
Abstract
Background
Nowadays, mobile technologies are part of everyday life, but the lack of instruments to assess their acceptability for the management of chronic diseases makes their actual adoption for this purpose slow.
Objective
The objective of this study was to develop a survey instrument for assessing patients’ attitude toward and intention to use mobile technology for diabetes mellitus (DM) self-management, as well as to identify sociodemographic characteristics and quality of life factors that affect them.
Methods
We first conducted the documentation and instrument design phases, which were subsequently followed by the pilot study and instrument validation. Afterward, the instrument was administered 103 patients (median age: 37 years; range: 18–65 years) diagnosed with type 1 or type 2 DM, who accepted to participate in the study. The reliability and construct validity were assessed by computing Cronbach’s alpha and using factor analysis, respectively.
Results
The instrument included statements about the actual use of electronic devices for DM management, interaction between patient and physician, attitude toward using mobile technology, and quality of life evaluation. Cronbach’s alpha was 0.9 for attitude toward using mobile technology and 0.97 for attitude toward using mobile device applications for DM self-management. Younger patients (Spearman’s ρ=−0.429; P<0.001) with better glycemic control (Spearman’s ρ=−0.322; P<0.001) and higher education level (Kendall’s τ=0.51; P<0.001) had significantly more favorable attitude toward using mobile assistive applications for DM control. Moreover, patients with a higher quality of life presented a significantly more positive attitude toward using modern technology (Spearman’s ρ=0.466; P<0.001).
Conclusion
The instrument showed good reliability and internal consistency, making it suitable for measuring the acceptability of mobile technology for DM self-management. Additionally, we found that even if most of the patients showed positive attitude toward mobile applications, only a moderate level of intention to indeed use them was observed. Moreover, the study indicated that barriers were truthfulness and easiness to use.
Introduction
Mobile technology has become increasingly affordable and important in society, with new emerging concepts, such as mHealth. Although, mobile applications belong to our everyday life, embracing these gadgets in managing chronic conditions, such as diabetes and heart disease, is still slow.Citation1
Diabetes mellitus (DM) is one of the most common widespread chronic diseases. Like other chronic diseases, DM has a major impact on both patient’s health status and quality of life. The patient’s quality of life may be decreased both in a direct and in an indirect manner: diagnosis of the disease has an immediate impact on patient’s lifestyle; for DM management, the diagnosed patient has to improve his/her diet-related habits and has to adopt a special schedule for taking the specific medication. On the other hand, the possible associated acute and chronic DM complications lead in a direct manner to an impairment in the patient’s perception toward the quality of life. Acceptance of mobile technology among patients with DM may lead to a better self-management and a better support from health care providers.Citation2 Disease management among patients with DM is not just a matter of choice but also a social problem. Moreover, successful self-management demands knowledge and understanding of disease effects on the body, the goals of the treatment, and the consequences of various actions on glucose regulation.Citation3,Citation4 Hence, responsible behaviors, such as the capacity to learn, reason, and solve problems, result in better health behavior and overall self-management.Citation5,Citation6 Consequently, the continuous process of DM self-management is influenced not only by the socioeconomic factors but also by the cognitive skills.Citation7
Many mHealth solutions for DM assistive control were proposed, ranging from technical interventions,Citation8 web-based applications,Citation9 clinical decision support systems,Citation10 online self-management programs,Citation11 and specific-task mobile applicationsCitation12–Citation15 to applications promoting behavior change techniques, but the actual use has been demonstrated to be still limited.Citation16–Citation19 However, the acceptance and use of mobile technology for disease management requires positive attitude and openness.Citation20,Citation21
Various survey-based instruments were developed and validated for DM care research, ranging from evaluation of patient satisfaction about disease managementCitation22 to instruments measuring self-care,Citation23 disease knowledgeCitation24 or DM self-management barriers.Citation25
The aim of this study was twofold, namely, 1) to develop an instrument that evaluates the attitude and behavior toward mobile technology for DM self-management and 2) to investigate if sociodemographic characteristics and health-related quality of life factors are drivers or barriers in accepting innovative technologies for DM management. Additionally, the study focused on real-time notifications and risk assessment that are expected from mobile applications and how the interaction between a physician and patient might change.
