Abstract
Valsartan is a potent antagonist of the type 1 angiotensin receptor (AT1). By blocking the actions of angiotensin II on the AT1, it inhibits vasoconstriction and synthesis of aldosterone thus lowering systemic blood pressure. Valsartan has been approved by the FDA for the treatment of hypertension in children aged 6 years and older. Valsartan can be dosed once a day with a sustained 24-hour effect on blood pressure reduction. The starting dose recommended in children is 1.3 mg/kg once daily (maximum 40 mg) which needs adjustment according to blood pressure response (dose range 1.3–2.7 mg/kg daily; up to 160 mg). A suspension form (4 mg/mL) is available for children who cannot swallow tablets. In patients aged 6 to 16 years, valsartan treatment (from a low dose of 10–20 mg to a high dose of 80–160 mg) resulted in dose-dependent reductions of 7.9–11.5 mmHg in systolic blood pressure and 4.6–7.4 mmHg in diastolic blood pressure. In 1- to 5-year-olds, valsartan (from a low dose of 5–10 mg to a high dose of 40–80 mg) reduced the systolic blood pressure by 8.4–8.6 mmHg and the diastolic blood pressure by 5.5 mmHg. Similar to adults and other antihypertensive medications, the most frequent side effect in children subsequent to valsartan use is headache. Current studies have not shown adverse effects on linear growth, weight gain, head growth, or development in children aged 1 to 5 years subsequent to valsartan use. Based on limited pediatric data, valsartan appears to be well tolerated and efficacious in reducing elevated blood pressure.
Valsartan is an angiotensin receptor blocker (ARB)
The angiotensin II receptor blockers (ARBs) are drugs designed to inhibit the renin-angiotensin system (RAS). ARBs interact with the receptor for angiotensin II thereby selectively blocking its physiological actions. This class of drugs was developed after the angiotensin-converting enzyme (ACE) inhibitors, as an alternative to provide more specific inhibition of the RAS.Citation1 Valsartan (trade name Diovan) was the second orally active ARB to be marketed in Europe and the USA for the treatment of hypertension (HTN) ().Citation2
Table 1 Angiotensin receptor blockers
The RAS regulates blood pressure through its effect on sodium balance, extracellular fluid volume, and renal and systemic vascular resistance. The final step of the pathway is the activation of the angiotensin II receptors. The actions of angiotensin II are mediated by two types of receptors, type 1 (AT1) and type 2 (AT2). The influence on blood pressure is exerted through activation of AT1. These actions include vasoconstriction of systemic arterioles; activation of the sympathetic nervous system; stimulation of aldosterone secretion which results in sodium and water reabsorption; smooth muscle cell hypertrophy; and stimulation of vascular and myocardial fibrosis. By blocking the action of angiotensin II on the AT1 receptor, valsartan decreases peripheral resistance and causes less sodium and water reabsorption in the kidneys thereby lowering the blood pressure.Citation3 Additionally, blockage of the AT1 receptor leads to a compensatory increase in angiotensin II levels which increases stimulation of the AT2 receptor. In contrast to stimulation of AT1, the stimulation of AT2 leads to the inhibition of cell growth, tissue repair, and possibly vasodilation.Citation1
The increased stimulation of AT2 could possibly promote vasodilation,Citation4,Citation5 and thereby contribute to the blood pressure lowering effect of valsartan. There have been reports that AT2 stimulation also has an antiproliferative effect on cardiac muscleCitation6 by inhibition of cell growth, promotion of cell differentiation, and apoptosis.Citation7 This action could have a beneficial influence on cardiac remodeling in response to elevated blood pressure.
Advantages of ARBs over the more commonly used ACE inhibitors
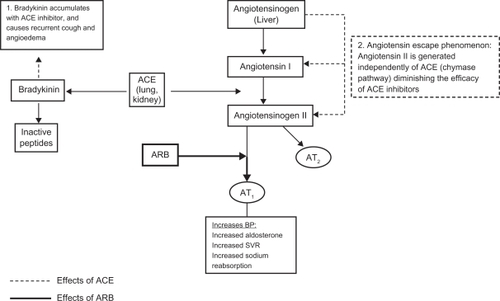
Due to the direct blockage of angiotensin II, the ARBs do not have the same limitations as ACE inhibitors. Bradykinin, which is also a substrate for ACE, accumulates with the use of ACE inhibitors. This accounts for the two most common side effects of ACE inhibitors, cough, and angioedema. When there is competitive inhibition of ACE, there can be a reactive increase in renin and angiotensin I levels which may overcome the blockade effect.Citation8 There are also alternative pathways through which angiotensin II is formed independently of ACE. In patients on chronic ACE inhibitor treatment, an “angiotensin escape phenomenon” is described, whereby the reduced stimulation of AT1 and AT2 receptors is counteracted by an increase in AT1 receptor stimulation of angiotensin II formed by an alternative pathway.Citation4 The use of ARBs circumvents this problem by acting directly on the angiotensin II receptor and therefore resulting in complete angiotensin II inhibition ().
