
Abstract
Introduction
Health-related quality of life (HRQoL) has emerged as an important consideration in the care of patients with chronic hepatitis B (CHB). However, whether benefits from the improved HRQoL that occurs after antiviral treatment or drug discontinuation outweigh the risks of viral relapse is an unanswered question. The aim of this study was to evaluate the HRQoL among patients with CHB during antiviral treatment and withdrawal of treatment.
Patients and methods
There were 102 patients who met the enrollment criteria with 54 patients in the treatment group and 48 patients in the discontinuation group. Sociodemographic information was collected. The 36-Item Short-Form Health Survey (SF-36), European Quality of Life-5 Dimensions, and Beck Depression Inventory (BDI) were adopted to evaluate life quality and mental health.
Results
In the treatment group, SF-36 showed that the physical functions were significantly increased. In the discontination group, the psychological functions showed improvement. A multivariate regression analysis indicated that baseline SF-36 score was a predictor for improvement in HRQoL (odds ratio =1.17, P=0.003) and baseline BDI score was a factor for remission of depression (odds ratio =0.75, P=0.005) after medical intervention. When the cutoff value of SF-36 score was set at 79.5, the sensitivity and specificity to predict improvement in HRQoL were 82.8% and 74.0%, respectively. When the cutoff value of BDI was found as 8.5, the sensitivity and specificity to predict alleviation of depression were 58.6%, and 76.0%, respectively.
Conclusion
Antiviral treatment benefits the physical health of the patients with CHB, while conferring no obvious improvement in their psychological condition. Improved psychological interventions for patients with CHB, especially for those with lower baseline SF-36 scores and higher BDI scores, may improve their quality of life.
Introduction
Approximately 2 billion people worldwide have been infected with hepatitis B virus (HBV), and ~5% of them have chronic infections.Citation1 Patients with chronic hepatitis B (CHB) are at increased risk of developing end-stage liver diseases such as cirrhosis, liver failure, and hepatocellular carcinoma (HCC).Citation2,Citation3 Antiviral treatment can suppress HBV replication and improve the survival rate. Nucleos(t)ide analogs (NUCs) are safe and effective antiviral drugs, and they are recommended for first-line treatment of CHB by most guidelines.Citation2,Citation4 Although NUCs are potent inhibitors of HBV replication, they do not eliminate HBV. Before starting long-term NUC treatment in patients with CHB, issues of compliance, economic burden, and quality of life (QoL) should be taken into consideration, especially in low-income populations.Citation5
Despite remarkable progress in the use of NUCs for the treatment of CHB, the effects of therapy with these drugs on the QoL and mental health (MH) of patients have received limited attention. As modern medical practice has evolved from traditional biomedical models to modern biopsychosocial medical paradigms, health-related quality of life (HRQoL) has emerged as an important consideration in the care of patients with CHB.Citation6 Chronic diseases, and especially CHB, impose a heavy psychosocial burden, including worse HRQoL, depression, and anxiety. A study reported that HBV carriers have significantly lower social function than healthy controls.Citation7 Furthermore, it has been reported that HRQoL of patients, as assessed by European Quality of Life-5 Dimensions (EQ-5D) and 36-Item Short-Form Health Survey (SF-36) questionnaires, decreases as CHB progresses to its more severe stages, from chronic inactive hepatitis to HCC.Citation6 In addition, depression and anxiety were also more common in patients with CHB than in healthy controls.
However, the majority of previous research has involved cross-sectional studies, and there is a general lack of longitudinal data. Only one prospective study has been published that shows that subjects with CHB had an improvement in HRQoL after 24 weeks of antiviral treatment.Citation8 This improvement was more obvious in females and hepatitis B e antigen (HBeAg)-positive subjects. In addition, few studies have addressed the predictors or risk factors for low HRQoL and depression in patients with CHB.