Methods
Study design and participants
In using mobile technology for better disease management, successful solutions for changing behavior proved to be those involving not only smart software engineering but also psychology theories and techniques.Citation26 Therefore, we decided to design an assessment questionnaire from scratch, using the theory of planned behavior (TPB), designed to explain and predict human behavior in specific contexts.Citation27
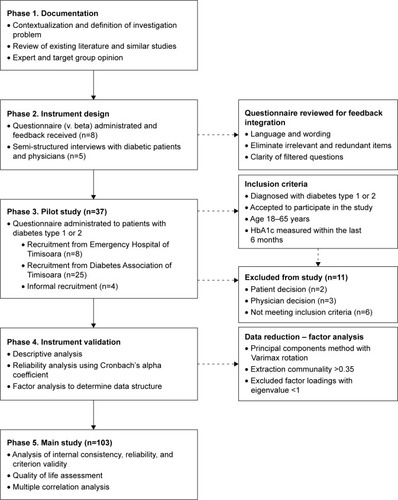
We followed sequential developing stages, namely, literature review and qualitative research and semi-structured interviews with physicians and diabetic patients. Afterward, we conducted a pilot study, which was subsequently followed by the development of the final version of the instrument. An overview of the study flow is illustrated in .
Figure 1 Summary of the study design.
Participants were aged between 18 and 65 years and had hemoglobin A1c (HbA1c) measured within the last 6 months. We excluded from the study patients who were not meeting the inclusion criteria or refused to participate in the study. The participants were recruited from the Emergency Hospital of Timisoara and the Diabetics Association of Timisoara, Romania. The enrollment held from April to December 2014, while the pilot study was conducted and validated in 2015. At the Emergency Hospital of Timisoara, the instrument was applied by a diabetic resident physician, while at the Diabetics Association of Timisoara, it was self-administered by diabetic patients. The study protocol and informed consent were reviewed and approved by the ethics committee of the Emergency Hospital of Timisoara. Each patient signed an informed consent.
Pilot study
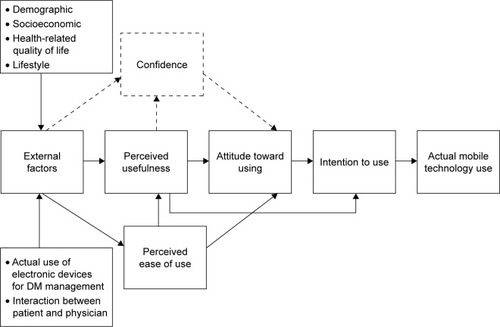
The pilot version of the instrument included statements about the actual use of electronic devices, the attitude toward mobile technology, the disease management decisions, the confidentiality issues, and the evaluation of health-related quality of life and lifestyle. The instrument design followed the TPB,Citation27 in conjunction with technology acceptance-related models.Citation28,Citation29 We considered that perceived usefulness influences both confidence and attitude toward using mobile technology. In addition, external factors were demographic and socioeconomic characteristics, quality of life level, as well as the actual use of electronic devices for DM self-management and the interaction between the patient and physician. A schematic representation of the used model is presented in .
Figure 2 Mobile technology acceptance model for DM self-management.
The rewording suggestions were integrated into the instrument’s statements. The aim of the pilot data analysis was to develop and validate an investigation and a data collection instrument, an instrument that can be used and applied on a larger number of respondents in the next study phase.
