
Abstract
Study objectives
Patients with comorbid posttraumatic stress disorder (PTSD) and obstructive sleep apnea (OSA) manifest low adherence to continuous positive airway pressure (CPAP) due to fixed, pressure-induced expiratory pressure intolerance (EPI), a subjective symptom and objective sign aggravated by anxiety sensitivity and somatosensory amplification. As advanced PAP therapy modes (ie, auto-bilevel PAP [ABPAP] or adaptive servo-ventilation [ASV]) may address these side effects, we hypothesized such treatment would be associated with decreased expiratory intolerance and increased adherence in posttraumatic stress patients with co-occurring OSA.
Methods
We reviewed charts of 147 consecutive adult patients with moderately severe posttraumatic stress symptoms and objectively diagnosed OSA. All patients failed or rejected CPAP and were manually titrated on auto-adjusting, dual-pressure ABPAP or ASV modes in the sleep laboratory, a technique to eliminate flow limitation breathing events while resolving EPI. Patients were then prescribed either mode of therapy. Follow-up encounters assessed patient use, and objective data downloads (ODDs) measured adherence.
Results
Of 147 charts reviewed, 130 patients were deemed current PAP users, and 102 provided ODDs: 64 used ASV and 38 used ABPAP. ODDs yielded three groups: 59 adherent per insurance conventions, 19 subthreshold compliant partial users, and 24 noncompliant. Compliance based on available downloads was 58%, notably higher than recently reported rates in PTSD patients with OSA. Among the 19 partial users, 17 patients were minutes of PAP use or small percentages of nights removed from meeting insurance compliance criteria for PAP devices.
Conclusion
Research is warranted on advanced PAP modes in managing CPAP failure in PTSD patients with comorbid OSA. Subthreshold adherence constructs may inform clinical care in a patient-centric model distinct from insurance conventions. Speculatively, clinical application of this transitional zone (“subthreshold” number of hours) may increase PAP use and eventual adherence.
Plain language summary
Obstructive sleep apnea (OSA), a sleep breathing disorder, frequently co-occurs among patients with posttraumatic stress disorder (PTSD), a mental health condition arising after traumatic experiences. Continuous positive airway pressure (CPAP) therapy is the standard OSA treatment that pushes air through the nose or mouth, functioning as a physiological stent to maintain airway patency. CPAP failure is common in PTSD patients, possibly due to expiratory pressure intolerance triggered by fixed pressurized air delivery in which the patient reports difficulty breathing out against the incoming air flow. Advanced positive airway pressure (PAP) devices known as auto-bilevel PAP and adaptive servo-ventilation can be manually tested in the sleep laboratory to decrease expiratory intolerance in order to improve patient comfort and thereby increase use. These objectives are achieved with advanced PAP by diminishing the volume of pressurized air against which the patient breathes during exhalation. Some research suggests PTSD patients using advanced devices will use their PAP machines more consistently. In our study, advanced PAP was associated with PAP adherence rates higher than typically observed in PTSD patients using CPAP.
Introduction
The prevalence of comorbid PTSD and OSA appears to be much higher than previously recognized.Citation1,Citation2 The gold standard intervention for OSA is CPAP therapy, and therapeutic effects are most apparent among patients achieving adherence to therapy.Citation3 Interestingly, both older researchCitation4,Citation5 and very recent studiesCitation6,Citation7 also indicate treatment of OSA in PTSD patients is associated with decreased PTSD symptom severity. Unfortunately, trauma survivors demonstrate low adherence rates or partial use for PAP therapy.Citation8–Citation11 Lettieri et al reported PTSD/OSA patients used PAP on 53.3%±35.6% of nights for an average of 3.4±2.8 hours/night, but only 30.2% were adherent per standard insurance compliance metrics compared to 55.1% of OSA patients without PTSD.Citation9 In a recent study examining the effects of PAP therapy on PTSD symptoms, Orr et al assessed 59 patients prescribed a device, yet only 12 (20%) were compliant at 6-month follow-up. Another 15 patients were using prior to being lost to follow-up, and half were probably adherent, yielding an approximate overall compliance rate of 34%.Citation7 In contrast to these low adherence rates, Orr et al demonstrated very high partial use rates in their sample; for example, at 3 months, although 18 patients were lost to follow-up, the remaining 41 patients were all using their devices at least some of the time. At 6 months, after another 9 patients were lost to follow-up, 81% of the remaining 32 patients were still using PAP.Citation7
Low adherence and partial use of PAP are widespread among sleep apnea patients in the general population,Citation12–Citation14 and more so in psychiatric patients with OSA comorbidity.Citation15–Citation17 Poor PAP compliance is typically investigated through frameworks attending to behavioral change models,Citation18 psychoeducation,Citation13,Citation14 and other coaching strategies; and, many clinical practice models have been researched and described to improve adherenceCitation12,Citation19–Citation22 though few address the issue of partial use, an outcome incisively explored by Stepnowsky et al.Citation23,Citation24 Though partial use (subthreshold adherence) research studies are sparse, they have consistently demonstrated improved clinical outcomes, most notably daytime sleepiness.Citation25–Citation29 Such exploratory findings in subthreshold adherence suggests a potential value in defining the clinical importance of partial PAP use. However, research on partial use in PTSD patients is even more scarce, perhaps due to the influences of insurance carriers on dispensing PAP devices wherein subjective outcomes are often relegated to objective duration of use.Citation30,Citation31
Our clinic implements a compliance protocol also focusing on psychological attributes, but we differ from conventional approaches by targeting the patient’s experiential and emotional reactions to pressurized air.Citation32 In brief, psychiatric patients exposed to CPAP are susceptible to the problems of anxiety sensitivityCitation33,Citation34 and somatosensory amplification.Citation35–Citation37 In our clinical experience, both of these transdiagnostic vulnerabilities are triggered when attempting to use fixed pressurized air. As CPAP delivers the same pressure setting on inspiration and expiration for any given breath, the patient is always exhaling against a pressure greater than required to maintain a patent airway, an objectively proven observation described in the sleep literature since 1990.Citation38 This fixed pressure on exhalation often produces an uncomfortable sensation sufficient to trigger PAP intolerance,Citation39 and in vulnerable patients, claustrophobic or panic reactions flare up.Citation40–Citation42 Thus, at our sleep medical center, which specializes in the treatment of psychiatric patients with sleep disorders,Citation43 we observe CPAP technology itself as a major cause of low adherence or outright rejection.
