
Abstract
Objective
The objective of this study was to compare the differences in the five-level EuroQol-5 dimensions (EQ-5D-5L) health state utility scores derived from Chinese, Japanese, Korean, and UK tariffs.
Methods
Six hundred and twenty-one breast cancer patients were invited for a face-to-face interview in Qingdao Municipal Hospital, China. EQ-5D-5L was scored using tariffs from China, Japan, Korea, and the UK. The null hypothesis of normal distribution of the EQ-5D-5L utility score was tested by the Shapiro–Wilk test. Nonparametric Friedman test and Wilcoxon signed-rank test were used to determine the difference among the four tariffs. The intraclass correlation coefficients (ICCs) and Bland–Altman plots were used to study the agreement among the four EQ-5D-5L scores. Known-groups validity was studied using a regression framework.
Results
There were 608 participants in the final analysis, with a mean ± standard deviation (SD) age of 48.0±9.6 years. EQ-5D-5L utility scores were non-normally distributed. The means (median) ± SD of EQ-5D-5L utilities derived from Chinese, Japanese, Korean, and UK tariffs were 0.828 (0.879) ±0.184, 0.802 (0.823) ±0.164, 0.831 (0.829) ±0.137, and 0.838 (0.866) ±0.154, respectively. Among pairwise comparisons, the difference of median EQ-5D-5L utility scores was only insignificant between Chinese and UK tariffs. Excellent agreements (with ICCs >0.9) were found among the four tariffs albeit the limits of agreement between each pair of tariffs were wide. Known-groups validity was supported.
Conclusion
Although four country-specific EQ-5D-5L tariffs have shown an overall high level of correlation and agreement, none of them could be regarded as interchangeable. The higher correlation and agreement between Chinese and UK tariffs may be due to the similar functions that were used in the tariff development. In the absence of Chinese-specific tariff, the UK tariff is the second-best option to be applied in the Chinese population. Results of this study further contribute to the explanation of variations among country-specific tariffs.
Introduction
Given the limited health resources, cost–utility analysis (CUA) becomes increasingly important for decision makers to compare the effects of alternative health care interventions.Citation1,Citation2 The most common effectiveness measure in CUA is quality-adjusted life years (QALYs), expressed as health outcome in time (life years) combined with quality adjustments, that is, health state utility (HSU).Citation3 HSU values range on a 0–1 (dead–full health) QALY scale; negative utilities also exist, representing health states are worse than death.Citation4 The HSU scores can be elicited using both direct and indirect methods.Citation5 The direct approach mainly includes the visual analog scale, time trade-off (TTO), and standard gamble. The indirect approach refers to the use of multi-attribute utility (MAU) instruments, such as the EuroQol-5 dimensions (EQ-5D) instruments,Citation6 the short-form (SF) six dimensions derived from the SF-36,Citation7 and the Health Utilities Index.Citation8
The three-level version of EQ-5D (EQ-5D-3L) was introduced in the 1990s and has become the most widely used generic MAU instrument internationally.Citation9,Citation10 EQ-5D-3L includes five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, with three levels in each dimension: no problems, some problems, and extreme problems. Although widely used in clinical trials, the EQ5D-3L instrument is not without limitations; for example, it is not sensitive to mild health changes and it suffers from ceiling effects.Citation11,Citation12 To solve the issues previously mentioned, a new five-level EQ-5D (EQ-5D-5L) instrument was developed by the EuroQol Group.Citation13 It retains the original dimension and expands the number of levels of severity in each dimension from three to five. The five levels in EQ-5D-5L include “no problems,” “slight problems,” “moderate problems,” and “severe problems” for all five items, and “unable to do” for mobility, self-care, and usual activities, or “extreme problems” for pain/discomfort and anxiety/depression, resulting in 3,125 (=5Citation5) unique health states.Citation13,Citation14
The MAU instrument contains two components, a descriptive system of the instrument and a tariff (also called “value sets,” “preference weights,” or “scoring algorithm”). It is commonly suggested that country-specific tariff better reflects the preference of a population in each country. When country-specific tariffs were unavailable, researchers opted to use the UK tariffCitation9,Citation15 or the tariff derived from a country that was geographically or culturally closer. However, previous studies suggest that there are substantial differences in different countries’ preference values for health states.Citation16,Citation17 It is unclear whether country-specific tariffs have high agreements or not for the new EQ-5D-5L instrument. This study aimed to empirically compare EQ-5D-5L HSU scores derived from Chinese, Japanese, Korean, and UK tariffs,Citation15,Citation18–Citation20 based on a breast cancer patient sample in mainland China. Breast cancer is currently the most common cancer in Chinese women.Citation21 By 2008, cases in China accounted for 12.2% of all newly diagnosed breast cancers and 9.6% of all deaths from breast cancer worldwide.Citation22 A prediction suggested that in 2015, breast cancer accounted for 15% of all new cancers in women in China.Citation21 To the best of our knowledge, this is the first study using the EQ-5D-5L Chinese value set in patients. The results of this study further contribute to the explanation of variations among country-specific tariffs.
