
Abstract
Background
There is a need to evaluate the professionals’ perception about the consequences of the lack of therapeutic adherence in the evolution of patients with co-occurring disorders.
Methods
An online survey, released on the Socidrogalcohol [Spanish Scientific Society for Research on Alcohol, Alcoholism and other Drug Addictions] and Sociedad Española de Patología Dual [the Spanish Society of Dual Pathology] web pages, was answered by 250 professionals who work in different types of Spanish health centers where dual diagnosis patients are assisted.
Results
Most professionals perceived the existence of noncompliance among dual diagnosis patients. Almost all of these professionals (99%) perceived that noncompliance leads to a worsening of the progression of the patient’s disorder, in both the exacerbation of mental disorders and the consumption of addictive substances. Most of the professionals (69.2%) considered therapeutic alliance as the main aspect to take into account to improve the prognosis in this population. The primary purpose of treatment must be the improvement of psychotic-phase positive symptoms, followed by the control of behavior disorders, reduction of craving, improvement of social and personal performances, and reduction of psychotic-phase negative symptoms.
Conclusion
Most professionals perceived low adherence among dual diagnosis patients. This lack of adherence is associated with a worsening of their disease evolution, which is reflected in exacerbations of the psychopathology and relapse in substance use. Therefore, we propose to identify strategies to improve adherence.
Introduction
Dual disorders (DDs)/dual pathology/co-occurring disorders are the terms commonly accepted within the mental health field to refer to patients suffering from an addictive disorder and other mental disorders. DDs can occur simultaneously or, even more importantly, sequentially throughout their life spanCitation1–Citation4 and constitute a serious problem for the public health.Citation5,Citation6
Up to 70% of individuals who have been diagnosed with a substance use disorder (SUD) show a lifetime disorder, that is, a second psychiatric diagnosis throughout their life,Citation7 and 50% of the patients diagnosed with a mental disorder have a history of substance use.Citation8–Citation11 In Spain, the prevalence rate of population with a mental disorder associated with SUD ranges between 25% and 70%.Citation12–Citation14 This percentage varies depending on the research methodology and, especially, the health care center where the study was conducted.Citation15,Citation16
Lifetime diagnoses of any mental disorder, and particularly personality disorders and psychotic disorders, were found to be associated with higher prevalence of transition from substance use to SUDs across most categories of substances.Citation17
This prevalence is higher when tobacco is included and is considered a potentially addictive substance.Citation9 Moreover, even though it is widely accepted that the prevalence of DDs is significantly higher in men,Citation18 the increasingly high number of diagnosed females in SUD treatment unitsCitation19 has raised controversy.Citation20
Underreporting of substance use is common in individuals with severe psychiatric disorders,Citation19 and the majority of the studies that have investigated this did not include tobacco.
The dual diagnosis patients’ level of insight (patient’s awareness) of their psychotic disorder, as occurs with SUD, is low.Citation21 Furthermore, the lack of insight is independent of the used substance, whether it is alcohol, which is used very frequently,Citation11,Citation22 cocaine,Citation23 or cannabis.Citation24 Low insight and high polymedicationCitation25 are the main causes of low therapeutic adherence, particularly in patients with psychosis,Citation26–Citation28 increasing the suicide risk.Citation29 There is evidence of the relationship between a patient’s level of insight of his/her disorder and treatment compliance.Citation30,Citation31
A study conducted by Roncero et alCitation27 about health care professionals’ perception suggests that ~70% of dual diagnosis patients do not properly comply with their treatment. This percentage is significantly higher than that observed in patients diagnosed with only one mental disorder,Citation32,Citation33 whereas treatment adherence must be improved.Citation34 Furthermore, the lack of adherence results in negative prognostic implications,Citation35,Citation36 which are even more significant in the dual diagnosis population than in other populations with other mental disorders.Citation37
There are limited health resources for the approach to DDs in Spain, which confirms the need for additional efforts and strategies for the treatment of individuals suffering from comorbid disorders.Citation38,Citation39 Among other aspects, there is a need for the creation of a register with clear information on the resources available for this group of patients in Spain,Citation40 as well as the enhancement of nonpharmacologic therapies.Citation41,Citation42
Few studies exist on the perception of the management of pharmacological treatment, where different health professionalsCitation27 or specific groups of professionals who assist patients suffering from mental disordersCitation43,Citation44 or DD patientsCitation45 are included. Nevertheless, information on professionals’ attitude and perception is an important factor to improve the management of schizophrenic or dual diagnosis patientsCitation43,Citation46 and may also help to improve the negative prognostic implications that are a consequence of noncompliance, optimize the implementation of health and social resources, and produce consensus and protocols to manage this population.Citation12,Citation35
The aims of the present study are the evaluation of Spanish professionals’ perception about the level of compliance, the factors affecting prognosis and therapeutic adherence, the rate of use of different pharmacologic strategies, and the training of our professionals in this field. Thus, we can expect a perception of low adherence among the participants and also low awareness of the negative consequences associated with noncompliance among the affected patients. On this basis, the recommendation of specific strategies to improve this situation can be developed.
Methodology
Study design
After a thorough review of the literature, a group of clinical and academic experts on DDs () designed a survey on adherence and the consequences of therapeutic noncompliance in dual diagnosis (annexed survey).
Table 1 List of clinical and academic experts on DDs
This online survey, which was open to any professional involved in dual diagnosis assistance who wanted to participate, was made available through the institutional websites of two scientific societies (the Spanish Society of Dual Pathology [SEPD]; www.patologiadual.es and the Spanish Scientific Society for Research on Alcohol, Alcoholism and other Drug Addic tions [Sociodrogalcohol]; http://www.socidrogalcohol.org) and was answered between October 1, 2013 and December 31, 2013.
Sample
The survey was answered by 250 professionals from the following care centers: outpatient drug clinics (47.2%), mental health centers (25.2%), psychiatric hospitalization units (11.2%), inpatient drug addiction units (7.2%), private centers (6.8%), and primary care centers (2.4%).
Most of the professionals (68.3%) who participated in the survey were members of scientific societies, mainly the SEPD (56.6%) and Socidrogalcohol (20.1%). A total of 54.0% of the participants were women, and 90.0% were Spaniards. Most participants (60.0%) were older than 45 years.
