
Abstract
Background
Poor adherence to treatment is a problem in glaucoma, and patient dissatisfaction with topical glaucoma medication is a barrier to adherence. The objective of this study was to evaluate glaucoma patients’ satisfaction with fixed-combination bimatoprost/timolol ophthalmic solution (BTFC).
Methods
This observational, multicenter study was conducted in China in adults with glaucoma treated with BTFC for 1–3 months. Five hundred patients answered a questionnaire concerning their demographic characteristics, history of glaucoma and topical glaucoma treatment, and use of BTFC. The primary endpoint was patient satisfaction with BTFC assessed on a 10-point scale (1= very dissatisfied, 10= very satisfied).
Results
Patients received BTFC alone (65%) or with other treatments (35%), most commonly a carbonic anhydrase inhibitor. Most patients (87%) used BTFC as a replacement for other medication, usually a β-blocker or prostaglandin analog; 13% received BTFC as add-on treatment. Key reasons for initiating BTFC therapy were poor efficacy of previous treatment (72% of patients) and side effects of previous treatment (32% of patients). Most patients agreed or very much agreed that BTFC provided better control of intraocular pressure (85% of patients), had a simpler administration (87% of patients), and was associated with better tolerance and comfort (82% of patients) compared with their previous treatment. Mean satisfaction scores were significantly higher for BTFC than for previous treatments among all patients (7.8 versus 6.0; P<0.0001) and within patient subgroups based on demographic characteristics, pattern of BTFC use, and previous treatment.
Conclusion
Patients were highly satisfied with BTFC used alone or concomitantly with another topical medication. Patients previously treated with a β-blocker, prostaglandin analog, carbonic anhydrase inhibitor, α-adrenergic agonist, or combination of two medications were more satisfied with BTFC than with their previous treatment. Most reported that intraocular pressure control, tolerability, and ease of administration improved with BTFC.
Introduction
The goal of treatment in patients with glaucoma is to reduce intraocular pressure (IOP) and consequently lower the risk of visual field loss.Citation1 Many topical medications that effectively lower IOP are available, including β-blockers, carbonic anhydrase inhibitors, prostaglandin analogs, sympathomimetics, and miotics.Citation2 In China, the most commonly used topical IOP-lowering medications are β-blockers (eg, timolol), prostaglandin analogs (bimatoprost, latanoprost, and travoprost), the α-agonist brimonidine, the carbonic anhydrase inhibitor brinzolamide, and fixed combinations of a prostaglandin analog, brimonidine, or brinzolamide with timolol. However, poor adherence of glaucoma patients to topical IOP-lowering therapy is endemic. Patient surveys and studies using devices that measure drops dispensed from medication bottles have suggested that at least 20% of patients do not use their medication as prescribed.Citation3–Citation5 Furthermore, pharmacy claims data studies have suggested that patients have medication available for dosing on an average of only 56% (range, 37%–92%) of days in the year following the index prescription,Citation4 and in one study, only 10% of patients had medication available for dosing each day of the year.Citation6 Poor adherence remains a significant limiting factor in the management of glaucoma because it is associated with greater loss of the visual field.Citation7,Citation8
Barriers to adherence to topical glaucoma treatment are common and include difficulty in eye drop administration, dosing frequency, inconvenience, forgetfulness, side effects, lack of understanding of the disease, and medication cost.Citation9–Citation12 Furthermore, patients with glaucoma frequently have ocular surface disease, which can affect the tolerability of topical glaucoma medication.Citation13 In a multicenter international study, ocular surface disease was reported to be present in 59.2% of glaucoma patients using topical IOP-lowering medication.Citation14 It is understood that adherence is better when patients have no problems with their medication and are satisfied with their treatment. A survey study by Day et alCitation15 demonstrated that glaucoma and ocular hypertensive patients’ satisfaction with the effectiveness, ease, and convenience of topical treatment was significantly associated with reduced reluctance of the patients to use the treatment. In another study, most patients with glaucoma expressed a preference for dosing with a single drop each day, and 20% of patients believed that this dosing schedule would improve adherence.Citation16 These results suggest that simplifying the treatment regimen using effective IOP-lowering medication may improve patient satisfaction and adherence to treatment.
