
Abstract
Background
There is a well-known problem in hypertension care with patients’ adherence to treatment. Patients who score high in answering the instrument Satisfaction with Information about Medicine Scale are reported to have greater adherence to their medication.
Aim
To explore how hypertensive patients’ satisfaction with information about their medicines was affected by nurses’ education in Motivational Interviewing.
Material and methods
The Stages of Change model and Motivational Interviewing was the theoretical base for consultation training for nurses. Nineteen nurses attended 3 days of video-recorded consultation training with simulated patients. They were updated in hypertensive medication and were trained in motivating patients to improve their self-management as well as adherence to lifestyle changes and medication. The satisfaction with information instrument identifies patients’ satisfaction with information about the action and usage of medication as well as potential problems with it. The instrument was used to assess how well the needs of individual patients for medicine information were met at baseline and 2 years after the training. The 19 trained nurses in the intervention group worked with 137 patients, and a control group of 16 nurses, who gave normal care, worked with 51 patients.
Results
There was a difference between the intervention and control group in total score (P=0.028) 2 years after the intervention. Patients in the intervention group perceived higher satisfaction with the action and usage of their medication (P=0.001) and a lower degree of potential problems with their medication (P=0.001). Patients in the control group also perceived a lower degree of potential problems with their medication (P=0.028).
Conclusion
We suggest that consultation training for nurses with the aim of motivating patients to be more self-directed in their self-care improves satisfaction with information about medication.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Background
Decades of research have highlighted the importance of adherence to antihypertensive medication for decreasing cardiovascular risk of high blood pressure.Citation1–Citation3 Besides the importance of suitable antihypertensive therapy, the result of the therapeutic regimen is affected by socioeconomic factors, lifestyle, and associated comorbidity.Citation4 Furthermore, as hypertension is a long-term condition, and as the patients manage the regimen by themselves, patient participation and satisfaction with and understanding of the regimen may be critical for the outcome of the care. To achieve concordance, ie, a mutual understanding of the need for medication, health providers need to understand patient information needs regarding the medicines prescribed.Citation5
We conducted a 3-day residential training course to increase patient-centeredness by the use of motivational interviewing (MI),Citation6 the Stages of Change (SOC) model,Citation7 and guidelines for cardiovascular prevention.Citation8 In the randomized controlled study, 212 patients and 35 nurses participated. The beneficial effects of the consultation training on blood pressure controlCitation9 emphasized the importance of consultation training and the use of behavioral models in motivating patients to adhere to treatment.
The interrelationship between patient-centeredness and satisfaction with care has recently been outlined by Ferguson et al.Citation10 Patients want more information on potential drug-related problems.Citation11 With the use of the instrument Satisfaction with Information about Medicine Scale (SIMS), the patients with a variety of diseases reported increased adherence to their medication.Citation12 The 826 patients were recruited from anticoagulant, asthma and diabetic, cardiac rehabilitation, and oncology outpatient clinics, and from cardiac and general medical wards. The patients at the cardiac rehabilitation clinic reported a positive correlation with reported adherence to anticholesterol medicines (P<0.05); the higher the score on the SIMS, the greater the adherence to their medicines.
Aim
The purpose of the study was to explore how hypertensive patients’ satisfaction with information about their medicines was affected by nurses’ education in patient-centeredness.
Subjects and methods
Nurses were recruited for the study from a register of all nurses who were members of the Swedish Hypertension Society and from a register of all nurse-led hypertension clinics at health centers in Sweden. They were randomly allocated to the intervention group (IG) (n=19) or control group (CG) (n=16). Only one nurse was recruited from each health center. During the winter of 2003 and 2004, the residential multifactorial educationCitation13 was held for 3 days. The nurses in the intervention group were educated in the SOC model,Citation7 MICitation6 with patient-centeredness (),Citation14 and applying guidelines for cardiovascular prevention,Citation8 lifestyle factors, and pharmacological treatment.Citation15 Simulated patients were used in the video-recorded role-play where the nurses practiced their consultation technique. The recordings were reviewed in small groups with supervision of the research team (ED, AB, KIK). The nurses only had this training once. The results of the consultation training on nurses’ communication with patients have previously been reported.Citation9,Citation14,Citation16,Citation17 Patients in the CG received normal care. The patient inclusion criteria were: hypertensive patients consulting nurses at health centers; men and women aged <75 years; systolic blood pressure ≥160 mmHg and/or diastolic blood pressure ≥90 mmHg; body mass index ≥25 kg/m2; serum cholesterol ≥6.5 mmol/L and/or serum triglycerides ≥2.3 mmol/L; and not reporting regular physical activity. The trained nurses in the IG worked with 153 patients, and only 60 patients were worked with in the CG, although the inclusion period lasted for 4 years. The decision to stop the inclusion period was taken after a new power analysis was performed. As the amount of eligible hypertensive patients at the health centers differed greatly, the nurses worked with one to 14 patients each. There were no statistical differences between the groups at baseline except for systolic blood pressure (IG: 159.1 mmHg [standard deviation: 16.57] versus CG: 167.0 mmHg [standard deviation: 17.59], P<0.01). In the statistical analyses, patients were only included if they had complete data, collected from all three measurements at baseline, after 1 year, and after 2 years. Reasons for loss at follow-up are presented in .
