
Abstract
Issues
Patient-centered care (PCC) is increasingly accepted as an integral component of good health care, including addiction medicine. However, its implementation has been controversial in people with alcohol use disorders.
Approach
A systematic search strategy was devised to find completed randomized controlled trials enrolling adults (>18 years) with alcohol use disorders. Studies had to use a PCC approach such that they should have been individualized, respectful to the patients’ own goals, and empowering. Studies until September 2015 were searched using PubMed, Scopus, the Cochrane Library, PsychINFO, and Web of Knowledge.
Key findings
In total, 40 studies enrolling 16,020 patients met the inclusion criteria. Assessment revealed two main categories of study: psychosocial (n=35 based on motivational interviewing) and pharmacological (n=5 based on an as needed dosing regimen). Psychosocial interventions were further classified according to the presence or absence of an active comparator. When no active comparator was present, studies were classified according to the number of sessions (≥1). Results from single sessions of motivational interviewing showed no clear benefit on alcohol consumption outcomes, with few studies indicating benefit of PCC versus control. Although the results for studies of multiple sessions of counseling were also mixed, many did show a significant benefit of the PCC intervention. By contrast, studies consistently demonstrated a benefit of pharmacologically supported PCC interventions, with most of the differences reaching statistical significance.
Implications
PCC-based interventions may be beneficial for reducing alcohol consumption in people with alcohol use disorders.
Introduction
The Institute of Medicine has included patient-centered care (PCC) as one of the major aims in care quality and defines it as “providing care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions”.Citation1 Although not a new phenomenon, it has recently attracted renewed attention.Citation2,Citation3 PCC advocates for a shift from disease-oriented to patient-oriented medicine. Doctors should no longer be authoritative figures who make all the relevant decisions. Instead, they must engage in a shared decision-making model where patients are acknowledged to be experts with regard to their own symptoms and values and where they are recognized as unique and diverse. In such a model, the responsibility is shared between a patient and a physician, and the physician’s key role is to strengthen the patient’s capabilities to handle his or her part of responsibility.Citation4
Application of PCC in the field of mental disorders remains a controversial issue. It has long been argued that patients with psychiatric disorders are vulnerable to impediments in decision making,Citation5–Citation8 and a paternalistic approach has been the preferred norm in the field.Citation9,Citation10 Conversely, a number of studies indicate that patients engaged in the decision-making process show greater satisfaction and collaboration, with greater efficacy of treatment.Citation11,Citation12
While considering the field of alcohol use disorders, it is also likely that ideological bias and stigma have exacerbated the paternalistic approach. The harmful use of alcohol is one of the world’s leading health risks and is the leading risk factor for death of people aged 15–49 years.Citation13 However, patients with alcohol use disorders often receive a lower quality of health care than those with other chronic conditions; many dependent patients go without treatment, and even when they are treated, pharmacotherapy is underutilized.Citation14–Citation16 Abstinence has been the prevailing goal, usually irrespective of patients’ own aims or desire.Citation17 Crucially, patients do not always view abstinence as an acceptable, desirable, or realistic treatment goal, and there is an increasing debate about the possibility and the convenience of broadening treatment goals in accordance with a PCC model.Citation18 For example, this could mean establishing reduction in heavy drinking as a possible objective for some patients.Citation18–Citation20 Reduction of alcohol consumption has been shown to reduce the annual and lifetime risk of alcohol-related death, and it could attract patients who are currently not inclined to seek treatment or do not accept abstinence as a treatment goal.Citation20–Citation22 Indeed studies show that patients with alcohol use disorders are more likely to achieve self-set goals (eg, reduction or abstinence), rather than goals that are imposed on them.Citation23,Citation24
Several treatment options (psychosocial and pharmacological) are available for people with alcohol use disorders, but no single therapy has been proven to be more effective than another. PCC and shared decision making are considered especially appropriate when outcomes of the different treatments are similar and when an active role of the patient is needed.Citation25 Thus, some experts consider alcohol use disorders as potentially a suitable situation to use a PCC approach.Citation2 Although some of the components of PCC might have been previously tested for the treatment of alcohol use disorders, for example, in the form of individually tailored feedback and treatment, these have not been systematically assessed in a cohesive manner. The aim of this review was to systematically assess the efficacy of interventions based on a PCC health care approach, both pharmacological and psychosocial, for the management of alcohol use disorders.
Methods
This systematic review was conducted in accordance with the principles recommended by the Cochrane Handbook for Systematic Reviews of Interventions.Citation26 The Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidance was followed for the reporting of procedures; its checklist can be seen in Supplementary materials.
Definition of PCC
Although patient centeredness is not an easy concept to define in a concise manner, a previous systematic review operationalized it under four defining attributes: holistic, individualized, respectful, and empowering.Citation27 Many studies might be considered as PCC, but they might not use this exact expression, or any of the attributes of PCC previously reported. Thus, in order to conduct an appropriately sensitive electronic search, we predefined several adjectives and expressions to cover the four attributes. For example, alternative terms for “empowering” included “patient involvement”, “patient perspective”, “shared decision-making”, and “patient decision”, and alternative terms for “individualized” included “tailored”, “personalized”, and “customized”.
