
Abstract
Objectives
We examined rheumatologists’ motivation for prescribing biosimilars, assessed their treatment preferences in relation to prescribing behavior and explored patient attitudes to biosimilars.
Methods
Data were taken from the Adelphi Real World Biosimilars Programme, a real-world, cross-sectional study undertaken with German rheumatologists and patients with rheumatoid arthritis, ankylosing spondyloarthritis or psoriatic arthritis in 2015–2016. Rheumatologists provided data on their prescribing behavior and attitudes toward biosimilars and invited the next eight eligible consecutive consulting patients to complete a questionnaire. Rheumatologists were split into “investigative”, “conservative” and “other” groups.
Results
Overall, 50 rheumatologists and 261 patients participated. Biosimilars accounted for <10% of all biologic therapy prescriptions, and >95% of rheumatologists would prescribe a biooriginator rather than biosimilar as the first- or second-line therapy if unrestricted. Patients showed some reluctance to accept biosimilars, and a small proportion of patients were unhappy when switched from a biooriginator to a biosimilar. Satisfaction with treatment was highest in patients who started treatment with a biooriginator prior to biosimilar availability. Patient concerns when starting treatment with a biooriginator or a biosimilar included not knowing enough about the drug (25%–41%), potential side effects (26%–32%) and potential long-term problems (19%–30%).
Conclusion
Study results demonstrate that there is some reluctance from patients to accept biosimilars and the need to educate patients who are unsure to allow them to be involved in decision making, highlighting the importance of patient and physician communication. There remains a need for further research into nonclinical switching and the long-term impact of prescribing biosimilars.
Introduction
The World Health Organization defines biosimilars as “biotherapeutic products […] similar in terms of quality, safety and efficacy to an already licensed reference biotherapeutic product”. For generic drugs, demonstration of identical structure and bioequivalence to the reference product is required for licensing purposes; however, biotherapeutic products (biologics) are larger and more complex entities, and this approach is not considered appropriate for biosimilars.Citation1 A biosimilar must therefore be developed strictly in accordance with procedures used for the reference product (or biooriginator) to ensure that no clinically meaningful differences exist between the “quality, safety and efficacy” and the “safety, purity and potency” of the two.Citation2,Citation3
In 2013, the European Medicines Agency’s (EMA) Committee for Medicinal Products for Human Use (CHMP) approved the marketing of two infliximab biosimilar compounds for the same indications as the biooriginator.Citation4 While Europe has historically been supportive of biosimilar products, this was the first example of a biosimilar monoclonal antibody being approved and provided a defining moment for the use of biosimilars in a highly regulated market.Citation4 Both products were launched in major European markets, including Germany, in February 2015.Citation5,Citation6 Germany has seen some of the highest market shares in the European biosimilars market, with ~50% volume uptake reported.Citation7 Automatic substitution of biooriginators with biosimilars by pharmacists is not allowed in Germany (this is mandated for generics); however, recommended prescribing quotas have been set, although targets vary across regions.Citation8–Citation11
There has been a paucity of published evidence regarding the impact of the launch of biosimilars on physician prescribing, but it would appear that, despite a high level of acceptance from a regulatory standpoint, there is still a marked reluctance from physicians to prescribe biosimilars.Citation12,Citation13 Before prescribing a biosimilar, a physician would require reassurance that it has the same activity and safety profile as the biooriginator and that the quality of the production process is guaranteed – regulatory requirements in both EuropeCitation2 and the USACitation3 ensure this, but concerns apparently remain.Citation14
In one study using an online survey of European physicians across a range of disciplines, lack of a complete and accurate understanding of biosimilars, and the differences between generics and biosimilars, was identified, which might be one factor in the low acceptance levels by physicians.Citation15 In a discrete choice experiment, Hungarian gastroenterologists showed some reluctance to prescribe biosimilars rather than biooriginators in inflammatory bowel disease, although this was less marked in patients who were biologic naive.Citation16,Citation17 In another online survey in Europe, Brazil, Japan and China, rheumatologists with ≤10 years of practicing experience were less likely to prescribe, or more doubtful about prescribing, biosimilars than those with longer experience.Citation18 Less experienced rheumatologists stated that treatment guidelines and a lack of local data were key reasons for not prescribing biosimilars; these were not cited as reasons for nonprescribing by those with >20 years’ practice experience.Citation18 Despite prescription quotas, it has been reported that only a quarter of rheumatologists in Germany feel under pressure from health care authorities to switch patients to biosimilar therapies and that less than a third were aware that approval of the two licensed infliximab biosimilars was for all indications approved for the biooriginator.Citation19
As the active involvement of patients in treatment decisions is advocated, the attitudes of patients to biosimilars are also important; however, little is available in the literature on this topic.Citation20–Citation22 One of the few related publications reports an online survey in Europe and the USA showing only 6% of the general population with even a general impression of biosimilars, although significantly higher awareness (20%–30%) in patients diagnosed with a disease for which one or more biologic therapy is available and who are members of a patient advocacy group.Citation23
A biosimilar for etanercept was approved by CHMP in January 2016, and approval of further biosimilars, a number of which will be treatment options in rheumatoid arthritis (RA), is extremely likely over the next months and years.Citation24 Biosimilars for adalimumab, certolizumab pegol, golimumab, ustekinumab and rituximab are in development.Citation25–Citation28 To ensure optimum uptake of available products, it will be essential to have an in-depth understanding of physicians’ and patients’ perspectives with regard to biosimilars. In particular, it will be important to understand where nonclinical factors are playing a part, something which is clearly lacking in the literature.
