
Abstract
Objectives
This study aimed to assess the reliability and validity of the Chinese version of the 10-item Perceived Efficacy in Patient–Physician Interaction (PEPPI-10) scale in hospitalized patients with severe knee osteoarthritis in the People’s Republic of China.
Methods
Between January and March 2015, the Chinese versions of PEPPI, self-efficacy for exercise scale, osteoporosis self-efficacy scale, and modified fall efficacy scale were applied to assess 110 severe knee osteoarthritis patients who were hospitalized in the second ward of the department of arthroplasty surgery of Tianjin Hospital.
Results
The Chinese version of the PEPPI-10 scale had a high coefficient of internal consistency (Cronbach’s α coefficient, 0.907). The score of the Chinese version of PEPPI was weakly correlated with the scores of the Chinese versions of self-efficacy for exercise scale, osteoporosis self-efficacy scale, and modified fall efficacy scale.
Conclusion
The Chinese version of the PEPPI-10 scale exhibits sufficient internal consistency and convergent validity in hospitalized patients with severe knee osteoarthritis in the People’s Republic of China.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Background
Osteoarthritis is the most prevalent arthritic disease and affects older adult populations worldwide, and knees are the most commonly affected joints.Citation1 In its advanced stages, it may cause knee dysfunction, pain, and rigidity. In the US, it is estimated that ~27 million patients suffer from osteoarthritis every year, of whom about 10 million suffer from knee osteoarthritis.Citation2 One out of every ten people over the age of 60, on average, suffers from knee osteoarthritis. With the aging of the population in the People’s Republic of China, the incidence of knee osteoarthritis is also increasing annually.Citation3,Citation4 For 2002, the burden of osteoarthritis in disability-adjusted life years was 34,150 person years.Citation5
Since the 1970s, the patient–physician interaction has attracted extensive attention. Due to the unequal status of patients and physicians, patients are often passive, and the patient–physician relationship is very complicated.Citation6 Studies have verified that patient–physician communication can improve the satisfaction of patients, treatment persistency, understanding of medical information, quality of life, and even health.Citation7 Effective patient–physician communication has been shown to be associated with a broad range of improved outcomes of care.Citation8,Citation9 The confidence of patients in communicating with physicians can significantly affect the quality of the patient–physician relationship to a certain extent.Citation10 Another study found that the Perceived Efficacy in Patient–Physician Interaction (PEPPI)-5 (the five item version of PEPPI) was strongly correlated with perceived health management skills, and moderately with social support and psychosocial aspects of health.Citation11 Good patient–physician interaction has been shown to be associated with improved satisfaction with care and health outcomes.Citation12
Self-efficacy is the belief that one can successfully take appropriate and meaningful action.Citation13 The English version of the PEPPI scale is used to test the confidence of patients when they communicate with physicians. The English PEPPI scale has two versions: a full ten-item scale and a simplified five-item scale, both of which have good reliability and validity (Cronbach’s α coefficient for PEPPI-10 is 0.91, respectively, Cronbach’s α coefficient for PEPPI-5 is 0.83.Citation10 The English version of PEPPI-5 has been translated into Dutch, and its clinical feasibility has been verified.Citation11 However, further studies are required to study the differences of this scale in assessing populations of different backgrounds, races, and beliefs. Until now, no studies have investigated the application of this scale in hospitalized patients with severe knee osteoarthritis in the People’s Republic of China. This study aimed to assess the reliability and validity of the Chinese version of PEPPI-10 scale in hospitalized patients with severe knee osteoarthritis in Tianjin, People’s Republic of China.
Patients
A total of 115 patients with severe knee osteoarthritis hospitalized between January and March 2015 were included in the study. Only patients who were hospitalized for knee osteoarthritis of Kellgren–Lawrence grade III and above by X-ray were included. Patients with known cognitive impairments or literacy problems were excluded. The survey was accompanied by a cover letter and consent form explaining the purpose and voluntary nature of the study. In addition to the PEPPI-10, the survey contained questions on other self-efficacy scales. This study was approved by the Tianjin Hospital Ethics Committee and the patients and the Chinese investigators signed the informed consent before the survey.
Methods
Survey methods
The survey was performed using a method where respondents filled out the questionnaire at admission to the hospital. In the data collection process, investigators explained the survey purpose, rights, obligations, and other precautions to the eligible respondents and gained consent from the respondents. The investigators explained the requirements of the questionnaire to the respondents using uniform guidance language. The privacy of the respondents was protected during the investigation process, and all the questionnaires were collected at the time of their completion.
