
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Objectives
To assess disease-modifying therapy (DMT) preferences in a population of patients with multiple sclerosis (MS) and to estimate the association between sociodemographic and clinical factors and these preferences.
Methods
Preferences for DMTs attributes were measured using a discrete choice experiment. Analysis of preferences was assessed using mixed-logit hierarchical Bayes regression. A multilinear regression was used to evaluate the association between the preferences for each attribute and patients’ demographic and clinical characteristics. A Student’s t-test or Welch’s t-test was used for subgroup comparisons.
Results
A total of 125 patients were included in the final analysis (62.9% female, mean age 44.5 years, 71.5% with relapsing-remitting MS diagnosis). The most important factor for patients was the possibility of suffering from the side effects of the treatment (relative importance [RI] =50%), followed by a delay in disease progression (RI =19.4%), and route and frequency of administration (RI =14.3%). According to maximum acceptable risk, patients were willing to accept an increase of 3.8% in severity of side effects, for a delay of 1 year in disease progression. Treatment duration was the most prevalent factor affecting preferences, followed by the age of patients, type of MS, level of education, and the type of current treatment. Patients treated orally were significantly more concerned about the route and frequency of administration (P=0.026) than patients on injectable therapy. Naïve patients stated significantly less importance to prevention of relapses (P=0.021) and deterioration of the capacity for performing usual daily life activities (P=0.015). Finally, patients with >5 years since diagnosis were significantly less concerned about preventing disease progression (P=0.021), and more concerned about treatment side effects (P=0.052) than compared with patients with <5 years of MS history.
Conclusion
The most important attribute for MS patients was side effects of DMTs, followed by delay in disability progression. Experience with DMTs and time since MS diagnosis changed patients’ preferences. These results give information to adjust new DMT treatment in order to satisfy patients’ preferences and therefore, improve adherence to treatment.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating disease of the central nervous system characterized by inflammation and axonal degeneration. It is the most common neurologic disability in young adults.Citation1 Nearly 90% of MS patients initially experience a relapsing-remitting MS (RRMS), characterized by neurological dysfunction episodes followed by disease remission and stability.Citation2 Over time, nearly 50% of RRMS patients gradually develop secondary progressive MS (SPMS), characterized by permanent disability.Citation2 In 10%–20% of patients, MS gradually gets worse from the onset of symptoms, without early relapses or remissions, representing a primary progressive MS (PPMS).Citation2
Disease-modifying therapies (DMTs) are considered a key component of comprehensive MS care.Citation3 However, even though there is wide evidence of the benefits of DMTs in the reduction of frequency and severity of MS relapses and in slowing disease progression,Citation3–Citation5 treatment discontinuation in MS patients is common.Citation6 Medication adherence and persistence have been associated with better clinical outcomes and lower MS-related medical costs.Citation7 Treatment adherence should be considered a crucial factor in the management of these patients. It has been suggested that patient-reported outcomes may be improved by matching the treatment with the preferences and expectations of the patients.
The therapeutic options for MS have significantly increased during recent years,Citation4 and each treatment has its unique risks and benefits.Citation5 For this reason, deciding on the most suitable therapeutic strategy is becoming a more complex process for both patients and physicians. Some studies report a substantial disparity between physicians’ and patients’ perspectives.Citation8 This underlies the need to elucidate patients’ preferences regarding their treatment, and involve them in the decision-making process. Moreover, when more than one reasonable treatment option is available, patients’ preferences become more important in decision making.Citation9
Over the past two decades, the number of publications on health-related discrete choice experiments (DCE) providing insight into patients’ preferences has increased dramatically.Citation10 These reports highlight the importance of eliciting and incorporating patient preferences in treatment decision making.
The aim of this study was to perform DCE to assess MS patients’ preferences for attributes associated with DMTs and to estimate the association between sociodemographic and clinical factors and these preferences.