This study was undertaken to begin to address the lack of evidence in this evolving field, by examining what motivates prescribing of infliximab biosimilars by rheumatologists, to assess whether rheumatologist preferences match actual prescribing behavior, to explore rheumatology patient acceptance of biosimilars and to understand patient satisfaction and concerns and how these relate to treatment with biooriginators and biosimilars.
Methods
Data were drawn from the Adelphi Real World Biosimilars Programme (2015/2016), a real-world, cross-sectional study based on the completion of detailed record forms by physicians and a self-completion questionnaire by patients (Supplementary materials). The study was undertaken between December 2015 and March 2016 with rheumatologists across Germany. The methodology was based on that used in the Adelphi Real World Disease Specific Programmes, which has been published previously.Citation29
Study population and data collection
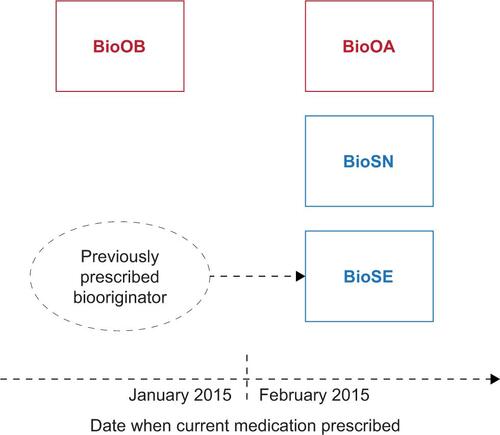
Rheumatologists were identified from public lists, and those meeting the eligibility criteria were invited to participate in the program. Key eligibility criteria were as follows: qualified in rheumatology between 2 and 35 years; actively involved in the management of patients with RA, ankylosing spondyloarthritis (AxSpA) and psoriatic arthritis (PsA) and managing at least one patient with each disease in each of the following patient groups ():
BioSN: patient receiving infliximab biosimilar who was previously biologic naive
BioSE: patient receiving infliximab biosimilar who has experience of a biooriginator
BioOA: patient receiving infliximab biooriginator, initiated after February 2015
BioOB: patient receiving infliximab biooriginator, initiated before January 2015
Participating rheumatologists provided data on their prescribing behavior and attitudes toward biosimilars via a 30-min online survey. They also recruited the next eight consecutive consulting patients aged ≥18 years, with a formal physician-confirmed diagnosis of RA, AxSpA or PsA and being treated with either a biooriginator or a biosimilar. The quota for the study dictated that twice the number of patients being treated with a biosimilar was recruited than those being treated with a biooriginator. Each patient was invited to complete an online patient self-complete form, containing detailed questions on demographics, current conditions, level of satisfaction with current treatment and perspectives and opinions on using biologic therapies, including biosimilars and biooriginators.
Analysis
Rheumatologists were asked to indicate the relative importance to them of a number of factors when making prescribing decisions. Physicians allocated 100 points across prespecified factors in response to the question “When making prescribing decisions which factors are most important to you?” At analysis, factors relating to similar themes were combined into the following three groups:
Investigative: primarily concerned with symptom improvement and disease modification (prespecified factors = “reduction of symptoms”, “disease modification”, “impact on quality of life”)
Conservative: primarily concerned with safety (prespecified factors = “safety”)
Other: influenced primarily by other factors (prespecified factors = “extent of scientific evidence”, “budgetary impact”, “out of pocked cost to patient”, “ease of prescribing”, “likelihood of patient compliance” and “patient acceptability/comfort”)
Physicians were allocated to one of the three groups based on the sum of points they allocated to the factors in the group. If a physician’s allocation of points was higher than the sample mean for a certain group, they were assigned to that group; if their allocation of points was higher than the sample mean for more than one group, they were assigned to the group for which they allocated most points.
Based on their prior experience of biooriginators and biosimilars, patients were split into the four groups indicated previously for analysis. Patients currently receiving biooriginators were classified depending on whether they were prescribed the BioOB or BioOA; a biosimilar alternative was available, as it was considered that this might affect a patient’s attitude toward their medication.