We recently reported on this phenomenon in a consecutive series of psychiatric patients with comorbid OSA or UARS.Citation30 Using CMS criteria,Citation44 we measured adherence (>4 hours/night on >70% of nights) and subthreshold compliance (subcompliant regular users, who were PAP users not meeting CMS guidelines but who averaged regular, nightly use >3 hours/night) in 113 patients naïve to treatment who failed CPAP and subsequently filled prescriptions for advanced PAP devices. Among 113 patients, 104 (92%) were current users at 7-month follow-up. ODDs available for 93 patients showed 59 adherent, averaging 42.0 (SD 12.1) hours/week, and 21 subthreshold compliant (partial users), averaging 18.0 (SD 5.6) hours/week.Citation30 Adherence equaled 63% for patients with ODDs; another 10 partial users achieved levels minutes removed from the 4 hours/night criteria or a few percentage points from attaining 70% of nights criteria for adherence.Citation30
The advanced PAP modes applied in the prior and current research were dual-pressure, auto-adjusting devices, manually titrated in the sleep laboratory, that is, ABPAP or ASV, the latter in those qualifying for complex sleep apnea, a condition in which iatrogenic central apneas emerge upon exposure to CPAP.Citation45 As described elsewhere, advanced PAP technology has been associated with reversing CPAP failure,Citation46 improving adherence in chronic insomnia patients with comorbid OSA/UARS,Citation47,Citation48 decreasing residual sleepiness,Citation49 and yielding higher-than-usual rates of compliance in psychiatric patients.Citation30
The use of manually titrated, advanced PAP technology derives from our sleep center’s 2005 policies and procedures, emphasizing the need to address the adverse experiences reported by patients while attempting CPAP technology.Citation32,Citation43,Citation50–Citation56 To reiterate, the model was formulated to address “claustrophobic tendencies”Citation41,Citation42,Citation57 in psychiatric or other patients who demonstrate anxiety sensitivity or somatosensory amplification to pressurized air, often appearing as awkward attempts to overcontrol one’s breathing while struggling to adapt to PAP.Citation32 This pressure-related distress manifests as subjective (awake) or objective (asleep) EPI, and usually both problems emerge during titration PSG.Citation30,Citation46,Citation48 As the patient struggles to gain sufficient air or fights smothering sensations from excessive air, claustrophobic tendencies emerge, which for vulnerable patients leads to rapid termination of the titration procedure, culminating in the patient displacing the mask.Citation32 Among patients who continue to use the device, central apneas and eventually complex sleep apnea may emerge.Citation30,Citation45
While some research focuses on the mask as the restrictive element triggering claustrophobic tendencies,Citation41,Citation57 in our experience, most patients with mask difficulties report discomfort or poor fit and request a different mask, whereas only a small proportion report restrictive sensations triggering claustrophobic tendencies. For example, in a recent study on adherence, >50% of patients with claustrophobia requested a full-face mask when filling their PAP prescriptions, a counterintuitive finding.Citation30 In contrast, the distress related to pressurized air is the more common instigating complaint as patients frequently exclaim, “I just cannot breathe with the device” or “the machine is trying to control my breathing”. As one patient recently remarked, “It feels like driving a motorcycle without a wind visor”. Paradoxically, mask issues may signal a covert pressure intolerance problem.Citation32
For PTSD patients already suffering high levels of anxiety and anxiety sensitivity,Citation33,Citation34 both generalized pressure intolerance and EPI-induced claustrophobic tendencies may arise during the process of somatosensory amplification.Citation35–Citation37 Anecdotally, vulnerable PTSD patients’ attempts at PAP may deteriorate to an unambiguous phobic response,Citation40 after which they avoid further trials. Likewise, some patients describe these events as traumatizing, and this conceptualization is supported by subsequent treatment avoidance behavior or long lapses between the initial traumatizing PAP experience and efforts to reattempt PAP therapy.Citation46
The current retrospective chart review examined a consecutive series of OSA/UARS patients with moderately severe posttraumatic stress symptoms, presumptively diagnosed with chronic PTSD and prescribed PAP therapy. We hypothesized the use of advanced PAP technology would be associated with two outcomes: 1) 50% adherence in a sample of patients previously experiencing CPAP failure, intolerance, or rejection; and 2) a substantial subgroup would achieve subthreshold adherence (partial use), leaving them just shy of CMS-derived compliance.