Figure 1 Flow diagram of patients.
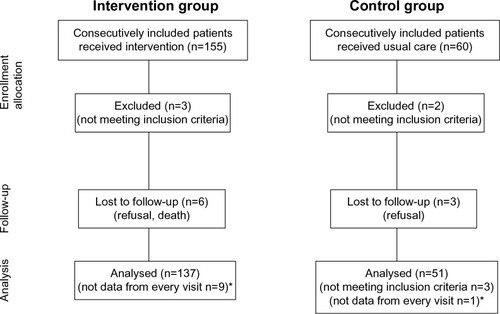
Table 1 Description of every part of patient-centeredness
The validated instrument, SIMS,Citation12 was chosen as patients scoring high in answering it have greater adherence to their medication. Adherence to medication is of great importance in hypertension care to help the patients achieve blood pressure control. The intervention with consultation training, amongst other patient-centeredness interventions, was used with the aim of helping the nurses to individualize their counseling with their patients, which was expected to increase adherence to both medication and change of lifestyle. The instrument contains two subscales: patients’ satisfaction with information about the action and usage of their medication (items 1–9) and the potential problems of medication (items 10–17) (). Examples of questions were “Have you received information about your medicine?”, questions regarding “what it is called”, “how it works”, “whether the medicine has any side effects”, and “what you should do if you forget to take a dose”. The patients were asked to rate the amount of information they had received for all 17 items using the alternatives “too much”, “about right”, “too little”, “none received”, or “none needed”. The alternatives “about right” and “none needed” were given a score of 1, and the rest of the alternatives were given a score of 0. This means that a high score indicate a high degree of overall satisfaction with the amount of information received according to Horne et al.Citation12 Besides analyzing each subscale one by one, a total satisfaction rating was made. The Cronbach’s alpha coefficients of items 1–9 was 0.92 and of items 10–17 was 0.91. Questions were added to the instrument about where the patients had received their information () and how useful they found it. For the latter question, the patient could choose the alternatives “very useful”, “useful”, “fairly useful”, “not useful”, or “don’t know”.
Table 2 The items of the Satisfaction with Information about Medicine Scale instrument
Table 3 Added questions about where the patient had received information from
Statistics
Due to the ordinal character of the SIMS scale, nonparametric statistical methods were applied. For comparison of SIMS values at baseline and 2-year follow-up between IG and CG, the Mann–Whitney U-test was used. For comparisons within each group between baseline and follow-up at 2 years, the Wilcoxon signed rank test was used. The same statistical methods were applied to analyze sex differences. Cronbach’s alpha was calculated for each of the subscales in SIMS.
Ethics
The study adhered to the principles outlined in the Declaration of Helsinki and was approved by the Local Ethics Committee at the Faculty of Medicine, University of Gothenburg, Sweden (Ö363-00).
Results
There were 137 and 51 patients in the IG and CG, respectively, who completed the questionnaire at baseline and at follow-up at 1 and 2 years. There was a significant increase (P<0.001) in the SIMS score in the IG from baseline to the 2-years follow-up both in part 1 (information about the action and usage of medication) and in part 2 (information about potential problems of medication), as well as for the total score (). A significant difference between the IG and CG could be seen in part 2 (P=0.037) and in the total score (P=0.028) after 2 years. Where the patients had received their information about their medicines and how useful the information was at the 2-year follow-up is presented in . Most often, information was received from the pharmacy and from physicians and nurses at hospitals and health centers. Besides information from the pharmacy, the information from the nurses was the most useful.