Fixed combinations of IOP-lowering medications reduce the inconvenience associated with administration of multiple drops each day and may improve adherence.Citation17 The fixed combination of bimatoprost 0.03%/timolol 0.5% (BTFC; Ganfort®, Allergan plc, Dublin, Ireland) has been shown to be well tolerated and effective in lowering IOP in multiple clinical studies, including studies in Chinese patients with glaucoma or ocular hypertension.Citation18–Citation21 However, patient satisfaction with BTFC treatment has not been fully explored. The primary objective of the present study was to assess glaucoma patients’ satisfaction with BTFC and with the efficacy, tolerability, and ease of use of BTFC in clinical practice in China.
Methods
This observational, multicenter, survey study was conducted from July 2015 to November 2015 at 20 sites in eight cities in China (Beijing, Shanghai, Guangzhou, Hangzhou, Nanjing, Changsha, Fuzhou, and Chengdu). All study procedures were in accordance with the Helsinki Declaration of 1975, as revised in 2000. The study was exempt from approval by the local ethics committees because it involved a survey procedure only, with adult participants, and no personally identifiable data were collected. There was no potential harm or risk to the participants. The participants’ responses were confidential, and the nature of the survey was such that if there were a breach, the disclosure of participants’ responses would not place the participants at risk of criminal or civil liability or be damaging to the participants’ financial standing, employability, or reputation. There were no negative repercussions for patients who chose not to participate. Patients were informed of the objective of the study, that their participation was voluntary, and that their responses would remain anonymous and confidential. They were also informed that they could withdraw from participation at any time and for any reason. Patients who completed the survey after being so informed were deemed to have provided informed consent.
A participating physician at the site introduced patients who were potentially eligible for the study to an investigator who then screened them for eligibility. Any adult outpatient diagnosed with glaucoma who had been using BTFC for 1–3 months was eligible. An upper limit of 3 months’ use was chosen to avoid bias, because we wanted to compare patients’ satisfaction with BTFC versus their previous treatment, and patients may better remember their satisfaction with a previous regimen when it was used within the past 3 months. The investigator administered a questionnaire to all eligible patients who agreed to participate. There were eight investigators (one per site), and all of the surveys at a site were administered by the same investigator. The investigator read the survey questions aloud and recorded the patient’s answers, because we anticipated that some of the patients would have very poor vision due to advanced glaucoma and would be unable to read and respond to a written survey. The questions were designed with simple wording to make them easily understandable and minimize any ambiguity. All of the investigators were trained to present the survey in a standard and objective manner. The questionnaire took approximately 10 minutes to complete. Data collected included patient demographics (gender, age, employment status, insurance status, household income), history of glaucoma, previous use of glaucoma treatment, duration and patterns of use of BTFC, reasons for the treatment change to BTFC, patient overall satisfaction with BTFC, and patient satisfaction with the IOP control provided by BTFC, the tolerability of BTFC, and the ease of administration of BTFC compared with previous treatment. In the assessment of reasons for using BTFC, patients were asked to indicate “yes” or “no” to potential reasons including poor efficacy of previous medication(s), safety profile/side effect of previous medication(s), BTFC recommended by friends/family members/other patients, inconvenient administration of previous medication(s), patient’s desire to try BTFC, cost of previous medication(s), and physician’s recommendation. Patients were also encouraged to provide other reasons.
Patients rated their overall satisfaction with BTFC and their overall satisfaction with their previous treatment on a 10-point scale from 1= extremely dissatisfied to 10= extremely satisfied. To evaluate patient satisfaction with the efficacy, tolerability, and ease of administration of BTFC, patients were asked whether they very much agreed, agreed, neither agreed nor disagreed, disagreed, or very much disagreed with the following statements: 1) BTFC provides better control of IOP compared with previous treatment; 2) BTFC has characteristics of better tolerability and comfort compared with previous treatment; and 3) administration of BTFC is simpler compared with previous treatment.
All statistical analyses were performed using SAS software (SAS Institute Inc, Cary, NC, USA). Between-group comparisons of mean satisfaction scores used independent samples t-tests; within-group comparisons used paired t-tests. The planned sample size was 500 patients.
Results
Patients were recruited at 20 investigational sites. Of the patients who were screened as potential candidates for the survey, approximately 70% met the criteria for participation in the study. Approximately 40% of eligible patients declined to participate, and 60% were administered the questionnaire.