Methods
Informed consent
Patients provided consent during completion of the online intake at MSAS to use their information anonymously for research purposes. All data were de-identified for this case series. The intake questionnaire assessed sleep symptoms based on nosology for sleep disorders in the International Classification of Sleep Disorders.Citation58 The Los Alamos Medical Center Institutional Review Board found the chart review exempt because it was a retrospective analysis of a de-identified dataset, and patients received no experimental procedures or interventions.
Sample and inclusion criteria
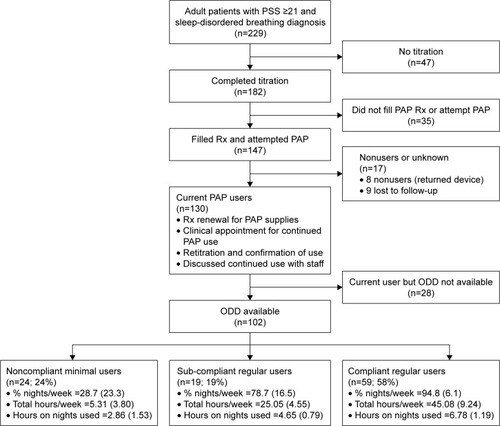
This retrospective chart review included adult patients (≥18 years old), presenting to MSAS between December 2009 and January 2016, who 1) reported a history of traumatic exposure and scored ≥21 on the PSS;Citation59 2) were diagnosed with OSA (AHI ≥5) or UARS (AHI <5 and RDI ≥15) during objective sleep testing; 3) failed CPAP therapy during titration or at home; 4) completed an attended, manual titration (or split-therapy PSGCitation60) of an advanced auto-titrating device (ABPAP or ASV); and 5) filled a prescription for ABPAP or ASV therapy with attempted home use (). After starting the chart review with 229 eligible patients with PSS ≥21 and a diagnosis of sleep-disordered breathing, 47 did not complete titration PSG. Of the remaining 182, 35 did not fill their prescription for PAP, leaving 147 patients who attempted PAP. Of the 147 PAP attempters, 130 were current PAP users ( provides the use criteria) at follow-up, and 17 were nonusers (8 returned device to DME; 9 lost to follow-up). ODDs were available for 102 of the 130 current users. A significantly larger proportion of users with ODD (76.5%) were anxiety cluster positive compared to users without ODD (53.6%; P=0.02). There was no difference in the remaining psychiatric histories between the two groups. Comparison of sociodemographics, PTSD symptoms scores, subjective intake sleep indices, and objective sleep breathing indices between our final sample of 102 users with ODD and the 28 current users without ODD yielded no significant differences.
Figure 1 Flowchart showing inclusion and exclusion criteria resulting in the 102 patients comprising our three compliance groups: 1) compliant regular users, 2) subcompliant regular users, and 3) noncompliant minimal users.
PAP titration protocol
An overarching premise embedded within our policies and procedures is the well-documented fact that early experiences with PAP are highly predictive of success or failure.Citation20,Citation61–Citation64 When we encounter patients with high probability for CPAP failure, we err on the side of a proactive practice model focusing on the individual’s early subjective experiences with the CPAP mode. Although for insurance purposes any patient must “fail” CPAP to be switched to an advanced form of PAP, there are no formal criteria for CPAP failure. In these circumstances where an individual develops an immediate panicky or frank claustrophobic response when attempting to breathe outward against continuous pressure delivered inward, further attempts at patient persuasion by the physician or sleep technologist to “try a little harder” with CPAP may prove counterproductive. More commonly, pushing this incipient failing strategy often elicits emotional responses from the patient, including frustration, discouragement, anxiety, and fear.Citation43
In these early attempts at PAP initiation, acceptance, and adaptation, discretion has guided us to switch the individual to an expiratory relief mode, which may rapidly enhance the patient’s level of comfort and evoke a more positive attitude. During the course of the titration itself as these patients manifest objective expiratory tolerance, even with APAP, EPR, or BPAP devices, we attempt to smooth out the airflow signalCitation65 with the use of ABPAP or ASV devices, the latter when meeting complex sleep apnea diagnosis (CAI ≥5, CAI/AHI >50%).Citation45 Central apneas are not uncommon at higher elevations (Albuquerque, NM [elev. 1,627.6 meters]) or among anxiety patients prone to hyperventilationCitation30,Citation48 that may trigger CO2 decrements and resultant drop off in breathing drive (loop gain).Citation45,Citation66
When manually titrated, the sleep technologist overrides the aspects of the auto-adjusting algorithms that appear to have responded ineffectually to the dueling problems of residual flow limitation and iatrogenic EPI.Citation46,Citation67 As described elsewhere, this nuanced approach to titrations often requires changes in the 0.2- to 0.4-cm H2O range, while adjusting both inspiratory and expiratory settings.Citation48 Although our experience reflects case series, we have published on this clinical care model, involving 744 OSA/UARS patients,Citation30,Citation46–Citation48,Citation67 and have treated 3,934 clinical patients in this manner at our sleep center from 2008 to the present.