Specific objectives of the analysis were as follows:
To highlight the prescribing behaviors of rheumatologists who already prescribe biosimilars, to explore the factors that motivate them to do so and to investigate whether these factors differ between rheumatologists with different prescribing patterns
To explore whether rheumatologists encounter difficulties in convincing patients to accept biosimilars and whether this differs between patients who were offered a biosimilar when biologic naive, those who were switched from a biooriginator to a biosimilar when a switch was indicated for clinical reasons and those who were switched from a biooriginator to a biosimilar for nonclinical reasons
To assess patient understanding of, and satisfaction and concerns with, biologic treatment and how these differ between those switched to a biosimilar from a biooriginator, those receiving a biosimilar who are biologic naive and those who remain on a biooriginator
Descriptive statistics presented are as follows: for numeric variables, the mean and standard deviation; for categorical variables, the number and percentage of subjects in each category.
Ethics
Patients provided informed consent via a tick box on the front of the patient self-completion questionnaire. The data were collected according to market research guidelines; hence, no source validation was possible or required.Citation30 Patient and doctor identities were not known to the analysis team. No identifiers were recorded for the patients; patient and physician forms for the same “matched” patients were linked by unique numeric codes preprinted on the questionnaires. The study performed in accordance with the European Pharmaceutical Marketing Research Association (EphMRA) guidelines and the US Health Insurance Portability and Accountability Act 1996.
Results
A total of 50 rheumatologists participated in this study, with 23 rheumatologists assigned to the “investigative” analysis group, 17 rheumatologists assigned to the “conservative” group and 10 rheumatologists assigned to the “other” group. Patient self-completion questionnaires were completed by 261 patients (133 RA, 65 PsA and 63 AxSpA), with 88, 86, 40 and 47 patients in the BioSN, BioSE, BioOA and BioOB groups, respectively.
Prescribing behaviors
Biosimilars made up <10% of the biologic therapies and <4% of all drugs that rheumatologists prescribed for the three conditions under study (). There was an expectation by the participating rheumatologists that this would increase over the following 12 months, with the greatest proportion of future biosimilar prescribing anticipated for patients with AxSpA (). When asked about their preferences for prescribing under the assumption of unrestricted circumstances (ie, no prescribing guidelines or other restrictions), >95% of rheumatologists indicated that they would prefer to prescribe a biooriginator to a biosimilar as either the first-line therapy or the second-line therapy; this decreased to 80%–92% when considering the third-line therapy ().
Figure 1 Rheumatologist prescribing preference when it is assumed that there are no restrictions or guidelines.
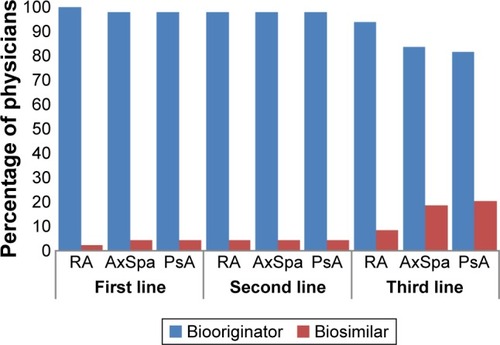
Table 1 Rheumatologist-stated prescribing of biosimilars currently and expected in 12 months
When asked their reasons for prescribing biosimilars instead of biooriginators, 86% of investigative rheumatologists indicated that a desire to get experience with the new product(s) was a reason and 64% of them indicated that a belief that efficacy is equivalent to the biooriginator was a reason (). A desire to get experience with the new product(s) and a belief that efficacy is equivalent to the biooriginator were indicated as reasons for prescribing biosimilars instead of biooriginators by 65% of conservative rheumatologists and 50% of those in the other group (). Only 64% of investigative rheumatologists selected the lower cost of the biosimilar as a reason for prescribing a biosimilar rather than the biooriginator, compared to 71% of conservative rheumatologists and 88% of those in the other group ().
Figure 2 Rheumatologists’ prescribing behaviors.
*Compared to the prescription of a biooriginator.
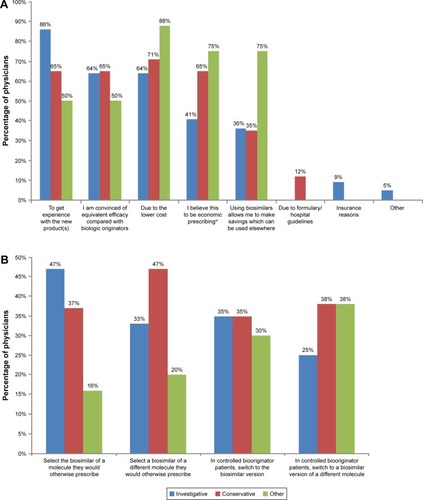
In providing as many responses as they wished to the question “Once biosimilars are more widely available, how do you expect to use them?”, the response selected by the highest proportion (47%) of investigative rheumatologists was “When a treatment change is required, I will select the biosimilar version of a molecule I would otherwise have prescribed”; this was selected by 37% of conservative rheumatologists and only 16% of those in the other group ().