Figure 1 Effects of ACE and ARB on the renin angiotensin system.
Hypertension in children and adolescents
HTN is the most commonly diagnosed disease in the United States.Citation9 The recent increase in obesity rates in the US and higher incidence and risk for HTN in obese individuals has increased the focus on the diagnosis and management of high blood pressure. HTN in children can be either secondary, in which an underlying cause is identified, or primary which is a diagnosis of exclusion that is reached after a systematic work-up is done looking for secondary causes. Pharmacologic treatment of HTN is indicated in the presence of secondary HTN, symptomatic HTN, when blood pressure remains elevated in spite of lifestyle modifications, and when there is evidence of end organ damage.Citation10 The goal of antihypertensive treatment should be a reduction of blood pressure to below the 95th percentile for gender, age, and height for children without comorbidities. For children with chronic kidney disease, diabetes, and target-organ damage the goal blood pressure should be less than the 90th percentile.Citation10 Since there is a lack of studies comparing long-term clinical endpoint data of multiple antihypertensive medications in children, the initial drug is chosen based on the prescribing physicians’ own preference. The Fourth report on the diagnosis, evaluation and treatment of high blood pressure in children and adolescents recommends ACE inhibitors, ARBs, beta blockers, calcium channel blockers, and diuretics as acceptable drug classes for use in children.Citation10
Role of RAS activation in pediatric hypertension
The association between obesity and HTN has been known for several decades.Citation11–Citation16 Activation of the RAS in these patients may represent an important link between obesity and HTN.Citation17 Since adipocytes can produce angiotensinogen, increased adiposity in obese patients can lead to inappropriately normal or elevated plasma renin activity (PRA).Citation18 Despite increased sodium intake, sodium/water retention, and blood pressure, increased levels of angiotensinogen, renin, aldosterone, ACE, and increased expression of the angiotensinogen gene in visceral adipose tissue are found in obese patients. The levels of angiotensinogen, renin, aldosterone, and ACE decrease after 5% in weight loss and the reduction in angiotensinogen expression and levels correlates with reduction in the systolic blood pressure.Citation19 Recently, a treatment approach for hypertension based on PRA has been proposed. Hypertensive patients with low levels of PRA have an excess of sodium and volume, and would benefit more from diuretic therapy, whereas patients with high PRA levels would respond better to RAS inhibitors.Citation20,Citation21
The effects of RAS that are important in the progression of chronic kidney disease (CKD) include intraglomerular hypertension and increased filtration of proteins, cell growth, inflammation, and fibrosis.Citation22 In view of this; ACE/ARB are considered the preferred antihypertensive medications in children with kidney disease as inhibition of the RAS can additionally decrease the rate of progression of CKD.Citation23,Citation24
Valsartan: pharmacokinetics and palatability
Adult studies have shown that the bioavailability of valsartan is 23% for the capsule and 39% for the solution.Citation25 Valsartan has a higher affinity for the AT1 receptor than losartan, but a lower affinity than candesartan, telmisartan, and olmesartan.Citation26 The half life of the drug is around 7 hours which is shorter than the half life of telmisartan and olmesartan, however it can be given once a day with a sustained 24-hour effect on blood pressure reduction.Citation26 Valsartan undergoes little hepatic metabolism and is excreted primarily as the unchanged drug via biliary elimination. Most of the drug is excreted in the feces, with the rest being renally excreted (7%–13% of the drug).Citation26
The pharmacokinetics of valsartan in a pediatric population has been studied in a group of children aged 1 to 16 years. These patients received a dose of 2 mg/kg of valsartan suspension up to a maximum dose of 80 mg. Initially age and body size were found to have similar influence in the clearance of the drug. However, as valsartan is expected to have minimal distribution in fatty tissues, adjustment was done for body size using fat free mass. This subsequent analysis accounting for body size showed that the effect of increasing age was only 2% per year on valsartan clearance, which was considered to be not significant. Therefore, this study shows that body weight dosing up to 80 mg provides comparable exposure in children as in adults.Citation3
In pediatric populations, the taste of a medication is an important factor to consider in the adherence to a treatment regimen. The taste and smell acceptability of several ARBs has been compared in young children (4 to 11 years of age) and found valsartan to have low ratings of palatability compared to candesartan and telmisartan, which were rated by the patients to have better taste.Citation27 However this study gave the medications in the form of crushed and pulverized tablets. Pediatric patients who are not able to swallow a tablet take the suspension form of the medication. A suspension form is available for preparation from the tablets for valsartan and olmesartan. The taste of valsartan suspension has not been compared to other ARBs.