In all, 57.2% of the total number of participants had >15 years of clinical experience. Most of the professionals (67.2%) were working in specialized addiction care units when participating in the survey ().
Table 2 Professionals who participated in the survey
This study included professionals from every Spanish regions (autonomous communities) except Cantabria and the autonomous cities of Ceuta and Melilla. The communities with a higher number of participants were Andalucía, Madrid, and Catalonia ().
Table 3 Percentage of participants in different communities
The 250 participants included in the survey did not receive any economic compensation for completing the questionnaire.
The questionnaire consisted of 41 questions distributed in eight sections: participant sociodemographic profile (nine questions), prevalence (one question), prognosis improvement and therapeutic goals (two questions), use of substances (one question), disease acknowledgment (three questions), therapeutic adherence (six questions), professional continuing education (two questions), and pharmacological strategies (16 questions). The section on pharmacological strategies included seven subsections: psychopharmacologic groups and multiple therapies (three questions), use of antipsychotics (six questions), use of anticonvulsive euthymic drugs (one question), use of antidepressant drugs (one question), use of modulators of the endogenous opioid system (one question), use of benzodiazepines (three questions), and polymedication (one question).
In 15 questions – excluding the eleven questions aimed to define the sociodemographic profiles – the professionals were asked to sort the answers proposed by the researchers on the basis of their importance or frequency of use. A total of 19 questions were responded employing different intervals using Likert scales.
Data analysis
With the requested information, a descriptive statistical analysis was performed using the SPSS Version18 statistical software (SPSS Inc., Chicago, IL, USA).
Results
The 250 survey participants perceived that 40.2% of the patients in their practice are affected with DDs ().
Table 4 Patients with dual pathology
Prognosis improvement
The participants considered that therapeutic alliance is the main aspect to take into account to improve this population’s prognosis (69.2%), followed by proper and maintained compliance (66.0%), patient’s disease awareness (59.2%), and family support (52.4%; ).
Table 5 Important variables in the prognosis of a dual pathology patient (according to the perceptions of the professionals surveyed)
Therapeutic goals
The results of the questionnaire showed that, in the participants’ opinion, the primary treatment goal must be the improvement of the psychotic-phase positive symptoms, followed by the control of behavior disorders, reduction of craving, improvement of social and personal performances, and reduction of psychotic-phase negative symptoms ().
Table 6 Importance of therapeutic targets
Abuse/addiction substances for which treatment is demanded
In the participants’ opinion, alcohol is the substance mostly used by dual diagnosis patients, followed by cocaine, cannabis, benzodiazepines, heroine, and different psycho-stimulants, such as 3,4-methylenedioxymethamphetamine and methamphetamines, among others ().
Table 7 Substances of abuse/dependence that demand treatment
Level of disease awareness
In all, 96.0% of the participants in the survey considered that patients have a deficient level of awareness (insight) of their psychotic disease. Moreover, 87.2% of the experts also considered that patients have a deficient level of awareness of addictive diseases and only 10.8% believed that patients are aware of the negative effect of the use of substances on their dual diagnosis ().
Table 8 Degree of awareness (according to the perceptions of the professionals surveyed)
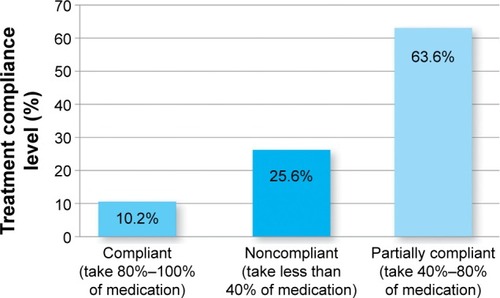
Treatment compliance
Based on international recommendations,Citation36 a patient is defined as “compliant” when taking ≥80% of their medication, “partially compliant” when the intake of medication is between 40% and 80%, and “noncompliant” when they take <40% of the prescribed treatment. In this respect, 10.8% of the participants stated that their patients are compliant, 63.3% that their patients are partially compliant, and 25.6% that their patients are noncompliant ().
Figure 1 Level of treatment compliance.
Hindering pharmacological factors for therapeutic adherence
Regarding the professionals’ clinical experience, the outcomes showed that the association of side effects to the intake of psychiatric drugs is the main explanation for the lack of adherence in this group of patients ( and ).
Figure 2 Common consequences of therapeutic noncompliance.
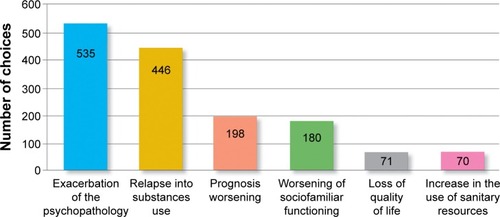
Table 9 Pharmacological factors that hinder treatment adherence
Nonpharmacological strategies for adherence improvement
Most professionals (73.5%) affirmed that they are certainly satisfied with the outcomes of the nonpharmacological strategies implemented in their dual diagnosis patients. Moreover, the implementation of motivational strategies and psychoeducation for the patient and family are considered the most important nonpharmacological strategies ().
Table 10 Nonpharmacological strategies that favor treatment adherence (according to the perceptions of the professionals surveyed)
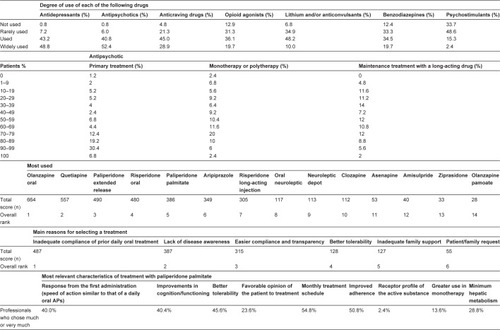
Use of pharmacological treatments
The most frequently used drugs for the treatment of dual diagnosis patients are antipsychotics, “commonly used” or “widely used” in 93.2% of the patients; antidepressants (92.0%); and anticraving drugs (73.9%).