Methods
DCE
Stated-preference methods in the form of DCE are widely used in outcomes research. They allow the identification and evaluation of patient preferences for treatment and their relative importance in decision making.Citation11 In DCE, patients choose between two hypothetical treatment alternatives described by attributes and their corresponding levels. Attributes may include effectiveness, safety, and route and frequency of drug administration. Attribute levels describe the possible values associated with each attribute.Citation11
The DCE was applied according to the International Society for Pharmacoeconomics and Outcomes Research (ISPOR) good practices recommendations for conjoint analysis in health.Citation12
Attributes and levels selection
The full set of possible attributes and levels that characterized the profiles to be evaluated in the DCE were initially identified through a literature review. Key terms were used () to search international free-access databases recommended by the Cochrane Handbook for systematic reviews of interventionsCitation13 (MEDLINE/PubMed, Cochrane Library, ISI Web of Knowledge). The studies that assessed the preferences of MS patients for DMT attributes, published until December 31, 2014, were reviewed. A total of six previous studies related to MS patient preferences were identified.Citation14–Citation19
After literature review and the identification of potential attributes to include in the DCE, individual semistructured interviews by telephone with two MS specialists with vast experience in the management of MS and three MS patients were conducted. The main purpose of the semistructured interviews was to validate the potential attributes identified in the literature, to assess their relevance for MS Spanish population, to identify attributes not retrieved in the literature but relevant for MS Spanish population, and finally to assess the comprehensibility of the attributes and levels proposed. The result of literature review and semistructured interviews produced six attributes with a maximum of three levels each ().
Table 1 Final attributes and levels used in the discrete choice experiment
Experimental design and survey instrument
The support.CEs package for R statistical software (Hideo Aizaki, Tsukuba, Japan) environmentCitation20 was used to generate the DCE design. Following the recommendation of ISPOR good practices for conjoint analysis in health,Citation12 the design was orthogonal (all attributes levels vary independently and are not correlated) and balanced (each level of an attribute occurs the same number of times). Two attributes (frequency and route of administration) were redefined into one (“mode and frequency of administration”) in order to avoid illogical combinations, including only realistic levels. The fractional factorial analysis (main effects orthogonal matrix) generated 36 scenarios, with a mix-and-match algorithm being used to generate the choice sets. Stated preferences were used to identify and minimize the number of dominated scenarios. presents an example of the choice set.
Table 2 Example of the choice set
To avoid participant fatigue, the inclusion of between 8 and 16 choice sets is recommended.Citation12 For this reason, the 36 scenarios were distributed among three versions of questionnaires of 12 multiple-choice sets each.
In addition to the choice sets, the survey instrument collected patients’ sociodemographic and clinical variables. Each participant received a randomly assigned version of the questionnaire.
Before answering the questionnaire, all participants received a clear explanation stating that all presented treatments scenarios were hypothetical.
Study participants
Patients with MS were contacted through Spanish MS patient associations and invited by e-mail. The participants received a personal access password and the link to the electronic questionnaire that was hosted in a website. The questionnaire was available between September 2015 and November 2015.
All patients provided written informed consent to participate in the study. Their data were treated confidentially and dissociated in accordance with Spanish regulations (15/1999 Personal Data Protection Law). Patients were blinded to the sponsor of the study and no incentives were offered to any of the participants for questionnaire completion.
Patients aged 18 years or older with a diagnosis of RRMS or SPMS (MS type was reported by the patient and not confirmed by any other data source) were included in the study.
Study sample and data collection procedures
The minimum sample size necessary for the DCE was established according to a rule-of-thumb and recommendation proposed by OrmeCitation21
, where n is the number of respondents, t is the number of tasks (t=36 scenarios), a is the number of alternatives per task (a=2 alternatives), and c is the largest number of levels for any one attribute (c=3 maximum number of levels). As a result, a minimum number of 125 MS patients had to complete the survey.
Statistical analyses
Analysis of preferences was assessed using a mixed-logit model (random parameters logit) (RSGHB R packageCitation22). This model enhances the multinomial logit by allowing the coefficients to randomly vary across respondents, thus leading to individual sets of utility values rather than mean preferences, which foster more accurate further analysis.
Statistical analyses of patient characteristics were performed using SPSS 20.0 (IBM Corporation, Armonk, NY, USA). Possible explanatory variables for the preferences were analyzed by consecutively evaluating the individual partial utility values and the relative importance of the attributes (as dependent variables) against the potential explanatory variables (individuals’ demographic or clinical facts). After analyzing possible correlations between them (Pearson’s correlation coefficients), multilinear regressions (stepwise method) were applied to the dependent variables using the demographic and clinical factors as independent. The Student’s t-test or Welch’s t-test (whether for equal or unequal variances) were run to assess subgroup comparisons as suggested by the stepwise results. In case of more than two subgroups, analysis of variance with a least significant difference post hoc test was performed.
