
Abstract
Background
Computed tomography enterography (CTE) and double-balloon enteroscopy (DBE) are widely used in diagnosis of small bowel diseases. Both of these examinations bring discomfort to patients. The aim of this study was to compare patients’ tolerance and preference between CTE and DBE.
Methods
From August 1, 2014 to December 31, 2016, patients with suspected or known small bowel diseases who underwent both CTE and DBE were prospectively enrolled in our study. They were asked to fill out a questionnaire evaluating discomfort of the procedure after each examination.
Results
One hundred and seven patients completed our study. Abdominal distension, painfulness, tenesmus, general discomfort, prolonged duration, difficulty in completing the test, and discomfort after the examination were significantly lower with CTE than with DBE (P<0.001, respectively). Mannitol intake (47.7%), bowel preparation (31.9%), and radiation exposure (15.0%) were regarded as the three most intolerable burdens in CTE. Painfulness (38.3%), bowel preparation (26.2%), and invasiveness (16.8%) were considered as the three most unacceptable parts of DBE. More patients (61.7%) preferred to repeat CTE rather than DBE (P<0.001).
Conclusion
Compared to DBE, CTE was a more tolerable and less burdensome examination and enjoyed higher preference by most patients.
Introduction
Study of the small bowel is considered difficult due to its length, special anatomy, and location, thus the diagnosis and management of patients with suspected small bowel diseases are quite challenging for gastroenterologists. With the rapid development of endoscopic techniques and radiologic approaches, there are multiple new diagnostic tools available for doctors to better evaluate the small bowel, among which include computed tomography enterography (CTE) and double-balloon enteroscopy (DBE).Citation1–Citation4
CTE is a recently introduced technique for small intestine disorders. Patients who undergo CTE ingest a certain amount of neutral contrast agents before the procedure, which enables luminal distention and allows a better view of the entire small bowel.Citation5,Citation6 Moreover, besides its noninvasiveness, fast collecting and image reconstructing, CTE provides the visualization of the whole abdomen including the extraintestinal lesions. The main limitations of CTE are radiation exposure and inability of biopsy.Citation7–Citation9
DBE, which was developed by Yamamoto et al,Citation10 provides us a clearer and more direct visualization of the small intestine. Moreover, biopsy and treatment such as hemostasis, polypectomy, and dilation are possible during DBE. However, invasiveness, prolonged time duration, difficulty in completing the whole small bowel examination, and additional need for an assistant are the main disadvantages of DBE.Citation7,Citation8,Citation11,Citation12
Both CTE and DBE could bring discomfort to patients during the procedure.Citation13,Citation14 Therefore, patients’ acceptance and tolerance should be taken into account when doctors choose the diagnostic tools, especially for those individuals suffering from chronic diseases such as inflammatory bowel disease (IBD) who need repeated examinations during their follow-ups.Citation13,Citation15 Up to now, some studies have been raised to compare the diagnostic yield between CTE and DBE.Citation7,Citation16 However, as far as we know, there is no study comparing patients’ acceptance between these two procedures. This study was aimed to assess patients’ tolerance and preference between CTE and DBE.
Methods
Patients
From August 1, 2014, to December 31, 2016, patients with suspected or known small bowel diseases who underwent both CTE and DBE (via anal) examinations were prospectively enrolled in our study in Ruijin Hospital. Exclusion criteria included allergies to contrast media (previous adverse events during iodinated contrast media injection), severe small bowel stricture or obstruction, recent use of antiplatelet or anticoagulant drugs, pregnancy or breast-feeding, electrolyte disturbance, inability to understand or finish the questionnaires independently, other serious diseases.
This study was approved by the ethics committee of Ruijin Hospital affiliated to School of Medicine Shanghai Jiao Tong University, and written informed consent was signed by each patient or parent or legal guardian (for patients <18 years old).
Methods
All patients first underwent CTE examination and then DBE examination via anal. The time interval between CTE and DBE was restricted to less than 2 months. Patients were asked to fill in a questionnaire 1 week after each examination.