Internal consistency
Internal consistency evaluates the strength of statements within their measured domains. Cronbach’s alpha was used to evaluate the internal reliability of all the sections of the pilot and final survey instrument. An acceptable coefficient is ≥0.7.Citation30
Criterion and face validity
The criterion validity ensures that a measurement instrument evaluates what it is meant to assess.Citation31 It was achieved by administrating the questionnaire to two independent groups of participants who were expected to have different attitude toward and intention to use mobile technology.
Face validity ensures the appropriateness and ease to complete the questions.Citation32 It was guaranteed by professionals’ and patients’ review during the pilot study.
Content validity
Content validity was assessed by analyzing if the semantic is compatible with the study population and if the presentation of attributes is adequate. In addition, semi-structured interviews with diabetic patients and physicians were conducted, and the received feedback was integrated into a revised version of the instrument during the pilot study.
Construct validity
Construct validation was assured by performing exploratory factor analysis with principal component analysis and orthogonal rotation via the Varimax method. The principal component analysis was used to extract the factors with eigenvalues >1.0 and factor loading >5.0. Initial sampling adequacy was evaluated by using the Kaiser–Meyer–Olkin (KMO) test and the Bartlett’s test of sphericity.
Main study
The final version of the instrument included five main sections, which measured 1) actual use of electronic devices for DM self-management; 2) interaction between patient and physician, and attitude toward mobile technology and mobile device applications for DM self-management, which was indirectly measured by 3) perceived ease of use; 4) perceived usefulness; and 5) confidence. The actual use of electronic monitoring was assessed by five statements designed on 5-point Likert scale, 1 indicating complete disagreement and 5 indicating complete agreement. The perceived ease of use and confidence about mobile technology were assessed by four statements each, also designed on 5-point Likert scale, 1 indicating complete disagreement and 5 indicating complete agreement. The perceived usefulness of mobile device applications for DM management was assessed by statements designed on 10-point Stapel scale, 1 corresponding to not at all useful and 10 corresponding to very useful.
Health-related quality of life and lifestyle
Health-related quality of life was evaluated by three main aspects, considering 1) the degree of satisfaction about usual activities of a diabetic patient, such as the time spent to measure the glycemic level and the time spent to make physical activities; 2) how often DM negatively influences patients’ life; and 3) how often (in the last 3 months) the DM-related events caused problems when doing usual physical activities.
For assessing the first aspect, we included seven statements on 5-point Likert scale, 1 corresponding to very unsatisfied and 5 corresponding to very satisfied, while the other two aspects were each one evaluated by six statements designed on 5-point Likert scale, 1 indicating very often and 5 indicating very rare. For each patient, we quantified a total score, which was considered a measure of the patients’ health-related quality of life.
Lifestyle was assessed by open-answer and multiple-choice questions about the frequent physical activities, the usual method of transport, or the number of days with at least 30 minutes of physical activity of moderate or high intensity, such as actively walking, riding bicycle, swimming, and jogging.
Statistical analysis
For categorical variables, description was done by their absolute frequencies or percent and for continuous variables with non-Gaussian distribution by median and interquartile range (IQR). The applied statistical tests were Mann–Whitney U test for investigation of differences between central tendency in case of rang variables and Kruskal–Wallis test for comparing median ranks for more than two groups. To assess the existence of correlation between patient’s age, quality of life, optimal glycemic control, and attitude toward and intention to use modern technologies and mobile device applications for assistance in DM self-management, we computed the Spearman’s ρ correlation coefficient, while Kendall’s τ was derived to investigate the existence of correlation between education level, working status, income, and attitude toward and intention to use mobile technologies.
The degree of positive attitude toward and intention to use mobile technology and mobile device applications was calculated as the weighted mean of the corresponding points and the number of respondents, for statements designed on 5-point Likert and 10-point Stapel scales. The obtained coefficient ranged between 0 as the lower limit, corresponding to a total negative attitude and intention, and 1 as the upper limit, corresponding to a total positive attitude and intention. For multiple-choice questions, attitude was expressed as proportions of patients who had chosen the respective options.