Drug withdrawal is another key problem in CHB management. There are several problems associated with long-term NUC treatment, including development of drug resistance, poor adherence, economic burdens, and psychological stressors.Citation9,Citation10 The Asian Pacific Association for the Study of the Liver (APASL) Guidelines recommend that NUC treatment for CHB could be considered successful after serum HBV DNA is undetectable, HBeAg seroconversion has occurred, and alanine aminotransferase levels have normalized for at least 12 months. Treatment is then completed after another 12 months (HBeAg-positive patients) or 18 months (HBeAg-negative patients) of medication.Citation11 However, relapse occurs in ~50% of HBV patients after withdrawal of NUCs, even when the recommendations are followed.Citation12,Citation13 European association for the study of the liver (EASL) guidelines recommend that discontinuation of NUC treatment can be considered when hepatitis B surface antigen (HBsAg) seroconversion occurs.Citation14 However, the possibility of HBsAg seroconversion during NUC therapy is limited and requires at least a decade of treatment. But long-term NUC treatment may lead to low HRQoL in patients with CHB. Whether benefits from the improved HRQoL that occurs after drug discontinuation outweigh the risks of viral relapse is an unanswered question. Thus, in summary, we speculate whether the ongoing NUC treatment increases HRQoL in patients with CHB and whether treatment interruption in patients with CHB will correlate with depressive symptoms, which is measured by Beck Depression Inventory (BDI).
Therefore, as we begin to focus on the relationship between MH and the evolution of disease outcome, how antiviral drug treatment and withdrawal influence the QoL of patients with CHB needs to be addressed. Our study examines whether, 1) ongoing NUC treatment enhances the HRQoL of patients with CHB, and 2) drug withdrawal benefits their psychological well-being.
Patients and methods
Patients
Patients treated for CHB with NUCs in the First Affiliated Hospital of Xiamen University were examined. The patients were included in our study when it was convenient and they fulfilled the inclusion criteria. We defined the diagnosis of CHB as serum HBsAg-positive for at least 6 months combined with a repeated or continued increase in the serum alanine aminotransferase level.Citation14 Patients were excluded if they had cirrhosis; HCC; metabolic liver disease; co-infections with hepatitis C virus, hepatitis D virus, or HIV; autoimmune hepatitis; were suffering from heavy alcohol abuse; were pregnant; or were previously treated with interferon. Patients with CHB were enrolled in the treatment group if they were being treated with NUCs for the first time and were enrolled in the discontinuation group if they had fulfilled the criteria by stopping medication treatment. Sociodemographic details, such as gender, age, ethnicity, education level, and income, were collected for all participating subjects. The definition was as follows: i) level of education – primary, less than 6 years of formal school education; secondary, 6–12 years of formal school education; and tertiary, university and postgraduate studies; and ii) income – low, <1,999 RMB/month; middle, 2,000–3,999 RMB/month; and high, >4,000 RMB/month.
The demographic and baseline characteristics of the two groups are shown in .
Table 1 Characteristics of patients in the treatment group and discontinuation group
Follow-up
Of the 112 patients who met the enrollment criteria, 54 patients in the treatment group and 48 patients in the discontinuation group completed the 48-week follow-up. There were 10 patients in the discontination group who discontinued follow-up prematurely. Among them, three patients dropped out due to pregnancy and seven dropped out due to their request. The treatment group attended the Department of Infectious Diseases, First Affiliated Hospital of Xiamen University. Patients with CHB were asked to fill in the SF-36, the EQ-5D, and the BDI questionnaires. For the treatment group, the SF-36, EQ-5D, and BDI questionnaires were filled in at baseline and 48 weeks after starting the antiviral treatment. For the discontinuation group, the questionnaires were filled in when they discontinued treatment and again after 48 weeks.
All the subjects completed the questionnaire surveys in a quiet room without any interference or disruptions. Professional staff members were available to answer questions if any problems occurred with understanding the survey questions.
Questionnaires
SF-36
The SF-36 is a brief self-administered HRQoL instrument commonly used in various disease populations. It includes eight items: physical functioning, role limitations due to physical problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, and MH. In addition, there are two summary measures: the physical component summary and mental component summary scales. Items with higher scores mean better health conditions. The Chinese version of the SF-36 questionnaire is available and provided by the developer. The tool’s validity and screening ability have been documented in various samples in the People’s Republic of China.Citation15,Citation16
EQ-5D
The EQ-5D self-reported questionnaire has been used as an outcome measure in many international clinical trials. The Chinese (Taiwanese) version of the EQ-5D questionnaire was authorized by the EuroQol Group in 2000. Five dimensions were included: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each item has one question, with the following possible ratings: no problem, a moderate problem, or an extreme problem. In addition, a visual analog scale (VAS) was also included for the patients to summarize their overall health status, with higher scores indicating worse health. Thus, we found that the EQ-5D is a useful instrument for surveying a large population with relatively low education levels.