Data sources and searches
The following databases were searched: PubMed, Scopus (which contains EMBASE), the Cochrane Library, PsychINFO, and the Web of Knowledge. The search strategies for PubMed, Scopus, and the Cochrane Library are listed in Supplementary materials. The searches were run until September 2015. Additional hand searches of the reference lists of included randomized controlled trial and relevant systematic reviews were conducted. Finally, the following clinical trial registries were also searched for relevant studies: ClinicalTrials.gov, ISRCTN Register, UK Clinical Trials Gateway, and metaRegister of Controlled Trials.
Study selection
Individual (not cluster) randomized controlled trials enrolling adults (≥18 years) with alcohol use disorders (including hazardous or harmful drinking, alcohol dependence, or any other alcohol use disorder) were included. All the studies had to use a PCC approach such that they should have been individualized, respectful to the patients’ own goals, and empowering. Computerized interventions were not included in this review.
As described earlier, although interventions might not have been described with these same adjectives, they were fully reviewed to check whether they met the criteria (ie, the description of the intervention was individually assessed to determine whether it could be considered PCC). Studies could use any standardized outcome regarding alcohol consumption (eg, heavy drinking days, grams of alcohol, days of abstinence, percentage of patients drinking below recommended limits on validated screening tools). Only publications in English were considered.
To homogenize the review, studies of patient populations with psychiatric comorbidities were excluded from this review as were studies including populations with relevant and differential psychological variables (eg, mandated or incarcerated patients and pregnant women). Studies conducted in the inpatient setting and short-term studies with <3 months of follow-up were also excluded. Studies using cover stories where patients did not know the real intention of the intervention were also excluded, as this is clearly contrary to the concept of PCC. Finally, any comparator was eligible as long as it was not PCC based.
Data extraction
PB and AG independently screened all the studies for inclusion. Disagreements were resolved by discussion when possible. If not, a third person was consulted. Data were extracted by PB and independently checked by AG. The extracted data consisted of participant characteristics, setting, study methods, intervention characteristics, comparators, outcomes, and results.
Quality assessment
PB and AG independently evaluated the quality of the studies. Following the Cochrane guidelines and the methods used in a recent systematic review undertaken by Mdege et al,Citation28 a domain-based approach was used. The following criteria were applied: power calculation, adequacy of randomization, allocation concealment, adjustment for covariates in the analysis, blinding of participants when possible, blinding of outcome assessors, explanation of dropouts, and use of intention-to-treat analysis.
Data synthesis
Considerable heterogeneity existed between the studies, mainly in terms of reported outcomes, how the outcomes were defined and reported, and the duration of the studies. Given the different methodologies that were employed, the studies were grouped according to whether they primarily assessed a pharmacological or a psychosocial intervention. In the psychosocial group, a further grouping was made according to the number of sessions received, categorizing studies between 1 or >1 sessions.
A meta-analysis was conducted on the basis of our findings, by trying to build an outcome construct based on construct validity. However, given the significant methodological issues involved, the analysis was deemed inappropriate and a narrative synthesis was instead conducted.
Results
Literature search
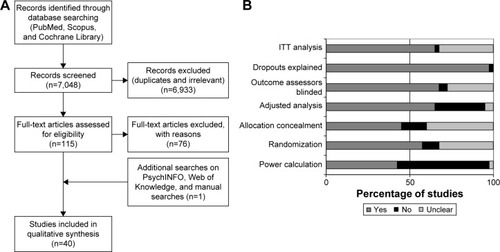
A total of 7,048 records were screened through the search strategy, and 115 full-text articles were assessed for eligibility. An additional reference was identified by hand searching, and eventually, after exclusion criteria were applied (reasons for exclusion of full-text papers are available in the Supplementary materials), a total of 40 studies were included in the systematic review.Citation29–Citation68 depicts the flow diagram of the study.
Figure 1 (A) Study flow chart and (B) quality assessment.
Study characteristics
The 40 studies included in this review involved a total of 16,020 enrolled patients. Sample size in each study ranged from 54 to 987 patients. An initial assessment of the studies revealed two groups according to the main treatment evaluated: psychosocial or pharmacological, with 35 evaluating psychosocial interventions and five evaluating primarily pharmacological interventions.
All psychosocial interventions that met the inclusion criteria in this review were based on motivational interviewing (MI) principles, which might be considered as the cornerstone of patient-centered psychosocial interventions nowadays. MI is defined as “a directive, client-centered counseling style for eliciting behavior change by helping clients to explore and resolve ambivalence”.Citation69 Compared to nondirective counseling, it is more focused and goal directed. The examination and resolution of ambivalence is its central purpose, and the counselor is intentionally directive in pursuing this goal.
Regarding pharmacological interventions, all those fulfilling the inclusion criteria were based on the “as needed” concept. The “as needed” [or pro re nata] treatment paradigm is a well-understood medical concept, where the patient takes the medication in response to individual circumstances and not on a scheduled basis. Although it has been a standard practice for many years in asthma, diabetic, and allergy care, it represents a paradigm shift in the way that pharmacotherapy is used in the management of alcohol use disorders.Citation70
For further grouping studies, psychosocial interventions based on MI and with no active comparator (defined as receiving no further intervention or receiving only information, either orally or written materials) were divided according to the number of sessions they contained (1 or >1), while the studies containing an active comparator (like cognitive behavioral therapy [CBT], for example) were included in a separate category. Thus, four categories were created to report the results of the systematic review: single-session PCC with no active comparator, more than one session PCC with no active comparator, PCC with active comparator, and patient-centered pharmacological interventions.