Methods
Study sample
Participants were breast cancer patients who underwent inpatient treatment in Qingdao Municipal Hospital, China, between October 2014 and February 2015. Patients were excluded if they were unwilling to provide informed consent, or unable to understand the questionnaires, or diagnosed with other serious diseases, such as cardiovascular or cerebrovascular diseases, psychosis, or if the patient was <18 years at the time of the survey. All participants included were invited to a face-to-face interview, 1 day prior to discharge.
The face-to-face interviews included questions on socio-demographic characteristics and self-assessed quality of life. Clinical information for each participant was collected by the interviewer based on the medical record. Ethical approval (reference no 20131002) was obtained from the Ethics Review Board of the School of Public Health, Shandong University, and the research adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from all participants after a detailed explanation of the study.
EQ-5D-5L: China, Japan, Korea, and UK preference weights
In the Chinese valuation study,Citation20 86 health states were valued by composite TTO (cTTO). To generate the tariff, the eight-parameter multiplicative model, including coefficients of the five dimensions (βMO, βSC, βUA, βPD, βAD) and parameters for levels 2, 3, and 4 (L2, L3, and L4), was chosen as the best model with random intercept variants.
The UK preference valuation for 86 health states was selected using cTTO and 196 pairs of health states using discrete choice experiments (DCE). A single combined-data value function for EQ-5D-5L, including 20 parameters (4 levels × 5 dimension), was developed by using the three-group model, the least restrictive model, and a hybrid modeling approach.Citation15
In the Korean preference study,Citation18 cTTO and DCE were used to estimate tariff for EQ-5D-5L health states. Because of being logically inconsistent, the final valuation model only used TTO data, which estimated 86 health state values for all EQ-5D-5L health states. The N4 model was selected as the final preferred model. The model included basic indicator variables with N4, which was added to the model to indicate if any of the five health dimensions contains a level ≥4.
The Japanese valuation studyCitation19 elicited 86 health states, which were valued by cTTO. The linear mixed model was adopted to predict all health states of EQ-5D-5L. The specific coefficients, functional model derived from four national preference weights, are shown in .
Table 1 Chinese, Japanese, Korean, and UK tariffs for EQ-5D-5L utilities calculation
Statistical analysis
EQ-5D-5L utility scores were calculated using the Chinese, Japanese, Korean, and UK tariffs. The null hypothesis of normal distribution of the EQ-5D-5L utility score was tested by the Shapiro–Wilk test. The nonparametric Friedman test and Wilcoxon signed-rank test were applied to examine the differences among the four HSU scores when the HSU scores were not normally distributed. Intraclass correlation coefficients (ICCs)Citation23 and Bland–Altman plotsCitation24 were adopted to assess the agreements. An agreement was considered strong if the ICC value was >0.70.Citation23 Known-groups validity was studied under a regression framework. It is hypothesized that breast cancer patients at a more advanced stage according to the tumor, node, and metastases classification of malignant tumors (TNM) or patients with metastatic breast cancer will have a significantly lower mean EQ-5D-5L utility score. Owing to a large proportion of patients were classified as in full health with HSU =1 according to the EQ-5D-5L classification system, a Tobit model was used in the regression analysis instead of the classical ordinary least squares estimator.Citation25 Regressions controlled for patients’ sociodemographic characteristics. With the exception of the Bland–Altman plot, which was drawn using MedCalc version 16.8 (MedCalc Software, Ostend, Belgium), all other statistical analyses were conducted using Stata 14.0 (StataCorp LP, College Station, TX, USA).
Results
Characteristics of participants
Six hundred and twenty-one patients who were diagnosed with breast cancer were interviewed in this study. Among them, 13 participants were excluded due to incomplete answers to key questions. The final sample included 608 patients (97.9%).