BDI
The BDI is widely used for assessing depression severity with high reliability and efficacy. It is a self-reporting measure involving 21 items. Each item is rated on a scale ranging from 0 to 3, and the average provides a global depression score, with higher scores representing greater severity of depression.
We used two stable HRQoL questionnaires and a psychometric inventory in our study that complemented each other. EQ-5D was used to calculate quality-adjusted life years directly. Conversely, SF-36 provided a more comprehensive and multidimensional assessment of HRQoL. Hence, SF-36 and EQ-5D provided different information, which enabled the HRQoL evaluation of HBV patients to be more comprehensive and informative.
Statistical analysis
Continuous variables were expressed as mean and standard deviation, and categorical variables were expressed as percentages. The chi-square test and paired Student’s t-test were applied as appropriate to determine statistically significant differences. Univariate (logistic regression) and multivariate analyses (stepwise multivariate logistic regression) were used to find factors associated with QoL. In addition, we constructed receiver-operating characteristic curves for determining the factors predicting QoL. The statistical significance of all tests was set as P<0.05 by two-tailed tests. Data analyses and quality control procedures were performed using SPSS for Windows, version 13.0 (SPSS Inc., Chicago, IL, USA).
Ethical approval
The Institutional Review Board of First Affiliated Hospital of Xiamen University approved this study. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation and with the 1975 Declaration of Helsinki, as revised in 2008. Written informed consent was obtained from all patients before inclusion in the study.
Results
Demographic data
A total of 102 patients completed the SF-36 and EQ-5D questionnaires at follow-up visits; 54 subjects were in the treatment group and 48 subjects were in the drug discontinuation group. The characteristics of the subjects are shown in . All the patients were Chinese, and 80% of them were males.
Dynamic change of HRQoL in treatment group and discontinuation group
SF-36 score
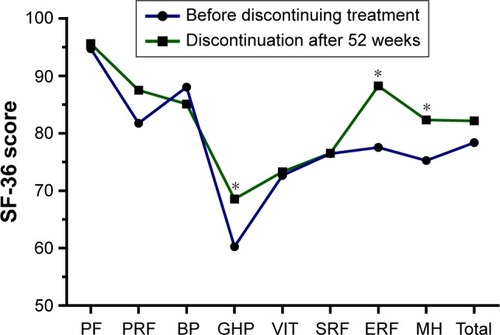
Physical aspects of QoL, including physical functioning, physical role functioning, bodily pain, and general health perceptions, were significantly increased after the treatment, but the psychological measures, including vitality, social role functioning, emotional role functioning, and MH, did not significantly increase after the antiviral drug treatment (). There were no significant differences between the patients before discontinuing treatment and the patients ending treatment after 52 weeks in most of the SF-36 scales, with the exception of general health perception, emotional role functioning, and MH, where the patients who discontinued treatment had significantly higher scores than the patients who continued NUCs during the study period ().
Figure 1 SF-36 scores for patients before and after antiviral treatment.
Abbreviations: SF-36, 36-Item Short-Form Health Survey; PF, physical functioning; PRF, physical role functioning; BP, bodily pain; GHP, general health perceptions; VIT, vitality; SRF, social role functioning; ERF, emotional role functioning; MH, mental health.

Figure 2 SF-36 scores for patients before and after discontinuation of treatment.
Abbreviations: SF-36, 36-Item Short-Form Health Survey; GHP, general health perceptions; ERF, emotional role functioning; MH, mental health; PF, physical functioning; PRF, physical role functioning; BP, bodily pain; VIT, vitality; SRF, social role functioning.