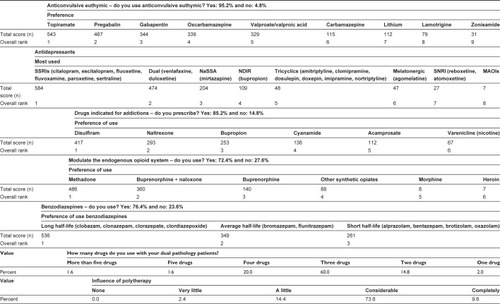
In this context, in the participants’ opinion, 2.0% of the patients receive just one drug, as the more common treatment is polymedication. Most of these patients receive a total of three drugs, although almost 25% of the professionals confirmed that they receive four or more different drugs. This is worth highlighting, since polytherapy significantly affects –“very much” according to 73.6% of the surveyed participants and “completely” according to 9.6% of the surveyed participants – the patients’ quality of life ().
Figure 3 Treatment of your patients with dual pathology.
Consequences of therapeutic noncompliance
The vast majority of the participants in the survey (98.8%) perceived that therapeutic noncompliance worsened the overall course of dual diagnosis patients ().
Table 11 Degree of deterioration due to therapeutic noncompliance (according to the perceptions of the professionals surveyed)
Professionals’ educational background
The most valued training resources were the courses (60.0%), workshops (54.8%), and guidelines (47.2%; ).
Table 12 Tools to improve professional development
Discussion
Knowing the perception of professionals is very important since, as they are responsible for prescribing and administering the treatment, as well as for the drug efficiency,Citation43,Citation47 they are able to detect noncompliant patients and the consequences resulting from their lack of adherence. Thus, they can also identify the necessary interventions to improve this situation.
Professionals perceived that 40.2% of the patients cared for in different health care settings are affected with DDs. This prevalence is lower than that detected by epidemiologic studies, extending the debate on the underdiagnosis of this disease. In this evaluation, professionals did not usually take into account tobacco, which is also a controversial matter in this field. Nevertheless, the prevalence of DDs may possibly depend on the health care setting where the study is carried out, varying from 24.9% in psychiatric hospitalization unitsCitation13 and 40% in emergency unitsCitation34 to 56%–67% in addiction treatment units.Citation14,Citation15 Moreover, the survey results also showed alcohol and cocaine, to a lesser degree, as the most used drugs by the DD patients. These data coincide with the studies conducted without including the evaluation of tobacco.Citation7,Citation16,Citation18
Professionals’ perception on the main therapeutic goals to be achieved to manage dual diagnosis patients should be the improvement of the psychotic-phase positive symptoms, control of behavior disorders, and reduction of craving. These are very important aims, as established by a large number of articles published in the literature.Citation48–Citation50
In the CATIE study,Citation51 60% of the psychotic patients suffered from SUD sometime in their life, without mention of tobacco. Regardless of the accessibility to health care resources, DD patients present a lower degree of therapeutic adherence than those who have been diagnosed with just one mental disorder.Citation35 This coincides with the participants’ perception, which shows that 89.2% of these patients are totally or partially noncompliant. This rate is superior to that observed (68.3%) in previous similar studies carried out in SpainCitation27 with different professionals and in international studies developed exclusively with psychiatrists, varying between 53%Citation43 and 57%.Citation44
Participants adduce the occurrence of adverse effects as the main pharmacologic factor to explain for the low rate of compliance. Likewise, a similar perception is observed when analyzing the patients’Citation52 and professionals’Citation43 opinions. Based on this perception, as concluded in the study performed by Ziedonis et al,Citation42 those drugs that may contribute to poor adherence due to their adverse effects should be avoided. Moreover, regarding the rest of the pharmacologic factors that affect compliance, professionals pointed out the inefficacy in controlling the symptoms and the complexity of some treatment regimens. It should be taken into account that DD patients are often a polymedicated population,Citation25 and in most cases, they receive two or more antipsychotic drugs.Citation53 Therefore, in the professionals’ opinion, the prescription of single-dose regimens should be recommended.Citation27 However, in this study, 98% of the professionals treat their patients with more than one drug and 83.2% with three or more drugs, whereas three is the average number of drugs received by each patient. This is a very important finding, since the majority of the survey respondents perceived that polymedication influences – in varying degrees, “much” or “completely” for 83.2% of the sample – the patients’ quality of life, which is in line with evidence found in the literature.Citation54
Likewise, all participants perceived, as evidenced in numerous studies,Citation55–Citation57 that nonadherence to treatment determines worse evolution in the prognosis of dual diagnosis patients, very significant in up to 98.8% of the cases. This is a similar finding to that observed in the study performed by Roncero et al,Citation27 in which 96.2% of the participants considered that noncompliance is severely or very severely related to poor patient evolution.Citation27 There is a large number of studies that verify that the lack of adherence is directly associated with a worsening of the disorder’s evolution.Citation37,Citation58 It should be taken into account that the population affected with severe mental disorders and SUD presents more severe symptoms of the psychopathology and a higher rate of hospitalization, relapse, violence, and suicideCitation29 (in short, a worse evolution of the disease) than patients with only one diagnosis.Citation58,Citation59 In this context, the participants in this study considered that the worsening of the prognosis is the third most important consequence of noncompliance, only surpassed by an exacerbation of the psychopathology and relapse to substance use.
The difficulties involved in guaranteeing treatment continuity entail a nonnegligible risk of psychopathologic decompensations as well as behavioral ones in DD patients.Citation60 This risk together with the relapse in substance consumption is relevant, as shown by several researchers.Citation61–Citation63 Nonetheless, in the literature, few objective studies have been conducted on the lack of adherence, whereas we cannot know which one of these is the most frequent. This finding was already detected in a previous study performed by Roncero et al,Citation27 in which it was not possible to elucidate whether psychopathologic decompensation is more frequent than relapse in SUD or vice versa.
Noncompliance also involves a worsening of social and family functioning,Citation64 loss in quality of life,Citation65 and an increase in the use of public and private health resources, especially hospitalizations.Citation66 These three situations are considered the fourth, fifth, and sixth most important consequences related to the lack of adherence found in our survey.
To improve patients’ prognosis, the participants mainly assessed the need for therapeutic alliance – 69.2% of the participants. This percentage coincides with the research that concluded that establishing a relationship of cooperation between the patient and professional facilitates the achievement of the therapeutic goals.Citation67,Citation68 They also assessed the need for treatment adherence (66.0%) and patient awareness (insight) of the disease (59.2%). The latter is correlated with the evolution of the disease and also with the level of compliance.Citation69,Citation70 However, only 4% of the professionals perceived that they are well aware of their patients’ psychotic disease, a consideration that in the case of SUD is shared by 12.8% of the professionals. In addition, according to their clinicians’ perception, only 10.8% of the patients are aware of the damage that the use of substances can produce on their psychotic illness. In European studies,Citation43,Citation44 this percentage is 25%.