As an aside, as long as patients attempt standard PAP modes during the presleep desensitization or the titration PSG or through home use, subsequent subjective or objective failure of the treatment usually provides sufficient grounds for insurance purposes to escalate the patient’s care to receive a trial with an advanced PAP mode. In our extensive clinical experience, the manual titration of ABPAP or ASV in the sleep laboratory has proven consistently superior to home use of prescribed, default settings for these advanced devices. Thus, the sleep laboratory plays a critical role in this protocol.Citation46,Citation67,Citation68
Adherence metrics
The 102 patients with objective compliance data were divided into three subgroups: C-RU, patients averaging ≥4 hours/night on ≥70% of nights used, thus meeting CMS criteria; SC-RU, patients using PAP regularly with average nightly use ranging from 3 to almost 6 hours per night but not meeting the 4 hours of use on 70% of nights metric for compliance; and NC-MU, patients with minimal PAP use and averaging <2 hours/night. Rare differences were noted in baseline characteristics among the three groups (). We also calculated compliance using an alternate metric based on total weekly PAP hours derived from Medicare criteria where their minimum of 4 hours/night on 4.9 nights/week totaled 19.6 hours/week. Rounding up to 20 hours/week, we defined two groups: adherent, averaging >20 hours/week and non-adherent, averaging <20 hours/week.
Table 1 Comparison of intake PSS, ISI, and ESS total scores, subjective sleep indices, psychiatric history, objective sleep breathing diagnostic data, and objective titration data for complex sleep apnea cases
Data analysis
One-way ANOVA compared continuous variables, and Hedge’s g calculated effects between unequal-sized subsamples. Chi-square analyzed dichotomous variables, and effect sizes were based on proportional differences between groups. A P-value of 0.05 was considered statistically significant. Data were analyzed with IBM SPSS Statistics, version 11.0 for Windows, 2002 (IBM Corporation). All continuous variables are expressed as mean (SD).
Results
Sociodemographics and baseline sleep metrics
The final 102 patients were predominantly middle aged (average age = 49.0 years), overweight (average BMI = 32.5), Caucasian (55.9%) or Hispanic (32.4%), females (56.0%) who were married/living with partner (55.9%), and completed some college or less (62.8%). At intake, the mean PSS score (30.63 [8.03]) equated to moderately severe symptoms, mean ISI score (20.53 [4.66]) moderately severe insomnia, and mean Epworth Sleepiness Scale score (11.34 [6.48]) was in the mild range for daytime sleepiness (). The average time to follow-up was 12.72 (12.71) months.
Nearly 90% of patients were diagnosed with OSA (n=88), and the remainder suffered UARS (n=12) and primary central sleep apnea (n=2). By diagnostic breathing event indices, sleep breathing was severe based on RDI, moderate based on AHI, and very mild based on CAI. Ultimately, 64 patients (62.75%) were diagnosed with complex sleep apnea, necessitating the use of ASV mode of treatment (). Thirty-eight remaining patients used ABPAP.
CMS compliance metric
By standard CMS compliance metrics (), there were 59 C-RU, 19 SC-RU, and 24 NC-MU patients. Thus, 58% of patients were compliant, and 42% noncompliant. On ODD among the 43 noncompliant patients, there were 19 SC-RU patients (partial users) within minutes from averaging 4 hours/night or a few percentage points from attaining adherence on 70% of nights. And, 17 of 19 SC-RU patients averaged >4 hours of PAP use on nights used yet were noncompliant due to insufficient nights used per week. PTSD symptom severity and insomnia severity did not correlate significantly with adherence status, albeit small nonsignificant effects were present demonstrating higher PSS and ISI scores in the non-adherent group compared to the adherent group ().
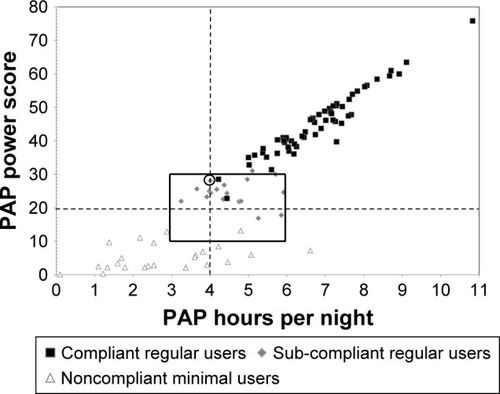
highlights SC-RU patients’ PAP use relative to C-RU and NC-MU patients. The boxed area demarcates a “transitional zone” comprising 3–6 hours of nightly use (horizontal sides of box) and 10–30 hours of weekly use (vertical sides of box). Note the two C-RU patients (black squares) within this transitional zone were deemed CMS compliant, whereas by comparison numerous SC-RU patients (gray diamonds) exceeded the nightly or the weekly hours of use of these two compliant patients, including 17 who documented ≥20 weekly hours. As seen in , 15 of 19 SC-RU patients averaged >4 hours/night but were noncompliant due to not meeting the CMS 70% requirement. One example (circled gray diamond) is the patient who averaged 4.0 hours/night and 28.0 hours/week but was noncompliant because PAP use was 7 hours on 4 of 7 nights of the week, thus achieving compliance on only 56% of nights.
Figure 2 Scatter plot of weekly PAP hours used as a product of nightly PAP average (hours/night) and percentage of nights used (nights/week) for C-RU, SC-RU, and NC-MU.
Abbreviations: PAP, positive airway pressure; C-RU, compliant regular users; SC-RU, sub-compliant regular users; NC-MU, noncompliant minimal users; CMS, Center of Medicare and Medicaid Services.