Maximum acceptable risk (MAR) was estimated as the quotient between two utility differences, one associated with an improvement in outcomes and the other with a less desirable attribute.Citation23
Ethical consideration
The study followed the principles of the Declaration of Helsinki. It was developed to ensure compliance with good clinical practices, in keeping with the principles of the Tripartite Harmonized International Conference on Harmonization GuidelineCitation24 (International Conference on Harmonization, 1996). The study protocol was submitted to the Spanish Agency of Medicines and Medical Devices (Agencia Española del Medicamento y Productos Sanitarios) for classification and to the Clinical Research Ethics Committee of Bellvitge University Hospital (Barcelona) for approval, which was granted.
Results
Patient demographics
One hundred and forty-six patients completed the electronic questionnaire. Of these, 125 patients were included in the final data analysis. Twenty-one patients (14%) with a PPMS diagnosis were excluded from the analysis after the study selection criteria were applied. Given that patients were contacted through patient associations, no previous verification of their MS diagnosis could be done until data analysis.
The mean age of participants was 44.5 years (standard deviation [SD]: 10.9), most of whom were females (62.9%) and married or living with a partner (63.2%). Half of the participants had completed higher education (university or postgraduate) and 36.8% were employed. Mean time since MS diagnosis was 13.4 years (SD: 7.9). Most of the participants had a RRMS diagnosis (71.5%). Among current treatment, the most common current route of administration was oral (43.4%), followed by subcutaneous (26.3%). Mean time on MS treatment (time since MS treatment initiation) was 9.3 years (SD: 6.2), and the mean time on current treatment was 4.3 years (SD: 5.2). Ten patients (8%) had never received MS treatment. Mean time between patients’ MS diagnosis and the initiation of MS treatment was 4.8 years (SD: 7.3) ().
Table 3 Participant sociodemographic and clinical characteristics (n=125)
MS patients’ preferences for DMT attribute levels
and show the results of the mixed logit of patient preferences for DMTs. To obtain the partial utilities (preference scores expressed as odds ratios [ORs]) for levels within the attributes, beta coefficients from the mixed logit were exponentiated. All levels addressing route and frequency of administration, disease progression, side effects, and daily life activities were statistically significant as determinants of patients’ preferences. Relapse prevention and treatment follow-up were not significantly associated with preferences.
Figure 1 Preferences for levels within each attribute.
Abbreviations: IM, intramuscular; OR, odds ratio; ref, reference; SC, subcutaneous.
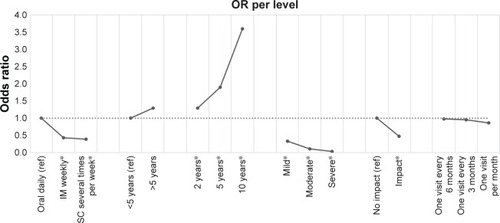
Table 4 MS patient preferences
The results of the analysis showed that subcutaneous treatment administered several times a week (OR: 0.428; P<0.01) and intramuscular injections given weekly (OR: 0.389; P<0.01) was less preferred, compared with daily oral administration. As expected, higher treatment efficacy (reduction of disability progression over 10 years vs reduction of disability over 2 years) (OR: 3.597; P<0.01) was preferred. Treatments associated with severe side effects (serious or life-threatening) (OR: 0.034; P<0.01) or that significantly compromised patients’ daily life (OR: 0.468; P<0.01) were less preferred.
Relative importance of each attribute
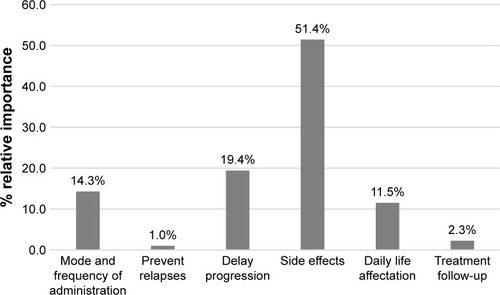
The relative importance of each attribute was calculated to establish their importance in treatment decision making.