Quality assessment
The results of quality assessment of the included studies are shown in Supplementary materials. Overall, less than half (42.5%) of the studies were deemed as adequately powered, 57.5% had an adequate randomization, and 45% adequate allocation concealment. Around two-thirds (65%) used adjusted analysis and 67.5% reported blinding of the outcome assessors, and all but one study reported adequate information on the patients who dropped-out. Most (65%) of the studies stated clearly an intention-to-treat analysis (). In psychosocial intervention studies, it was not considered possible to blind participants to the delivered intervention; therefore, participant blinding was only assessed in pharmacological intervention studies, which were all deemed as adequate on this item.
Efficacy of PCC
Single-session PCC with no active comparator
Seventeen studies were included in this subgroup ().Citation29–Citation45 Globally, they failed to show a clear benefit of the PCC intervention over the control groups.
Table 1 Single-session patient-centered counseling – no active comparator
Amount and frequency of alcohol consumption
Seven studies reported on the number of drinks per week at study end,Citation35–Citation37,Citation40,Citation42–Citation44 with only Daeppen et alCitation36 reporting a statistically significant difference from baseline to follow-up (−1.5 vs 0.8; P=0.004) favoring the PCC group.
Bischof et al reported a nonsignificant difference in grams of alcohol per day between groups,Citation30 Emmen et al reported a nonsignificant difference in drinks per day,Citation38 and Soderstrom et al reported on the number of drinks in the last 90 days, with no differences between groups.Citation45
Five studies reported the number of drinks per drinking day. Four could not find significant differences,Citation33–Citation35,Citation44 while Carey et al only reported a small effect size, with no significance value.Citation32
Four studies reported on drinking days per week,Citation34,Citation35,Citation42,Citation44 none of them reaching statistical significance between groups. Similarly, Lee et al reported on drinking days/month, with no differences between groups.Citation41 Chang et al reported no differences in the percentage of drinking days between groups,Citation33 and Senft et alCitation44 reported no differences in the percentages of abstinent patients.
Hazardous and heavy drinking
Seven studies reported on the number of binge episodes per month.Citation33,Citation35–Citation37,Citation39,Citation41,Citation43 Only Daeppen et al (2011) reported a statistically significant difference favoring the PCC group (baseline to follow-up difference −1.5 vs −0.8, P=0.04).Citation36
Murphy et al reported the number of binges per week and Soderstrom et al reported the number of binges in the last 90 days, both of them showing no significant differences between groups.Citation43,Citation45 Brown et al (2007) reported a significant difference only for men in the reduction in number of risky drinking days (30% vs 12.9%, significance not reported),Citation31 and Senft et al found no differences in the frequency of risky drinking.Citation44
Three studies reported the percentage of heavy drinkers at study end. Two could not find any significant difference,Citation35,Citation37 while the remaining study by Bischof et al reported a statistically significant difference only in the subgroup of patients with alcohol abuse (25% vs 41.3%; P=0.039), with no difference in the alcohol-dependent or heavy episodic drinking-only subgroups.Citation30 Cherpitel et al reported a non-significant difference in the percentage of at risk drinkers between groups or in the maximum number of drinks per occasion.Citation34 Carey et al reported a medium effect size in peak blood alcohol favoring the PCC group (significance not reported),Citation32 while Senft et al reported no significant difference in this outcome.Citation44
Scores
Bazargan-Hejazi et al reported a nonsignificant difference in the percentage of patients changing their drinking risk status according to the Alcohol Use Disorders Identification Test (AUDIT) score.Citation29 In the subgroup of moderate risk (scores 7–18), the PCC group had a larger reduction (34% vs 13%; P=0.0099). Daeppen et al reported a nonsignificant difference between groups regarding the change in the AUDIT score.Citation35
More than one session PCC with no active comparator
Fifteen studies were included in this subgroup ().Citation46–Citation60 Taken together, data show mixed results, with some studies reporting significant differences between groups, whereas others do not.