A limit of 0.05 was considered the statistical significance threshold. Statistical processing was performed with SPSS v17 (SPSS Inc., Chicago, IL, USA).
Results
Participants
Demographic, socioeconomic, and anthropometric characteristics of the participants are presented in . The median age of the participants was 37 years (IQR: 26–59 years), and female participants were in proportion of 50.5%. Most of the participants were patients diagnosed with type 1 DM (61.2%), while only a low proportion of patients had an optimal DM management (HbA1c <7.5%) in the last 6 months (35.9%). More than a half of the patients (52.4%) were diagnosed with DM for >10 years. Most of the patients (64.0%) had high school or bachelor as their highest education level, while 9.8% did not have an education. The highest proportion of patients (52.2%) were unemployed or independent, while a proportion of 35.0% were retired and only 28.2% were full-time workers. A total of 38.9% and 30.1% of patients had middle- and low-income levels, respectively, while only 7.8% had a high-income level and 23.3% did not know or did not want to answer.
Table 1 Patients’ anthropometric, demographic, and socioeconomic characteristics
Participants indicated that they used classical auxiliary instruments for various activities related to DM management, namely, noting glycemic values (63.1%), eaten food types (24.3%), physical activities (14.6%), and tracking administered medication (32.0%). Most of the patients used glucometer (90.3%) and blood pressure monitor (33.0%). For disease management, most of the patients, 80.6% and 66.0%, declared that the decisions were taken by the physician and themselves, respectively, while only a small proportion (15.5%) said that their family participates in taking decisions about their disease.
A large proportion of patients had Internet access (75.7%). Almost half of them used a PC (46.6%) and fewer used a mobile phone (44.7%), a laptop (39.8%), or a tablet (11.7%). More than a half of the patients used Internet several times a day (57.3%), while only 6.8% had Internet access only once in a day. Most of the patients indicated that they usually use Internet for social networks (58.3%), e-mails (48.5%), news or weather forecast (40.8%), documentation (35.0%), forums dedicated to patients (31.1%), games and entertainment (29.1%), and online shopping (21.4%).
We found that most of the patients (94.1%) owned a mobile phone and only a half (51.0%) had a smartphone, while 10.4% of the patients did not know the type of their mobile phone.
Pilot study
The first version of the survey instrument was analyzed question by question. We chose to present the analysis for one statement, but we went through all statistical procedures for the entire instrument. For example, the actual use of electronic devices for DM self-management was evaluated by five items. Each item was separately rated on a 5-point Likert scale, where 1 represented a strongly disagree and 5 denoted a strongly agree. We calculated Cronbach’s alpha coefficient on all five items, obtaining a value below the recommended limit of 0.7 for internal consistency, which suggested an internal design issue for the statement. For improving the score, a solution was to eliminate the items. In addition, factor analysis with principal component method was applied. Two factors were extracted with eigenvalues >1, explaining 57.3% of total items variance. For a better interpretation of factor loadings, the initial extraction solution was rotated using the Varimax method and only those with communalities >0.35 were accepted.
The results obtained through rotated solution confirm the reliability analysis made on the statement. Items were factored in a separate component, confirming that they belonged to a different dimension than the one investigated. Rerunning the principal component analysis with only four items included led to an improved KMO and a new Cronbach’s alpha coefficient of 0.85.
Construct validity
Considering the results of the pilot study, we designed the final version of the survey instrument. The KMO measure of the sampling adequacy was 0.877, while the Bartlett’s test of sphericity showed a significant relationship among instrument’s statements (χ2(496) =3,746.8; P<0.001). presents the loadings of the statements belonging to the five extracted components, after Varimax rotation with Kaiser normalization. Coefficients with an absolute value <0.5 were not considered. Components depicting the perceived usefulness loaded on the first factor explained 45.5% of the variance on the sample, while components about the actual use of electronic devices for DM management loaded on a second factor explained 13.8% of the variance. In addition, components about the perceived ease of use loaded on a third factor explained 10.1% of the variance, while the components about confidence and patient–physician interaction loaded on factors four and five explained 4.6% and 4.4% of the variance, respectively.