CTE procedure
Bowel cleansing was performed with a single dose of 2 L PEG electrolytes powder on the day before the examination. Patients were asked to drink 2,000 mL 2.5% iso-osmotic mannitol solution approximately 45 minutes before the examination in order to obtain optimal small bowel distension. Before the examination, 20 mg of anisodamine was administered intramuscularly to reduce bowel peristalsis. CTE scan was performed on a 64-slice multi-slice multi-detector computed tomography scanner (GE Medical Systems, Milwaukee, WI, USA) from the porta hepatis to pubic symphysis. After plain computed tomography (CT) scanning, patients were injected with nonionic contrasts (Ioversol, Optiray 320; Tyco Healthcare, Montreal, Canada) via the antecubital vein at a rate of 3 to 4 mL/sec and a total of 90 to 120 mL (1.5 mL/kg of body weight). Then arterial phase and portal venous phase imaging was performed. Images were reconstructed using the workstation (ADW4.2 and ADW4.4).
DBE procedure
After bowel preparation with PEG electrolytes powder (the same regimen as used in CTE) and 20 mg injection of anisodamine, DBE was performed using a video endoscope (Fujinon EN-450P5/20; FujinonInc., Saitama, Japan) with a working length of 200 cm and an overtube of 145 cm in length, both of which have balloons at their distal ends. All the DBE examinations were performed by the same endoscopist via the anal approach with conscious sedation (injection of 10 mg diazepam intramuscularly before the procedure). The indication to stop insertion was discovery of the lesion or difficulty in further advancing.
Questionnaires
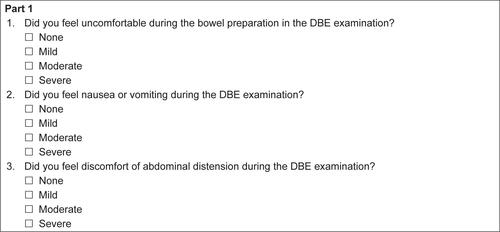
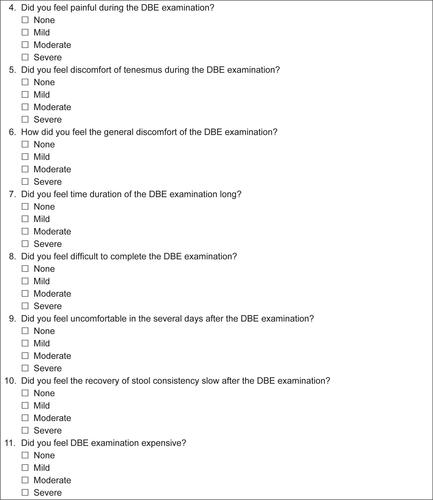
One week after CTE, the patients were asked to complete the first questionnaire () composed of two parts. The first part included eleven questions assessing patients’ acceptance of CTE, including discomfort of the bowel preparation, nausea and vomiting during the test, abdominal distension during the examination, pain during the procedure, tenesmus during the test, discomfort of the entire examination, time duration of the entire procedure, difficulty in completing the test, discomfort several days after the examination, time until stool consistency recovery, and cost of the test. Each question used a 4-point scale. For example, “Did you feel uncomfortable during the bowel preparation in the CTE examination?”: 1 (none), 2 (mild), 3 (moderate), 4 (severe). The second part was a question to patients to list the three most unacceptable burdens of CTE. The six selectable options were discomfort of the bowel preparation, ingesting large amount of mannitol, radiation exposure, prolonged time duration of the test, high cost, and slow recovery of bowel function after the exam.
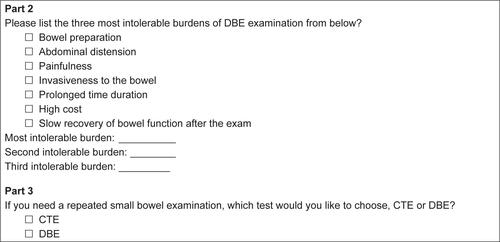
One week after DBE, the patients were asked to fill in another questionnaire (), which consisted of three parts. The first part was the same eleven questions evaluating the individual’s tolerance of the test as used after CTE. The second part asked the patients to list the three most intolerable burdens of DBE. The seven selectable options were discomfort of the bowel preparation, abdominal distension during the procedure, painfulness during the test, invasiveness to the bowel, prolonged duration of the test, high cost, and slow recovery of bowel function after the exam. The third part was a direct question concerning the preference of CTE or DBE (“If you need a repeated small bowel examination, which test would you like to choose, CTE or DBE?”).