Survey tools
PEPPI
In this study, the ten-item PEPPI was adapted (Supplementary materials), and the English version of the PEPPI was translated into the Chinese version after obtaining consent from the author. It was then back-translated into English and the English and Chinese versions were reconciled by both Chinese- and English-speaking investigators. Compared to the English version, the Chinese version consisted of ten items to assess the confidence of patients when they interacted with physicians (such as get a doctor to take your chief health concern seriously, or knowing what questions to ask the physicians). Each item of the scale was translated into an initial Chinese version by two clinical experts in Tianjin. The respondents were mostly hospitalized patients with severe knee osteoarthritis, and they mainly interacted with physicians and nurses. The modified Chinese version of the PEPPI was formally determined after discussion in a team meeting. Two items of the translated PEPPI scale were raised as being of concern with regard to the Chinese words employed to describe “answer” (item 5 “Get a doctor to answer all of your questions”) and “do something with” (item 9 “Get a doctor to do something about your chief health concern”). A modified Chinese version was developed after a series of meetings with members of the study team. This procedure was intended to ensure that the Chinese version of the PEPPI scale was linguistically appropriate.Citation10 Then, preliminary tests were conducted to confirm the readability and feasibility of the scale in the actual survey by recruiting ten hospitalized patients with severe osteoarthritis.
In recent years, researchers have tested the internal consistency of the PEPPI, and have also analyzed the correlation between the scale and main psychological scales. For example, PEPPI-5 was positively but weakly correlated with perceived health management skills (Effective Musculoskeletal Consumer Scale, EC-17), mental health (the MOS 36-Item Short Form, SF-36 MCS), and support from family and friends (Arthritis Impact Measurement Scales 2, AIMS2).Citation11
Other assessment tools
The self-efficacy for exercise scale (SEE-C) was mainly used to study self-efficacy for exercise in aged people.Citation14 The Cronbach’s α coefficient of its English version was 0.92, displaying a high internal consistency. This scale consisted of nine items, and the Likert ten-grade scoring was applied, where a high score referred to a stronger exercise self-efficacy. The Cronbach’s α coefficient of the Chinese version SEE-C was 0.75, which is adequate and is applicable in clinical studies (PEPPI).Citation15 The modified fall efficacy scale (MFES) was used to assess the confidence in overcoming the fear of falling. Most of the MFES termsCitation16 were based on the fall efficacy scale,Citation17 and they consisted of 14 items to quantitatively analyze the fear of falling in daily activities for the elderly. A Likert 11-point scoring system was adopted, where 0 points referred to no confidence and 10 points referred to absolute confidence. Studies have confirmed that the MFES had good reliability and validity in the elderly population in the People’s Republic of China, with a Cronbach’s α coefficient of 0.9774.Citation18 The osteoporosis self-efficacy scale (OSES) consisted of 21 items, and was divided into two subscales: osteoporosis motion efficacy subscale (1–10) and osteoporosis calcium intake efficacy scale (11–21)Citation19 where the Cronbach’s α coefficient of each scale was 0.90, showing good internal consistency. A visual analog scoring was applied in the English version of the OSES,Citation19 where a high score referred to stronger self-efficacy in preventing osteoporosis. A Likert 11-point scoring was adopted in the revised Chinese version of the OSES, and the Cronbach’s α coefficient of this version was 0.93, suggesting a high level of internal consistency.Citation20
Statistical analysis
Statistical analyses were performed using Statistical Product and Service Solutions 19.0 (SPSS 19.0) (IBM Corporation, Armonk, NY, USA; 2010). Structural validity was examined using confirmatory factor analysis with LISREL 8.7 (Scientific Software International, Lincolnwood, IL, USA). Due to small loss of data, no missing data patterns were identified. Factor analyses were performed to assess the validity of the Chinese version of the PEPPI, in order to determine the hidden representative factors among many variables. Testing results showed that factor analyses were applicable in scales with Kaiser–Meyer–Olkin index >0.7 and P<0.05.Citation21 In this study, factors that met the requirements (eigenvalue >1) were extracted using principal component analysis and varimax rotation. The obtained component matrices were rotated using varimax rotation, and the variables that scored >0.6 were included in the factors.
Based on previous instruments assessing similar constructs of PEPPI,Citation22,Citation23 we tested the correlation coefficients of the Chinese version of PEPPI and SEE-C, MFES, OSES, age, gender, education level, marital status, and disease duration.