Table 2 Results of factor analysis – rotated component matrix
Internal consistency
Computing Cronbach’s alpha, we found a very good internal consistency for the attitude toward mobile technology for DM self-management and the compound parts, namely, perceived ease of use of mobile technology for DM self-management, confidence about technology and latest generation products, and perceived usefulness of notifications about the risk of DM-related complications. Alpha values were >0.7 for all the components measuring the attitude toward mobile technology for DM self-management ().
Table 3 Attitude toward mobile technology for DM self-management
Cronbach’s alpha indicated a good internal reliability for both the attitude toward mobile device applications for DM self-management and the compound parts, namely, tracking functions of glycemic values, ingested carbohydrates, administered medication, security and confidentiality of personal data, backup system, data portability, multiple user profiles, off-line notifications, and notifications about medication administration, eating behaviors, and physical effort optimization. Alpha values were >0.7 for all the components measuring the attitude toward mobile applications for DM self-management ().
Table 4 Perceived usefulness about the inclusion of various attributes into a mobile device application for DM self-management
Criterion validity
Total scores for the section measuring the attitude toward using mobile technology for DM control of the group using Internet and the group not using Internet were compared. Scores differed statistically significantly between groups for the respective section (Mann–Whitney U test, U=486; P<0.001). At the same time, total scores for the section measuring the attitude toward various attributes of a mobile device application for DM self-management of the group using smartphone and the group not using smartphone were compared. Similarly, scores differed statistically significant between groups for the respective section (Mann–Whitney U test, U=360; P<0.001).
Health-related quality of life and lifestyle
We found a moderate level of patients’ satisfaction about their current treatment of DM (0.676) and the time spent for DM-related activities (0.61). Additionally, we observed moderate frequencies, when looking how often DM negatively influences the social life of the patients and their overall well-being. In addition, almost a half of patients (49.15%) declared that they were not satisfied about their weight.
Attitude toward and intention to use mobile technology
A rather moderate rate (0.682) of positive attitude toward using innovative technologies for DM control and a moderate level (0.63) of confidence that these technologies could indeed be helpful for DM self-management were measured. In addition, we found that 28.2% of the patients liked to be among the first ones who use cutting-edge products. Similar proportions, 30.1% and 27.2%, used mobile technology to stay in touch with other people or to stay in contact with the family, while 10.7% of patients could live without a mobile phone.
On the contrary, a high rate (0.832) of perceived usefulness of modern technologies and a high rate of intention (0.811) to use these technologies for receiving advice and notifications about the risk to develop certain complications associated with DM were observed.
Attitude toward and intention to use mobile device applications
We observed a high rate of positive attitude (0.852) toward mobile device applications for DM control. In addition, high rates of positive attitude were observed when considering the inclusion of different attributes, such as security and confidentiality of personal data (0.831); backup system for information already included (0.751); send, export, and print data (0.75); multiple user profiles (0.788); notifications about Internet connection (0.763); availability on many operating systems (0.767); and availability on many languages (0.836). Similarly, we observed a high rate of positive attitude toward and intention to use mobile application if it would be free.
Considering application’s functions of tracking glycemic values, ingested carbohydrates, daily physical activity, and administered medication, we found a high level of perceived usefulness (0.814) about their inclusion into a mobile application. Similarly, we observed high levels of confidence about the inclusion of notifications for medication administration (0.815), eating behaviors (0.811), physical activities optimization (0.788), and alerts of potential DM-related risks (0.849). When asking about what information would be more useful to include into an assistive mobile application, most of the patients said glycemic values (71.8%) and medication administration with daily doses (43.7%) and less answered information about ingested carbohydrates (32.0%), weight (33.0%), laboratory results (34.0%), and daily physical activity (27.2%). A statement about the intention to use mobile applications was formulated negatively instead of positively to force patients to evaluate every statement on its own. We found that almost a half of the patients would not use applications if the information already inserted would be lost (48.5%), the price would be high (40.8%), in case of not receiving notifications (36.9%), and in case it would be in a foreign language (35.9%). Moderate proportions of patients answered that reasons for not using mobile applications would be having to learn by themselves how to use the application (21.4%), having to insert too much information in the application (22.3%) and lack of experience using mobile technologies (17.5%).