Table 2 More than one session patient-centered counseling – no active comparator
Amount and frequency of alcohol consumption
Nine studies reported data regarding the amount of alcohol consumption. Five studies reported it in the form of units of alcohol per week.Citation49,Citation51,Citation52,Citation57,Citation58 Two failed to show statistically significant differences between groups,Citation49,Citation51 while the other three reported significant differences for the intervention groups.Citation52,Citation57,Citation58 The amount of alcohol consumption in the two intervention groups in D’Onofrio et al decreased from 20.4 and 19.8 to 13.0 and 14.3, respectively, while that in the control group ranged from 20.9 to 17.6 (P=0.045).Citation52 The reductions in Monti et al for the intervention and the control group were 13.07–6.10 and 10.77–8.83, respectively (P<0.01 in the treatment × time interaction).Citation57 Noknoy et al reported decreases from 13.27 to 4.72 and from 10.55 to 11.24 for the intervention and control group, respectively (P=0.04).Citation58 Maisto et al reported significant decreases for brief interventions but not for MI in the number of drinks in the past month.Citation55
Two studies reported on the amount of grams of alcohol per week,Citation46,Citation47 with no significant differences between groups at study end. These two studies also reported on the number of drinks per drinking day, again failing to reach any significant difference between groups. Noknoy et al also reported on this outcome, finding a statistically significant difference at 6 months follow-up favoring the PCC group (2.26 vs 4.02; P=0.018).Citation58
Finally, five studies reported on the number of days drinking. Three of them failed to find any significant difference,Citation46,Citation47,Citation55 whereas Monti et al reported a significant difference in the time × treatment interaction favoring the PCC group (4.52 vs 6.54 in the last month; P<0.001).Citation57 Sellman et al reported no difference regarding the percentage of abstinent patients.Citation59
Hazardous and heavy drinking
Ten studies reported outcomes related to heavy or hazardous drinking. Curry et al reported a 19% difference between groups in the proportion of patients reporting any at risk drinking pattern, favoring the PCC group (42% vs 61%; P=0.003).Citation51 Allen et al failed to show any significant difference on the same outcome.Citation48 Sellman et al reported a significant decrease in the percentage of heavy drinking days in the past 6 months favoring PCC (42.9% vs 65%).Citation59
Sommers et al and Beich et al reported on the relative risk of heavy drinking between groups. Although differences favored the PCC group, they were not statistically significant at study end.Citation49,Citation60
Three studies reported on the number of risky drinking days in the last month. Brown et al did not find any significant difference,Citation50 whereas the other two reported statistically significant differences favoring the PCC groups. D’Onofrio et al reported a decrease from 7.5 and 7.2 to 4.7 and 5.1 versus a decrease from 7.2 to 5.8 (P=0.03).Citation52 Monti et al reported a statistically significant difference in the treatment × time interaction (4.52 versus 6.54; P<0.001).Citation57 Longabaugh et al found no significant difference in the number of heavy drinking days between groups.Citation54
Noknoy et al reported on the number of binge episodes in the last week, with no significant differences between groups,Citation58 and Sommers et al reported on the maximum units of alcohol in a 6-hour period, with no significant differences between groups at study end.Citation60
Alcohol scores
Two studies reported no significant changes in AUDIT or AUDIT-C scores between groups.Citation53,Citation56 Hermansson et al reported a significant decrease for the whole sample in the AUDIT score.Citation53
PCC – active comparator
Three studies were included in this subgroup ().Citation61–Citation63 Patient-centered counseling strategies, mainly through MI, where compared against CBT and 12 steps facilitation in one study,Citation61 against CBT in another,Citation63 and against social behavioral network therapy in the other.Citation62 Taken together, data from these studies suggest that all these counseling strategies are effective in the treatment of alcohol use disorders, with no significant differences between any of them.
Table 3 Patient-centered counseling – active comparator
Amount and frequency of alcohol consumption
The three studies failed to report a significant difference between groups while measuring outcomes related to alcohol consumption. Two reported on number of drinks per drinking day, with no significant differences between groups, although globally the whole study sample improved significantly (in the UK Alcohol Treatment Trial study, eg, the reduction was from 26.8 to 19.2).Citation61,Citation62 The same two studies reported also on percentage of days abstinent, with the same general improvement, with no group significant differences (again, in the UK Alcohol Treatment Trial study, it changed from 29.5% to 46.0% for the whole sample). The study by Shakeshaft et al reported a significant within PCC group decrease in the number of drinks per week (from 32.7 to 24.9; P<0.01), with no statistically significant differences when compared to CBT.Citation63
Hazardous and heavy drinking
Two studies reported on measures related to heavy drinking.Citation61,Citation63 Project MATCH (Matching Alcoholism Treatments to Client Heterogeneity) reported a statistical superiority of 12 steps facilitation against CBT and motivational enhancement therapy in the survival analysis in relapse to heavy drinking (defined as three consecutive days of >5 drinks per day for men and >3 drinks per day for women), where 53% of 12 steps facilitation patients did not relapse, and 49% and 48% in the motivational enhancement therapy and CBT groups did not relapse.Citation61 Shakeshaft et al reported a significant within PCC group decrease in heavy drinking episodes in the last 30 days (from 20.9 to 15.4; P<0.01). Again, no statistically significant differences were noted between groups.Citation63
Patient-centered pharmacological interventions
Five studies were classified in this group ().Citation64–Citation68 They all shared the same strategy: targeted or as-needed medication. Three used nalmefene as the study medication, and two used naltrexone. Overall, data clearly suggest a benefit of the PCC intervention, when compared with the control groups, in terms of reduction in alcohol consumption and heavy drinking, with most of the differences reaching statistical significance.