A total of 500 patients with glaucoma from eight cities in China (56% from Tier 1 cities, 44% from Tier 2) completed the survey. Demographic characteristics of the patients are presented in . The mean age was 51 years, and 56.6% of the patients were female. Most patients either worked full time or were retired and had relatively good economic status (46.2% had a household income ≥60,000 RMB). Overall, 85% of the 500 respondents had medical insurance.
Table 1 Demographic characteristics
On average, the patients had been diagnosed with glaucoma 27 months previously and had used topical IOP-lowering drops for the previous 26 months (). All patients had begun IOP-lowering drops within 1 year of the diagnosis, and nearly 91% had initiated treatment immediately after diagnosis. Patients had been using BTFC for at least 1 month and no more than 3 months at the time of the survey; the majority (62.8%) had been using BTFC for 1–2 months ().
Table 2 Glaucoma and treatment history
BTFC was used alone by 65% of patients; the other 35% of patients used BTFC in a regimen that included other topical IOP-lowering medication, most commonly a carbonic anhydrase inhibitor (14.2% of patients, ). A significant number of patients (9.4%) used BTFC as adjunctive therapy with a prostaglandin analog (usually latanoprost or travoprost), 5.0% of patients used BTFC with a β-blocker, and 4.6% of patients used BTFC with an α-adrenergic agonist. Only four patients (0.8%) used BTFC in a multiple-drug regimen that included two or more other medications ().
Table 3 Pattern of BTFC use
For 87% of patients, BTFC replaced some or all of the medication(s) used in their preexisting regimen: 32.2% of patients replaced a β-blocker with BTFC, and 20.8% replaced a prostaglandin analog with BTFC (). For 13% of patients, BTFC was added to the preexisting regimen. The most common reason for initiating BTFC therapy was poor efficacy of the previous treatment (67.2% of patients, ). Other common reasons were side effects of the previous treatment (30.8% of patients), recommendations from friends, family, or other patients (31.0% of patients), and inconvenient administration of the previous treatment (20.0% of patients).
Table 4 Reasons for initiating BTFC therapy
Patients reported greater satisfaction with BTFC than with their previous treatment. Mean (± standard deviation, SD) satisfaction scores in the total patient population were 7.8±1.6 for BTFC versus 6.0±1.5 for previous treatment (P<0.0001, ). Patient satisfaction scores for BTFC were also significantly higher than for previous treatment in patient subgroups defined by the pattern of BTFC use (used alone or with at least one other drug, and used as replacement or add-on therapy), previous treatment, reasons for changing treatment, and duration of BTFC treatment (), as well as in patient subgroups defined by gender, age, insurance coverage, employment status, and household income ().
Table 5 Mean BTFC and previous treatment satisfaction scores in all patients and subgroups based on treatment parameters
Table 6 Mean BTFC and previous treatment satisfaction scores in patient subgroups based on demographics
The level of patient satisfaction with BTFC was higher in patients who used BTFC as a replacement for other medication than in those who added it to previous treatment (mean ± SD scores of 8.0±1.4 versus 6.8±2.3, P<0.0001). Similarly, the level of patient satisfaction with BTFC was higher in patients previously treated with a prostaglandin analog than in those previously treated with a carbonic anhydrase inhibitor (P=0.0004) or a combination of two drugs (P=0.0008) (mean ± SD scores of 8.1±1.4, 7.5±1.6, and 7.3±2.1, respectively). The mean score of patient satisfaction with BTFC was 7.1 in patients aged 18–30 years and ranged from 7.8–8.2 in patients aged 41–70 years ().
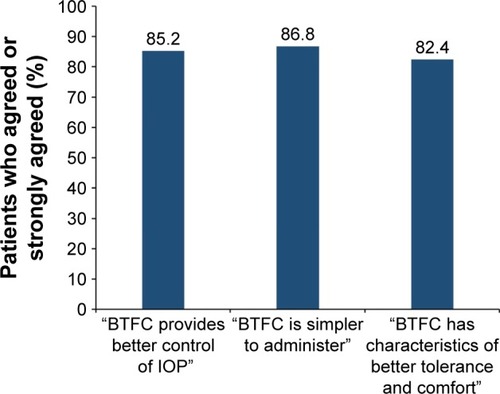
Most patients agreed or very much agreed with statements that BTFC could provide better control of IOP, was simpler to administer, and had characteristics of better tolerance and comfort compared with their previous treatment ().
Figure 1 Percentage of patients who agreed or strongly agreed with statements regarding IOP control, ease of use, and tolerability of BTFC compared with previous treatment.