The survey results also showed the high degree of satisfaction of the professionals with nonpharmacological strategies, emphasizing interventions aimed to optimizing the patient’s level of adherence, motivational strategies, as well as patient and family psychoeducation; interventions with a clearly established efficacy as evidenced by several investigations.Citation71,Citation72 In this context, however, it should be taken into account that between 20% and 70% of the patients who start psychosocial therapies in mental health services do not properly comply with them.Citation73
In relation to different pharmacologic therapies, antipsychotics, antidepressants, and the so-called anticraving drugs are the mostly used. This finding is similar to the results observed in a study conducted in Spain.Citation20 It should be remembered that, in the participants’ opinion, the therapeutic goals in this population should include the management of psychotic symptoms as well as decrease of craving. This also coincides with several studies that concluded that the approach to dual diagnosis patients requires combination therapy for addictive behavior and other mental disorders.Citation35,Citation74 It is not in vain that, among other aspects, the remission of substance dependence or abuse is a critical factor for the proper management of mental disease symptoms.Citation75
The findings of this survey also showed that professionals prefer using atypical antipsychotics to the detriment of conventional neuroleptics, a tendency supported by the efficacy of atypical antipsychotics in the approach to dual diagnosis,Citation76–Citation78 which is significantly higher than the efficacy observed with classical neuroleptics.Citation75,Citation79 Moreover, whereas most patients receive antipsychotic polytherapy, in practically half of the cases, professionals prefer the administration of a maintenance therapy with a long-acting antipsychotic drug. In this context, among other reasons adduced by the participants to explain the need for a treatment with a long-acting antipsychotic, the lack of adherence to daily oral therapies and the lack of awareness of the disease were highlighted. In this respect, it could suggest that this strategy meets the need to improve the current rates of compliance. Moreover, as asserted in the study by van Zaane et al,Citation80 when treating comorbidities, maintaining the treatment as long as possible should always be considered.
The most frequently used antipsychotics by up to 93.2% of the professionals are daily oral olanzapine, quetiapine, extended-release paliperidone, daily oral risperidone, and paliperidone palmitate, all of which have been proved to be effective in the management of dual diagnosed patients.Citation76,Citation77,Citation81,Citation82 In line with this, whenever there is an antipsychotic drug with oral and long-acting administration available, it is important to consider long-acting treatments versus daily intake options, as the first provides a better response in dual diagnosis patients.Citation83 In the professionals’ perception and taking into account the improvement of psychotic-phase positive symptoms, the control of behavior disorders and the decrease of craving are the main therapeutic goals in dual diagnosis patients. Paliperidone palmitate has proven to be the most used long-acting antipsychotic and is perceived as a drug that offers better tolerability than all the other antipsychotics. Its advantages include improving cognition/functioning and a simple route of administration;Citation77 both characteristics are considered to be the main pharmacologic factors required to facilitate therapeutic compliance.
Antidepressants were used by 92% of the participants. The study results showed that professionals preferred using selective serotonin reuptake inhibitors and, to a lesser degree, dual-action drugs such as noradrenergic and specific serotonergic antidepressants. Moreover, 85.2% of the participants affirmed that they prescribe drugs indicated for addiction treatments, especially disulfiram and, less frequently, naltrexone and bupropion, very effective drugs for addiction treatments;Citation84 95.2% prescribe anticonvulsive euthymic drugs, mostly topiramate, to manage their patients, although there is limited evidence about its appropriateness for the treatment of addictions;Citation85 and 72.5% prescribe modulators of the endogenous opioid system for opioid-dependent patients, mainly methadone, the combination of buprenorphine and naloxone, which have been shown useful for dual diagnosis patients.Citation86 In this context, it is important to point out the high prescription rates of benzodiazepines for the population affected with dual diagnosis: 76.4% of the professionals prescribe long half-life benzodiazepines to their patients, a much higher rate than that observed in a previous international study.Citation87 This occurs in spite of the fact that the use of benzodiazepines can increase the risk of abuse potential and therefore generate a new problem with abuse/dependence, as stated in the research performed by Brunette et al.Citation88 This is why careful assessment and close monitoring are recommended in the use of benzodiazepines, if not totally avoided, in dual diagnosis patients.Citation12 Furthermore, professionals also found that 59% of their patients use benzodiazepines for self-medication. This result is consistent with studies in which the use of benzodiazepines without prescription has been evaluated.Citation89,Citation90
Finally, the professional’s education is relevant.Citation46,Citation91 The present study shows that 60% of the participants considered that courses are the main educational tool, followed by workshops and access to clinical practice guidelines. In fact, this appreciation is similar to that observed in previous works focusing on professionals’ perception.Citation27,Citation44
Strengths and limitations
As for the limitations of this study, it should be noted that the participants in this open online survey are highly motivated professionals very interested in participating in a study on DDs. Therefore and since results may not represent the opinion of all of the professionals who care for DD patients, it is necessary to compare the outcomes with the perception of other groups of professionals with a different profile. Also, it has been considered that generally the strength of studies based on open conducting online surveys is not too significant, although the choice of this methodology is supported by numerous previous studies published in the literature.Citation27,Citation43,Citation44
Nevertheless, due to the importance of the professionals’ opinion on health care planning, the relevance of the topic, the number of participants, and the fact that they work in a variety of dual diagnosis patient health care units, these results should be highly valued. Furthermore, due to the few works previously published in the literature on this topic, they should be especially valued.Citation27,Citation43,Citation44
Conclusion
Professionals perceived that most dual diagnosis patients do not comply with the prescribed treatment. This lack of adherence is associated with a worsening of their disease evolution, which is reflected in exacerbations of the psychopathology and relapse in substance consumption. Undoubtedly, these circumstances lead to a worse prognosis; therefore, it is very necessary to implement pharmacologic and nonpharmacologic strategies in order to improve the rate of compliance. Taking into account the main objectives of the surveyed professionals, when treating their patients, one should include not only effective pharmacological therapies for symptom control, with a moderate side effect profile, which have proven to reduce the employment of health care resources and improve the patient’s functioning, but also nonpharmacological therapies, which also improve therapeutic compliance, as these are influential factors for a better prognosis.