Statistical analysis
Student’s t-test was used for comparison of the tolerability between CTE and DBE. The results were considered significant at P<0.05. The reasons of non-acceptance of CTE and DBE are briefly described using frequencies and percentages. Data analysis was conducted using SPSS 21.0 (IBM Corporation, Armonk, NY, USA).
Results
During our research, 115 patients underwent both CTE and DBE examinations in our hospital. Among them, six patients refused to answer our questionnaires and another two patients did not fill out the questionnaires completely. Finally, 107 patients completed our study, whose demographic and disease-related characteristics are summarized in .
Table 1 Demographic and disease-related characteristics
The scores of the eleven evaluated items about burdens of CTE and DBE are described in . The average score of each item and comparison between the two procedures are shown in . For abdominal distension, painfulness, tenesmus, general discomfort, prolonged time duration, difficulty in completing the test and discomfort after the examination, patients reported DBE more burdensome than CTE (P<0.001, respectively). However, regarding other items including bowel preparation, nausea and vomiting, time until stool consistency recovery and cost of the test, patients reported similar acceptance (P>0.05, respectively).
Figure 1 Tolerability of the eleven evaluated burdens of CTE and DBE on a 4-point scale.
Abbreviations: CTE, computed tomography enterography; DBE, double-balloon enteroscopy.
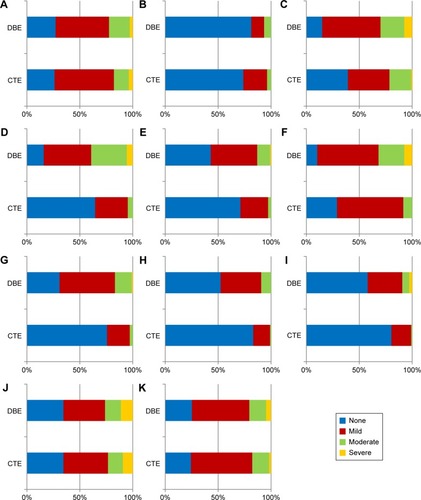
Table 2 Comparison of patients’ tolerance between CTE and DBE
Patients’ feedback on why they did not like CTE is shown in . It was shown that the most intolerable burden of CTE reported was mannitol intake (47.7%). The next important reason was discomfort of the bowel preparation (31.9%), and the third important item was radiation exposure (15.0%). High cost (3.7%), prolonged time duration of the test (0.9%), and slow recovery of bowel function after the exam (0.9%) were ranked the fourth to sixth items in reported importance. Feedback on why patients did not like DBE is shown in , pain during the test (38.3%) was considered as the most burdensome by the majority of patients. The second most unacceptable item was discomfort of the bowel preparation (26.2%). Invasiveness to the bowel (16.8%) was the third most important reason responsible for intolerability of DBE, while abdominal distension during the procedure (11.2%) was ranked fourth. Furthermore, the fifth to seventh in reported importance were high cost (5.6%), prolonged time duration of the test (0.9%), and slow recovery of bowel function after the exam (0.9%).
Table 3 Rating of the importance of different burdens of CTE examination
Table 4 Rating of the importance of different burdens of DBE examination
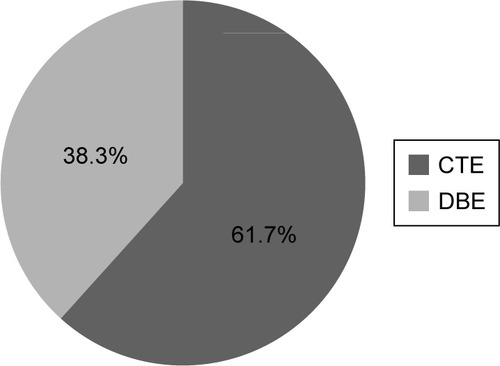
As shown in , 66 (61.7%) patients preferred CTE if a repeated small bowel examination was needed, as compared to 41 (38.3%) patients who preferred DBE (P<0.001).
Figure 2 Proportions of patients’ preference for CTE or DBE.