The reliability of the Chinese version of the PEPPI was assessed using Cronbach’s α coefficient, which refers to the mean value of the split-half reliability coefficients obtained using all possible methods to divide items and is the most common reliability measure.Citation24 A Cronbach’s α coefficient >0.7 represents a good consistency of the scale or good reliability, and the scale is applicable in clinical studies.Citation25
Results
Patients
Descriptive analyses of the data were performed with all study variables to describe the study participants. Of the 115 participants recruited, five were excluded because of missing responses to questions in the scale, resulting in a total sample size of 110. Of the study participants, 65 were female, the mean age was 63 years, and most of them were married (). The overall characteristics of the respondents were comparable to other cross-sectional surveys of patients with knee osteoarthritis.
Table 1 Sample characteristics (N=110)
Distribution
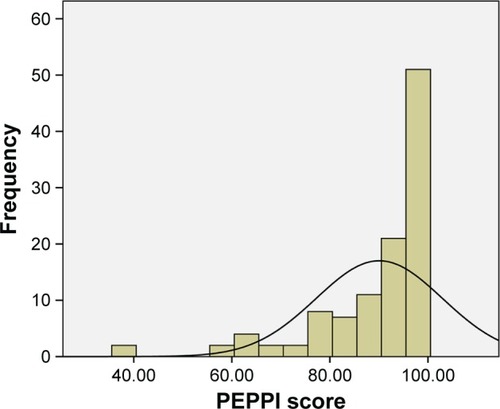
The overall score of PEPPI for the patients was relatively high. Statistical analyses were performed using SPSS 19.0 software. The results revealed that the majority of patients tended to have a high score; the skewness was −1.873 and the kurtosis was 3.773. The results of the survey showed that the Chinese version of the PEPPI was negatively skewed and mostly concentrated above the mean value (68.2%). None of the patients scored 0 points, and 31 patients (28.2%) obtained a score of 100 points (). Meanwhile, our survey results were not normally distributed due to the floor and ceiling effects.
Figure 1 Distribution of total PEPPI scores.
Abbreviation: PEPPI, Perceived Efficacy in Patient–Physician Interactions.
Factor analysis
The Cronbach’s α coefficient was 0.907, indicating sufficient internal consistency of this scale, or close correlation between the internal items in the scale. The data of the PEPPI in the 110 patients with knee osteoarthritis were analyzed, and the Kaiser–Meyer–Olkin index was found to be 0.889 and the results of the Bartlett’s test of sphericity revealed a χ2 value of 812.813 (P<0.01), where factor analysis was applicable. Two common factors with eigenvalue ≥1 were extracted using principal component analysis and varimax rotation, and the cumulative contribution rate was 71.178%. The eigenvalue of the first common factor was 6.111, and was 3.955 after rotation, including the 2–7 items, with a contribution rate of 61.105%. The eigenvalue of the second common factor was 1.007 and 3.163 after rotation, including the 1, 8–10 items, with a contribution rate of 10.073% (, ).
Figure 2 Scree plot.
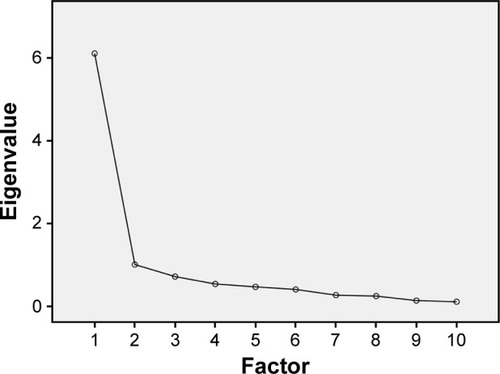
Table 2 Factor analysis of the Chinese version of PEPPI
Structural validity and internal consistency
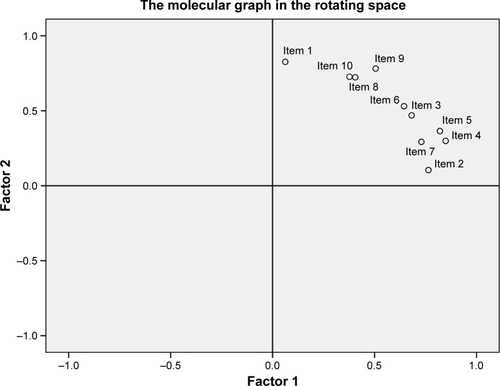
With the exception of the root mean square error of approximation, which was above the cutoff value for good fit, confirmatory factor analysis showed good fit indices for a two-factor model of the PEPPI-10 (df=33, P-value =0.000, root mean square error of approximation =0.164). Standardized factor loadings ranged between 0.75 for item 1 and 1.02 for item 2 (). The median residual correlation between the items was 0.25 and the largest residual correlation (between items 2 and 9) was 0.46. The correlation coefficient between the two factors was 0.89 ( and ).