Valsartan: dosing, efficacy, and safety
Valsartan was initially approved in Europe in 1996 and in the USA in 1997 for the treatment of HTN in adults. This drug has shown efficacy in reducing blood pressure in adult populations. Additionally, it has been shown to have cardioprotective effects, with reduced morbidity and mortality in adults with heart failure and following myocardial infarction.Citation26 These effects are comparable to those achieved with ACE inhibitors, with the additional benefit of a lower incidence of side effects such as cough and angioedema.Citation26
In December of 2007 the FDA approved valsartan for the treatment of HTN in children aged 6 to 16 years.Citation28 The starting dose recommended in children is 1.3 mg/kg once daily (maximum dose 40 mg) which should be adjusted according to blood pressure response. The dose range is 1.3–2.7 mg/kg once daily (up to 40–160 mg). A suspension form of the drug (4 mg/mL) can be prepared for children who cannot swallow tablets or for children for whom the dose does not correspond to the available tablet strengths. The recipe for preparation of the suspension is available in the valsartan package insert.Citation28 An oral suspending vehicle (Ora-Plus®) and an oral sweetening vehicle (Ora-Sweet SF®), both registered trademarks of Paddock Laboratories, Inc are recommended for making the oral suspension. As per the recommendations, 8 tablets of valsartan (80 mg each) are mixed with 80 mL of Ora-Plus. After shaking this mix and allowing it to stand for 1 hour, 80 mL of the Ora-Sweet SF are added. The suspension obtained has a concentration of valsartan of 4 mg/mL. This suspension can be stored for 30 days at room temperature or up to 75 days refrigerated. The exposure to valsartan with the suspension is 1.6 times greater than with the tablet, therefore when the suspension is replaced by a tablet the dose may have to be increased.Citation28
Two studies with the same design except for the ages of the study cohort were done to assess the efficacy and safety of valsartan in pediatric populations. The studies were conducted in two phases. In Phase I the patients were randomly assigned to receive low, medium, and high doses of valsartan for two weeks. Children who completed Phase I were then re-randomized to continue the same dose of valsartan or to receive placebo for two additional weeks. The study by Wells et alCitation29 which included children aged 6 to 16 years (n = 261) showed a reduction in systolic and diastolic BP in all three study groups (). Flynn et al’s studyCitation30 with a similar design including patients aged 1 to 5 years (n = 90) also showed reduction in both systolic and diastolic blood pressure (). However, it is important to note that the reduction in the systolic and diastolic BP is dose dependent in older children (6 to 16 years)Citation29 while this effect was not reported in the younger age group (1 to 5 years).Citation30 It should be noted that both studies do not comment on the statistical significance of reduction in the systolic and diastolic BP noted in study Phase I.