Table 4 Overview of the results of the patients’ answers to the Satisfaction with Information about Medicine Scale instrument part 1 (information about the action and usage of medication), part 2 (information about potential problems of medication), and the total of the scores
Table 5 The patients’ answers to where they had received their information about their medicines and how useful the information was at the two year follow-up
Patients in the CG found the information from family or friends and medical books useful or very useful to a greater extent (>10%) than patients in the IG. Furthermore, patients in the IG found the information from other people with the same disease, family or friends, and helping organization to be not useful to a greater extent (>10%) than patients in the CG.
Discussion
The patients in the IG significantly increased their satisfaction with information about the action and usage of their medication as well as for potential problems of the medication from baseline to the 2-year follow-up, and did so significantly more so than patients in the CG. The information from nurses, physicians, and the pharmacy was the most useful as reported by the patients. Patients in the CG thought that the information they had from certain people or institutions was more useful than did patients in the IG. Furthermore, the patients in the IG were more negative regarding the usefulness of information from people with the same disease, family or friends, helping organization, and medical books compared to the patients in the CG.
The SIMS instrument has not been used in research to any great extent. For that reason, we do not have many other results to relate to. Another limitation of our study is that the results apply to the 2-year follow-up, but we do not know how long the effect of the intervention persists. On the other hand, the MI intervention means that the patient should follow behavior that is induced of their own free will and, therefore, will persist more than if they behave at someone else’s demand.Citation6 For that reason we assume that the behavior of adherence to medication will be maintained. Another factor is that we do not know how well the nurses performed their counseling during the years after the one-time training.
After being counseled by educated nurses during the 2-year study period, the patients in the IG had higher scores in the SIMS instrument than patients in the CG. The reason why they scored higher, we assume, is that these patients became more secure and independent regarding their medication. The training was intended to help the nurses in the patient-centered counseling to make their patients more competent in taking care of themselves. This means that taking medicines is a kind of self-care that the patients exercised.Citation18 Feeling competent and independent may then have had the result that these patients perceived that they were content with the information they had received from the health care providers. For that reason, they needed less information from other sources than patients in the CG.
We can compare the results from this study with how the same patients scored high in the Exercise of Self Care Agency instrument.Citation19 Scoring high in the Exercise of Self Care Agency instrument means that you value your health and take care of yourself. A natural conclusion of this is that patients who value their health and take care of themselves include adherence to their medication in these strategies, which helps the hypertensive patient to maintain controlled blood pressure. This is confirmed in our earlier results, which showed that, after 2 years, 52.6% of the patients in the IG reached the target of ≤140/90 mmHg compared with 39.2% in the CG.Citation9
Patients in the IG felt reassured by the information provided by their nurses, physicians, and the pharmacy, and thought generally that other sources for information about their medicines were less useful than did the patients in the CG. The patients in the CG appreciated these sources too, but they thought other sources, eg, family and friends, helping organizations, and people with the same disease, were useful too and did not distance themselves from these other sources to the same extent as the patients in the IG did. This is confirmed with the negative answers about what was perceived as less/not useful for both groups. The information available from these other sources is, perhaps, not always accurate or up-to-date, which, for the patients in the CG, might imply that they did not have the same opportunity to perform their self-care; in other words, they did not have the same opportunity to adhere to their medication as the patients in the IG. This applies not just to the patients in the CG as all patients have the right to, and also want to, have information about their medication.Citation11 Furthermore, all patients, without any exceptions, benefit from having controlled blood pressure.Citation2 Moreover, we may presume that there was a difference in the quality of information that was given to the patients in the CG compared to the patients in the IG due to the training these nurses had had.
As the patients in the IG had higher SIMS score than the patients in the CG, we may assume that their nurses talked about the patients’ medication to a greater extent or in another way than the nurses in the CG. From this we can draw the conclusion that training of nurses in MI and the SOC model in order to be able to communicate information in a comprehensive manner is very important and even crucial for patients in improving adherence to medication. This was exemplified in a meta-analysis on effects of MI used with patients in primary care,Citation20 and was further confirmed in another meta-analysis specifically studying cognitive-based behavior-change techniques.Citation21 Whether or not our results are valid for patients with other cardiovascular disorders or other diseases in other contexts is a subject for further research.