Last, of potential clinical import, the proportions of ASV and ABPAP users were nearly identical for C-RU and NC-MU groups, but the SC-RU group demonstrated a significantly higher proportion of patients using ASV (n=15) compared to ABPAP (n=4) (contingency coefficient =0.50). Regarding residual breathing events on ODD, there was no significant difference (P=0.50) in AHI between C-RU (2.10 (3.11) events/hour) and SC-RU (2.68 [4.04]) patients.
Alternate metric (weekly use hours)
Rounding up to 20 hours/week, our sample would have yielded an additional 17 patients for an adherence total of 74.5% (76/102 patients) and a non-adherence total of 25.5% (26/102 patients) if CMS permitted total hours of use for adherence criteria.
Discussion
This research provides evidence for the use of advanced PAP therapies such as ABPAP or ASV to treat subjective and objective EPI in PTSD patients who failed CPAP therapy for the treatment of their comorbid OSA or UARS. The findings are consistent with a clinically meaningful comfort effectCitation69 that counters distress experienced by patients with anxiety sensitivity or somatosensory amplification who struggle to exhale against fixed pressurized airflow. Due to the retrospective, uncontrolled design of the study, however, these findings can only be classified as an association.
This study also highlights the lack of a patient-centric perspective in the CMS compliance metric, which could have led to termination of therapy in 17 patients (, gray diamonds) who were minutes or portions of nights removed from the 4 hours/70% nights standard despite >20 hours/week of use. Given the time course required for vulnerable psychiatric patients to adapt to PAP therapy,Citation46 we have previously raised the question on whether the concept of hours of use is a more pragmatic and appropriate metric in the management of more complex sleep-disordered breathing patients,Citation30 which also aligns with Stepnowsky’s “dose–response” model of PAP care.Citation23,Citation24 Moreover, by neglecting this clinical care principle, current insurance directives may discourage sub-threshold partial PAP users who need a longer interval of adaptation to meet coverage standards; likewise, a partial use framework would also promote a longer transitional window for problem-solving mask and pressure complaints as well as other adaptation issues, all essential ingredients to achieving adherence.Citation12–Citation14,Citation19,Citation21,Citation22,Citation61,Citation64
Along the same lines, whereas adherence is largely an insurance-driven policy,Citation44 partial use offers the potential for a patient-centric model of care because the latter provides opportunities to more accurately investigate dose–response relationships between the symptoms reported by sleep-disordered breathing patients and hours of use, a more precise continuous variable. In our recent study on adherence, outcomes improved in subthreshold compliant patients, and small correlation coefficients indicated that increasing hours of use were associated with decreasing symptoms of insomnia (r=0.20) and nocturia episodes (r=0.25). On the other hand, Orr et al’s study demonstrated a small effect for decreased PTSD symptoms associated with an increased number of nights used, whereas neither hours of use nor number of nights >4 hours showed significant effects for improvement in PTSD symptoms, albeit their sample size was small.Citation7 Once again, these distinctions highlight how the two constructs of adherence and use may lead to paradoxical findings, which may interfere with our ability to more effectively treat OSA and UARS patients. Prospective research is needed to determine the clinical advantages and disadvantages in the application of adherence or use.
The current study is limited by the retrospective, uncontrolled design. Future studies using randomized controlled trials may investigate the benefits of advanced vs traditional PAP devices in PTSD patients with comorbid sleep-disordered breathing. And prospective studies should also compare outcomes between PTSD and non-PTSD patients with OSA to discern how clinical care models may require different resources for each group. In particular, studies should compare the adherence rates of physician-prescribed APAP pressure ranges at setup (per Orr et alCitation7) vs in-laboratory, manually titrated settings for dual-pressure auto-adjusting devices. In addition, selection bias is a concern in this cohort because we were unable to obtain data downloads in 28 (22%) of the user group and thus could not confirm if they were adherent, albeit it is worth reiterating that based on our clinical follow-up encounters, 130 (88%) of these 147 total PAP attempters appeared to be current users.
This distinction between use and adherence raises another clinical question on how to delineate the proper baseline in a sample of PAP patients assessed for adherence. We chose a construct similar to Orr et al (“willingness-to-use PAP”)Citation7 by creating a baseline of patients who filled a PAP prescription. Arguments, pro and con could be made to use more or less stringent starting points in determining adherence rates in various cohorts of OSA/UARS patients.
In summary, though not well described in the sleep literature, certain sleep-disordered breathing patients describe CPAP attempts as “traumatizing experiences”. Related theories point to the potential for a CPAP user to experience a phobic responseCitation40 to the mask itself or pressurized air, and OSA patients may also be susceptible to activation of a “false suffocation alarm” due to rapid changes in carbon dioxide, leading to panic attacks.Citation41 Taken together, at-risk OSA patients with anxiety disorders, as the best examples, are already vulnerable to claustrophobic tendencies prior to attempting CPAP because they are at risk for anxiety sensitivity and somatosensory amplification. When initiating fixed pressurized air treatment, these patients develop intolerance and irregular breathing patterns, including instances of iatrogenic central apneas.Citation32,Citation45,Citation46 PTSD patients in particular and psychiatric patients in general who cannot adapt rapidly to PAP therapy may be served by monitoring their graded levels of adherence through which they would be encouraged to traverse steps from minimal use to subthreshold levels (partial users) and eventually full adherence during extended time periods.Citation23,Citation24,Citation30,Citation46 These time frames may prove longer than the standard 60- to 90-day CMS mandated window for clinical follow-up. A testable hypothesis is proposed to determine whether advanced PAP modes facilitate this process.