Among all of the attributes studied, the probability of suffering treatment side effects was the most important attribute to patients, and influenced half of their decision-making processes. Delayed progression and route and frequency of administration were also important for patients’ decisions, representing 19.4% and 14.3% of importance, respectively ().
Figure 2 Relative importance in patients’ decisons.
Maximum acceptable risk
By estimating the MAR, the maximum risk that patients are willing to accept in order to achieve a therapeutic benefit of pharmacotherapy can be assessed.Citation25 Patients were willing to accept a severity increase of 3.8% in side effects for a delay of 1 year in disease progression.
Factors defining preferences
Explanatory variables for the revealed preferences were analyzed using stepwise multilinear regression. When partial utilities (preference scores) were used as dependent variables, and sociodemographic and clinical characteristics as independent variables, the results () showed that actual duration of treatment was the most prevalent factor affecting preferences, followed by patient age, type of MS, level of education and the type of treatment currently received. shows the variation in patients’ preferences regarding the side effects according to patients’ age and level of education. Older patients were more concerned about side effects. On the other hand, people with higher education were less concerned about side effects development. shows that patients who had been receiving their current treatment for longer duration were more willing to accept subcutaneous treatment several times per week or intramuscular weekly. This preference was stronger when patients had a RRMS diagnosis, compared with a SPMS diagnosis.
Figure 3 Preference for side effects by patients’ age and level of education.
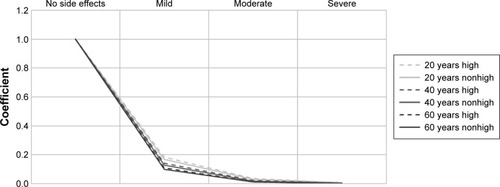
Figure 4 Preference for the route and frequency of administration by duration of the current treatment and type of multiple sclerosis.
Abbreviations: MS, multiple sclerosis; RR, relapse-remitting; RRMS, relapsing-remitting MS; SPMS, secondary-progressive MS; SP, secondary progressive.
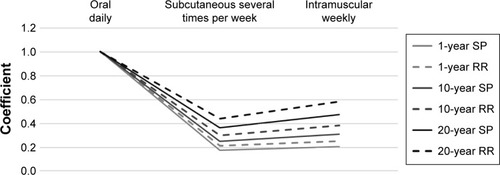
Table 5 Stepwise multilinear regression of partial utilities
When the relative importance of the attributes were used as dependent variables, the regression showed that actual treatment duration was again the most influential factor, followed by educational level and age ().
Table 6 Stepwise multilinear regression of relative importance
Regression analysis results suggested that it would be interesting to make comparisons between subgroups, so we proceeded to conduct these analyses.
Current route of administration
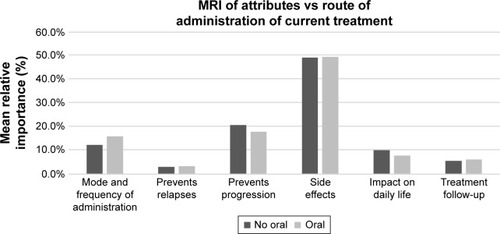
A total of 99 patients of the study population were receiving treatment during the study and included for analysis. The analysis (t-tests for independent samples) of the subgroup of patients that were receiving treatment (n=99, ) showed that patients treated orally (n=43) were significantly more concerned about the route and frequency of administration (15.9% vs 12.1%, P=0.026) than other patients (n=47) and, in a less significant but also relevant measure, they differed in the importance assigned to the impact on daily life (7.7% vs 9.9%, P=0.09) ().
Figure 5 MRI of attributes by route of administration.
Previous experience with treatment
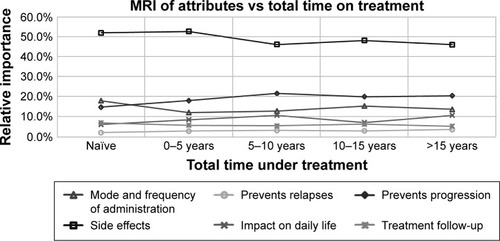
Patients were divided into five groups depending on their experience on treatment (naïve [n=10], 0–5 years [n=29], 5–10 years [n=30], 10–15 years [n=28], and >15 years [n=24]) and the analysis of variance test was performed. Although no significant differences were revealed at a P≤0.05 level, preferences changed in naïve patients with respect to the other patients (). A Welch’s t-test was conducted to evaluate differences between naïve and experienced patients. Naïve patients gave significantly less importance to prevention of relapses (2.1% vs 3.1%; P=0.021), deterioration of ability to perform usual daily life activities (6.1% vs 9.2%; P=0.015), and prevention of progression (14.8% vs 20.0%). They were more concerned about the route and frequency of administration (18.0% vs 13.4%), side effects (52.0% vs 48.6%), and treatment follow-up (7.0% vs 5.8%).