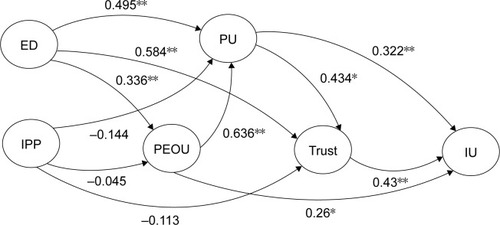
We observed a very low confidence about using mobile device applications for taking decisions about the disease (4.9%), when comparing to physician advice, but a higher proportion of patients (21.4%) would use both applications and their physician, when comparing to physicians alone, themselves, or their family. In addition, 43.5% considered that using applications would change the interaction with their physician. A high percent of patients (63.1%) would agree to give their DM-related data for developing an application. Finally, we observed only a moderate level of intention (0.671) to actually use mobile applications for assistance in DM control. To further underline the results, we tested the structural acceptance model, as described in . The actual use of electronic devices for DM self-management was found to have a significant influence on perceived usefulness. Additionally, we observed that the perceived ease of use and perceived usefulness had a strong impact on trust and intention to use (). This highlights the importance of usability and usefulness for mobile technology and mobile device applications.
Figure 3 The correlated factors of the mobile technology acceptance model for DM self-management.
Abbreviations: DM, diabetes mellitus; IPP, interaction patient-physician; ED, electronic devices; PEOU, perceived ease of use; PU, perceived usefulness; IU, intention to use.
A multiple correlation analysis evaluated the association between both sociodemographic characteristics and quality of life factors and attitude toward using mobile technology and mobile device applications for DM self-management. We found that younger patients had a significantly more positive attitude toward using mobile technology (Spearman’s ρ=−0.393; P<0.001) and mobile device applications (Spearman’s ρ=−0.429; P<0.001). In addition, patients with a higher quality of life presented a significantly more favorable attitude toward mobile technology (Spearman’s ρ=0.37; P<0.001) and mobile device applications (Spearman’s ρ=0.466; P<0.001). Moreover, patients with optimal glycemic control had more positive attitude toward both mobile technology for DM self-management (Spearman’s ρ=−0.322; P<0.001) and mobile applications (Spearman’s ρ=−0.317; P<0.001). A higher education level significantly correlated with more favorable attitude toward mobile applications (Kendall’s τ=0.33; P<0.001). Similarly, participants who had higher income presented a significantly more favorable attitude toward mobile applications (Kendall’s τ=0.33; P=0.002). Gender had no significant impact on the attitude toward mobile technology (Mann–Whitney test, U=727.5; P=0.46), neither the length of DM (Kruskal–Wallis test, H(3) =3.331; P=0.343). On the contrary, superior employment status significantly associated with a more positive attitude toward mobile technology (Kruskal–Wallis test, H(8) =28.62; P<0.001).
Discussion
Novelty of the study is brought by the proposed instrument to assess the attitude toward and intention to use modern technology and mobile device applications for DM self-management, as well as its design and validation process. Assessment of the instrument’s validation and reliability was done on a national sample, in conjunction with multiple correlation analysis, including demographic and socioeconomic characteristics, as well as health-related quality of life factors.
The instrument was self-administered or administered by a diabetic resident physician. On the site where the instrument was self-administered, the participants were younger and had a higher education level. On the contrary, on the site where the instrument was administered by a resident physician, the participants were older and had a lower education level. Moreover, each participant was trained about how to fill-in the questionnaire before completion. Therefore, the way the instrument was administered should not influence the answers.