Table 4 Patient-centered pharmacological interventions
Amount and frequency of alcohol consumption
Four of the five studies in this group reported statistically significant reductions in the intervention group when compared with the control. Mann et al found a significant reduction in grams per day for the nalmefene group (−50.7 vs −39.7).Citation64 Heinala et al reported a significant difference in grams/week when comparing the coping-naltrexone group with the rest combined (231 vs 354, 357, and 326; P=0.05).Citation67 Karhuvaara et al reported statistically significant differences in both drinks per week and drinks per drinking day favoring the targeted nalmefene group (drinks per week in the last month: 23.2 vs 28.5, P=0.0018; drinks per drinking day in the last month: 6.3 vs 7.3, P=0.0134).Citation66 Kranzler et al reported the targeted naltrexone group drinking 16.5% less than the other groups, although differences were not statistically significant.Citation68 However, among men at week 12, the differences did reach significance (P=0.027). The remaining study by Gual et al reported a baseline to 6-month difference of −5.0 g/day favoring the PCC group, but it did not reach statistical significance (95% CI −10.6 to 0.7; P=0.08).Citation65
Hazardous and heavy drinking
The four studies assessing this outcome (Heinala et al, 2001, Karhuvaara et al, 2007, Mann et al, 2013, and Gual et al, 2013) reported statistically significant differences in heavy drinking favoring the PCC groups.Citation64–Citation67 The 6-month differences in heavy drinking days per month reported by Gual et al and Mann et al were −1.7 days/month (95% CI −3.1 to 0.4; P=0.012) and −2.3 days/month (P=0.0021), respectively, both favoring the nalmefene group.Citation64,Citation65 In the study by Heinala et al, the targeted naltrexone group combined with nonabstinenceoriented group therapy did better than the others in survival analysis for preventing relapse to heavy drinking, reaching statistical significance (exact numbers not reported).Citation67 Karhuvaara et al reported a statistically significant decrease in heavy drinking days per month favoring the targeted nalmefene group (from 15.5 to 8.8 vs 16.2 to 10.6; P=0.0065).Citation66
Discussion
In this paper, we systematically reviewed the efficacy of interventions based on a PCC health care approach for the management of alcohol use disorders. When reviewing the studies identified by our search, it was realized that all PCC trials selected for the review could easily be categorized into two groups: psychosocial interventions and pharmacological supported interventions, and hence, this grouping was adopted. Psychosocial interventions could then be classified further into single sessions of PCC and multiple sessions of PCC.
Regarding psychosocial interventions, our results are in line with previous systematic reviews conducted specifically for MI, which, as mentioned earlier, was the cornerstone of PCC psychosocial interventions found in this review.Citation28,Citation71 Findings within the categories of trials on PCC interventions based on MI appeared mixed. If differences in alcohol consumption emerged between intervention and control groups, they were usually not significant if participants attended one counseling session only. The proportion of studies suggesting that PCC is more effective than control interventions increased if participants took part in several counseling sessions; that is, the number of counseling sessions seems to moderate the effectiveness of PCC. This is in line with the finding of a previous systematic review which concluded that PCC interventions of more than one session work by first increasing the patients’ readiness to change during the first session, and then effecting reduction in alcohol consumption in the follow-up sessions.Citation28
Regarding pharmacologically supported PCC interventions, based on the as needed approach, an effect seemed to emerge from our review. However, the effect cannot be attributed fully to pharmacological elements, since studies in this group also had a psychosocial component, and therefore interactions between the two should be taken into account when interpreting the findings. Considering the fact that only a very small percentage of patients with alcohol use disorders (<10%) receive treatment,Citation72,Citation73 this finding has significant implications for current health care. All the studies of pharmacological interventions were included in this review on the basis of their “as needed” use. This paradigm has been controversial in addiction medicine for many years, with many believing that medications for alcohol use disorders need to be taken on a supervised, strict basis. In this respect, a recent analysis of clinical trial data for nalmefene concluded that people with alcohol dependence are able to adhere to an as needed regimen.Citation68 The data indicate that medication intake varies according to drinking patterns with some patients taking the medication daily and others taking medication at tailored intervals. In their recent editorial, Bradley and KivlahanCitation2 suggested that pharmacological interventions might help bring the concepts of PCC into the alcohol field. By understanding that effective treatments are available, health care professionals are better able to offer people with alcohol use disorders various evidence-based options, including medications and psychosocial support, to achieve recovery.
A key difficulty in conducting this review was the definition and operationalization of PCC as a concept that translates into alcohol use disorders. PCC is not a binary concept (present or absent), and the potential alcohol interventions had to be judged along a continuum of PCC interventions. Despite this fact, we had to simplify and finally dichotomize interventions as PCC or not PCC. For example, the efficacy of pharmacologically supported interventions was considered a key component of this research. Although medications are not PCC (they are just chemical compounds), as needed use allows them to be prescribed in accordance with the principles of PCC. Conversely, computerized interventions were not included in this review. Although one might argue that they can also be considered PCC depending on how they are structured and conducted, they are ultimately based on a predefined number of algorithms and options, thus making it difficult to truly individualize the intervention according to the needs of each patient.
The considerable heterogeneity of the studies included made it impractical to perform any meta-analyses of the data, and so we were limited to narrative descriptions. As discussed by the authors of other systematic reviews of alcohol interventions, this will remain a barrier until consensus is reached in the preferred methods for measuring alcohol consumption.Citation28,Citation71,Citation74 It is therefore important to note that the European Medicines Agency now recommends total alcohol consumption and the number of heavy drinking days as suitable outcomes for studies of alcohol reduction as well as the continued abstinence rate for studies where abstinence is the stated goal. It further suggests that total alcohol consumption and heavy drinking days can also be used to assess the impact of an abstinence-based intervention when patients have a relapse (or lapse or slip).Citation17 It is hoped that such guidance will aid the future standardization of studies.