When a treatment change is required, I will select a biosimilar of a different molecule rather than the branded molecule I would otherwise have prescribed
Patient attitudes
The mean percentage of patients in the BioSN group (never previously prescribed a biooriginator or a biosimilar) reported by rheumatologists to accept a biosimilar without reluctance was 70%, compared to 56% of patients currently receiving a biooriginator and with no clinical reason for a change in therapy (). A small proportion of patients would not accept treatment with a biosimilar but would accept the biooriginator; the mean values across rheumatologists were 7.3% of biologic-naive patients and 18.5% of those currently treated with a biooriginator and with no clinical indication for a therapy change (). Rheumatologists reported that a small proportion (mean ~5%) of patients refused any form of biologic therapy, regardless of the patient’s prior experience with biologic therapy or the reason for a switch in therapy ().
Table 2 Patient acceptance of biosimilars
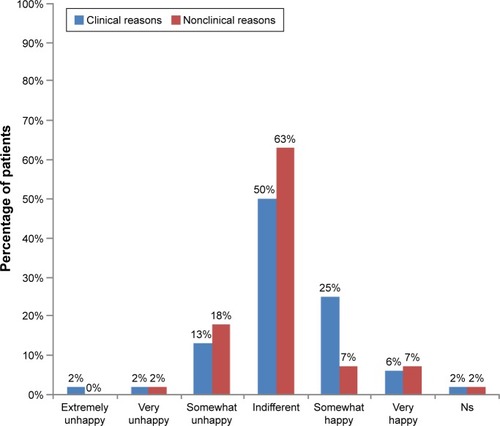
The majority of patients being changed from a biooriginator to a biosimilar were indifferent to the change (). A slightly higher proportion of patients with no clinical reason for the change indicated some degree of unhappiness compared with those being switched for clinical reasons, and a numerically greater proportion of patients who were somewhat happy with the change were being changed for clinical reasons ().
Figure 3 Patient happiness to switch from biooriginator to biosimilar.
Patient understanding, concerns and satisfaction
The majority of patients were satisfied with the current treatment of their condition (). Patients who had been receiving a biooriginator since before biosimilars were introduced (BioOB group) appeared to be more satisfied than those in other groups, with 38% of this group being very satisfied (), compared to 27%, 30% and 22% in the BioSN, BioSE and BioOA groups, respectively.
Figure 4 Patient perceptions of biosimilars.
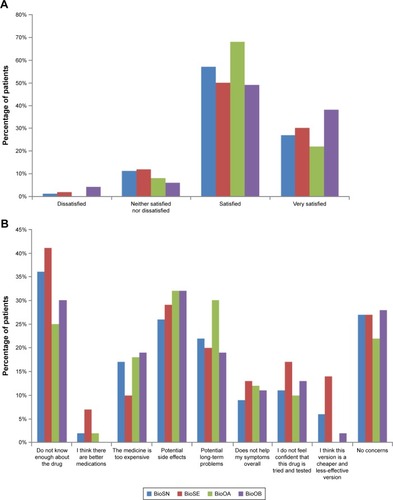
When patients were asked what concerns they had when they were first prescribed their current treatment, the concern most commonly indicated was that they did not know enough about the drug; 36%–41% of patients prescribed a biosimilar selected this option compared to 25%–30% of patients prescribed a biooriginator (). Few patients expressed a concern that there were better medications available or that they were being given a cheaper and less effective medication, although this was more of a concern for patients prescribed a biosimilar who had previously received a biooriginator than those from the other patient groups (). Concern about potential side effects was expressed by 26%–32% of patients, with the highest proportions indicating this as a concern being those groups receiving biooriginators (). The proportion of patient concerned that their medication was too expensive was similar (17%–19%) between the group of previously biologic-naive patients prescribed a biosimilar and both groups prescribed a biooriginator; it was somewhat lower (10%) in those prescribed a biosimilar who had previously received a biooriginator (). However, 14% of biologic-naive patients prescribed a biosimilar felt they were being given a cheaper and less-effective version compared to 0–6% of patients in the other groups.
Discussion
This article reports current and anticipated prescribing of biosimilars, prescribing preferences and behavior and patient attitudes regarding biosimilars, in the disease areas of RA, AxSpA and PsA.