Author contributions
Ms Obando and Mr Ulibarri were responsible for acquisition of data. Ms Obando, Mr Ulibarri, Dr Krakow, and Ms McIver were responsible for data analysis and interpretation. Dr Krakow was responsible for the conception and design of the study. All authors contributed to the revision of manuscript, approved the final manuscript version for publication, and have agreed to be accountable for all aspects of this manuscript.
Abbreviations
| ABPAP | = | auto-bilevel PAP |
| AHI | = | apnea–hypopnea index |
| APAP | = | auto-CPAP |
| ASV | = | adaptive servo-ventilation |
| BPAP | = | bilevel positive airway pressure |
| CAI | = | central apnea index |
| CMS | = | Center of Medicare and Medicaid Services |
| CPAP | = | continuous positive airway pressure |
| C-RU | = | compliant regular PAP users |
| EPI | = | expiratory pressure intolerance |
| EPR | = | expiratory pressure relief |
| ISI | = | insomnia severity index |
| MSAS | = | Maimonides Sleep Arts & Sciences |
| NC-MU | = | non-compliant minimal PAP users |
| ODD | = | objective data download |
| OSA | = | obstructive sleep apnea |
| PAP | = | positive airway pressure |
| PSG | = | polysomnography |
| PSS | = | PTSD Symptom Scale |
| PTSD | = | posttraumatic stress disorder |
| RDI | = | respiratory disturbance index |
| SC-RU | = | sub-compliant regular PAP users |
| UARS | = | upper airway resistance syndrome |
Acknowledgments
The authors thank the Los Alamos Medical Center and the Los Alamos Medical Center Sleep Laboratory for administrative and clinical assistance in the completion of this research project.
Disclosure
Dr Krakow is involved in six main activities related to his work on sleep medicine: He owns and operates six sites that provide education and offer products and services (www.nightmaretreatment.com, www.ptsdsleepclinic.com, www.sleeptreatment.com, www.sleepdynamictherapy.com, www.soundsleepsoundmind.com, and www.nocturiacures.com). He is the medical director of a national DME company Classic Sleep Care in which his sole functions are consultation and QA; he has neither patient encounters nor does he benefit from the sale of any DME equipment. He markets and sells three books for patients with sleep disorders (Insomnia Cures, Turning Nightmares into Dreams, and Sound Sleep, Sound Mind). He owns and operates one commercial sleep center (Maimonides Sleep Arts & Sciences). He conducts CME/CEU educational programs for medical and mental health providers to learn about sleep disorders. Sometimes, programs involve the attendee paying a fee directly to their center. Other times, the workshops at other locations may be paid for by vendors such as Respironics and RESMED or other institutions such as the AMEDDC&S, VAMC, and regional sleep center conferences. He is the president of a nonprofit sleep research center, the Sleep & Human Health Institute (www.shhi.org), that occasionally provides consultation services or receives grants for pilot studies, the most recent of which was ResMed (~$400,000, January 2015, funding for randomized control trial of PAP treatment in insomnia patients). Ms Obando, Mr Ulibarri, and Ms McIver report no conflicts of interest in this work.
References
- JaoudePVermontLNPorhomayonJEl-SolhAASleep-disordered breathing in patients with post-traumatic stress disorderAnn Am Thorac Soc201512225926825535907
- KrakowBJUlibarriVAMooreBAMcIverNDPosttraumatic stress disorder and sleep-disordered breathing: a review of comorbidity researchSleep Med Rev201524374525644985
- WangYAiLLuoJEffect of adherence on daytime sleepiness, fatigue, depression and sleep quality in the obstructive sleep apnea/hypopnea syndrome patients undertaking nasal continuous positive airway pressure therapyPatient Prefer Adherence20171176977928442894
- KrakowBLowryCGermainAA retrospective study on improvements in nightmares and post-traumatic stress disorder following treatment for co-morbid sleep-disordered breathingJ Psychosom Res200049529129811164053
- YouakimJMDoghramjiKSchutteSLPosttraumatic stress disorder and obstructive sleep apnea syndromePsychosomatics19983921681719584544
- El-SolhAAVermontLHomishGGKufelTThe effect of continuous positive airway pressure on post-traumatic stress disorder symptoms in veterans with post-traumatic stress disorder and obstructive sleep apnea: a prospective studySleep Med20173314515028449895
- OrrJESmalesCAlexanderTHTreatment of OSA with CPAP is associated with improvement in PTSD symptoms among VeteransJ Clin Sleep Med2017131576327707436
- LettieriCJWalterRJGroup education on CPAP – a responseJ Clin Sleep Med20139997597623997713
- LettieriCJWilliamsSGCollenJFOSA syndrome and posttraumatic stress disorder: clinical outcomes and impact of positive airway pressure therapyChest2016149248349026291560
- CollenJFLettieriCJHoffmanMThe impact of posttraumatic stress disorder on CPAP adherence in patients with obstructive sleep apneaJ Clin Sleep Med20128666767223243400