Table 2 Results of randomized, double-blind clinical studies on the safety and effectiveness of valsartan in children
In Phase II, in 6- to 16-year-olds, the systolic blood pressure of patients who continued to receive valsartan at medium (40–80 mg) and high doses (80–160 mg) was 4 and 7 mmHg lower than patients who received placebo.Citation29 The statistical significance of this reduction was not mentioned. In 1- to 5-year-olds the mean difference in the change of systolic (3.9 mmHg, P = 0.02) and diastolic blood pressures (3.7 mmHg, P < 0.01) between the pooled valsartan and placebo groups was significant.Citation30
Prescription patterns for ARB
The therapeutic efficacy of ARB when compared to ACE inhibitors is a critical issue and one that has important implications for ARB prescriptions. Currently there is no consensus as to whether pharmacological differences between ACE inhibitors and ARB translate into significant differences in therapeutic outcomes. Existing literature suggests that the antihypertensive effects of ARB are similar to ACE inhibitors and that they are an acceptable alternative as first choice drugs for the management of hypertension especially in patients intolerant to ACE inhibitors.Citation31 In adults, ACE inhibitors are the drug of choice in heart failure, cardiac dysfunction after MI, and diabetic nephropathy, and ARBs offer an acceptable alternative. A retrospective study evaluating the use of ARBs as antihypertensives showed that 53.4% of the patients were new to all antihypertensive therapies and more than 40% of these had no other antihypertensive. The study also reported increased use of fixed drug combinations with diuretics when losartan and valsartan were used initially to control BP in comparison to the newer ARB such as telmisartan, irbesartan, or candesartan.Citation32
In children, the FDA has approved the use of valsartan for elevated blood pressure for those who are older than 6 years of age. In addition to the reduction of blood pressure, valsartan’s antiproteinuric effects contribute towards additional benefit in children with CKD.Citation33,Citation34 Although ARBs have shown to be effective in the reduction of proteinuria and the rate of progression of renal failure,Citation35,Citation36 there is limited information regarding the renoprotective effects of ARBs in children with CKD. A study in children (n = 10) with CKD showed that adding an ARB (losartan) to ACE inhibitor treatment further reduced proteinuria.Citation37 Valsartan may have an important role in this population and more studies are needed in children with CKD to further determine the benefits of valsartan in slowing the progression of renal disease. There is a clinical trial being conducted to compare the long-term safety and effectiveness of valsartan in combination with enalapril versus enalapril alone in children with CKD. This trial will also evaluate proteinuria reduction, renopreservation and tolerability of valsartan and enalapril in combination versus enalapril monotherapy in patients with CKD.Citation38
Valsartan versus other ARBs
A meta-analysis of published randomized controlled trials involving ARB (valsartan, losartan, irbesartan, and candesartan) has shown a similar blood pressure lowering efficacy within the ARB class, a flat ARB-dose response when titrating from lower to maximum recommended doses, and potentiation of the antihypertensive effect with the addition of a diuretic (hydrochlorthiazide).Citation39 In children, studies are needed to compare the efficacy of the different ARBs. It is possible that olmesartan may offer a better alternative in view of its longer half life () and therefore better control with daily dosing.
Valsartan in combination with other antihypertensives is widely used in adults. These combinations have been shown to have better efficacy than valsartan monotherapy in the reduction of blood pressure.Citation40 The commercially available combinations include: 1) Valturna (valsartan with aliskiren, a direct renin inhibitor); 2) Exforge (valsartan and amlodipine, calcium channel blocker); 3) Diovan HCT (valsartan and hydrochlorothiazide, diuretic); and 4) Exforge HCT (valsartan with both amlodipine and hydrochlorothiazide). These combinations have not yet been approved for use in children.
Valsartan: side effects
Adverse reactions to valsartan are generally mild and transient. The discontinuation rate due to adverse effects is only 2.3%. The most common reasons for discontinuation of this drug are headache and dizziness.Citation28 Cardiovascular side effects of ARBs are similar to other antihypertensives and include hypotension, postural hypotension, and syncope. Central nervous system side effects include dizziness, fatigue, postural dizziness, headache, blurred vision, and vertigo. Gastrointestinal side effects include diarrhea, abdominal pain, and nausea; rarely do ARBs cause elevated liver enzymes. Hematologic side effects include neutropenia and decrease in hemoglobin. The incidence of cough is 2.6%, which is less than when taking ACE inhibitors.Citation28 Renal side effects include hyperkalemia and renal dysfunction with elevated creatinine. Musculoskeletal side effects include arthralgia and back pain. Rash can also be caused by ARBs and angioedema has also been reported although it is considered to be a rare side effect.
Drugs that inhibit the renin-angiotensin system can cause fetal defects if used during pregnancy. These defects include neonatal skull hypoplasia, anuria, oligohydramnios associated with craniofacial deformities and hypoplastic lungs, prematurity, renal failure, intrauterine growth retardation, patent ductus arteriosus, and death. In pediatrics, if used in female adolescents they should be counseled regarding these risks and if sexually active should take contraceptives or be prescribed alternative antihypertensives.
Although the risk of derangement of liver function tests, potassium, and creatinine is low, the prescriber may want to consider monitoring these tests when valsartan therapy is started.
A recent warning has been issued by the FDA regarding the possible association between the use of ARB and cancer. This warning is based on a recent meta-analysis that reported the frequencies of new cancer occurrence to be 7.2% for patients receiving ARBs compared to 6.0% for patients not taking ARBs. The risk ratio was 1.08 with a 95% confidence interval of 1.01–1.15.Citation41 However, this study has several limitations and the FDA has not concluded that ARBs increase the risk of cancer and is still evaluating this safety concern. In children, the duration of ARB therapy could be longer given their young age; therefore the association between ARB and cancer could possibly influence the prescription patterns for this medicine class.