Reported levels of biosimilar prescribing were low, with fairly modest increases anticipated by physicians over the following 12 months. This may reflect the relatively recent introduction of biosimilars in the field of rheumatology; biosimilars for the treatment of chemotherapy-induced neutropenia have 60%–80% market share across the European “big 5” countries.Citation7 A report published in March 2016 predicted that biosimilars will result in a highly competitive marketplace over the next 5 years.Citation28 There was a marked reluctance on the part of rheumatologists to prescribe biosimilars; the majority indicated they would prefer to prescribe a biooriginator to a biosimilar if there were no guidelines or restrictions for prescribing. Marginally more would prescribe a biosimilar for patients with AxSpA or PsA compared to those with RA; this might reflect the greater range of treatment options currently available for RA than for the other conditions.
More than half of the participating rheumatologists in each of the analysis groups included a wish to gain experience with biosimilars as a reason for prescribing a biosimilar over a biooriginator; this was a reason for 86% of rheumatologists in the investigative analysis group. However, investigative rheumatologists appeared less concerned about economic factors than those in the conservative or other analysis group. Very little has been published about the reasons that physicians prescribe biosimilars; in a survey of Italian oncologists, 26% indicated that they would use a biosimilar for the treatment of chemotherapy-induced anemia as they felt this was scientifically supported, while 54% indicated cost saving as motivation for the treatment choice.Citation29 All participating rheumatologists were required to be currently prescribing biosimilars at the first-line therapy; however, a strong preference was indicated for using biooriginators as the first-line therapy should no prescribing restrictions exist, suggesting a possible disconnect between rheumatologists’ prescribing behaviors and preferences and some resistance to payer-driven guidelines.
Some reluctance was observed in patients’ willingness to accept being prescribed a biosimilar, particularly among patients currently treated with a biooriginator and with no clinically indicated reason for a switch of therapy; 21% of patients with no clinical reason for the change were somewhat or very unhappy about the switch. As the methodology did not allow for probing to understand the reasons for particular responses, we cannot be certain why some patients were unhappy to be changed from a biooriginator to a biosimilar and others appeared unconcerned. Not knowing enough about the drug was the most common concern of patients when first prescribed their medication; it is likely that this lack of knowledge was critical in the reservations some patients had with regard to biosimilars. It is also likely that the interaction between the rheumatologist and patient will have influenced the patient’s viewpoint, either due to the rheumatologist taking the time to ensure that the patient was well informed to reach a shared treatment decision or due to the patient trusting the rheumatologist to make an appropriate treatment decision on their behalf. It is interesting that fewer patients prescribed a biosimilar who had previously received a biooriginator felt that their medication was too expensive compared with the other patient groups, yet more of this group was concerned that they were being given a cheaper and less-effective version than the other groups. It seems likely that these findings reflect patient perceptions of the differing balance of cost and likely effectiveness between biooriginators and biosimilars.
Limited research of patient acceptance of biosimilars has been identified; a survey of patients with type 1 and type 2 diabetes in the USA reported that 66% of patients indicated that they would “definitely” or “likely” use a less-expensive insulin biosimilar if one were available.Citation30 In the current study, the most common concern indicated by patients when prescribed a new treatment was that they did not know enough about the drug, especially for patients prescribed a biosimilar. The fact that, despite this, 27% of patients receiving a biosimilar had no concerns when first prescribed this treatment might reflect differing physician–patient interactions, with patients whose rheumatologist ensured that they know all they wish to about the treatment having no concerns, while other patients were not well informed by their rheumatologists and indicated this as a concern. These results indicate that patient and physician communication is important and further investigation may be required to determine the extent that additional factors are influencing the conversations. Potential factors, such as volume of patients seen at hospital, care setting and clinician empathy, may affect the time spent on discussing the prescribing of a biosimilar, and such research will help determine how this impacts on patient outcomes. Concern that there are better medications available was low in this study, although a little higher in those receiving biosimilars compared to those on biooriginators. Concern about potential side effects was indicated by around one-quarter to one-third of patients receiving biosimilars and around one-third of those receiving biooriginators. Patients with diabetes expressed concerns about the efficacy and side effects of a biosimilar insulin compared with the biooriginator.Citation30 In a survey of patients diagnosed with diseases with biologic treatment options together with members of the general public, 46%–51% of respondents who were aware of biosimilars agreed that biosimilars were effective, with 43%–47% agreeing that they were safe.Citation23
Some limitations of this study are acknowledged. The study was performed in Germany, which has an advanced health care system and broad access to treatment, which is not universally the case; generalization of the findings beyond Germany warrants caution.Citation31–Citation34 The eligibility criteria might have resulted in participating rheumatologists being skewed toward those with a higher workload, and the requirement for rheumatologists to be prescribing biosimilars as the first-line treatment might have resulted in participants who are early adopters of new therapies with different perceptions of biosimilars to rheumatologists who do not prescribe biosimilars. Only patients who presented to a rheumatologist and agreed to participate were included; as a result, the sample might include overrepresentation of patients who consult more frequently and whose characteristics, perceptions, attitudes and concerns differ from the broader patient population. This study did not explore the reasons for patients’ medication-related concerns and any lack of satisfaction with treatment; a further in-depth qualitative study would provide further insight to patient’s perspectives on these issues. Finally, the relatively low sample sizes precluded statistical testing for differences between analysis groups, and this was a cross-sectional study rather than a longitudinal study; thus, descriptive data are presented assessing the association between factors rather than an assessment of causality.