EQ-5D score
For the patients treated with NUCs, high percentages reported improved mobility, ability to do normal activities, and pain relief after treatment, while the percentage of patients with depression did not decrease. In contrast, lower percentages of patients complained of depression and pain after completion of treatment, compared to before discontinuing treatment ().
Table 2 EQ-5D scores for patients in each group
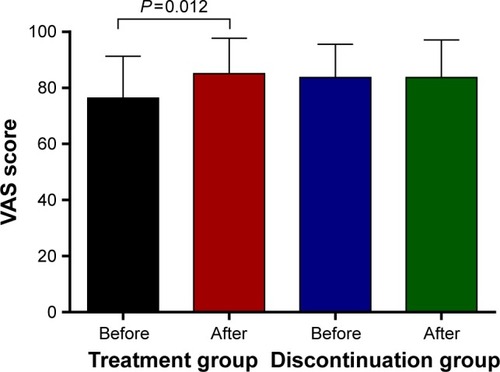
VAS score
The VAS score, indicating subjective health status, was significantly increased after the NUC treatment, compared to the baseline values (76.4±14.9 vs 85.1±12.6, P=0.012). However, there was no significant improvement or decrease after patients discontinued treatment after 52 weeks (83.7±11.9 vs 83.7±13.4, P=0.36; ).
Figure 3 The VAS score for health condition of patients.
Abbreviation: VAS, visual analog scale.
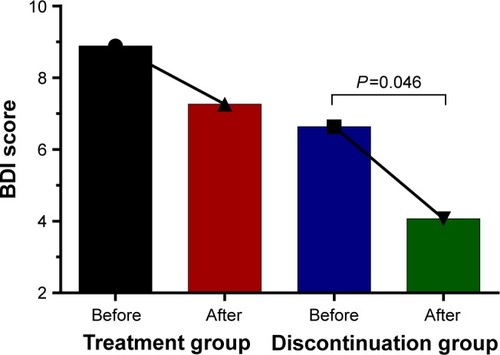
BDI
When we compared the patients before and after the NUC treatment, no significant decrease in the BDI score occurred after treatment. However, the BDI score was significantly decreased after medication treatment was discontinued (6.6±4.9 vs 4.07±4.9, P=0.046), suggesting that the severity of depression is alleviated after the completion of pharmacotherapy ().
Figure 4 The BDI score for patients.
Abbreviation: BDI, Beck Depression Inventory.
Factors associated with HRQoL after intervention
To explore the relationships between baseline characteristics and the SF-36 scores after intervention, univariate analyses were performed and the results showed that the type of intervention (P=0.007) and the baseline SF-36 score (P<0.001) were the predictors for QoL. Multivariate logistic regression analysis of the SF-36 score included baseline characteristics and type of treatment (). Baseline SF-36 scores were strong predictors for improvement in HRQoL after intervention. Patients with CHB tended to achieve higher QoL after intervention if they had higher baseline SF-36 scores (odds ratio =1.17, 95% confidence interval [CI]: 1.06–1.29, P=0.003).
Table 3 Factors associated with HRQoL after intervention
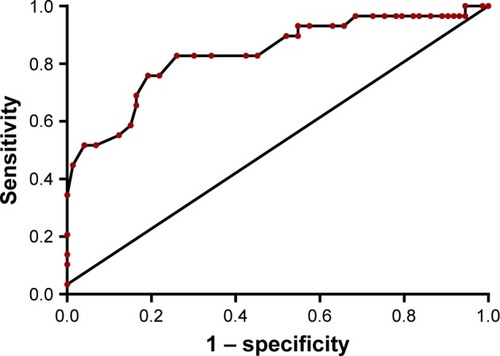
To validate the results, the receiver-operating characteristic curve was calculated. The area under the receiver-operating characteristic curve using the baseline SF-36 score to predict improvement in HRQoL was 0.84 (95% CI: 0.74–0.93, P<0.001; ). When the cutoff value for SF-36 was set at 79.5, the sensitivity and specificity for predicting QoL improvement were 82.8% and 74.0%, respectively.
Figure 5 ROC curves of baseline SF-36 score in predicting the life quality.