Overall, in the clinical studies that looked at the safety of valsartan in children,Citation29,Citation30 this drug was well tolerated. In the 6- to 16-year-old group there was a similar adverse event profile to that seen in adults, with headache as the most frequent adverse event noted.Citation29 The 1- to 5-year-old group had a low incidence of adverse events, with the most frequent being cough, fever, upper respiratory infection, and diarrhea which are common illnesses in children in that age group. Four patients had increases in liver enzymes; however, no relationship to the study drug could be determined. The effects of treatment with valsartan on growth and development were studied in this age group. Valsartan did not appear to have adverse effects on linear growth, weight gain, head growth, or development over the 13 months of the study.Citation30
Summary
Valsartan is one of the ARBs that are FDA approved for use in hypertensive children. This drug has a high affinity for the AT1 receptor and lowers the blood pressure by inhibiting vasoconstriction and synthesis of aldosterone. In comparison to ACE inhibitors, valsartan blocks the actions of angiotensin II by inhibiting its interaction with AT1. Thus, valsartan and other ARBs have fewer side effects of recurrent cough and angioedema in comparison to ACE inhibitors. Valsartan is a good candidate for the treatment of hypertensive children as it has been shown to be effective in reducing systolic and diastolic blood pressure and is well tolerated.Citation29,Citation30 The activation of the RAS is a contributing factor in progressive CKD; therefore valsartan is a good choice for managing hypertension and/or proteinuria in children with CKD.
Disclosure
No conflicts of interest were declared in relation to this paper.
References
- BurnierMBrunnerHRAngiotensin II receptor antagonistsLancet200035563764510696996
- ChioleroABurnierMPharmacology of valsartan, an angiotensin II receptor antagonistExpert Opin Investig Drug1998719151925
- HabtemariamBSallasWSunkaraGKernSJarugulaVPillaiGPopulation pharmacokinetics of valsartan in pediatricsDrug Metab Pharmacokinet20092414515219430170
- WernerCBaumhakelMTeoKKRAS blockade with ARB and ACE inhibitors: current perspective on rationale and patient selectionClin Res Cardiol20089741843118454336
- Hernandez-HernandezRSosa-CanacheBVelascoMArmas-HernandezMJArmas-PadillaMCCammarataRAngiotensin II receptor antagonists role in arterial hypertensionJ Hum Hypertens200216S93S9911986904
- BoozGWBakerKMRole of type 1 and type 2 angiotensin receptors in angiotensin II-induced cardiomyocyte hypertrophyHypertension1996286356408843890
- StollMSteckelingsMPaulMBottariSPMetgerRUngerTThe angiotensin AT2-receptor mediates inhibition of cell proliferation in coronary endothelial cellsJ Clin Invest1995956516577860748
- BarrerasAGurk-TurnerCAngiotensin II receptor blockersBUMC Proc200316123126
- CherryDKWoodwellDANational Ambulatory Medical Care Survey: 2000 summaryAdvance Data200232813212661586
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and AdolescentsThe fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescentsPediatrics200411455557615286277
- RobinsonRFBatiskyDLHayesJRNahataMCMahanJDBody mass index in primary and secondary pediatric hypertensionPediatr Nephrol2004191379138415503182
- PludowskiPLitwinMSladowskaJBone mass and body composition in children and adolescents with primary hypertensionHypertension200851778317984369
- McGavockJMTorranceBMcGuireKAWoznyPLewanczukRZThe relationship between weight gain and blood pressure in children and adolescentsAm J Hypertens2007201038104417903685
- Urrutia-RojasXEgbuchunamCUBaeSHigh blood pressure in school children: prevalence and risk factorsBMC Pediatrics20066323817109750
- HiramatsuKYamadaTIchikawakTIzumiyamaTNagataHChanges in endocrine activity to obesity in patients with essential hypertensionJ Am Geriatr Soc19812925307005295
- TuckMISowersJDornfieldLKledzikGMaxwellMThe effect of weight reduction on blood pressure, plasma renin activity and plasma aldosterone level in obese patientsN Engl J Med19813049309337010165
- RocchiniAPChildhood obesity and blood pressure regulationPortmanRJSorofJMIngelfingerJRPediatric HypertensionTotowa, NJHumana Press2004307334