It is predicted that by 2020, biologics will form 28% of the global pharmaceutical market by value across all therapeutic areas, with biosimilars offering potential savings of >50 billion euros across the European big 5 countries and the USA.Citation28 Objective patient education about the safety, efficacy and other attributes of all available therapies, including nonbiologics, biooriginators and biosimilars, is critical to allow informed shared decision-making. The findings reported here support a number of publicationsCitation35,Citation36 suggesting that education of physicians and patients, among other stakeholders, about biosimilars is essential to assist informed decision-making and improve acceptance and use of biosimilars where appropriate.Citation20,Citation37,Citation38 Further research with rheumatologists and patients to further investigate their understanding, perspectives, and concerns in regard to biooriginators and biosimilars will help ensure that appropriate information is included in any educational initiative.
Key messages
Cost and desire for experience are key factors driving physicians to prescribe biosimilars.
Study results demonstrate that there is some reluctance from patients to accept biosimilars.
There remains a need to educate patients and rheumatologists who are unsure about biosimilars.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
This study was funded by Merck & Co.
Supplementary materials
Questions asked of physicians were as follows:
– What percentage of your patients with each condition are currently receiving each product?
– What percentage of your patient do you expect will be receiving each product in 12 months’ time?
– Assuming there were no restrictions on your prescribing or guidelines you need to follow, what advanced therapy would you prefer to use first, second and third for each condition?
– Why did you prescribe the biosimilar(s) rather than the originator biologic(s)?
○ I wanted to get experience with the new product(s)
○ I am convinced of equivalent efficacy compared with biologic originators
○ Due to the lower cost
○ I believe this to be economic prescribing
○ Using biosimilars allows me to make savings which can be used elsewhere
○ Due to formulary/hospital guidelines
○ Insurance reasons
○ Other, specify
– Once biosimilars are more widely available, how do expect you might use them?
○ When a treatment change* is required I will select the biosimilar version of a molecule I would otherwise have prescribed.
○ When a treatment change* is required I will select a biosimilar of a different molecule rather than the branded biologic molecule I would otherwise have prescribed.
○ In controlled patients currently receiving a branded biologic, I will switch the branded biologic to the biosimilar version.
○ In controlled patients currently receiving a branded biologic, I will switch the branded biologic to a bio-similar version of a different molecule.
– Thinking of all the patients who had never before received a biologic originator or biosimilar (ie, biologic/biosimilar naive) for whom you tried to prescribe a biosimilar, what proportion?
○ Accepted the switch onto a biosimilar without any reluctance.
○ Were reluctant to take a biosimilar but finally accepted as they had no other choice.
○ Refused the biosimilar and remained on their existing biologic originator.
○ Refused the biosimilar and either switched to an alternative biologic originator or discontinued biologic therapy completely.
– Thinking of all the patients who were receiving an originator biologic who, when they needed a switch of therapy you tried to prescribe a biosimilar, what proportion?
○ Accepted the switch onto a biosimilar without any reluctance.
○ Were reluctant to take a biosimilar but finally accepted as they had no other choice.
○ Refused the biosimilar and remained on their existing biologic originator.
○ Refused the biosimilar and either switched to an alternative biologic originator or discontinued biologic therapy completely.
– Thinking of all the patients who were receiving an originator biologic who did not clinically need a switch of therapy but you tried to prescribe a biosimilar, what proportion?
○ Accepted the switch onto a biosimilar without any reluctance.
○ Were reluctant to take a biosimilar but finally accepted as they had no other choice.
○ Refused the biosimilar and remained on their existing biologic originator.
○ Refused the biosimilar and either switched to an alternative biologic originator or discontinued biologic therapy completely.
Questions asked of patients were as follows:
– How happy were you to switch from a biooriginator to your current treatment?
○ Extremely unhappy
○ Very unhappy
○ Somewhat unhappy
○ Indifferent
○ Somewhat happy
○ Very happy
○ Extremely happy
– Which option best describes your satisfaction with how well your current treatment is controlling your condition/symptoms?