Acknowledgments
We would like to thank Entheos Editorial Group members for their assistance in writing this article. We would also like to thank all the authors who responded to the survey and agreed to being named: José Antonio Acal Gutiérrez, José Ángel Alcalá Partera, Francisco Carlos Alcántara López, Juan Manuel Alonso Ramis, Benjamín Altozano Aguila, Isabel Álvarez, Adolfo Álvarez Villarino, Raquel Álvarez García, Joan Alvarós, Ana Aparicio, Rosario Azcorbebeitia Lamiquiz, Gerardo Aznar Rivera, Diana Bachiller, Abel Baquero, Carmen Barral, Diego Barral Tafalla, Mª Ángeles Barreda, Ana Mª Bastida de Miguel, Cipriano Beccar Varela, Patricia Bernal, Mª Asunción Berrueco Quintero, Luisa Mª Blanco Caramés, Octavio Blanes Pla, Mª Dolors Bosch Balcells, Victoria Boticario, Mª Amparo Buján López, David Cáceres Anillo, Pilar Calvo Estopiñán, Teresa Carot Subirats, Federico Guillermo Castellanos Gutiérrez, Ricardo Castillo Falla, María de Guía Castro Granados, Olga Chapinal, Antonio Evaristo Clavero Machado, Luciano Cobos Luna, María Conde, Gloria Cordeiro Crespo, Isabel María de Haro García, Antonio de María García, Francisco de Orta Sequera, Mª Belén del Amo, Celia del Pino Lidón, Juan Carlos Díaz del Valle, Enrique Aníbal Díaz Ramos, Helen Dolengevich, Álvaro José Doña Díaz, Marisa Dorado, Caridad Espinosa Delgado, Esther Estaún, Jaime A. Fernández, José Manuel Fernández Fernández, Nieves Fernández Rodríguez, José Luis Frías Pulido, Paula María Fuertes, Óscar David Galera, Gladys Gamboa, Angustias García, José María García Basterrechea, Maruja García Gómez, Dionisio García Osuna, María Llanyra García Ullán, Pilar Gardeta Sabater, Vicente Garijo García, Alfonso Gil Martínez, José Manuel Giménez García, José Luis Gómez Juárez, Esperanza González Marín, Juan Bautista González Palomino, Begoña Gonzalvo Cirac, Alfredo Gurrea Escajedo, Inmaculada Gutiérrez Porcel, Ana María Hernández Cordero, Miguel Ángel Hernández Las Heras, Isabel Hernández Otero, Agustín Mª Herrero Matías, Ana Jiménez Bidón, Juan Manuel Jiménez-Lerma, Yacksary Juárez Ortega, Miguel Landabaso, Rodrigo Leal, Isabel López Escamilla, David López Gómez, Alex Raúl Lorie Vega, Eloina Mallada, Letizia Irene Manchado López, Julia Elena Márquez-Arrico, Esther Marticorena, Lucía Martín Calvo, Manuel José Martín Esquinas, José Manuel Martínez Delgado, Francisco Ignacio Mata Cala, Piedad Medina Álvarez, Desiderio Mejías, Irene Milla, Argiñe Mingo Idoyaga, Diana Miranda Abal, Fabiola Modrego, Antonio Jesús Molina, Hugo Mongay Sánchez-Gijón, Esther Montero Manzano, Cristina Montilla Bueno, Josué Monzón-Díaz, María Antonia Mora, Juan Andrés Moreno Nieto, Jordi Morillo Vera, Fernando Morrás, Raimundo Juan Muscellini, Adrián Neyra del Rosario, Mª de la Concepción Nogales Romero, Beatriz Nogueras Ormanzábal, Mª Pilar Notario Poves, Daniel Núñez Arias, Jesús Núñez García, Enriqueta Ochoa Mangado, Mª Soledad Olmeda, Carlos Ordóñez, Teresa Orengo Caus, María Bettina Ortiz-Medina, Ana Mª Palé Esteve, Gemma Parramón, Juan Manuel Pascual Paño, Susana Pelegrina Gómez, Salvador Peralta, Mª Pilar Pérez, Joseba Pérez Acha, Blanca Pérez Molina, Jesús Pérez-Pazos, Alicia Picazo Menéndez, Carlos José Pino Serrano, Silvia Piñeiro Carrió, Gabriela Pizzi Guevara, Sofía Prieto Sebastiá, Carmen Quesada Romero, Emilio Rato, Analeda Regalado, Manuel Reus Martínez, Joseba Rey, Laura Reyes, Manuela Reyes Requena, Antonia Rico Soliveres, León Riera Fueyo, María Ríos, María Peñitas Ríos Muñoz, Carmen Ripoll, Mª Ángeles Rodríguez, Carles Rodríguez, María José Rodríguez Melgar, María Soledad Rodríguez Verdugo, Alfonso Rodríguez-Palancas Palacios, Emma Román Fernández, José Paulo Romero Flores, Samuel Leopoldo Romero Guillena, Néstor Romo, J. Javier Rosa, Alfonso Rosa Ruiz, Carmen Rubio Otero, Estela Sáez, José María Salgado, Pilar San Juan, Amparo Sánchez, Mª del Mar Sánchez, Pablo Sánchez Arrobas, Paloma Sánchez de la Nieta Aragonés, Sabrina Sánchez Quintero, Ana María Sánchez Viñas, Mario Sánchez-Morate Tristante, Armando Santiago, Ma Luisa Sanz, Juan Sanz Arroyo, Catherine Séiquer de la Peña, Daniel Serrani, Ma Carmen Serván, Antonio Silvestre Segovia, Fco. Javier Suárez Guzmán, Marta Elsa Suárez Merialdo, José Torroba Molina, Carmen Tosio, Javier Gerardo Trejo Canseco, Marta Vallcanera Cabrera, Luis Vasallo, Urbano Vázquez Fernández, José María Vázquez Vázquez, Dolores Velo, Albert Vicente València, Carlos Villegas, María de Gracia Viseu Pinheiro Lopes do Rego, and Augusto Zafra.