- El-SolhAAAyyarLAkinnusiMReliaSAkinnusiOPositive airway pressure adherence in veterans with posttraumatic stress disorderSleep201033111495150021102991
- SawyerAMGooneratneNSMarcusCLOferDRichardsKCWeaverTEA systematic review of CPAP adherence across age groups: clinical and empiric insights for developing CPAP adherence interventionsSleep Med Rev201115634335621652236
- ChenXChenWHuWHuangKHuangJZhouYNurse-led intensive interventions improve adherence to continuous positive airway pressure therapy and quality of life in obstructive sleep apnea patientsPatient Prefer Adherence201591707171326648703
- La PianaGEScartabellatiAChiesaLLong-term adherence to CPAP treatment in patients with obstructive sleep apnea: importance of educational programPatient Prefer Adherence2011555556222114470
- KovacevicIWallaceDMVargasSSShafazandSPAP compliance in hispanic veterans with psychiatric disordersSleep201134A252
- LajosLEMolinaPEImSSGonzalesTAGarzaPCIngmundsonPTContinuous positive airway pressure adherence among veterans with and without posttraumatic stress disorderSleep200427A228
- MeansMKUlmerCSEdingerJDEthnic differences in continuous positive airway pressure (CPAP) adherence in veterans with and without psychiatric disordersBehav Sleep Med20108426027320924838
- StepnowskyCJJrBardwellWAMoorePJAncoli-IsraelSDimsdaleJEPsychologic correlates of compliance with continuous positive airway pressureSleep200225775876212405612
- AloiaMSArnedtJTStepnowskyCHechtJBorrelliBPredicting treatment adherence in obstructive sleep apnea using principles of behavior changeJ Clin Sleep Med20051434635317564399
- BudhirajaRParthasarathySDrakeCLEarly CPAP use identifies subsequent adherence to CPAP therapySleep200730332032417425228
- SmithSSLangCPSullivanKAWarrenJA preliminary investigation of the effectiveness of a sleep apnea education programJ Psychosom Res200456224524915016585
- WickwireEMLettieriCJCairnsAACollopNAMaximizing positive airway pressure adherence in adults: a common-sense approachChest2013144268069323918114
- StepnowskyCJDimsdaleJEDose-response relationship between CPAP compliance and measures of sleep apnea severitySleep Med20023432933414592195
- StepnowskyCJJrMoorePJNasal CPAP treatment for obstructive sleep apnea: developing a new perspective on dosing strategies and complianceJ Psychosom Res200354659960512781315
- AnticNACatchesidePBuchanCThe effect of CPAP in normalizing daytime sleepiness, quality of life, and neurocognitive function in patients with moderate to severe OSASleep201134111111921203366
- FaccendaJFMackayTWBoonNADouglasNJRandomized placebo-controlled trial of continuous positive airway pressure on blood pressure in the sleep apnea-hypopnea syndromeAm J Respir Crit Care Med2001163234434811179104
- KingshottRNVennelleMHoyCJEnglemanHMDearyIJDouglasNJPredictors of improvements in daytime function outcomes with CPAP therapyAm J Respir Crit Care Med20001613 Pt 186687110712335
- StradlingJRDaviesRJIs more NCPAP better?Sleep200023Suppl 4S150S15310893091
- WeaverTEMaislinGDingesDFRelationship between hours of CPAP use and achieving normal levels of sleepiness and daily functioningSleep200730671171917580592
- KrakowBUlibarriVAFoley-SheaMRTidlerAMcIverNDAdherence and subthreshold adherence in sleep apnea subjects receiving positive airway pressure therapy: a retrospective study evaluating differences in adherence versus useRespir Care20166181023103227118876
- AndersonLIn Search of ComplianceBirminghamCahaba Media Group, Home Care2012
- KrakowBUlibarriVMelendrezDKiktaSTogamiLHaynesPA daytime, abbreviated cardio-respiratory sleep study (CPT 95807-52) to acclimate insomnia patients with sleep disordered breathing to positive airway pressure (PAP-NAP)J Clin Sleep Med20084321222218595433
- CollimoreKCMcCabeRECarletonRNAsmundsonGJMedia exposure and dimensions of anxiety sensitivity: differential associations with PTSD symptom clustersJ Anxiety Disord20082261021102818093798
- KiliçEZKiliçCYilmazSIs anxiety sensitivity a predictor of PTSD in children and adolescents?J Psychosom Res2008651818618582616
- KotelesFDoeringBKThe many faces of somatosensory amplification: the relative contribution of body awareness, symptom labeling, and anxietyJ Health Psychol201621122903291126060240
- NakaoMBarskeyAJClinical application of somatosensory amplification in psychosomatic medicineBiopsychosoc Med200711717371572
- YavuzBGAydinlarEIDikmenPYIncesuCAssociation between somatic amplification, anxiety, depression, stress and migraineJ Headache Pain2013145323799958
- SandersMHKernNObstructive sleep apnea treated by independently adjusted inspiratory and expiratory positive airway pressures via nasal mask. Physiologic and clinical implicationsChest19909823173242198134
- KushidaCAChediakABerryRBClinical guidelines for the manual titration of positive airway pressure in patients with obstructive sleep apneaJ Clin Sleep Med20084215717118468315
- CasasIde la CalzadaMDGuitartMRocaADiagnastico y tratamiento de fobia a la terapia con presion nasal positiva continua de aire [Diagnosis and treatment of the phobia due to treatment with air using nasal continuous pressure]Rev Neurol2000306593596 Spanish10863736