Discussion
When comparing different small bowel imaging techniques, most of the previous researches focused on their diagnostic efficacy.Citation7,Citation17–Citation19 However, patients’ tolerance of each procedure should also be taken into consideration, especially when repeated examinations are needed, as tolerance and acceptance of a certain examination may impact their choice and adherence to later follow-ups.Citation20
To our knowledge, this is the first study to directly compare CTE and DBE in terms of patient burden and tolerance. Our study showed most patients who had experienced both examinations preferred CTE rather than DBE. Patients considered DBE significantly more burdensome than CTE in terms of abdominal distension, painfulness, tenesmus, general discomfort, prolonged time duration, difficulty in completing the test, and discomfort after the examination.
In a previous study of comparison among DBE, capsule endoscopy (CE), and magnetic resonance (MR) enteroclysis, the results showed CE was significantly favored over the other two procedures in terms of bowel preparation, entire discomfort during the examination, time duration, and swallowing the capsule (compared to insertion of the tube/scope).Citation15 MR enteroclysis was preferred to DBE with respect to bowel preparation, painfulness, and burden of the entire examination while DBE was more tolerable than MR enteroclysis for insertion of the scope and procedure duration. In our study, most of the patients complained about bowel preparation, painfulness, and general discomfort during the DBE procedure. Besides, they found DBE a quite time-consuming examination which was difficult to accomplish. Previous researchCitation15 also suggested that CE and MR enteroclysis provided clearer pre-exam explanation of the modality than DBE, which probably could be explained by the fact that DBE is more unpredictable in advance. In their study, patients considered CE as the most preferable, followed by MR enteroclysis as the second, and DBE as the last. Our research got a similar result – fewer patients would be willing to repeat DBE rather than CTE.
Research of tolerance between other small bowel diagnostic techniques is also lacking. One study compared MR enterography (MRE) and MR enteroclysis. Patients ingested the contrast material either orally or through a nasogastric catheter. Abdominal pain and discomfort were reported to be lower with MRE than with MR enteroclysis, and more patients found it acceptable to repeat MRE.Citation21 Another study compared MRE with CE, indicating that CE was less burdensome in pre-exam discomfort, during-exam discomfort, nausea, vomiting, bloating, and abdominal pain.Citation13 They also found MRE was associated with a specific adverse event – claustrophobia. Consequently, CE was a better tolerated and more preferable test than MRE.
A systematic review and meta-analysis of preference for colonoscopy versus computerized tomographic colonography (CTC) showed colonoscopy was graded more uncomfortable by patients and CTC was preferred over colonoscopy in most of the studies.Citation22 Similar to CTC, MR colonography was also more tolerable than colonoscopy.Citation23 Patients in our study experienced less burden from CTE examination compared to DBE examination and regarded CTE as a more favorable procedure. It seems that imaging examinations have a higher acceptance than endoscopic modalities regardless of small bowel examination or colon disease screening.Citation24,Citation25
In the present study, we found patients’ main dissatisfactions about CTE were ingestion of a large amount of oral contrast agent, bowel preparation, and radiation exposure. Previous research evaluating tolerance of oral contrast agents with different quantity and osmolarity in CTE test indicated patients preferred the ingestion of 1,000 mL solution to the 1,500 mL solution, while no statistically significant differences in mean small bowel diameter were seen between both contrast agents.Citation26 For this reason, a lower quantity of solution ingestion should be considered to raise patients’ tolerance if similar small bowel distension could be achieved. Patients using sodium picosulfate with magnesium citrate (SPMC) for bowel preparation were less likely to have abdominal fullness, pain, nausea or vomiting, and reported SPMC to be more palatable compared to PEG, while no