○ Very dissatisfied
○ Dissatisfied
○ Neither satisfied or dissatisfied
○ Satisfied
○ Very satisfied
– What concerns, if any, did/do you have about taking this medication at the times indicated at the top of the columns?
○ Don’t know enough about the drug
○ I think there are better medications
○ The medicine is too expensive
○ Potential side effects
○ Potential long term problems
○ Doesn’t help my symptoms overall
○ I don’t feel confident that this drug is tried and tested
○ I think this version is a cheaper and less-effective version
○ Other
Note: *We are defining a treatment change as either initiation of 1st biologic or biologic switch.
Figure S1 Patient analysis groups based on current medication.
Notes: BioOA, patient receiving biooriginator who was initiated after February 2015; BioOB, patient receiving biooriginator who was initiated before January 2015; BioSN, patient receiving biosimilar who was previously biologic naive; BioSE, patient receiving biosimilar who has an experience of a biooriginator.
Disclosure
CMB and SK are employees of Merck & Co. and may hold stock and/or options. JW, ES and JP are employees of Adelphi Real World. The authors report no other conflicts of interest in this work.
References
- Expert Committee on Biological Standardization [webpage on the Internet]Guidelines on Evaluation of Similar Biotherapeutic Products (SBPs)GenevaWorld Health Organisation2009134 Available from: http://www.who.int/biologicals/areas/biological_therapeuticsAccessed July 29, 2016
- Committee for Medicinal Products for Human Use (CHMP)Guideline on similar biological medicinal products containing biotechnology-derived proteins as active substance: quality issuesLondon2012 cited July 29, 201619 Available from: http://www.ema.europa.eu/docs/en_GB/document_library/Scientific_guideline/2014/06/WC500167838.pdfAccessed March 2, 2017
- US Food and Drug AdministrationQuality Considerations in Demonstrating Biosimilarity to a Reference Product: Draft Guidance2012 Available from: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM291134.pdfAccessed July 29, 2016
- BeckAReichertJMApproval of the first biosimilar antibodies in EuropemAbs20135562162323924791
- McKee S [webpage on the Internet]Hospira launches Remicade biosimilar in major EU markets2015 Available from: http://www.pharmatimes.com/news/hospira_launches_remicade_biosimilar_in_major_eu_markets_971052Accessed August 12, 2016
- Hernandez R [webpage on the Internet]Celltrion Launches Remicade Biosimilar in European Markets Available from: http://www.biophar-minternational.com/celltrion-launches-remicade-biosimilar-european-marketsAccessed August 12, 2016
- Generics and Biosimilars Initiative [webpage on the Internet]Use of biosimilars in Europe differs across countries GaBOnline2014 [cited July 11, 2016]. Available from: http://www.gabionline.net/Reports/Use-of-biosimilars-in-Europe-differs-across-countriesAccessed July 11, 2016
- NiederwieserDSchmitzSBiosimilar agents in oncology/haematology: from approval to practiceEur J Haematol201186427728821175852
- Regulation RahmenvertragGerman Bundesministerium der Justiz German Social Law Book ‘Aut idem’§ 129;2008 p section 4 sentence 1. Available from: http://www.gesetze-im-internet.de/sgb_5/__129.htmlAccessed March 2, 2017
- GaBI Online – Generics and Biosimilars Initiative [webpage on the Internet]UK biosimilars uptake lower than in some other EU countries Available from: http://gabionline.net/Reports/UK-biosimilars-uptake-lower-than-in-some-other-EU-countriesAccessed August 12, 2016
- RoviraJEspínJGarcíaLOlry de LabryAThe impact of biosimilars’ entry in the EU market Report prepared for the European Commission (Directorate-General for Enterprise and Industry)BrusselsEuropean Commission2011 Available from: http://ec.europa.eu/DocsRoom/documents/7651/attachments/1/translations/en/renditions/pdfAccessed October 3, 2016
- WeiseMKurkiPWolff-HolzEBielskyM-CSchneiderCKBiosimilars: the science of extrapolationBlood2014124223191319625298038
- ZelenetzADAhmedIBraudELNCCN Biosimilars White Paper: regulatory, scientific, and patient safety perspectivesJ Natl Compr Cancer Netw20119suppl 4S1S22
- AaproMSWhat do prescribers think of biosimilars?Target Oncol20127suppl 1S51S5522258706
- DolinarROReillyMSBiosimilars naming, label transparency and authority of choice – survey findings among European physiciansGenerics Biosimilars Initiat J2014325862
- BajiPGulácsiLLovászBDTreatment preferences of originator versus biosimilar drugs in Crohn’s disease; discrete choice experiment among gastroenterologistsScand J Gastroenterol2016511222726059967