- ChasensERPackAIMaislinGDingesDFWeaverTEClaustrophobia and adherence to CPAP treatmentWest J Nurs Res200527330732115781905
- EdmondsJCYangHKingTSSawyerDARizzoASawyerAMClaustrophobic tendencies and continuous positive airway pressure therapy non-adherence in adults with obstructive sleep apneaHeart Lung201544210010625744632
- KrakowBSound Sleep, Sound Mind: 7 Keys to Sleeping through the NightNew YorkJohn Wiley & Sons2007
- BillingsMEKapurVKMedicare long-term CPAP coverage policy: a cost-utility analysisJ Clin Sleep Med20139101023102924127146
- WangJWangYFengJChenBYCaoJComplex sleep apnea syndromePatient Prefer Adherence2013763364123861580
- KrakowBUlibarriVAMcIverNDReversal of PAP failure with the REPAP retitration protocolRespir Care201762439640828223464
- KrakowBUlibarriVAMcIverNDNadorffMRA novel therapy for chronic sleep-onset insomnia: a retrospective, nonrandomized controlled study of auto-adjusting, dual-level, positive airway pressure technologyPrim Care Companion CNS Disord2016185
- KrakowBUlibarriVARomeroEAThomasRJMcIverNDAdaptive servo-ventilation therapy in a case series of patients with co-morbid insomnia and sleep apneaJ Sleep Disord Treat Care201321110
- SuMZhangXHuangMDingNAdaptive pressure support servoventilation: a novel treatment for residual sleepiness associated with central sleep apnea eventsSleep Breath201115469569920862555
- KrakowBMelendrezDWarnerTDDorinRHarperRHollifieldMTo breathe, perchance to sleep: sleep-disordered breathing and chronic insomnia among trauma survivorsSleep Breath20026418920212524572
- KrakowBMelendrezDHaynesPIntegrating psychosocial and biomedical CPAP adherence models. A commentary on: “Improving CPAP use by patients with the sleep apnea/hypopnea syndrome (SAHS)” (HM Engleman & MR Wild)Sleep Med Rev20037544144414573379
- KrakowBMelendrezDLeeSAWarnerTDClarkJOSklarDRefractory insomnia and sleep-disordered breathing: a pilot studySleep Breath200481152915026935
- KrakowBJMelendrezDCJohnstonLGSleep Dynamic Therapy for Cerro Grande Fire evacuees with posttraumatic stress symptoms: a preliminary reportJ Clin Psychiatry200263867368412197447
- KrakowBMelendrezDWarnerTDSigns and symptoms of sleep-disordered breathing in trauma survivors: a matched comparison with classic sleep apnea patientsJ Nerv Ment Dis2006194643343916772861
- KrakowBKrakowJUlibarriVAMcIverNDFrequency and accuracy of “RERA” and “RDI” terms in the Journal of Clinical Sleep Medicine from 2006 through 2012J Clin Sleep Med201410212112424532993
- KrakowBUlibarriVASanchezJNKiktaSMcIverNMelendrezDDriving on “auto”: hands-on is more effective than hands-freeJ Clin Sleep Med20128334334422701395
- MeansMKEdingerJDGraded exposure therapy for addressing claustrophobic reactions to continuous positive airway pressure: a case series reportBehav Sleep Med20075210511617441781
- American Academy of Sleep MedicineInternational Classification of Sleep Disorders: Diagnostic & Coding Manual2nd edWestchesterAmerican Academy of Sleep Medicine2005
- FoaEBRiggsDSDancuCVRothbaumBOReliability and validity of a brief instrument for assessing posttraumatic stress disorderJ Trauma Stress199364459473
- KuzniarTJGolbinJMMorgenthalerTIMoving beyond empiric continuous positive airway pressure (CPAP) trials for central sleep apnea: a multi-modality titration studySleep Breath200711425926617541664
- WangYGeaterAFChaiYPre- and in-therapy predictive score models of adult OSAS patients with poor adherence pattern on nCPAP therapyPatient Prefer Adherence2015971572326064041
- McArdleNDevereuxGHeidarnejadHEnglemanHMMackayTWDouglasNJLong-term use of CPAP therapy for sleep apnea/hypopnea syndromeAm J Respir Crit Care Med19991594 Pt 11108111410194153
- Reeves-HocheMKMeckRZwillichCWNasal CPAP: an objective evaluation of patient complianceAm J Respir Crit Care Med199414911491548111574
- WeaverTEKribbsNBPackAINight-to-night variability in CPAP use over the first three months of treatmentSleep19972042782839231953
- CondosRNormanRGKrishnasamyIPeduzziNGoldringRMRapoportDMFlow limitation as a noninvasive assessment of residual upper-airway resistance during continuous positive airway pressure therapy of obstructive sleep apneaAm J Respir Crit Care Med199415024754808049832
- StanchinaMRobinsonKCorraoWDonatWSandsSMalhotraAClinical use of loop gain measures to determine continuous positive airway pressure efficacy in patients with complex sleep apnea. A pilot studyAnn Am Thorac Soc20151291351135726214564
- KrakowBMcIverNDUlibarriVANadorffMRRetrospective, non-randomized controlled study on autoadjusting, dual-pressure positive airway pressure therapy for a consecutive series of complex insomnia disorder patientsNat Sci Sleep20179819528331381
- BrooksRTrimbleMThe future of sleep technology: report from an American Association of Sleep Technologists summit meetingJ Clin Sleep Med201410558959324812546
- WangYGaoWSunMChenBAdherence to CPAP in patients with obstructive sleep apnea in a Chinese populationRespir Care201257223824321762553