Socio-demographic and clinical characteristics of the sample are shown in . The mean age of participants was 48.0 years (standard deviation [SD]: 9.6; range: 24–90), and 32.9% were either illiterate or completed only primary school education. The majority (88.7%) of participants were married, ~65% were urban employees, and 50.8% lived in the city. The mean ± SD duration of breast cancer was 38.2±40.9 months (range: 1–242 months). Also, ~48% of respondents were classified as TNM stage III and IV, and 23% breast cancers were metastatic.
Table 2 Socio-demographic and clinical characteristics of breast cancer patients (n=608)
Comparison of health state utilities among four national tariffs
The mean (median) of EQ-5D-5L utility scores using the Chinese, Japanese, Korean, and UK preference weights was 0.828 (0.879), 0.802 (0.823), 0.831 (0.829), and 0.838 (0.866), respectively. Shapiro–Wilk test statistics suggested that regardless of the tariff used, the null hypothesis of normal distribution of EQ-5D-5L utility scores was rejected (P<0.001) (). In all, ~28.6% breast cancer patients were classified to be in full health with EQ-5D-5L utility score of 1. Differences of EQ-5D-5L utilities derived from the four national tariffs were significantly different according to the Friedman test (χ2=438.952, P<0.001) (). Wilcoxon signed-rank tests were adopted in respective pairwise comparison of the four national EQ-5D-5L utility scores. The results showed that differences of median EQ-5D-5L utility scores were insignificant when scored using Chinese and UK tariffs (P>0.05) ().
Figure 1 Distribution of EQ-5D-5L scores from four tariffs among breast cancer patients.
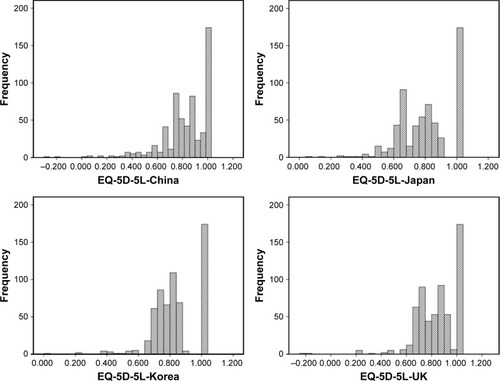
Table 3 EQ-5D-5L utility scores derived from Chinese, Japanese, Korean, and UK tariffs
Table 4 Equality and agreement tests of EQ-5D-5L utility scores derived from four national tariffs
Agreement
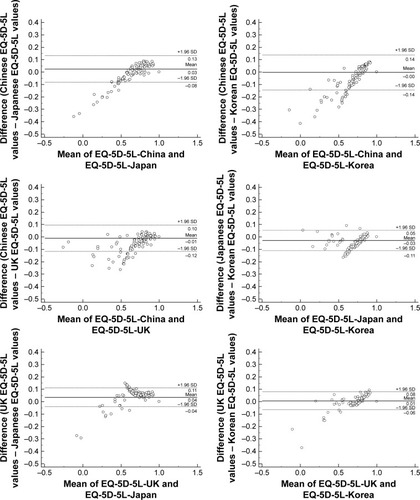
The overall ICC was 0.984 (95% CI: 0.979–0.988), which indicates excellent agreement among the four national tariffs. The ICC values for pairwise comparisons ranged from 0.948 (between Chinese and Korean tariffs) to 0.984 (between Korean and UK tariffs) (). The Bland–Altman plots of each pair of the four EQ-5D-5L tariffs are presented in . The mean of the utility differences and the limits of agreement are indicated by lines. As shown, the 95% limits of agreement among six pairs of comparison ranged from 0.14 to 0.28.
Figure 2 Bland–Altman plots of EQ-5D-5L values derived from four national tariffs.
Known-groups validity
presents the Tobit model estimates for dummy variables of advanced TNM stages (panel A) and metastatic breast cancer (panel B). In panel A, as expected, breast cancer patients in TNM stages III/IV had significantly lower HSU (ranged from −0.032 to −0.040) regardless of which tariff was used (all P<0.05). Similarly, in panel B, metastatic breast cancer patients had significantly lower HSU (ranged from −0.045 to −0.067) (all P<0.05). In both panels, the magnitudes of absolute value of coefficients were the largest for Chinese tariff and the smallest for Korean tariff.