Abbreviations: ROC, receiver-operating characteristic; SF-36, 36-Item Short-Form Health Survey; CI, confidence interval; QoL, quality of life.
Factors predicting the alleviation of depression
We also explored the relationships between baseline characteristics and depression. The univariate analysis showed that the baseline VAS score (P=0.03) and the baseline BDI score (P=0.001) predicted alleviation of depression. Multivariate logistic regression analysis showed that the baseline BDI score predicted risk of the patients suffering from depression (odds ratio =0.75, 95% CI: 0.62–0.92, P=0.005), suggesting that patients were less likely to get remission of depression when they have a lower baseline BDI score (). The receiver-operating characteristic for baseline BDI predicts depression alleviation after the intervention (0.78, 95% CI: 0.66–0.89, P<0.001). The optimal cutoff value was 8.5, and the sensitivity and specificity values for predicting depression remission were 58.6% and 76.0%, respectively. Patients with BDI score <8.5 at baseline had a higher chance of depression remission after the intervention ().
Figure 6 ROC curves of baseline BDI score in predicting the depression condition.
Abbreviations: ROC, receiver-operating characteristic; BDI, Beck Depression Inventory; CI, confidence interval.
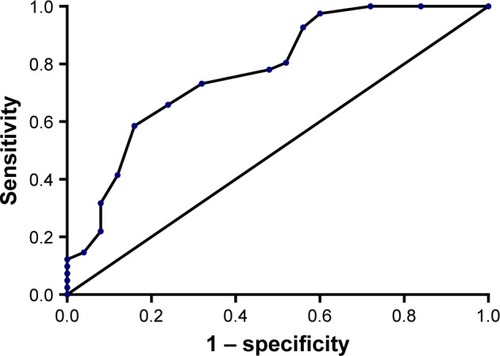
Table 4 Factors associated with depression after intervention
Discussion
Patients with CHB suffered from impaired physical health often accompanied by depressive symptoms.Citation17 HRQoL of patients with CHB was obviously inferior to that of the general population.Citation18,Citation19 NUCs have been widely used to treat CHB and prevent the development of end-stage liver disease, but their effects on HRQoL have not been fully documented. This study is the first to observe the change in SF-36, ED-5Q, and BDI after the initiation and termination of antiviral treatment in patients with CHB. We demonstrated that NUC pharmacotherapy benefits physical health but not psychological status, especially in those with high SF-36 scores and/or low BDI scores at baseline. Patients with previous history of MH, heavy alcohol consumption, and drug abuse need more attention paid to their psychological status during NUC antiviral treatment since studies have reported that patients with mental disorder history, alcohol, and/or drug abuse have poor HRQoL and MH.Citation20,Citation21
Few studies have addressed the effects of NUC treatment on the HRQoL and MH in patients with CHB. It was suggested that stopping the antiviral drugs too early can lead to relapse.Citation22 However, long-term treatment will also result in problems, including adverse drug effects, economic burdens, drug resistance, and psychological stressors. It is vital to balance the risks and benefits from continuing or terminating NUC pharmacotherapy. By analyzing outcomes in the patients who stopped antiviral medications according to guidelines from the APASL, our research showed that mental status improved significantly after cessation of NUC treatment, as shown by the EQ-5D anxiety score, the mental component of SF-36, and the BDI score. However, the multivariate logistic regression analysis indicated that the baseline SF-36 score is the only independent factor to predict which patients would obtain a better QoL irrespective of whether patients receive continued treatment or not. Our study demonstrated that patients with CHB have better QoL after interventions (continued treatment or not) if they had higher SF-36 scores at baseline. Given the risks of HBV relapse after termination of NUC treatment, continued antiviral therapy may be the more beneficial strategy for clinicians to advocate.
The present study also showed that mobility, pain, and the usual activities domain of the EQ-5D improved after 104 weeks of antiviral treatment. However, the anxiety domain of EQ-5D was not increased, favoring the idea that patients with CHB may benefit from psychotherapy during antiviral treatment, which is often overlooked by the treating clinicians. This could be affected by the stage of disease progression, which was not determined in this survey, as well as the cultural and social context of the study populations.