Figure 3 Standardized factor loadings and residuals for the items of the PEPPI.
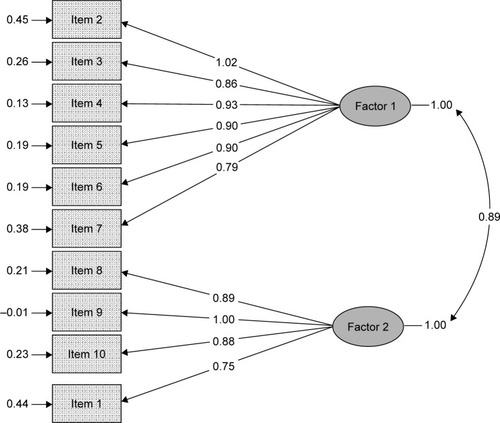
Figure 4 The correlation of main factors.
Correlation study
The Chinese version of the PEPPI was statistically, significantly, and positively correlated with other self-efficacies, including SEE-C, OSES, and MFES. The score of the Chinese version of the PEPPI was negatively correlated with age (r=−0.018, P>0.05) and disease duration (r=−0.016, P>0.05), but these relationships were not statistically significant ().
Table 3 Pearson correlations between the PEPPI and other measures
Discussion
The main purpose of this study was to introduce the PEPPI into the People’s Republic of China after translating it into the Chinese version, and to test its reliability and validity in a small sample of hospitalized patients with severe knee osteoarthritis. Our preliminary results confirmed that the Chinese version of the PEPPI has good reliability in hospitalized patients with severe knee osteoarthritis. A high internal consistency of the Chinese version of the PEPPI indicated the same measurement purpose of internal items, and confirmed the reasonability of the contents and items of the questionnaire. Factor analysis is the common and effective method of evaluating construct validity. Our study confirmed that the content of the Chinese version of PEPPI is reasonable. Our results showed that the Cronbach’s α coefficient of the Chinese version was consistent with that of the English version.Citation10 But the factor analysis result shows that the Chinese version of PEPPI-10 has two common factors, which is different from the English version of PEPPI-10.Citation10 The reason for this result may be that cultural background, social, and family roles can influence the PEPPI. The population of the People’s Republic of China is large and all patients undergoing total knee replacement need to pay a certain percentage of the cost of surgery in Tianjin. Although our study showed that the two common factors of the Chinese version of PEPPI-10 have a close relationship, analysis of the survey results showed a negative correlation between the PEPPI in hospitalized patients with severe knee osteoarthritis with age, disease duration, education level, but the correlations were not high. Due to the limited conditions, test–retest reliability was not conducted, which might have provided further evidence of the reliability of PEPPI. However, we preliminarily confirmed that the Chinese version of the PEPPI has sufficient reliability and convergent validity, and is applicable in hospitalized patients with severe knee osteoarthritis in the People’s Republic of China, with clinical value.
Due to the limited sample size, the results of this survey showed that the scores of the Chinese version of the PEPPI in our study population were negatively skewed instead of normally distributed. Therefore, we suggest the need for conducting long-term studies of the Chinese version of the PEPPI with a large sample size to promote the Chinese version in the People’s Republic of China and to identify its applicability in Chinese patients.
Correlation analysis of the Chinese version with the relevant self-efficacy scales for the orthopedic inpatients returned findings consistent with our prior assumptions, where the Chinese version of the PEPPI was positively but weakly correlated with the Chinese versions of the SEE-C, OSES, and MFES. It has been reported that self-efficacy in a specific domain does not emanate from a general sense of efficacy.Citation26 The Chinese version of the PEPPI is used to measure the PEPPI in specific environments. Due to the long-term burden of the disease, inpatients with severe knee osteoarthritis care about their own quality of life, and hope to improve their physical and mental health and quality of life in various aspects. In terms of clinical and demographic characteristics, the PEPPI score showed statistically non-significant correlations with age and disease course. This may be because most of the inpatients with severe knee osteoarthritis undergo long-term treatment, leading to skilled patient–physician interaction.