- BajiPGulácsiLGolovicsPAPerceived risks contra benefits of using biosimilar drugs in ulcerative colitis: discrete choice experiment among gastroenterologistsValue Health Reg Issues201610859027881284
- NarayananSRelationship between the duration of rheumatology practice experience and likelihood of use and perception towards biosimilars in rheumatoid arthritis arenaAnn Rheum Dis201473suppl 262462424257024
- Decision Resources Group [webpage on the Internet]German Rheumatologists and Gastroenterologists Say They Are Not Under Pressure to Switch Patients on Remicade to Infliximab Biosimilars2015 Available from: http://www.prnewswire.com/news-releases/german-rheumatologists-and-gastroenterologists-say-they-are-not-under-pressure-to-switch-patients-on-remicade-to-infliximab-biosimilars-300145025.htmlAccessed March 2, 2017
- NotaIDrossaertCHCTaalEVonkemanHEvan de LaarMAPatient participation in decisions about disease modifying anti-rheumatic drugs: a cross-sectional surveyBMC Musculoskelet Disord20141533325281209
- ZangiHANdosiMAdamsJEuropean League Against Rheumatism (EULAR)EULAR recommendations for patient education for people with inflammatory arthritisAnn Rheum Dis201574695496225735643
- CaseyDKey strategic factors for stakeholders in the current global biosimilar marketDrug Discov Today201621220821126375407
- JacobsISinghESewellKLAl-SabbaghAShaneLGPatient attitudes and understanding about biosimilars: an international cross-sectional surveyPatient Prefer Adherence20161093794827307714
- European Medicine AgencySummary of the risk management plan (RMP) for Benepali (etanercept)EMA201513 Report No: EMA/783235/2015. Available from: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Risk-management-plan_summary/human/004007/WC500196679.pdfAccessed August 12, 2016
- Generics and Biosimilars Initiative [webpage on the Internet]Biosimilars of adalimumab2014 Available from: http://www.gabion-line.net/Biosimilars/General/Biosimilars-of-adalimumabAccessed August 12, 2016
- Pfenex [webpage on the Internet]Pfenex, Biosimilars, and Better Health2015 Available from: http://www.pfenex.com/the-pfenex-difference/Accessed August 12, 2016
- Investor Overview – InvestorsEPIRUS Biopharmaceuticals, Inc. Available from: http://ir.epirusbiopharma.com/Accessed August 12, 2016
- Novartis [webpage on the Internet]Sandoz’ biosimilar rituximab regulatory submission accepted by European Medicines AgencyNovartis Available from: https://www.novartis.com/news/media-releases/sandoz-biosimilar-rituximab-regulatory-submission-accepted-european-medicinesAccessed August 12, 2016
- AndersonPBenfordMHarrisNKaravaliMPiercyJReal-world physician and patient behaviour across countries: Disease-Specific Programmes – a means to understandCurr Med Res Opin200824113063307218826746
- European Pharmaceutical Market Research Association [webpage on the Internet]European Pharmaceutical Market Research Association – Code of ConductEphMRA Available from: http://www.ephmra.org/Code-of-Conduct-SupportAccessed January 19, 2017
- IMSDelivering on the Potential of Biosimilar Medicines the Role of Functioning Competitive Markets2016140 Available from: https://www.imshealth.com/files/web/IMSH%20Institute/Healthcare%20Briefs/Documents/IMS_Institute_Biosimilar_Brief_March_2016.pdfAccessed August 12, 2016
- CortinovisDBerettaGPiazzaEAIOM LombardiaChemotherapy-induced anemia and oncologist perception on treatment: results of a web-based surveyTumori2013991455023548999
- WilkinsARVenkatMVBrownASPatient perspectives on biosimilar insulinJ Diabetes Sci Technol201481232524876533
- PutrikPRamiroSKvienTKWorking Group ‘Equity in access to treatment of rheumatoid arthritis in Europe’Inequities in access to biologic and synthetic DMARDs across 46 European countriesAnn Rheum Dis201473119820623467636
- Rak TkaczukKHJacobsIABiosimilars in oncology: from development to clinical practiceSemin Oncol201441suppl 3S3S12
- MoorkensEJonker-ExlerCHuysIDeclerckPSimoensSVultoAGOvercoming barriers to the market access of biosimilars in the European Union: the case of biosimilar monoclonal antibodiesFront Pharmacol2016719327445826
- PutrikPRamiroSLieELess educated and older patients have reduced access to biologic DMARDs even in a country with highly developed social welfare (Norway): results from Norwegian cohort study NOR-DMARDRheumatology (Oxford)20165571217122427012686
- PutrikPRamiroSKvienTKSokkaTUhligTBoonenAVariations in criteria regulating treatment with reimbursed biologic DMARDs across European countries. Are differences related to country’s wealth?Ann Rheum Dis201473112010202123940213