comprehensive research synthesisAm J Psychiatry19991561686169610553730
- BasileVSMasellisMMcintyreRSMeltzerHYLiebermanJAKennedyJLGenetic dissection of atypical antipsychotic-induced weight gain: novel preliminary data on the pharmacogenetic puzzleJ Clin Psychiatry200162Suppl 23456611603885
- LeffJSartoriusNJablenskyAKortenAErnbergGThe International Pilot Study of Schizophrenia: five-year follow-up findingsPsychol Med1992221311451574549
- DossenbachMErolAel Mahfoud KessaciMfor the IC-SOHO Study GroupEffectiveness of antipsychotic treatments for schizophrenia: interim 6-month analysis from a prospective observational study (IC-SOHO) comparing olanzapine, quetiapine, risperidone, and haloperidolJ Clin Psychiatry20046531232115096069
- Ascher-SvanumHYeWFlynnJFujikoshiSNakaharaNTakahashiMClinical and functional outcomes for patients with schizophrenia treated with olanzapine: One-year naturalistic outcomes for inpatients and outpatients in JapanClin Neuropsychopharmacol Ther201124555
- Ascher-SvanumHYeWFlynnJNakaharaNTakahashiMClinical and functional outcomes in the naturalistic treatment of inpatients and outpatients with schizophrenia in JapanPresented at the 164th Annual Meeting of the American Psychiatric AssociationMay 14–18, 2011Honolulu, HI
- ConcatoJShahNHorwitzRIRandomized, controlled trials, observational studies, and the hierarchy of research designsN Engl J Med20003421887189210861325
- HaroJMKontodimasSNegrinMARatcliffeMSuarezDWindmeijerFMethodological aspects in the assessment of treatment effects in observational health outcomes studiesAppl Health Econ Health Policy20065112516774289
- SimpsonGMAngusJWSA rating scale for extrapyramidal side effectsActa Psychiatr Scand Suppl197021211194917967