For half a century, a large number of studies on self-efficacy theory have been conducted by clinical physicians, psychologists, nursing scholars, and educators, including the establishment of self-efficacy management programs and design of the specific self-efficacy scale. Similar to other self-efficacy scales, the PEPPI was designed to assess self-efficacy for specific aspects in patients. Efficacy in the patient–physician interaction can be considered a tool to assess the effects of intervention on health treatment and adherence.Citation10
Conclusion
To our knowledge, this is the first time PEPPI was applied to assess hospitalized patients with severe knee osteoarthritis in the People’s Republic of China. Our results indicated that the Chinese version of the PEPPI can be used to measure the PEPPI in hospitalized patients with severe knee osteoarthritis. Although we found good reliability and convergent validity of the Chinese version of the PEPPI in this study, further clinical applications are required to assess its long-term merits and demerits.
Disclosure
The authors report no conflicts of interest in this work.
References
- DawsonJLinsellLZondervanKEpidemiology of hip and knee pain and its impact on overall health status in older adultsRheumatology200443449750414762225
- BurksKOsteoarthritis in older adults: current treatmentsJ Gerontol Nurs20053151119
- NIH Consensus Statement on total knee replacementNIH Consens State Sci Statements200320113417308549
- KurtzSMowatFOngKChanNLauEHalpernMPrevalence of primary and revision total hip and knee arthroplasty in the United States from 1990 through 2002J Bone Joint Surg Am20058771487149715995115
- Office of Statistics ROC Department of HealthUsing national health insurance data in Taiwan to enhance the function of national health expenditure statistics via health resource allocation approach2004 Available from: http://www.doh.gov.tw/statistic/table.xlsAccessed December 20, 2006
- ArrowKJUncertainty and the welfare economics of medical careJ Health Polit Policy Law20016851883
- FortinFKirouacSA randomized controlled trial of preoperative patient educationInt J Nurs Stud19761311241046018
- EgbertLDBattitGEWelchCEBartlenMKReduction of postoperative pain by encouragement and instruction of patientsN Engl J Med196427082582714108087
- GreenfieldSKaplanSWareJExpanding patient involvement in care: effects patient outcomesAm Intern Med19851024520528
- MalyRCFrankJCMarsballGNDiMatteoMRReubenDBPerceived Efficacy in Patient-Physician Interactions (PEPPI): validation of an instrument in older personsJ Am Geriatr Soc19984678898949670878
- KloosterPMTOostveenJCMZandbeltLCFurther validation of the 5-item Perceived Efficacy in Patient–Physician Interactions (PEPPI-5) scale in patients with osteoarthritisPatient Educ Couns201287112513021889864
- SchenkerYStewartANaBWhooleyMADepressive symptoms and perceived doctor–patient communication in the heart and soul studyJ Gen Intern Med200924555055619274477
- BanduraASelf-efficacy: toward a unifying theory of behavior changePsychol Rev1977842191215847061
- ResnickBPalmerMHJenkinsLSSpellbringAMPath analysis of efficacy expectations and exercise behavior in older adultsJ Adv Nurs20003161309131510849141
- LeeLLPerngSJHoCCHsuHMLauSCArthurAA preliminary reliability and validity study of the Chinese version of the self-efficacy for exercise scale for older adultsInt J Nurs Stud200946223023818950769
- HillKStudies of Balance in Older PeopleAustraliaThe University of Melbourne1998
- TinettiMRichmanDPowellLFalls efficacy as a measure of fear of fallingJ Gerontol1990456239243
- HaoYPLiuXQTesting of the modified fall efficacy scale in elderly population in ChinaChinese J Nurs2007421921
- HoranMLKimKKGendlerPDevelopment and evaluation of the osteoporosis self-efficacy scaleRes Nurs Health19982153954039761137
- ChenYPLiuXQA reliability and validity study of osteoporosis self-efficacy scaleNurs J PLA2005223839
- MonticoneMGiorgiIBaiardiPDevelopment of the Italian version of the tampa scale of kinesiophobia (TSK-I): cross-cultural adaptation, factor analysis, reliability, and validitySpine (Phila Pa 1976)201035121241124620216338
- ClaymanMLPanditAUBergeronARCameronKARossEWolfMSAsk, understand, remember: a brief measure of patient communication self-efficacy within clinical encountersJ Health Commun201015Suppl 2727920845194
- HanWTCollieKKoopmanCAzarowJBreast cancer and problems with medical interactions: relationships with traumatic stress, emotional self-efficacy, and social supportPsychooncology200514431833015386762
- CronbachLJCoefficient alpha and the internal structure of testsPsychometrika1951163297334
- CrotinaJMWhat is coefficient alpha? An examination of theory and applicationsJ Appl Psychol199378198104
- MadduxJEGosselinJTSelf-efficacyLearyMRTangneyJPHandbook of Self and IdentityNew YorkThe Guilford Press2003218238