Discussion
The glaucoma patients in urban China who were surveyed in this study were highly satisfied with BTFC treatment, as shown by their mean satisfaction score of 7.8 for BTFC compared with 6.0 for previous treatment. Most patients (87%) replaced other medication with BTFC, while 13% added BTFC to a preexisting regimen. The most common reasons for switching to or adding BTFC were poor efficacy of the previous treatment and side effects of the previous treatment. This suggests that both efficacy and tolerability are important motivators for changes in glaucoma treatment regimens in China.
In the current study, most patients reported that BTFC provided better control of IOP, had a simpler administration, and was associated with better tolerance and comfort than their previous therapy. Evidence in the literature suggests that efficacy, ease of use, and tolerability were factors that likely contributed to patients’ high level of satisfaction with BTFC.Citation15,Citation22 In a study by Day et alCitation15 in patients with glaucoma or ocular hypertension, patient satisfaction with treatment was significantly correlated with the perceived effectiveness of the medication, the ease and convenience of its use, and lack of side effects (all P<0.001). In a more recent study in patients with glaucoma and ocular hypertension, Kerr et alCitation22 found that satisfaction with the frequency of eye drop use, the convenience of use, and the ease of administration were all predictive of patient satisfaction with topical treatment (all P<0.001).
Switching between topical IOP-lowering medications is common in long-term glaucoma therapy. In this study, switching from other medication to BTFC was associated with greater patient satisfaction than adding BTFC to the preexisting regimen. These results are consistent with a previous study showing that patients with glaucoma or ocular hypertension who were prescribed one medication were more satisfied with treatment than patients who were prescribed multiple medications.Citation15 Minimizing the number of medications used may improve patient satisfaction both by increasing treatment convenience and by reducing ocular exposure to drugs and preservatives, which may improve ocular tolerability. The once-daily dosing schedule used with BTFC is also considered by patients to be more convenient than multiple daily dosesCitation15,Citation22,Citation23 and may be preferred by patients,Citation16 leading to higher patient satisfaction.
The majority of patients (80%) reported using BTFC alone or with a concomitant carbonic anhydrase inhibitor. Unexpectedly, however, approximately 14% of patients reported using BTFC with a concomitant prostaglandin analog or β-blocker. Almost all of these patients were seen at a single hospital in a province in southern China. This finding suggests that current recommended glaucoma treatment strategies are not used consistently throughout China, and there is a need to improve glaucoma therapy and standardize appropriate use of IOP-lowering medications in China.
A limitation of the study is that the survey was read to the patients, and although the investigators were trained to read the questions in an objective manner that would not influence patient responses, it is possible that responses might have differed if the patients had been given a written survey. Another limitation of this study is that patients were required to have used BTFC for a period of 1–3 months. No patients who stopped using BTFC within 1 month after beginning treatment completed the survey. Therefore, a patient selection bias could have affected mean satisfaction scores, if patients who were dissatisfied stopped using BTFC within the first month after treatment initiation. Also, the satisfaction of patients with BTFC after long-term use was not evaluated.
Conclusion
The results of this study demonstrate that glaucoma patients in China were more satisfied with BTFC than with their previous regimen of a β-blocker, prostaglandin analog, carbonic anhydrase inhibitor, α-adrenergic agonist, miotic, or two medications used concomitantly. More than 80% of patients agreed or very much agreed that BTFC was associated with improvements in IOP control, tolerability, and ease of administration compared with their previous treatment. The high levels of patient satisfaction with BTFC compared with previous treatment may lead to improved adherence to therapy, and ultimately, better visual outcomes. Additional studies of patient satisfaction with longer-term use of BTFC are warranted.
Acknowledgments
This study was sponsored by Allergan plc, Dublin, Ireland. Writing and editorial assistance was provided to the authors by Susan Cheer, PhD, Creative Ink Limited, Queenstown, New Zealand, and funded by Allergan plc. All authors met the ICMJE authorship criteria. Neither honoraria nor payments were made for authorship.
Disclosure
The authors have no proprietary interest in this work. Financial arrangements of the authors with companies whose products may be related to the present report are listed below, as declared by the authors. Dr Xinghuai Sun is a consultant or speaker for Alcon, Allergan, Pfizer, and Santen. Dr Mingkai Lin, Dr Xuanchu Duan, and Dr Chun Zhang have no financial arrangements to disclose. Jian Ming is an employee of Allergan plc. The authors report no other conflicts of interest in this work.