Table 5 Known-groups validity of four EQ-5D-5L national tariffs
Discussion
This study compared the Chinese EQ-5D-5L tariff against Japanese, Korean, and UK tariffs in a Chinese breast cancer patient sample. To our knowledge, this is the first study to apply Chinese EQ-5D-5L tariff in patients and examine the differences among the four country-specific tariffs in breast cancer patients.
The results firstly showed that the mean of the HSU score was the highest using the UK tariff, followed by Korean, Chinese, and Japanese tariffs. This finding differs from a previous study, based on the Chinese general population, using the EQ-5D-3L instrument (in which the HSU score was the highest using the Korean tariff, followed by Chinese, Japanese, and UK tariffs).Citation26
Secondly, this study indicated excellent agreement among Chinese, Japanese, Korean, and UK EQ-5D-5L tariffs, with all ICCs >0.9. The finding is consistent with previous studies which adopted the EQ-5D-3L instrument and corresponding value sets. For example, a study based on the Chinese general population showed that the EQ-5D-3L utility scores derived using Chinese, Japanese, Korean, and UK tariffs have excellent agreement (ICC >0.75).Citation26 In another study, the agreement between UK and Japanese tariffs was very high among Thai diabetes patients.Citation27 Although, in general, good agreements have been reported among different country-specific tariffs, the 95% limits of agreement (0.14) from the Bland–Altman plots were still much wider than the minimally important difference (MID) of ~0.074, based on EQ-5D-3L,Citation28 and also wider than the MID of ~0.069, based on the Chinese EQ-5D-5L tariff.Citation29 This suggests that none of the four tariffs could be regarded as interchangeable.
Thirdly, it is found that the difference in median EQ-5D-5L utility scores was insignificant when scored using Chinese and UK tariffs. This may be because Chinese and UK tariffs were derived using similar function forms (in which 20 parameters were estimated). On the other hand, the estimated function forms of the Japanese and Korean tariffs were relatively similar, which additionally included a constant. The Korean tariff further included an N4 dummy variable which equals 1 if any of the five health dimensions contains level 4 or above, 0 otherwise.Citation15,Citation18–Citation20
In an ideal scenario, the country-specific tariff should be adopted in conducting CUA.Citation30 However, in practice, the country-specific tariff is not always available, and in such scenarios, tariffs derived from other countries can be adopted. Literature indicates that different cultures could influence the derived utility scores.Citation31,Citation32 Previous studies regarding the EQ-5D-3L instrument and its tariffs showed that it would be better to choose tariffs with similar cultural backgrounds.Citation26,Citation27,Citation33 Our study supports previous findings about the excellent agreement on different country-specific tariffs, as well as the good known-groups validity in all four tariffs. However, the results from this study also highlight that these tariffs are not interchangeable.
There were three limitations in this study. First, the study was based on a patient sample with breast cancer; so, these results cannot be generalized to other patient populations. Second, the study was carried out in China, and the conclusion may not be generalized to other countries. Third, this is a cross-sectional study; so, we cannot assess test–retest reliability and the responsiveness to change among different country-specific tariffs.
In conclusion, there are excellent agreements among EQ-5D-5L HSU scores derived from Chinese, Japanese, Korean, and UK tariffs in breast cancer patients. However, none of them could be regarded as interchangeable. We recommend that the Chinese tariff be chosen, based on breast cancer patients in mainland China. In the absence of Chinese-specific tariff, the UK tariff is the second-best option to be applied in a Chinese population. The results of this study further contribute to the explanation of variations among country-specific tariffs.
Acknowledgments
The authors thank all the participants for their time and effort. Responsibility of any remaining errors lies solely with the authors. Financial support was provided by the Shandong Provincial Natural Science Foundation, China (ZR2013GM023).
Disclosure
The authors report no conflicts of interest in this work.