difference was shown among the two groups with respect to bowel cleansing grade (Ottwa Scale).Citation27 In our study, all the patients used PEG for bowel preparation. In the future, we may try other types of bowel preparation to help reduce patients’ burden in small bowel diagnostic examinations. It was reported that many IBD patients received high-dose radiation exposure with cumulative effective dose >50 mSv.Citation28–Citation32 About half of the participants in our cohort were Crohn’s disease patients and may need small bowel examination again in the future. MRE and trans-abdominal ultrasonography (US) would be alternative radiation-free imaging strategies, due to their equivalent diagnostic accuracy, better tolerance, and cost effectiveness.Citation33–Citation38
As for DBE, patients’ major complaints were painfulness, bowel preparation, and invasiveness. Since, occasionally, position changes were needed during the DBE procedure for smoother intubation, patients in our study were all provided with conscious sedation rather than general anesthesia. Nevertheless, painfulness still remained challenging for most of our patients. Therefore, general anesthesia could be taken into account in our future DBE examinations to reduce painfulness.Citation39–Citation44 It is inevitable that DBE examinations are invasive, which some of our patients found unacceptable. CE is a potential alternative because of its noninvasive quality and better tolerance, while having a comparable diagnostic yield with DBE in small bowel diseases.Citation18 But risk of capsule retention should be taken into account.Citation45,Citation46
There are several limitations to our study. First, we did not include CE in our research, which is considered as a small bowel examination with good tolerance and preference.Citation13,Citation15 This is because CE is an examination of high cost in our country and not covered by Chinese medical insurance. In further studies, we can add CE and other modalities such as MRE and US into comparison. Second, we needed the results of CTE examination to decide which patients were suitable for via anal DBE examinations. So, the order of CTE and DBE in our study was fixed, which might have had an effect on patients’ acceptance of these two procedures. Besides, we did not include via oral DBE in our research because of the small sample size. Only 21 patients received both CTE and via oral DBE examinations during our research time. Comparison of tolerance between via anal DBE, via oral DBE, and CTE will be done in our future studies when we have a larger sample size. Furthermore, the interval between these two tests was 2 months. During this interval, patients’ disease activity might have been different, which also could have impacted their tolerance of the examinations. Finally, we found that although DBE was a more burdensome test than CTE, there were still 38.3% of patients in our cohort who preferred to choose DBE next time. The reason why they had a preference for DBE should be studied in further research.
Conclusion
Our study found CTE was more tolerable and less burdensome than DBE in many aspects and preferred by more patients. Mannitol intake, bowel preparation, and radiation exposure were the three main reasons for patients’ intolerance of CTE while painfulness, bowel preparation, and invasiveness were the three major causes of patients’ burden in DBE. Further modifications of procedures should be made in order to improve patients’ tolerance and acceptance of both CTE and DBE.
Author contributions
All authors contributed toward data analysis, drafting and critically revising the paper, and agreed to be accountable for all aspects of the work.
Acknowledgments
This study was supported by National Natural Science Foundation of China (no 81670503 and 81602558) and Shanghai Committee of Science and Technology Foundation (no 16411950408 and 15ZR1426400).
Supplementary materials
Questionnaires used in our study comparing tolerance between computed tomography enterography and double-balloon enteroscopy.
Figure S1 Questionnaire A.
Abbreviation: CTE, computed tomography enterography.
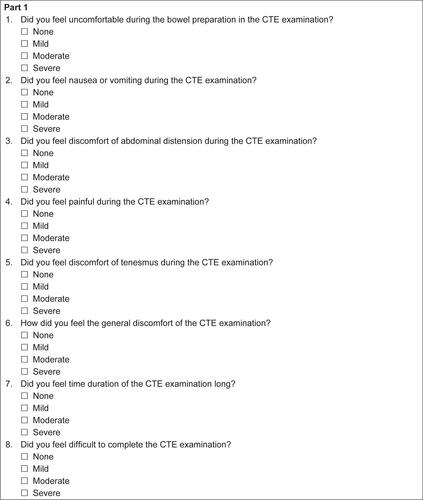
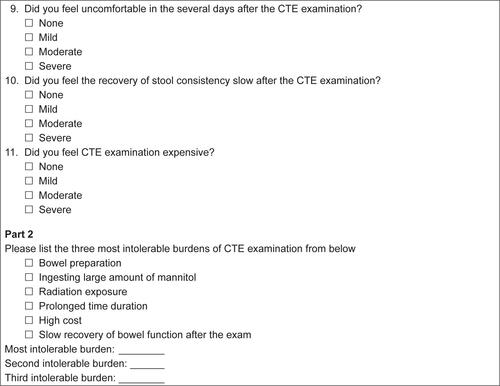
Figure S2 Questionnaire B.
Abbreviations: CTE, computed tomography enterography; DBE, double-balloon enteroscopy.
Disclosure
The authors report no conflicts of interest in this work.