References
- SambharaDArefAAGlaucoma management: relative value and place in therapy of available drug treatmentsTher Adv Chronic Dis201451304324381726
- BucoloCPlataniaCBReibaldiMControversies in glaucoma: current medical treatment and drug developmentCurr Pharm Des201521324673468126350532
- DeokuleSSadiqSShahSChronic open angle glaucoma: patient awareness of the nature of the disease, topical medication, compliance and the prevalence of systemic symptomsOphthalmic Physiol Opt200424191514687196
- ReardonGKotakSSchwartzGFObjective assessment of compliance and persistence among patients treated for glaucoma and ocular hypertension: a systematic reviewPatient Prefer Adherence2011544146322003282
- NordmannJPBaudouinCRenardJPMeasurement of treatment compliance using a medical device for glaucoma patients associated with intraocular pressure control: a surveyClin Ophthalmol2010473173920689790
- FriedmanDSQuigleyHAGelbLUsing pharmacy claims data to study adherence to glaucoma medications: methodology and findings of the Glaucoma Adherence and Persistency Study (GAPS)Invest Ophthalmol Vis Sci200748115052505717962457
- KonstasAGMaskalerisGGratsonidisSSardelliCCompliance and viewpoint of glaucoma patients in GreeceEye200014Pt 575275611116698
- SleathBBlalockSCovertDThe relationship between glaucoma medication adherence, eye drop technique, and visual field defect severityOphthalmology2011118122398240221856009
- PatelSCSpaethGLCompliance in patients prescribed eyedrops for glaucomaOphthalmic Surg19952632332367651690
- OlthoffCMSchoutenJSvan de BorneBWWebersCANoncompliance with ocular hypotensive treatment in patients with glaucoma or ocular hypertension an evidence-based reviewOphthalmology2005112695396115885795
- SchwartzGFHollanderDAWilliamsJMEvaluation of eye drop administration technique in patients with glaucoma or ocular hypertensionCurr Med Res Opin201329111515152224006861
- DreerLEGirkinCACampbellLWoodAGaoLOwsleyCGlaucoma medication adherence among African Americans: program developmentOptom Vis Sci201390888389723873033
- BaudouinCRenardJPNordmannJPPrevalence and risk factors for ocular surface disease among patients treated over the long term for glaucoma or ocular hypertensionEur J Ophthalmol20132314754
- Garcia-FeijooJSampaolesiJRA multicenter evaluation of ocular surface disease prevalence in patients with glaucomaClin Ophthalmol2012644144622536034
- DayDGSharpeEDAtkinsonMJStewartJAStewartWCThe clinical validity of the treatment satisfaction survey for intraocular pressure in ocular hypertensive and glaucoma patientsEye200620558359015933751
- StewartWCKonstasAGPfeifferNPatient and ophthalmologist attitudes concerning compliance and dosing in glaucoma treatmentJ Ocul Pharmacol Ther200420646146915684806
- HigginbothamEJConsiderations in glaucoma therapy: fixed combinations versus their component medicationsClin Ophthalmol201041920169043
- LewisRAGrossRLSallKNSchiffmanRMLiuCCBatoosinghALfor the Ganfort Investigators Group IIThe safety and efficacy of bimatoprost/timolol fixed combination: a 1-year double-masked, randomized parallel comparison to its individual components in patients with glaucoma or ocular hypertensionJ Glaucoma201019642442619855289
- LingZZhangMHuYSafety and efficacy of bimatoprost/timolol fixed combination in Chinese patients with open-angle glaucoma or ocular hypertensionChin Med J (Engl)2014127590591024571886
- LouHWangHZongYChengJWWeiRLEfficacy and tolerability of prostaglandin-timolol fixed combinations: an updated systematic review and meta-analysisCurr Med Res Opin20153161139114725867658
- FangYLingZSunXFixed-combination treatments for intraocular hypertension in Chinese patients – focus on bimatoprost-timololDrug Des Devel Ther2015926172625
- KerrNMPatelHYChewSSAliNQEadyEKDanesh-MeyerHVPatient satisfaction with topical ocular hypotensivesClin Experiment Ophthalmol2013411273522594958
- BullerAJMorganLHHerculesBLPatients prefer once-daily glaucoma dropsGraefes Arch Clin Exp Ophthalmol2007245229329416636837