Figure 6 MRI of attributes by total time on treatment.
Time since MS diagnosis
Patients with <5 years of MS history (n=15) were significantly less concerned about preventing progression than patients with 5 or more years since diagnosis (n=109) (13.5% vs 20.3%; P=0.021), and more concerned about treatment side effects (54.8% vs 48.3%; P=0.052).
Discussion
This study explored Spanish MS patients’ preferences for DMT characteristics. The study population had a mean age, sex and MS type comparable with national MS statistics.Citation26
In line with previous studies, the results of this DCE revealed that treatment side effects were the most important attribute defining DMT preferences. Recently, Wicks et alCitation27 reported that in oral DMT-naïve patients, liver toxicity, severe side effects, and common side effects were the attributes that emerged as the most important drivers of patients’ preferences; and patients expressed greater preference for product profiles with fewer serious side effects and fewer common side effects compared with those with higher efficacy. Similarly, Wilson et alCitation19 found that severe side effect risks had a higher impact on RRMS patient preferences. Furthermore, patients were willing to accept a relatively greater risk of death/disability as long as the benefit gained was substantial.
With regard to treatment efficacy, our findings showed that a delay in years to disability progression was the second most important DMT attribute in treatment choice. In contrast, relapse prevention was the least important DMT attribute. Several studies reported similar results, showing that MS patients strongly preferred preventing long-term disability progression over preventing relapses.Citation14,Citation19,Citation27,Citation28 According to the MAR assessed in this study, MS patients were willing to accept a change in the severity of side effects from mild to moderate or moderate to severe (33% increment in severity) in order to delay disease progression by 10 years.
This study also aimed to elicit patient preferences regarding DMT route and frequency of administration, showing that, as observed in previous studies,Citation19 patients strongly preferred oral daily medications compared with other routes and frequencies.
Subgroup analysis showed that experience with MS and MS treatment changes patients’ perceptions and values. Patients receiving oral treatment gave more importance to the route and frequency of administration than patients currently on injectable therapies. A review published by Bansback et alCitation29 showed that experienced patients on treatments for rheumatic diseases who perceived their routes of administration as fairly convenient assigned lower values to more suitable treatments.
Despite the small group of naïve patients (n=10) in this study, the results suggested that these patients gave less importance to the attributes related to treatment efficacy, and were more concerned about the route and frequency of administration and treatment-related side effects. A study performed in the Netherlands to gain insight into the reasons why MS patients use or do not use DMTs showed that for naïve patients, awareness about possible side effects was the most important reason for not adopting DMTs. In contrast with our findings, these authors observed that neither the route nor frequency of treatment administration were related to the patients’ decision to not start a DMT.Citation30 Instead, time since diagnosis also affected patients’ treatment preferences. Thus, results from our study showed that compared with patients with >5 years since diagnosis, patients who were more recently diagnosed (<5 years) worried more about side effects of treatment and were less concerned about treatment efficacy in the delay of MS progression.
The study results highlight the importance of eliciting and incorporating patient preferences in treatment decision making and evidence that, in order to improve treatment adherence and satisfaction, physicians should discuss with patients on their preferences of therapy options.
Study limitations
Our study had limitations. Although DCE is the recommended approach and it is widely used to assess patient preferences for treatment characteristics, there is always the risk of a gap between stated and revealed preferences.Citation12,Citation31 Half of the study participants had completed higher education, but uncertainty in interpreting the scenarios may have existed which could have affected the results. Despite the selection of the choice levels being performed according to the ISPOR recommendations, and after semistructured interviews with MS experts and MS patients, some relevant attributes for patients may have been omitted from this study and some of the attributes might not match the currently available treatments. For this reason, all participants received a clear explanation before answering the questionnaire stating that all presented treatments were hypothetical and in no case were to be compared against their current treatment.