Undoubtedly, several factors associated with HRQoL and depression in patients with CHB are not well understood. In addition to HBV effects on liver, patients with CHB may exhibit depression and reduction in their HRQoL. HBV infection could influence the central nervous system and cause cognitive dysfunction in many ways.Citation23,Citation24 However, the mechanism between behavioral disorders that negatively affect HRQoL and HBV chronic infection is still unknown. Previous studies have shown that disease severity, gender, HBeAg positivity, alcohol consumption, age, and lack of awareness of CHB may be related to the HRQoL of patients during treatment.Citation6,Citation25,Citation26 Kunkel et alCitation27 reported an association between BDI scores, higher psychosocial stress, poorer general functioning, and higher liver enzyme levels. In multiple regression analyses, older age and lack of awareness were predictors of stigma scores with CHB. One pitfall in most studies was the failure to consider baseline HRQoL and depression severity. This study was the first to include the baseline SF-36 score and BDI score in the multiple regression analysis, and we found that the baseline SF-36 score and BDI score were important predictors of HRQoL and MH. Therefore, the baseline assessment of HRQoL and MH should be included in the routine evaluation of these patients.
Our study has clinical relevance as mental health problems were reported to be common among patients with chronic liver diseases and they can have significant health implications.Citation18,Citation28,Citation29 Addressing depression and psychological problems with adequate interventions should improve the adjustment in patients with CHB. In addition, assessing MH at the initial encounter with the patient is useful, because individuals with low SF-36 scores and high BDI scores at baseline have a higher risk of having poor HRQoL and depression after treatment. Professional help, including educational or psychological interventions, should be given to these patients, as it has been shown that HRQoL of these patients significantly improves after a brief educational program.Citation30
Limitations
There are some limitations of our study. First, we have not considered the severity of the liver disease, although different disease stages can affect HRQoL to different degrees. Second, in view of the small sample size of this study, caution should be exercised before generalizing the conclusions to all patients with CHB.
Conclusion
Antiviral treatment with NUC benefits the physical health of the patients with CHB, while conferring no obvious improvement in their psychological condition. Improved psychological interventions for patients with CHB, especially for those with lower baseline SF-36 scores and higher BDI scores, may improve their QoL. Although discontinuing antiviral medications may improve their psychological status, the multivariate logistic regression analysis indicated that baseline SF-36 scores and BDI scores were the only independent factors that could predict whether the patients would obtain a better QoL and remission of depression, whether or not they received continued treatment. Considering the risk of HBV relapse after drug withdrawal, a continued antiviral treatment, with attendant psychological intervention, may be the more suitable clinical strategy.
Acknowledgments
We wish to thank Zhiyun Feng for his helpful assistance in the study.
Disclosure
The authors report no conflicts of interest in this work
References
- LiawYFChuCMHepatitis B virus infectionLancet2009373966358259219217993
- SarinSKKumarMLauGKAsian-Pacific clinical practice guidelines on the management of hepatitis B: a 2015 updateHepatol Int2016101198
- CaiSYuTJiangYZhangYLvFPengJComparison of entecavir monotherapy and de novo lamivudine and adefovir combination therapy in HBeAg-positive chronic hepatitis B with high viral load: 48-week resultClin Exp Med201616342943626164128
- TerraultNABzowejNHChangKMHwangJPJonasMMMuradMHAASLD guidelines for treatment of chronic hepatitis BHepatology201663126128326566064
- PengJYinJCaiSYuTZhongCFactors associated with adherence to nucleos(t)ide analogs in chronic hepatitis B patients: results from a 1-year follow-up studyPatient Prefer Adherence20159414525609925