Conclusion
We suggest that consultation training for nurses with the aim of motivating patients to be more self-directed in care improves satisfaction with medication.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in either drafting the article or revising it critically for important intellectual content; and gave final approval of the version to be published.
Acknowledgments
This work has been supported by the Swedish Research Council (K2003-27VX-14636-01A), the Swedish Heart and Lung Foundation, Pfizer AB, the Swedish Society of Hypertension and Institute of Health and Care Sciences, The Sahlgrenska Academy, University of Gothenburg. The authors wish to thank Inger Norvinsdotter Borg for coordinating the activities on the residential courses, and all participating nurses and patients.
Disclosure
The authors report no conflicts of interest in this work.
References
- CorraoGParodiANicotraFBetter compliance to antihypertensive medications reduces cardiovascular riskJ Hypertens201129361061821157368
- HerttuaKTabakAGMartikainenPVahteraJKivimakiMAdherence to antihypertensive therapy prior to the first presentation of stroke in hypertensive adults: population-based studyEur Heart J201334382933293923861328
- CollinsRPetoRMacMahonSBlood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: overview of randomised drug trials in their epidemiological contextLancet199033586938278381969567
- ArmarioPWaeberBTherapeutic strategies to improve control of hypertensionJ Hypertens201331Suppl 1S9S1223389085
- EkmanISchaufelbergerMKjellgrenKISwedbergKGrangerBBStandard medication information is not enough: poor concordance of patient and nurse perceptionsJ Adv Nurs200760218118617877565
- RollnickSMasonPButlerCHealth Behavior Change: a Guide for PractitionersPhiladelphiaChurchill Livingstone2002
- ProchaskaJOReddingCAEversKEThe transtheoretical model and stages of changeGlanzKRimerBKViswanathKHealth behavior and health education: theory, research, and practice4th edSan FranciscoJossey-Bass200897122
- ManciaGDe BackerGDominiczakA2007 ESH-ESC Guidelines for the management of arterial hypertension: the task force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)Blood Press200716313523217846925
- DrevenhornEBengtsonANilssonPMNybergPKjellgrenKIConsultation training of nurses for cardiovascular prevention – a randomised study of two years durationBlood Press201221529329922545932
- FergusonLMWardHCardSSheppardSMcMurtryJPutting the ‘patient’ back into patient-centred care: an education perspectiveNurse Educ Pract201313428328723602696
- MahlerCJankSHermannKHaefeliWESzecsenyiJInformation on medications – How do chronically ill patients assess counselling on drugs in general practice?Dtsch Med Wochenschr20091343316201624 German19650022
- HorneRHankinsMJenkinsRThe Satisfaction with Information about Medicines Scale (SIMS): a new measurement tool for audit and researchQual Health Care200110313514011533420
- BosworthHBOlsenMKNearyATake Control of Your Blood Pressure (TCYB) study: a multifactorial tailored behavioral and educational intervention for achieving blood pressure controlPatient Educ Couns200870333834718164894
- DrevenhornEBengtsonAAllenJKSäljöRKjellgrenKIA content analysis of patient centredness in hypertension care after consultation training for nursesThe Internet Journal of Advanced Nursing Practice2007821
- GlynnLGMurphyAWSmithSMSchroederKFaheyTInterventions used to improve control of blood pressure in patients with hypertensionCochrane Database Syst Rev20103CD00518220238338
- DrevenhornEBengtsonAAllenJKSäljöRKjellgrenKICounselling on lifestyle factors in hypertension care after training on the Stages of Change modelEur J Cardiovasc Nurs200761465316698320
- DrevenhornEBengtsonAKjellgrenKIEvaluation of consultation training in hypertension careEur J Cardiovasc Nurs20098534935419744889
- EldhACEkmanIEhnforsMConditions for patient participation and non-participation in health careNurs Ethics200613550351416961114
- DrevenhornEBengtsonANybergPKjellgrenKIHypertensive patients’ exercise of self-care agency after consultation training of nursesJ Am Acad Nurse Pract2014
- VanBuskirkKAWetherellJLMotivational interviewing with primary care populations: a systematic review and meta-analysisJ Behav Med Epub8112013
- EasthallCSongFBhattacharyaDA meta-analysis of cognitive-based behaviour change techniques as interventions to improve medication adherenceBMJ Open201338