- SarzaniRSalviFDessi-FulgheriPRappeliARenin-angiotensin system, natriuretic peptides, obesity, metabolic syndrome, and hypertension: an integrated view in humansJ Hypertens20082683184318398321
- EngeliSBohnkeJGorzelniakKWeight loss and the renin-angiotensin-aldosterone systemHypertension20054535636215630041
- LaraghJLaragh’s lessons in pathophysiology and clinical pearls for treating hypertensionAm J Hypertens20011418619411243312
- EganBMBasileJNRehmanSUPlasma renin test-guided drug treatment algorithm for correcting patients with treated but uncontrolled hypertension: a randomized controlled trialAm J Hypertens20092279280119373213
- RemuzziGPericoNMaciaMRuggenentiPThe role of renin-angiotensin-aldosterone system in the progression of chronic kidney diseaseKidney Int200568S57S65
- FlynnJTMitsnefesMPierceCfor the Chronic Kidney Disease in Children Study GroupBlood pressure in children with chronic kidney disease. A report from the Chronic Kidney Disease in Children StudyHypertension2008521718497371
- WuhlETrivelliAPiccaSStrict blood pressure control and progression of renal failure in childrenN Engl J Med20093611639165019846849
- FleschGMullerPLloydPAbsolute bioavailability and pharmacokinetics of valsartan, an angiotensin II receptor antagonist, in manEur J Clin Pharmacol1997521151209174680
- BlackHRBaileyJZappeDSamuelRValsartan: more than a decade of experienceDrugs2009692393241419911855
- MeierCMSimonettiGDGhigliaSPalatability of angiotensin II antagonists among nephropathic childrenBr J Clin Pharmacol20076362863117302913
- Diovan (valsartan) tablets [prescribing information]East Hanover, New JerseyNovartis Pharmaceuticals Corporation [cited 2008 Dec]. Available from: http://www.pharma.us.novartis.com/product/pi/pdf/diovan.pdf. Accessed February 16, 2011
- WellsTBlumerJLitwinMSafety and effectiveness of valsartan in hypertensive children ages 6–16 yearsJ Clin Hypertens (Greenwich)200795 Suppl AA79A80
- FlynnJTMeyersKECPacheco NetoJfor the Pediatric Valsartan Study GroupEfficacy and safety of the angiotensin receptor blocker valsartan in children with hypertension aged 1 to 5 yearsHypertension20085222222818591457
- RodgersJEPattersonJHAngiotensin II-receptor blockers: clinical relevance and therapeutic roleAm J Health Syst Pharm20015867168311329759
- YoungCHZhangKPoretAWPatterns of antihypertensive therapy in new users of angiotensin II-receptor blockersAm J Health Syst Pharm2005622381238516278329
- WuhlESchaeferFTherapeutic strategies to slow chronic kidney disease progressionPediatr Nephrol20082370571618335252
- SchaeferFMehlsOHypertension in chronic kidney diseasePortmanRJSorofJMIngelfingerJRPediatric HypertensionTotowa, NJHumana Press2004371387
- JafarTHSchmidCHLandaMACE inhibition in progressive renal disease study groupAngiotensin-converting enzyme inhibitors and progression of nondiabetic renal disease. A metaanalysis of patient-level dataAnn Intern Med2001135738711453706
- IzuharaYNangakuMInagiRRenoprotective properties of angiotensin receptor blockers beyond blood pressure loweringJ Am Soc Nephrol2005163631364116236804
- SeemanTPohlMMisselwitzJJohnUAngiotensin receptor blocker reduces proteinuria independently of blood pressure in children already treated with angiotensin-converting enzyme inhibitorsKidney Blood Press Res20093244044420016211
- Clinical Trials Search. Worldwide Clinical Trials Listings. Hypertension. Available from: http://www.clinicaltrialssearch.org/extension-study-to-assess-long-term-safety-tolerability-and-efficacy-of-valsartan-and-enal-april-combined-and-alone-in-children-with-hypertension-nct00446511.html Accessed February 16, 2011
- ConlinPRSpenceJDWilliamsBAngiotensin II antagonists for hypertension: are there differences in efficacy?Am J Hypertens.2000134 Pt 141842610821345
- WeinbergerMHGlazerRDCrikelairNAChiangYTAchieving blood pressure goal: initial therapy with valsartan/hydrochlorothiazide combination compared with monotherapyJ Hum Hypertens20102482383020182456
- SipahiIDebanneSMRowlandDYSimonDIFangJCAngiotensin-receptor blockade and risk of cancer: meta-analysis of randomized controlled trialsLancet Oncol20101162763620542468