- OngSCMakBAungMOLiSCLimSGHealth-related quality of life in chronic hepatitis B patientsHepatology20084741108111718318043
- AltindagACadirciDSirmatelFDepression and health related quality of life in non-cirrhotic chronic hepatitis B patients and hepatitis B carriersNeurosciences (Riyadh)2009141565921048575
- KwonSYLeeYSLeeJHKooHWChoiWLeeCHImpact of Antiviral Treatment on Health-Related Quality of Life in Chronic Hepatitis B Patients: A Prospective Longitudinal Study 2008Hoboken, NJJohn Wiley & Sons Inc2008
- PengJCaoJYuTPredictors of sustained virologic response after discontinuation of nucleos(t)ide analog treatment for chronic hepatitis BSaudi J Gastroenterol201521424525326228369
- CaiSHLvFFZhangYHJiangYGPengJDynamic comparison between Daan real-time PCR and Cobas TaqMan for quantification of HBV DNA levels in patients with CHBBMC Infect Dis2014148524528480
- LiawYFKaoJHPiratvisuthTAsian-Pacific consensus statement on the management of chronic hepatitis B: a 2012 updateHepatol Int20126353156126201469
- AhnSHChanHLChenPJChronic hepatitis B: whom to treat and for how long? Propositions, challenges, and future directionsHepatol Int20104138639520305758
- FungJLaiCLTanakaYThe duration of lamivudine therapy for chronic hepatitis B: cessation vs. continuation of treatment after HBeAg seroconversionAm J Gastroenterol200910481940194619455108
- European Association for the Study of LiverEASL clinical practical guidelines: management of alcoholic liver diseaseJ Hepatol201257239942022633836
- ChungJKwanAKwokJChanSHealth-related quality-of-life questionnaire for women with polycystic ovary syndrome: a Chinese translation and validation studyBJOG2016123101638164527412270
- ZhangLTuLChenJPsychological distress as a crucial determinant for quality of life in patients with noncardiac chest pain in Central China: a cross-sectional studyMedicine (Baltimore)20169546e528927861354
- ModabberniaAAshrafiMMalekzadehRPoustchiHA review of psychosocial issues in patients with chronic hepatitis BArch Iran Med201316211412223360635
- KaraivazoglouKIconomouGTriantosCFatigue and depressive symptoms associated with chronic viral hepatitis patients. health-related quality of life (HRQOL)Ann Hepatol20109441942721057161
- BaoZJQiuDKMaXAssessment of health-related quality of life in Chinese patients with minimal hepatic encephalopathyWorld J Gastroenterol200713213003300817589955
- NdikunoCNamutebiMKuteesaJMukunyaDOlwitCQuality of life of caregivers of patients diagnosed with severe mental illness at the national referral hospitals in UgandaBMC Psychiatry201616140027846822
- LozanoOMRojasAJFernandezCFPsychiatric comorbidity and severity of dependence on substance users: how it impacts on their health-related quality of life?J Ment Health Epub2016429
- WuXCaiSLiZPotential effects of telbivudine and entecavir on renal function: a systematic review and meta-analysisVirol J20161316427062520
- LvXFQiuYWTianJZAbnormal regional homogeneity of resting-state brain activity in patients with HBV-related cirrhosis without overt hepatic encephalopathyLiver Int201333337538323402608
- LvXFYeMHanLJAbnormal baseline brain activity in patients with HBV-related cirrhosis without overt hepatic encephalopathy revealed by resting-state functional MRIMetab Brain Dis201328348549223836055
- SpackmanDEVeenstraDLA cost-effectiveness analysis of currently approved treatments for HBeAg-positive chronic hepatitis BPharmacoeconomics2008261193794918850763
- WeinsteinAAKallmanPJStepanovaMDepression in patients with nonalcoholic fatty liver disease and chronic viral hepatitis B and CPsychosomatics201152212713221397104
- KunkelEJKimJSHannHWDepression in Korean immigrants with hepatitis B and related liver diseasesPsychosomatics200041647248011110110
- FosterGRGoldinRDThomasHCChronic hepatitis C virus infection causes a significant reduction in quality of life in the absence of cirrhosisHepatology19982712092129425939
- ModabberniaAAshrafiMKeyvaniHBrain-derived neurotrophic factor predicts physical health in untreated patients with hepatitis CBiol Psychiatry2011705e31e3221429476
- SharifFMohebbiSTabatabaeeHRSaberi-FirooziMGholamzadehSEffects of psycho-educational intervention on health-related quality of life (QOL) of patients with chronic liver disease referring to Shiraz University of Medical SciencesHealth Qual Life Outcomes200538116356186