Moreover, in order to reduce the complexity of the DCE, and as performed in previous studies,Citation28,Citation32 in this analysis a decision was made to limit the number of attributes. For this reason, route and frequency of administration were presented combined in the same attribute. This could be a possible limitation of the study, since Utz et alCitation18 published that the preference for oral DMTs changes when the frequency of the oral treatment is substantially higher than the frequency of injectable treatment. Even though the classification of side effects used in the study is not necessarily suited to categorize side effects in daily practice, semistructured interviews with patients and MS physicians revealed that, since severity of side effects is perceived differently for each patient, it will be more easy for them to evaluate each level of this attribute using the description of mild, moderate, and severe instead of describing side effects such as headache or flu-like symptoms. Due to the small sample size of some study subgroups, any extrapolation of results should be done with caution. Further research regarding preferences of patients in these subgroups is warranted. The comparison between patients’ subjective thoughts and physicians’ data may increase the strength of our results, however, since patients were contacted through patient’s associations, physicians’ data were not available, and this comparison was not possible to be performed. Finally, these results should be interpreted within the context of the study.
Conclusion
Our findings indicate that the most important attributes for MS patients were treatment side effects and the delay in progression of disability.
Experience with DMTs changed patients’ preferences. Patients receiving oral treatment gave more importance to the route and frequency of administration than patients treated with injectable therapies. Naïve patients were also concerned about this attribute in addition to treatment side effects, giving less importance to attributes related to treatment efficacy.
Time since MS diagnosis also affected patients’ preferences, with more recently diagnosed patients being more concerned about side effects than patients diagnosed >5 years ago. These results are important since they give information to adjust new DMT treatment in order to satisfy patients’ preferences and therefore, improve adherence to treatment.
Author contributions
All authors oversaw the development of the study, and the analysis and interpretation of results. They significantly contributed to the conception, design, progress, and conclusion of the study. All authors critically reviewed preliminary drafts for important intellectual content and contributed to its final version. They all gave final approval of the version being submitted.
Acknowledgments
This study was funded by Merck Serono. We are very grateful to all the patient associations and the study participants who devoted their time to participating in this research.
Supplementary material
Table S1 Search terms and search strategy
Disclosure
The study was sponsored by Merck Serono, Spain, a subsidiary of Merck KGaA, Darmstadt, Germany. The authors report no other conflicts of interest in this work.
References
- MurrayTJDiagnosis and treatment of multiple sclerosisBMJ2006332754052552716513709
- TremlettHZhaoYRieckmannPHutchinsonMNew perspectives in the natural history of multiple sclerosisNeurology201074242004201520548045
- CrossAHNaismithRTEstablished and novel disease-modifying treatments in multiple sclerosisJ Intern Med2014275435036324444048
- GajafattoABenedettiMDTreatment strategies for multiple sclerosis: when to start, when to change, when to stop?World J Clin Cases20153754555526244148
- LugaresiAdi IoiaMTravagliniDPietrolongoEPucciEOnofrjMRisk-benefit consideration in the treatment of relapsing-remitting multiple sclerosisNeuropsychiatr Dis Treat2013989391423836975
- TobinWWeinshenkerBGStopping immunomodulatory medications in MS: frequency, reasons and consequencesMult Scler Relat Disord20154543744326346792
- LizánLComellasMPazSPovedaJLMeleticheDMPolancoCTreatment adherence and other patient-reported outcomes as cost determinants in multiple sclerosis: a review of the literaturePatient Prefer Adherence201481653166425525341
- RiñonABuchMHolleyDVerdunEThe MS choices survey: findings of a study assessing physician and patient perspectives on living and managing multiple sclerosisPatient Prefer Adherence2011562964322259240