Other potential limitations of our review include the broad definition of alcohol use disorders (hazardous or harmful drinking, alcohol dependence, or any other alcohol use disorder) and the consequent inclusion of patients with and without a diagnosis of alcohol dependence. It may be that patients with dependence require longer periods of interventions than those without dependence, and this factor might have contributed to some of the findings, especially for PCC psychosocial interventions. To try and homogenize the review, we did not include studies of patients with psychiatric comorbidities or with relevant and differential characteristics (eg, mandated or incarcerated patients and pregnant women). Although necessary for the purposes of this review, application of these exclusion criteria resulted in the exclusion of a number of potentially interesting studies. For example, one large long-term study with nalmefeneCitation75 was excluded because it included patients taking antipsychotics or antidepressants for current psychiatric comorbidities. Also, it is important to remark that an important share of alcohol patients do suffer from negative emotional and affective states that might indeed be produced by alcohol itself. Therefore, this exclusion might have oversimplified a complex reality such as the one of alcohol use disorders. Finally, the external validity of our findings is handicapped by the fact that male patients were more than twice as frequent as females in all the categories.
Conclusion
The limitations of the review, as well as the mixed results found in some of the categories investigated, prevent firm conclusions to be drawn. Single-session studies did not appear to show a clear benefit, multiple-session studies showed mixed results, and active comparator studies did not report significant differences while measuring outcomes related to alcohol consumption. Although pharmacological studies were found the most robustly effective, the shorter follow-up periods and the concomitant presence of psychosocial components in the studies prevent a full and clear attribution to be done. However, since we believe that PCC is increasingly accepted as a central tenet of high-quality health care, and some of the results of this review suggest PCC could indeed be an appropriate strategy for alcohol use disorders, there is an urgent need for additional research evidence on the effectiveness of PCC-based alcohol interventions.
Acknowledgments
H Lundbeck A/S funded this systematic review. The authors were solely responsible for the collection, analysis, and interpretation of data and in the writing of the report. There was no payment for the writing of the report, and the decision to submit the report for publication also rested with the authors. The authors thank Anita Chadha-Patel (ACP Clinical Communications Ltd. funded by H Lundbeck A/S) for editorial assistance (English language editing and referencing).
Disclosure
The authors report no conflicts of interest in this work.
References
- Institute of Medicine Committee on Quality of Health Care in AmericaCrossing the Quality Chasm: A New Health System for the 21st CenturyWashington, DCNational Academy Press2001
- BradleyKAKivlahanDRBringing patient-centered care to patients with alcohol use disordersJAMA20143111861186224825640
- RathertCWyrwichMDBorenSAPatient-centered care and outcomes: a systematic review of the literatureMed Care Res Rev201370435137923169897
- LuskJMFaterKA concept analysis of patient-centered careNurs Forum2013482899823600637
- AppelbaumPSClinical practice. Assessment of patients’ competence to consent to treatmentN Engl J Med20073571834184017978292
- RobertsLWInformed consent and the capacity for voluntarismAm J Psychiatry200215970571211986120
- CoverdaleJHChervenakFAMcCulloughLBBayerTEthically justified clinically comprehensive guidelines for the management of the depressed pregnant patientAm J Obstet Gynecol19961741691738572002
- McCulloughLBCoverdaleJHChervenakFAEthical challenges of decision making with pregnant patients who have schizophreniaAm J Obstet Gynecol200218769670212237650
- GoossensenAZijlstraPKoopmanschapMMeasuring shared decision making processes in psychiatry: skills versus patient satisfactionPatient Educ Couns200767505617350214
- GossCMorettiFMazziMADel PiccoloLRimondiniMZimmermannCInvolving patients in decisions during psychiatric consultationsBr J Psychiatry200819341642118978325
- CoxKStevensonFBrittenNDundarYA systematic review of communication between patients and health care professionals about medicine-taking and prescribing King’s College London, GKT Concordance Unit, Guys’ King’s and St Thomas’ School of Medicine2003 Available from: www.medicines-partnership.orgAccessed December 1, 2015
- SwansonKABastaniRRubensteinLVMeredithLSFordDEEffect of mental health care and shared decision making on patient satisfaction in a community sample of patients with depressionMed Care Res Rev20076441643017684110
- LimSSVosTFlaxmanADA comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010Lancet20133802224226023245609
- AndersonPBraddickFReynoldsJGualAAlcohol policy in Europe: Evidence from AMPHORA. 2nd ed. The AMPHORA project2013 Available from: http://amphoraproject.net/view.php?id_cont=45Accessed December 1, 2015