For designing the survey instrument, we took advantage from the TPB and technology acceptance models, which clearly separate the attitude toward intention and actual adoption. We observed that the main components influencing the attitude toward mobile technology and mobile applications for DM self-management were the actual use of electronic devices for DM monitoring and perceived usefulness. In fact, the perceived usefulness has also been found as a principal factor increasing the acceptance of smartphones for health care professionals.Citation33
We observed that younger patients presented a more positive attitude toward and intention to use mobile technology. The result might relay on the fact that young patients are generally more enthusiastic about the use of communication technologies. This fact may overcome the usual barriers to technology adoption,Citation34 in comparison with older patients, for whom using mobile technology and mobile device applications is more challenging.Citation35
Nevertheless, even for the young patients, there is a gap between wanting to use technology in self-management and actually using it.Citation36 Considering the principles of the TPB, we could say that if behavioral intention is under volitional control, other factors may influence it, such as time, financial resources, and technological skills, which represent the actual control over the behavior. Indeed, we found that patients with a higher income, education level, and health-related quality of life had a more favorable attitude toward and intention to use mobile technology for assistive DM control.
Conclusion
New health care strategies should empower the users, the patients themselves, by engaging them in managing their own health. In this context, our study brings the instrument to assess the evidence of effectively beneficial changes mHealth and handheld devices would leverage in the management of chronic diseases.
Acknowledgments
The authors gratefully acknowledge the professionals from the Emergency Hospital of Timisoara and the Diabetics Association of Timisoara, Romania, for their support during the recruitment phase. At the same time, the authors kindly acknowledge their colleagues Otilia-Ana Porojan and Sergiu Gabriel Pop from the Polytechnic University of Timisoara, Romania, for the valuable contribution in the early stages of this work.
Disclosure
The authors report no conflicts of interest in this work.
References
- HamineSGerth-GuyetteEFaulxDGreenBBGinsburgASImpact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic reviewJ Med Internet Res2015172e5225803266
- DayerLHeldenbrandSAndersonPGubbinsPOMartinBCSmart-phone medication adherence apps, potential benefits to patients and providersJ Am Pharm Assoc2013532172181
- WeijmanaIRosWJGRuttenGESchaufeliWBSchabracqMJWinnubstJAMThe role of work-related and personal factors in diabetes self-managementPatient Educ Couns2005591879616198222
- BrunisholzKDBriotPHamiltonSDiabetes self-management education improves quality of care and clinical outcomes determined by a diabetes bundle measureJ Multidiscip Healthc2014753354225473293
- BanduraAHealth promotion by social cognitive meansHealth Educ Behav200431214316415090118
- OnwudiweNCMullinsCDWinstonRABarriers to self-management of diabetes: a qualitative study among low-income minority diabeticsEthn Dis2011211273221462726
- GottfredsonLSDearyIJIntelligence predicts health and longevity, but why?Curr Dir Psychol Sci20041314
- GaikwadRWarrenJThe role of home-based information and communications technical interventions in chronic disease management: a systematic reviewHealth Info J200915122145
- McMahonGTGomesHEHohneSHHuTMLevineBAConlinPRWeb-based care management in patients with poorly controlled diabetesDiabetes Care20052871624162915983311
- FrandesMTimarBToleAHolbanSLungeanuDMobile technology support for clinical decision in diabetic keto-acidosis emergencyStud Health Technol Inform201521031632025991157
- LorigKRitterPLLaurentDDOnline diabetes self-management program: a randomized studyDiabetes Care20103361275128120299481