References
- PashaSFLeightonJADetection of suspected small bowel bleeding: challenges and controversiesExpert Rev Gastroenterol Hepatol201610111235124427366927
- PashaSFHaraAKLeightonJADiagnostic evaluation and management of obscure gastrointestinal bleeding: a changing paradigmGastroenterol Hepatol (N Y)200951283985020567529
- PostgateADespottEBurlingDSignificant small-bowel lesions detected by alternative diagnostic modalities after negative capsule endoscopyGastrointest Endosc20086861209121419028234
- MarkovaIKluchovaKZborilRSmall bowel imaging – still a radiologic approach?Biomedical papers of the Medical Faculty of the University Palacky, Olomouc, Czechoslovakia2010154123132 Dissertation
- WangZChenJQLiuJLQinXGHuangYCT enterography in obscure gastrointestinal bleeding: a systematic review and meta-analysisJ Med Imaging Radiat Oncol201357326327323721134
- HuprichJEBarlowJMHanselSLAlexanderJAFidlerJLMultiphase CT enterography evaluation of small-bowel vascular lesionsAJR Am J Roentgenol20132011657223789659
- WangJGuoQZhaoJMultidetector CT enterography versus double-balloon enteroscopy: comparison of the diagnostic value for patients with suspected small bowel diseasesGastroenterol Res Pract20162016517287326962305
- GracaBMFreirePABritoJBIlharcoJMCarvalheiroVMCaseiro-AlvesFGastroenterologic and radiologic approach to obscure gastrointestinal bleeding: how, why, and when?Radiographics201030123525220083596
- HeBGongSHuCObscure gastrointestinal bleeding: diagnostic performance of 64-section multiphase CT enterography and CT angiography compared with capsule endoscopyBr J Radiol20148710432014022925248830
- YamamotoHSekineYSatoYTotal enteroscopy with a nonsurgical steerable double-balloon methodGastrointest Endosc200153221622011174299
- LiuKKaffesAJReview article: the diagnosis and investigation of obscure gastrointestinal bleedingAliment Pharmacol Ther201134441642321692820
- GillRSKaffesAJSmall bowel stricture characterization and outcomes of dilatation by double-balloon enteroscopy: a single-centre experienceTherap Adv Gastroenterol201473108114
- LahatAKopylovUAmitaiMMMagnetic resonance enterography or video capsule endoscopy – what do Crohn’s disease patients prefer?Patient Prefer Adherence2016101043105027354774
- PaparoFGarlaschiABiscaldiEBacigalupoLCevascoLRollandiGAComputed tomography of the bowel: a prospective comparison study between four techniquesEur J Radiol2013821e1e1022999647
- WiardaBMStolkMHeineDGPatient burden and patient preference: comparing magnetic resonance enteroclysis, capsule endoscopy and balloon-assisted enteroscopyJ Gastroenterol Hepatol201328346447122741615
- YenHHChenYYYangCWLiuCKSoonMSClinical impact of multidetector computed tomography before double-balloon enteroscopy for obscure gastrointestinal bleedingWorld J Gastroenterol201218769269722363142
- GoverdeAKorsseSEWagnerASmall-bowel surveillance in patients with Peutz-Jeghers syndrome: comparing magnetic resonance enteroclysis and double balloon enteroscopyJ Clin Gastroenterol2017514e27e3327404294
- PashaSFLeightonJADasADouble-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysisClin Gastroenterol Hepatol20086667167618356113
- MasselliGDi TolaMCascianiEDiagnosis of small-bowel diseases: prospective comparison of multi-detector row CT enterography with MR enterographyRadiology2016279242043126599801
- WeissfeldJLLingBSSchoenREAdherence to repeat screening flexible sigmoidoscopy in the Prostate, Lung, Colorectal, and Ovarian (PLCO) Cancer Screening TrialCancer200294102569257612173322
- NegaardASandvikLBerstadAEMRI of the small bowel with oral contrast or nasojejunal intubation in Crohn’s disease: randomized comparison of patient acceptanceScand J Gastroenterol2008431445118158695
- LinOSKozarekRAGluckMPreference for colonoscopy versus computerized tomographic colonography: a systematic review and meta-analysis of observational studiesJ Gen Intern Med201227101349136022700393
- van der PaardtMPBoellaardTNZijtaFMMagnetic resonance colonography with a limited bowel preparation and automated carbon dioxide insufflation in comparison to conventional colonoscopy: patient burden and preferencesEur J Radiol2015841192525455410