Disclosure
The editorial support of this article, as well as the survey on which it was based, were financed by Janssen. Carlos Roncero has received fees to give talks for Janssen-Cilag S.A., Bristol-Myers Squibb, Ferrer-Brainpharma, Pfizer, Reckitt Benckiser/Indivior, Lundbeck, Otsuka, Servier, Lilly, Shire, GlaxoSmithKline, and AstraZeneca. He has received financial compensation for his participation as a member of the Janssen-Cilag S.A., Lilly, and Shire boards. He has carried out the PROTEUS project, which was funded by a grant from Reckitt Benckiser. Néstor Szerman has received speaker fees from Janssen-Cilag S.A., Lundbeck, Servier, and Lilly. He has received financial compensation for his participation as a member of the Janssen-Cilag S.A. and Lundbeck boards. Antonio Terán has received fees to give talks for Lilly, Janssen, Pfizer, Shire, Lundbeck, GlaxoSmithKline, and Servier. He has received financial compensation for his participation as a member of the Janssen-Cilag S.A., Lilly, Reckitt Benckiser, and Lundbeck boards. Carlos Pino has received financial compensation from the following laboratories: Janssen-Cilag S.A., Lilly, Servier, Ferrer, Lundbeck, Almirall, Reckitt Benckiser, Wyeth, and Esteve. He has received financial compensation for his participation as a member of the Janssen-Cilag board. José María Vázquez has received financial compensation from the following laboratories: Janssen-Cilag S.A., Lilly, Lundbeck, Bristol Myers Squibb, Reckitt Benckiser, and Juste. He has received financial compensation for his participation as a member of the Janssen board. Elena Velasco and Marta García-Dorado work in the Medical Affairs Department of Janssen-Cilag S.A. Miguel Casas has received fees to give talks for Janssen-Cilag S.A., Bristol-Myers Squibb, Ferrer-Brainpharma, Pfizer, Reckitt-Benckiser, Lundbeck, Otsuka, Servier, Lilly, Shire, GlaxoSmithKline, Rovi, and Adamed. He has received financial compensation for his participation as a member of the Janssen-Cilag S.A., Lilly, and Shire boards. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed, and report no other conflicts of interest in this work.
References
- SzermanNMartinez-RagaJPerisLRethinking dual disorders/pathologyAddict Disord Their Treat201312110
- SzermanNMartinez-RagaJTwo different mental disorders? Advancing in dual diagnosisDual Disord201582
- VolkowNDAddiction and co-occurring mental disorders. Director’s perspectiveNatl Inst Drug Abuse NIDA Notes2007212
- World Health Organization [webpage on the Internet]Lexicon of Alcohol and Drug TermsGeneva1994 Available from: http://whqlib-doc.who.int/publications/9241544686.pdf?ua=1Accessed February 22, 2015
- McGovernMPLambert-HarrisCGothamHJClausREXieHDual diagnosis capability in mental health and addiction treatment services: an assessment of programs across multiple state systemsAdm Policy Ment Health201441220521423183873
- McHugoGJDrakeREBrunetteMFXieHEssockSMGreenAIEnhancing validity in co-occurring disorders treatment researchSchizophr Bull200632465566516849398
- AriasFSzermanNVegaPCocaine abuse or dependency and other psychiatric disorders. Madrid study on dual pathologyRevista de Psiquiatría y Salud Mental (Barc)201363121128
- ComptonWMConwayKPStinsonFSColliverJDGrantBFPrevalence, correlates, and comorbidity of DSM-IV antisocial personality syndromes and alcohol and specific drug use disorders in the United States: results from the national epidemiologic survey on alcohol and related conditionsJ Clin Psychiatry200566667768515960559
- Lev-RanSLe FollBMcKenzieKGeorgeTPRehmJCannabis use and cannabis use disorders among individuals with mental illnessCompr Psychiatry201354658959823375264
- SahaTDChouSPGrantBFToward an alcohol use disorder continuum using item response theory: results from the national epidemiologic survey on alcohol and related conditionsPsychol Med200636793194116563205
- SantamarinaSIglesiasCSchizophrenia and frequent psychotropic substance use in our environmentAdicciones2001134385391
- CasasMFrancoMDGoikoleaJMSpanish working group on bipolar disorders in dual diagnosis. Bipolar disorder associated to substance use disorders (dual diagnosis). Systematic review of the scientific evidence and expert consensusActas Españolas de Psiquiatría200836635036118803031
- Rodríguez-JiménezRAragüésMJiménez-ArrieroMADual diagnosis in psychiatric inpatients: prevalence and general characteristicsInvestigación Clínica200849219520518717266
- RonceroCFusteGBarralCPROTEUS Study InvestigatorsTherapeutic management and comorbidities in opiate-dependent patients undergoing a replacement therapy programme in Spain: the PROTEUS studyHeroin Addict Relat Clin Probl2011133516
- PereiroCPinoCFlórezGArrojoMBecoñaECOPSIAD GroupPsychiatric comorbidity in patients from the addictive disorders assistance units of Galicia: the COPSIAD studyPLoS One201386e6645123823135
- Szerman BolotnerNArias HorcajadasFVega AstudilloPPilot study on the prevalence of dual pathology in community mental health and substance misuse services in MadridAdicciones201123324925521814713
- Lev-RanSImtiazSRehmJLe FollBExploring the association between lifetime prevalence of mental illness and transition from substance use to substance use disorders: results from the national epidemiologic survey of alcohol and related conditions (NESARC)Am J Addict2013222939823414492
- Delegación del Gobierno para el Plan Nacional sobre Drogas [Government Delegation for the National Drugs Plan]PNSDMadridMinisterio de Sanidad y Consumo, Informe2009 Available from: http://www.pnsd.msssi.gob.es/Accessed August 16, 2016
- MiquelLRonceroCLópez-OrtizCCasasMEpidemiological and diagnostic axis I gender differences in dual diagnosis patientsAdicciones201123216517221647547
- GualADual diagnosis in SpainDrug Alcohol Rev2007261657117364838
- BahorikALNewhillCEQueenCCEackSMUnder-reporting of drug use among individuals with schizophrenia: prevalence and predictorsPsychol Med2014441616923551851