References
- EarnshawJLewisGNICE guide to the methods of technology appraisalPharmacoEconomics200826972572718767892
- GoldMRussellLSiegelJWeinsteinMCost-Effectiveness in Health and MedicineNew YorkOxford University Press1996
- DrummondMSculpherMTorranceGO’BrienBStoddartGMethods for the Economic Evaluation of Health Care Programmes3rd edNew YorkOxford University Press2005
- TorranceGWMeasurement of health state utilities for economic appraisalJ Health Econ19865113010311607
- BrazierJRatcliffeJSalomonJTsuchiyaAMeasuring and Valuing Health Benefits for Economic EvaluationNew YorkOxford University Press2007
- BrooksREuroQol: the current state of playHealth Policy1996371537210158943
- BrazierJRobertsJDeverillMThe estimation of a preference-based measure of health from the SF-36J Health Econ200221227129211939242
- FeenyDFurlongWTorranceGWMultiattribute and single-attribute utility functions for the health utilities index mark 3 systemMed Care200240211312811802084
- DolanPModeling valuations for EuroQol health statesMed Care19973511109511089366889
- KindPBrooksRRabinREQ-5D Concepts and Methods: A Developmental HistoryThe NetherlandsSpringer2005
- ZhouTGuanHMaALiuGComparison between the EQ-5D-5l and the EQ-5D-3l for general population in ChinaChinese Health Econ20163531720
- AgborsangayaCBLahtinenMCookeTJohnsonJAComparing the EQ-5D 3L and 5L: measurement properties and association with chronic conditions and multimorbidity in the general populationHealth Qual Life Outcomes20141211724382363
- HerdmanMCGudexCLloydADevelopment and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L)Qual Life Res201120101727173621479777
- LuoNLiMLiuGGLloydAde CharroFHerdmanMDeveloping the Chinese version of the new 5-level EQ-5D descriptive system: the response scaling approachQual Life Res201322488589022622627
- DevlinNShahKFengYMulhernBVan HoutBValuing health-related quality of life: an EQ-5D-5L value set for England2016 Available from: https://www.ohe.org/publications/valuing-health-related-quality-life-eq-5d-5l-value-set-englandAccessed November 18, 2016
- BadiaXRosetMHerdmanMKindPA comparison of United Kingdom and Spanish general population time trade-off values for EQ-5D health statesMed Decis Making200121171611206949
- LuoNJohnsonJAShawJWCoonsSJA comparison of EQ-5D index scores derived from the US and UK population-based scoring functionsMed Decis Making200727332132617545501
- KimSHAhnJOckMThe EQ-5D-5L valuation study in KoreaQual Life Res20162571845185226961008
- IkedaSShiroiwaTIgarashiADeveloping a Japanese version of the EQ-5D-5L value setJ Natl Inst Public Health20156414755
- LuoNLiuGLiMGuanHJinXRand-HendriksenKEstimating an EQ-5D-5L value set for ChinaValue Health201720466266928408009
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211526808342
- FanLStrasser-WeipplKLiJJBreast cancer in ChinaLancet Oncol2014157279289
- FayersPMachinDQuality of Life: The Assessment, Analysis and Interpretation of Patient-Reported OutcomesWiley, Chichester, UK2013
- BlandJMAltmanDGStatistical methods for assessing agreement between two methods of clinical measurementLancet1986184769319362871239
- ZhouZFangYZhouZAssessing income-related health inequality and horizontal inequity in ChinaSoc Indic Res20171321241256
- WuCGongYWuJChinese version of the EQ-5D preference weights: applicability in a Chinese general populationPLoS One20161110e016433427711169
- SakthongPCharoenvisuthiwongsRShabunthomRA comparison of EQ-5D index scores using the UK, US, and Japan preference weights in a Thai sample with type 2 diabetesHealth Qual Life Outcomes2008611918179687
- BrazierJEComparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6DQual Life Res20051461523153216110932
- McClureNSSayahFAXieFLuoNJohnsonJAInstrument-defined estimates of the minimally important difference for EQ-5D-5L index scoresValue Health201720464465028408007
- GalanteJAugustovskiFColantonioLEstimation and comparison of EQ-5D health states’ utility weights for pneumococcal and human papillomavirus diseases in Argentina, Chile, and the United KingdomValue Health2011145 Suppl 1S60S6421839901
- BaileyHKindPPreliminary findings of an investigation into the relationship between national culture and EQ-5D value setsQual Life Res20101981145115420496167
- KniesSEversSMCandelMJSeverensJLAmentAJUtilities of the EQ-5D: transferable or not?Pharmacoeconomics200927976777919757870
- WuYQLiuKTangXEmpirical research of measuring elderly health utility in the outskirts of Beijing by using European quality of life 5-dimensionsBeijing Da Xue Xue Bao2012443397 Chinese22692310