- MendelRTraul-MattauschEFreyDDo physicians’ recommendations pull patients away from their preferred treatment options?Health Expect2012151233121323824
- Clark DetermannDPetrouSMoroDBekker-GrobEWDiscrete choice experiments in health economics: a review of the literaturePharmacoeconomics201432988390225005924
- JohnsonRFLancsarEMarshallDConstructing experimental design for discrete-choice experiments: report of the ISPOR conjoint analysis experimental design good research practices task forceValue Health201316131323337210
- BridgesJFPHauberABMarshallDConjoint analysis applications in health: a checklist of the ISPOR good research practices for conjoint analysis task forceValue Health201114440341321669364
- HigginsJPTGreenSCochrane handbook for systematic reviews of interventions version 5.1.0 updated March 2011The Cochrane Collaboration2011 Available from: http://handbook.cochrane.org/
- JohnsonFRVan HoutvenGÖzdemirSMultiple sclerosis patient’s benefit-risk preferences: serious adverse event risks versus treatment efficacyJ Neurol2009256455456219444531
- HansonKAAgashivalaNWyrwichKWRaimundoKKimEBrandesDWTreatment selection and experience in multiple sclerosis: survey of neurologistsPatient Prefer Adherence2014841542224729689
- Glass-MarmorLPapernaTBen-YosefYMillerAChronotherapy using corticosteroids for multiple sclerosis relapsesJ Neurol Neurosurg Psychiatry200778888688817056624
- ShinglerSLSwinburnPAliSPerardRLloydAJA discrete choice experiment to determine patient preferences for injection devices in multiple sclerosisJ Med Econ20131681036104223730944
- UtzKSHoogJWentrupAPatient preferences for disease-modifying drugs in multiple sclerosis therapy: a choice-based conjoint analysisTher Adv Neurol Disord20147626327525371708
- WilsonLLoucksABuiCPatient centered decision making: use of conjoint analysis to determine risk-benefit trade-offs for preference sensitive treatment choicesJ Neurol Sci20143441–2808725037284
- AizakiHBasic functions for supporting an implementation of choice experiments in RJ Stat Softw201250212425317082
- OrmeBGetting Started with Conjoint Analysis: Strategies for Product Design and Pricing Research2nd edMadison WIResearch Publishers LLC20105766
- DumontJKellerJRSGHB: functions for hierarchical Bayesian estimation: a flexible approach Available from: https://cran.r-project.org/web/packages/RSGHB/index.htmlAccessed March 2016
- BridgesJFHauberABMarshallDConjoint analysis applications in health – a checklist: a report of the ISPOR good research practices for conjoint analysis task forceValue Health201114440341321669364
- International conference on harmonization of technical requirements for registration of pharmaceuticals for human use. ICH harmonized tripartite guideline: guideline for good clinical practice E6(R1)1996 Available from: http://www.ich.org/fileadmin/Public_Web_Site/ICH_Products/Guidelines/Efficacy/E6/E6_R1_Guideline.pdfAccessed March, 2016
- HauberABJohnsonRAndrewsEBRisk-benefit analysis methods for pharmaceutical decision-making – where are we now?ISPOR Connection2006126 Available from: https://www.rtihs.org/sites/default/files/Hauber,%20Johnson,%20et%20al._2006_Risk-Benefit_ISPOR%20Connections.pdfAccessed March, 2016
- Otero-RomeroSRamió-TorrentàLLPericotIOnset-adjusted incidence of multiple sclerosis in the Girona province (Spain): evidence of increasing risk in the south of EuropeJ Neurol Sci20153591–214615026671104
- WicksPBrandesDParkJLiakhovistskiDKoudinovaTSasaneRPreferred features of oral treatments and predictors of non-adherence: two web-based choice experiments in multiple sclerosis patientsInteract J Med Res201541e625749630
- WilsonLSLoucksAGipsonGPatient preferences for attributes of multiple sclerosis disease-modifying therapiesInt J MS Care2015172748225892977
- BansbackNTrenamanLHarrisonMHow important is mode of administration in treatments for rheumatic diseases and related conditions?Curr Rheumatol Rep201517651425903666
- VisserLHvan der ZandeAReasons patients give to use or not to use immunomodulating agents for multiple sclerosisEur J Neurol201118111343134921496180
- VineyRLanesarELouviereJDiscrete choice experiments to measure consumer preferences for health and healthcareExpert Rev Pharmacoecon Outcomes Res2002248996
- MorillasCFelicianoRCatalinaPFPatients’ and physicians’ preferences for type 2 diabetes mellitus treatments in Spain and Portugal: a discrete choice experimentPatient Prefer Adherence201591443145826508841