- StoopEMde HaanMCde WijkersloothTRParticipation and yield of colonoscopy versus non-cathartic CT colonography in population-based screening for colorectal cancer: a randomised controlled trialLancet Oncol2012131556422088831
- SaliLMascalchiMFalchiniMReduced and full-preparation CT colonography, fecal immunochemical test, and colonoscopy for population screening of colorectal cancer: a randomized trialJ Natl Cancer Inst20151082 pii: djv319
- AjajWGoyenMSchneemannHOral contrast agents for small bowel distension in MRI: influence of the osmolarity for small bowel distentionEur Radiol20051571400140615754160
- KimESLeeWJJeenYTA randomized, endoscopist-blinded, prospective trial to compare the preference and efficacy of four bowel-cleansing regimens for colonoscopyScand J Gastroenterol201449787187724940942
- DesmondANO’ReganKCurranCCrohn’s disease: factors associated with exposure to high levels of diagnostic radiationGut200857111524152918443021
- ChatuSSubramanianVPollokRCMeta-analysis: diagnostic medical radiation exposure in inflammatory bowel diseaseAliment Pharmacol Ther201235552953922239831
- EstayCSimianDLubascherJFigueroaCO’BrienAQueraRIonizing radiation exposure in patients with inflammatory bowel disease: are we overexposing our patients?J Dig Dis2015162838925420751
- ChatuSPoullisAHolmesRGreenhalghRPollokRCTemporal trends in imaging and associated radiation exposure in inflammatory bowel diseaseInt J Clin Pract201367101057106524073979
- JungYSParkDIKimERQuantifying exposure to diagnostic radiation and factors associated with exposure to high levels of radiation in Korean patients with inflammatory bowel diseaseInflamm Bowel Dis20131991852185723702806
- OgnibeneNMBasileMDi MaurizioMPetrilloGDe FilippiCFeatures and perspectives of MR enterography for pediatric Crohn disease assessmentRadiol Med2016121536237726838591
- MasselliGMastroiacovoIDe MarcoECurrent tecniques and new perspectives research of magnetic resonance enterography in pediatric Crohn’s diseaseWorld J Radiol20168766868227551337
- WesterlandOGriffinNMagnetic resonance enterography in Crohns DiseaseSemin Ultrasound CT MR201637428229127342892
- GriffinNWesterlandOThe role of magnetic resonance enterography in the evaluation of non-Crohns pathologiesSemin Ultrasound CT MR201637429230027342893
- ZakeriNPollokRCDiagnostic imaging and radiation exposure in inflammatory bowel diseaseWorld J Gastroenterol20162272165217826900282
- KralikRTrnovskyPKopacovaMTransabdominal ultrasonography of the small bowelGastroenterol Res Pract2013201389670424348544
- KawanoSOkadaHIwamuroMAn effective and safe sedation technique combining target-controlled infusion pump with propofol, intravenous pentazocine, and bispectral index monitoring for peroral double-balloon endoscopyDigestion201591211211625677385
- ZubekLSzaboLLakatosPLPappJGalJEloGDouble balloon enteroscopy examinations in general anesthesiaWorld J Gastroenterol201016273418342220632445
- TreeprasertsukSRerknimitrRAngsuwatcharakonPThe safety of propofol infusion compared to midazolam and meperidine intravenous bolus for patients undergoing double balloon enteroscopyJ Med Assoc Thai201497548348925065086
- ZubekLSzaboLGálJLakatosPLPappJEloGGeneral anesthesia during double balloon enteroscopy – Hungarian experiencesOrv Hetil20101514819761982 Hungarian21084249
- SchroederCKaoutzanisCTocco-BradleyRPatients prefer propofol to midazolam plus fentanyl for sedation for colonoscopy: results of a single-center randomized equivalence trialDis Colon Rectum2016591626926651114
- HsiehYHChouALLaiYYPropofol alone versus propofol in combination with meperidine for sedation during colonoscopyJ Clin Gastroenterol200943875375719169146
- OrmeciACAkyuzFBaranBRetention during capsule endoscopy: Is it a real problem in routine practice?J Int Med Res201644496897527377071
- LimYJLeeOYJeenYTIndications for detection, completion, and retention rates of small bowel capsule endoscopy based on the 10-year data from the Korean Capsule Endoscopy RegistryClin Endosc201548539940426473123