- AndersonPWojnarMJakubczykAManaging alcohol problems in general practice in Europe: results from the European ODHIN survey of general practitionersAlcohol Alcohol20144953153925031247
- RehmJAndersonPBarryJPrevalence of and potential influencing factors for alcohol dependence in EuropeEur Addict Res20152161825342593
- EMAGuideline on the development of medicinal products for the treatment of alcohol dependence. EMA/CHMP/EWP/20097/2008 (previously EMEA/CHMP/EWP/20097/2008)2010 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2010/03/WC500074898.pdfAccessed December 1, 2015
- GastfriendDRGarbuttJCPettinatiHMFormanRFReduction in heavy drinking as a treatment outcome in alcohol dependenceJ Subst Abuse Treat200733718017588491
- Sanchez-CraigMAnnisHMBornetARMacDonaldKRRandom assignment to abstinence and controlled drinking: evaluation of a cognitive-behavioral program for problem drinkersJ Consult Clin Psychol1984523904036747058
- AmbrogneJAReduced-risk drinking as a treatment goal: what clinicians need to knowJ Subst Abuse Treat200222455311849906
- HeiligMGoldmanDBerrettiniWO’BrienCPPharmacogenetic approaches to the treatment of alcohol addictionNat Rev Neurosci20111267068422011682
- LuquiensAReynaudMAubinHJIs controlled drinking an acceptable goal in the treatment of alcohol dependence? A survey of French alcohol specialistsAlcohol Alcohol20114658659121771742
- Al-OtaibaZWordenBLMcCradyBSEpsteinEEAccounting for self-selected drinking goals in the assessment of treatment outcomePsychol Addict Behav20082243944318778138
- HodginsDCLeighGMilneRGerrishRDrinking goal selection in behavioral self-management treatment of chronic alcoholicsAddict Behav1997222472559113218
- BarryMJEdgman-LevitanSShared decision making – pinnacle of patient-centered careN Engl J Med201236678078122375967
- Cochrane Collaboration2011Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0.2011
- McMillanSSKendallESavAPatient-centered approaches to health care: a systematic review of randomized controlled trialsMed Care Res Rev20137056759623894060
- MdegeNDFayterDWatsonJMStirkLSowdenAGodfreyCInterventions for reducing alcohol consumption among general hospital inpatient heavy alcohol users: a systematic reviewDrug Alcohol Depend201313112223474201
- Bazargan-HejaziSBingEBazarganMEvaluation of a brief intervention in an inner-city emergency departmentAnn Emerg Med200546677615988430
- BischofGGrothuesJMReinhardtSMeyerCJohnURumpfHJEvaluation of a telephone-based stepped care intervention for alcohol-related disorders: a randomized controlled trialDrug Alcohol Depend20089324425118054443
- BrownTGDongierMOuimetMCBrief motivational interviewing for DWI recidivists who abuse alcohol and are not participating in DWI intervention: a randomized controlled trialAlcohol Clin Exp Res20103429230119930236
- CareyKBCareyMPMaistoSAHensonJMBrief motivational interventions for heavy college drinkers: a randomized controlled trialJ Consult Clin Psychol20067494395417032098
- ChangGFisherNDHornsteinMDBrief intervention for women with risky drinking and medical diagnoses: a randomized controlled trialJ Subst Abuse Treat20114110511421489738
- CherpitelCJKorchaRAMoskalewiczJSwiatkiewiczGYeYBondJScreening, brief intervention, and referral to treatment (SBIRT): 12-month outcomes of a randomized controlled clinical trial in a Polish emergency departmentAlcohol Clin Exp Res2010341922192820659072
- DaeppenJ-BGaumeJBadyPBrief alcohol intervention and alcohol assessment do not influence alcohol use in injured patients treated in the emergency department: a randomized controlled clinical trialAddiction20071021224123317565563
- DaeppenJBBertholetNGaumeJFortiniCFaouziMGmelGEfficacy of brief motivational intervention in reducing binge drinking in young men: a randomized controlled trialDrug Alcohol Depend2011113697520729010
- D’OnofrioGPantalonMVDegutisLCBrief intervention for hazardous and harmful drinkers in the emergency departmentAnn Emerg Med200851742750.e74218436340
- EmmenMJSchippersGMWollersheimHBleijenbergGAdding psychologist’s intervention to physicians’ advice to problem drinkers in the outpatient clinicAlcohol Alcohol20054021922615699056
- GaumeJGmelGFaouziMBertholetNDaeppenJ-BIs brief motivational intervention effective in reducing alcohol use among young men voluntarily receiving it? A randomized controlled trialAlcohol Clin Exp Res2011351822183021777259
- HansenABBeckerUNielsenASGronbaekMTolstrupJSBrief alcohol intervention by newly trained workers versus leaflets: comparison of effect in older heavy drinkers identified in a population health examination survey: a randomized controlled trialAlcohol Alcohol201247253221949192
- LeeCSLópezSRHernándezLA cultural adaptation of motivational interviewing to address heavy drinking among HispanicsCultur Divers Ethnic Minor Psychol201117331732421787064
- MurphyJGDuchnickJJVuchinichRERelative efficacy of a brief motivational intervention for college student drinkersPsychol Addict Behav20011537337911767271
- MurphyJGBensonTAVuchinichREA comparison of personalized feedback for college student drinkers delivered with and without a motivational interviewJ Stud Alcohol20046520020315151350
- SenftRAPolenMRFreebornDKHollisJFBrief intervention in a primary care setting for hazardous drinkersAm J Prev Med1997134644709415794
- SoderstromCADiClementeCCDischingerPCA controlled trial of brief intervention versus brief advice for at-risk drinking trauma center patientsJ Trauma200762110217495708