- YenCFHsiaoRCChenCCThe role of insight to alcohol use disorders in insight to schizophreniaCompr Psychiatry2009501586219059515
- MoellerSJMaloneyTParvazMAImpaired insight in cocaine addiction: laboratory evidence and effects on cocaine-seeking behaviourBrain2010133pt 51484149320395264
- MillerRCaponiJMSevySRobinsonDThe Insight-adherence-abstinence triad: an integrated treatment focus for cannabis-using first-episode schizophrenia patientsBull Menninger Clin200569322023616178711
- Grau-LópezLRonceroCDaigreCObservational study on medications prescribed to dual-diagnosis outpatientsJ Addict Med201482848924562401
- McEvoyJPLiebermanJAStroupTSCATIE InvestigatorsEffectiveness of clozapine versus olanzapine, quetiapine, and risperidone in patients with chronic schizophrenia who did not respond to prior atypical antipsychotic treatmentAm J Psychiatry2006163460061016585434
- RonceroCGómez-BaezaSVázquezJMPerception of Spanish professionals on therapeutic adherence of dual diagnosis patientsActas Españolas de Psiquiatría201341631932924203504
- StroupTSLiebermanJAMcEvoyJPCATIE InvestigatorsEffectiveness of olanzapine, quetiapine, risperidone and ziprasidone in patients with chronic schizophrenia following discontinuation of a previous atypical antipsychoticAm J Psychiatry2006163461162216585435
- SzermanNLopez-CastromanJAriasFDual diagnosis and suicide risk in a Spanish outpatient simpleSubst Use Misuse201247438338922217297
- FrancisJLPennDLThe relationship between insight and social skill in persons with severe mental illnessJ Nerv Ment Dis20011891282282911794575
- VenderSPoloniNIs the insight a favourable prognostic factor in the treatment of mental disorders?Recenti Prog Med2006971056557017263048
- FarrenCKHillKPWeissRDBipolar disorder and alcohol use disorder: a reviewCurr Psychiatry Rep201214665966622983943
- TorrensMRossiPCMartinez-RieraRMartinez-SanvisensDBulbenaAPsychiatric co-morbidity and substance use disorders: treatment in parallel systems or in one integrated system?Subst Use Misuse2012478–91005101422676568
- RonceroCRodríguez-CintasLBarralCTreatment adherence to treatment in substance users referred from psychiatric emergency service to outpatient treatmentActas Españolas de Psiquiatría2012402636922508071
- RonceroCBarralCGrau-LopezLProtocols of dual diagnosis intervention in schizophreniaAddict Disord Their Treat2011103131154
- VelliganDIWeidenPJSajatovicMAssessment of adherence problems in patients with serious and persistent mental illness: recommendations from the expert consensus guidelinesJ Psychiatr Pract2010161344520098229
- Sánchez-PeñaJFAlvarez-CotoliPRodríguez-SolanoJJPsychiatric disorders associated with alcoholism: 2 year follow-up of treatmentActas Españolas de Psiquiatría201240312913522723131
- Spanish Society of Dual Disorders [webpage on the Internet]Proposal to the Strategy on Mental Health NHS2014 Available from: http://www.patologiadual.es/docs/propuesta_AEPD_estrategia_salud%20mental_sns.pdfAccessed November 10, 2014
- SzermanNVegaPGrau-LópezLDual diagnosis resource needs in Spain: a national survey of professionalsJ Dual Diagn2014102849025392250
- RonceroCVegaPMartínez-RagaJProfessionals’ perceptions about healthcare resources for co-occuring disorders in SpainInt J Ment Health Syst2014813525206926
- WarrenJISteinJAGrellaCERole of social support and self-efficacy in treatment outcomes among clients with co-occurring disordersDrug Alcohol Depend2007892–326727417329040
- ZiedonisDMSmelsonDRosenthalRNImproving the care of individuals with schizophrenia and substance use disorders: consensus recommendationsJ Psychiatr Pract200511531533916184072
- OlivaresJMAlptekinKAzorinJMCañasFDuboisVEmsleyRPsychiatrists’ awareness of adherence to antipsychotic medication in patients with schizophrenia: results from a survey conducted across Europe, the Middle East, and AfricaPatient Prefer Adherence2013712113223390361
- VietaEAzorinJMBauerMPsychiatrists’ perceptions of potential reasons for non- and partial adherence to medication: results of a survey in bipolar disorder from eight European countriesJ Affect Disord20121431–312513022840608
- ChanKKChinQPTangJYPerceptions of relapse risks following first-episode psychosis and attitudes towards maintenance medication: a comparison between nursing and social work professionalsEarly Interv Psychiatry20115432433421521490
- AdamsMWComorbidity of mental health and substance misuse problems: a review of workers’ reported attitudes and perceptionsJ Psychiatr Ment Health Nurs200815210110818211557
- Oller-CanetSFernández-San MartínMIGarcía-LecinaRDo depressed patients comply with treatments prescribed? A cross sectional study of adherence to the antidepressant treatmentActas Españolas de Psiquiatría201139528829321953358
- LehmanAFSteinwachsDMTranslating research into practice: the Schizophrenia Patient Outcomes Research Team (PORT) treatment recommendationsSchizophr Bull19982411109502542
- MartinottiGAndreoliSDi NicolaMDi GiannantonioMSarchiaponeMJaniriLQuetiapine decreases alcohol consumption, craving, and psychiatric symptoms in dually diagnosed alcoholicsHum Psychopharmacol200823541742418425995
- TietQQMausbachBTreatments for patients with dual diagnosis: a reviewAlcohol Clin Exp Res200731451353617374031
- SwartzMSWagnerHRSwansonJWSubstance use in persons with schizophrenia: baseline prevalence and correlates from the NIMH CATIE studyJ Nerv Ment Dis2006194316417216534433
- WongMMChenEYLuiSSTsoSMedication adherence and subjective weight perception in patients with first-episode psychotic disorderClin Schizophr Relat Psychoses20115313514121983497
- BaldessariniRJPerryRPikeJFactors associated with treatment non-adherence among US bipolar disorder patientsHum Psychopharmacol Clin Exp200823295105
- HajjarERCafieroACHanlonJTPolypharmacy in elderly patientsAm J Geriatr Pharmacother20075434535118179993