- TranJTranRWhiteJRSmartphone-based glucose monitors and applications in the management of diabetes: an overview of 10 salient “apps” and a novel smartphone-connected blood glucose monitorClin Diabetes2012304173178
- CurranKNicholsEXieEHarperRAn intensive insulinotherapy mobile phone application built on artificial intelligence techniquesJ Diabetes Sci Technol20104120922020167186
- DonaldHFranklinVGreeneAHThe use of mobile phones in dietary assessment in young people with type 1 diabetesJ Hum Nutr Diet2009223256257
- KnightBAMcIntyreHDHickmanIJNoudMQualitative assessment of user experiences of a novel smart phone application designed to support flexible intensive insulin therapy in type 1 diabetesBMC Med Inform Decis Mak20161611927629774
- HoppeCDCadeJECarterMAn evaluation of diabetes targeted apps for Android smartphone in relation to behaviour change techniques. J Hum Nutr DietEpub20161017113
- ConnellyJKirkAMasthoffJMacRurySThe use of technology to promote physical activity in type 2 diabetes management: a systematic reviewDiabet Med201330121420143223870009
- FreeCPhillipsGGalliLThe effectiveness of mobile-health technology-based health behaviour change or disease management interventions for health care consumers: a systematic reviewPLoS Med2013101e100136223349621
- BentleyCLOtesileOBacigalupoRFeasibility study of portable technology for weight loss and HbA1c control in type 2 diabetesBMC Med Inform Decis Mak2016169227418275
- KirwanMVandelanotteCFenningADuncanMJDiabetes self-management smartphone application for adults with type 1 diabetes: randomized controlled trialJ Med Internet Res20131511e23524225149
- PinnockHSlackRPagliariCPriceDSheikhAProfessional and patient attitudes to using mobile phone technology to monitor asthma: a questionnaire surveyPrim Care Respir J20061523724516843066
- PaddockLEVeloskiJChattertonMLGevirtzFONashDBDevelopment and validation of a questionnaire to evaluate patient satisfaction with diabetes disease managementDiabetes Care200023795195610895845
- StetsonBSchlundtDRothschildCFloydJERogersWMokshagundamSPDevelopment and validation of The Personal Diabetes Questionnaire (PDQ): a measure of diabetes self-care behaviors, perceptions and barriersDiabetes Res Clin Pract201191332133221215487
- EigenmannCASkinnerTColagiuriRDevelopment and validation of a diabetes knowledge questionnairePrac Diabetes2011284166170
- CoxEDFritzKAHansenKWDevelopment and validation of PRISM: a survey tool to identify diabetes self-management barriersDiabetes Res Clin Pract2014104112613524552680
- VuongAMHuberJCBolinJNFactors affecting acceptability and usability of technological approaches to diabetes self-management: a case studyDiabetes Technol Ther201214121178118223013155
- AjzenIThe theory of planned behaviorOrgan Behav Hum Decis Process199150179211
- DavisFDPerceived usefulness, perceived ease of use and user acceptance of information technologyMIS Q1989133319340
- KingWRHeJA meta-analysis of the technology acceptance modelInf Manage2006436740755
- DeVellisRScale Development: Theory and Applications: Theory and ApplicationThousand Oaks, CASage2003
- KimberlinCLWintersteinAGValidity and reliability of measurement instruments used in researchAm J Health Syst Pharm200865232276228419020196
- DeVonHABlockMEMoyle-WrightPA psychometric toolbox for testing validity and reliabilityJ Nurs Scholarsh200739215516417535316
- ChenJParkYPutzerGJAn examination of the components that increase acceptance of smartphones among healthcare professionals. electronicJ Health Inf201052e16
- PenaVWatsonAJKvedarJCGrantRWMobile phone technology for children with type 1 and type 2 diabetesJ Diabetes Sci Technol200931481148920144404
- NesAAvan DulmenSEideEThe development and feasibility of a web-based intervention with diaries and situational feed-back via smartphone to support self-management in patients with diabetes type 2Diabetes Res Clin Pract20129738539322578890
- DobsonKGHallPA pilot study examining patient attitudes and intentions to adopt assistive technologies into type 2 diabetes self-managementJ Diabetes Sci Technol20159230931525427965