- AaltoMSaksanenRLainePBrief intervention for female heavy drinkers in routine general practice: a 3-year randomized, controlled studyAlcohol Clin Exp Res2000241680168611104115
- AaltoMSeppaKMattilaPBrief intervention for male heavy drinkers in routine general practice: a three-year randomized controlled studyAlcohol Alcohol20013622423011373259
- AllenEPolikinaOSaburovaLThe efficacy of a brief intervention in reducing hazardous drinking in working age men in Russia: the HIM (Health for Izhevsk men) individually randomised parallel group exploratory trialTrials20111223822053775
- BeichAGannikDSaelanHThorsenTScreening and brief intervention targeting risky drinkers in Danish general practice – a pragmatic controlled trialAlcohol Alcohol20074259360317855332
- BrownRLSaundersLABobulaJAMundtMPKochPERandomized-controlled trial of a telephone and mail intervention for alcohol use disorders: three-month drinking outcomesAlcohol Clin Exp Res2007311372137917550366
- CurrySJLudmanEJGrothausLCDonovanDKimEA randomized trial of a brief primary-care-based intervention for reducing at-risk drinking practicesHealth Psychol20032215616512683736
- D’OnofrioGFiellinDAPantalonMVA brief intervention reduces hazardous and harmful drinking in emergency department patientsAnn Emerg Med20126018119222459448
- HermanssonUHelanderABrandtLHussARönnbergSScreening and brief intervention for risky alcohol consumption in the workplace: results of a 1-year randomized controlled studyAlcohol Alcohol20104525225720406791
- LongabaughRWoolardRENirenbergTDEvaluating the effects of a brief motivational intervention for injured drinkers in the emergency departmentJ Stud Alcohol20016280681611838918
- MaistoSAConigliaroJMcNeilMKraemerKConigliaroRLKelleyMEEffects of two types of brief intervention and readiness to change on alcohol use in hazardous drinkersJ Stud Alcohol20016260561411702799
- MelloMJBairdJNirenbergTDLeeCWoolardRLongabaughRDIAL: a randomised trial of a telephone brief intervention for alcoholInj Prev201319444822627778
- MontiPMBarnettNPColbySMMotivational interviewing versus feedback only in emergency care for young adult problem drinkingAddiction20071021234124317565560
- NoknoySRangsinRSaengcharnchaiPTantibhaedhyangkulUMcCambridgeJRCT of effectiveness of motivational enhancement therapy delivered by nurses for hazardous drinkers in primary care units in ThailandAlcohol Alcohol20104526327020236990
- SellmanJDSullivanPFDoreGMAdamsonSJMacEwanIA randomized controlled trial of motivational enhancement therapy (MET) for mild to moderate alcohol dependenceJ Stud Alcohol20016238939611414349
- SommersMSLyonsMSFargoJDEmergency department-based brief intervention to reduce risky driving and hazardous/harmful drinking in young adults: a randomized controlled trialAlcohol Clin Exp Res2013371753176223802878
- Project MATCH secondary a priori hypotheses. Project MATCH Research GroupAddiction199792167116989581001
- Team UREffectiveness of treatment for alcohol problems: findings of the randomised UK alcohol treatment trial (UKATT)BMJ200533154116150764
- ShakeshaftAPBowmanJABurrowsSDoranCMSanson-FisherRWCommunity-based alcohol counselling: a randomized clinical trialAddiction2002971449146312410785
- MannKBladstromATorupLGualAvan den BrinkWExtending the treatment options in alcohol dependence: a randomized controlled study of as-needed nalmefeneBiol Psychiatry20137370671323237314
- GualAHeYTorupLvan den BrinkWMannKthe ESGA randomised, double-blind, placebo-controlled, efficacy study of nalmefene, as-needed use, in patients with alcohol dependenceEur Neuropsychopharmacol2013231432142323562264
- KarhuvaaraSSimojokiKVirtaATargeted nalmefene with simple medical management in the treatment of heavy drinkers: a randomized double-blind placebo-controlled multicenter studyAlcohol Clin Exp Res2007311179118717451401
- HeinalaPAlhoHKiianmaaKLonnqvistJKuoppasalmiKSinclairJDTargeted use of naltrexone without prior detoxification in the treatment of alcohol dependence: a factorial double-blind, placebo-controlled trialJ Clin Psychopharmacol20012128729211386491
- KranzlerHRTennenHArmeliSTargeted naltrexone for problem drinkersJ Clin Psychopharmacol20092935035719593174
- RollnickSMillerWRWhat is motivational interviewing?Behav Cogn Psycoth199523325334
- SinclairJChickJSorensenPKieferFBatelPGualACan alcohol dependent patients adhere to an ‘as-needed’ medication regimen?Eur Addict Res20142020921724557083
- FoxcroftDRCoombesLWoodSAllenDAlmeida SantimanoNMMotivational interviewing for alcohol misuse in young adultsCochrane Database Syst Rev20148CD00702525140980
- World Health OrganizationAlcohol in the European Union: Consumption, Harm and Policy Approaches 20122012 Available from: http://www.euro.who.int/__data/assets/pdf_file/0003/160680/e96457.pdfAccessed December 1, 2015
- KohnRSaxenaSLevavISaracenoBThe treatment gap in mental health careBull World Health Organ20048285886615640922
- McQueenJHoweTEAllanLMainsDHardyVBrief interventions for heavy alcohol users admitted to general hospital wardsCochrane Database Syst Rev2011CD00519121833953
- van den BrinkWSorensenPTorupLMannKGualAthe SSGLong-term efficacy, tolerability and safety of nalmefene as-needed in patients with alcohol dependence: a 1-year, randomised controlled studyJ Psychopharmacol20142873374424671340