- SalloumIMMossHBDaleyDCSubstance abuse and schizophrenia: impediments to optimal careAm J Drug Alcohol Abuse19911733213361928026
- DixonLDual diagnosis of substance abuse in schizophrenia: prevalence and impact on outcomesSchizophr Res199935supplS93S10010190230
- NieuwlaatRWilczynskiNNavarroTInterventions for enhancing medication adherenceCochrane Database Syst Rev201411CD00001125412402
- UsietoEGPerniabMCPascualCComprehensive intervention in psychotic disorders with substance use disorder comorbid pathology from a dual unitRehabil Psicosoc2006312632
- BłachutMBadura-BrzozaKJarzabMGorczycaPHeseRTDual diagnosis in psychoactive substance abusing or dependent personsPsychiatr Pol201347233535223888766
- SzermanNAacute;lvarez-VaraCCasasMGlosaPatología dual en esquizofrenia. Opciones terapéuticasBarcelonaEditorial Glosa2007
- BenjaminABMossmanDGravesNSSandersRDTests of asymptom checklist to screen for comorbid psychiatric disorders in alcoholismCompr Psychiatry200647322723316635653
- DriessenMVeltrupCWetterlingTJohnUDillingHAxis I and axis II comorbidity in alcohol dependence and the two types of alcoholismAlcohol Clin Exp Res199822177869514288
- Pérez-GálvezBVicente-ManzanaroMPGarcía-FernándezLRomero-EscobarCOliveras-ValenzuelaMAPrevalence of psychopathology in alcohol-dependents outpatientsTrastornos Adictivos2008104248
- SoykaMSubstance misuse, psychiatric disorder and violent and disturbed behaviorBr J Psychiatry200017634535010827882
- BellackASBennettMEGearonJSBrownCHYangYA randomized clinical trial of a new behavioral treatment for drug abuse in people with severe and persistent mental illnessArch Gen Psychiatry200663442643216585472
- HuntGEBergenJBashirMMedication compliance and comorbid substance abuse in schizophrenia: impact on community survival 4 years after a relapseSchizophr Res200254325326411950550
- RedkoCRappRCElmsCSnyderMCarlsonRGUnderstanding the working alliance between persons with substance abuse problems and strengths-based case managersJ Psychoactive Drugs200739324125018159777
- TetzlaffBTKahnJHGodleySHGodleyMDDiamondGSFunkRRWorking alliance, treatment satisfaction, and patterns of posttreatment use among adolescent substance usersPsychol Addict Behav200519219920716011391
- MaremmaniAGRovaiLRuganiFCorrelations between awareness of illness (insight) and history of addiction in heroin-addicted patientsFront Psychiatry201236122787450
- GajskiAKarlovićDAssessment of nurse attitudes on psychiatric patient compliance with pharmacotherapyActa Clin Croat200847314915319175063
- CrowleyVRoseJSmithJHobsterKAnsellEPsycho-educational groups for people with a dual diagnosis of psychosis and mild intellectual disability: a preliminary studyJ Intellect Disabil2008121253918337299
- MartinoSCarrollKKostasDPerkinsJRounsavilleBDual diagnosis motivational interviewing: a modification of Motivational Interviewing for substance-abusing patients with psychotic disordersJ Subst Abuse Treat200223429730812495791
- GearingRETownsendLElkinsJEl-BasselNOsterbergLStrategies to predict, measure, and improve psychosocial treatment adherenceHarv Rev Psychiatry2014221314524394220
- PettinatiHMO’BrienCPDundonWDCurrent status of co-occurring mood and substance use disorders: a new therapeutic targetAm J Psychiatry20131701233023223834
- KellyTMDaleyDCDouaihyABTreatment of substance abusing patients with comorbid psychiatric disordersAddict Behav2012371112421981788
- BenabarreACastroPSánchez-MorenoJEfficacy and safety of long-acting injectable risperidone in maintenance phase of bipolar and schizoaffective disorderActas Españolas de Psiquiatría2009373s143s147
- HoughDLindenmayerJPGopalSSafety and tolerability of deltoid and gluteal injections of paliperidone palmitate in schizophreniaProg Neuro Psychopharmacol Biol Psychiatry200933610221031
- Núñez DomínguezLAAtypical neuroleptic in cannabis users with schizophreniaAdicciones20011316773
- SanLArranzBMartinez-RagaJAntipsychotic drug treatment of schizophrenic patients with substance abuse disordersEur Addict Res200713423024317851245
- van ZaaneJvan den BrinkWDraismaSSmitJHNolenWAThe effect of moderate and excessive alcohol use on the course and outcome of patients with bipolar disorders: a prospective cohort studyJ Clin Psychiatry201071788589320122372
- MurthyPChandPTreatment of dual diagnosis disordersCurr Opin Psychiatry201225319420022395768
- PotvinSStipELippOQuetiapine in patients with comorbid schizophrenia-spectrum and substance use disorders: an open-label trialCurr Med Res Opin20062271277128516834826
- GreenAIBrunetteMFDawsonRLong-acting injectable vs oral risperidone for schizophrenia and co-occurring alcohol use disorder: a randomized trialJ Clin Psychiatry201576101359136526302441
- GreenAINoordsyDLBrunetteMFO’KeefeCSubstance abuse and schizophrenia: pharmacotherapeutic interventionJ Subst Abuse Treat2008341617117574793
- MillerJRoacheJBenefits of topiramate treatment in a dual-diagnosis patientPsychosomatics200950442642719687186
- MaremmaniAGRovaiLPaniPPDo methadone and buprenorphine have the same impact on psychopathological symptoms of heroin addicts?Ann Gen Psychiatry2011101721569624
- ClarkREXieHBrunetteMFBenzodiazepine prescription practices and substance abuse in persons with severe mental illnessJ Clin Psychiatry200465215115515003066
- BrunetteMFNoordsyDLXieHDrakeREBenzodiazepine use and abuse among patients with severe mental illness and co-occurring substance use disordersPsychiatr Serv200354101395140114557527
- Fernandez SobrinoAMFernandezRVLopezCJBenzodiazepine use in a sample of patients on a treatment program with opiate derivatives (PTDO)Adicciones200921214314619578731
- RonceroCGrau-LópezLDíaz-MoránSMiquelLMartínez-LunaNCasasMEvaluation of sleep disorders in drug dependent inpatientsMedicina Clínica2012138833233522018396
- BremsCJohnsonMEBowersLLauverBMongeauVAComorbidity training needs at a state psychiatric hospitalAdm Policy Ment Health200230210912012680616