Abstract
Development of bone metastases in patients with advanced cancer is associated with skeletal-related events (SREs) such as pathologic fractures, spinal cord compression, the requirement for surgery or palliative radiotherapy to bone, and hypercalcemia of malignancy. Skeletal morbidity may reduce patient mobility, limit functional independence, and impair quality of life (QOL). Proactive management of new or worsening bone pain or motor impairment is crucial because of the potential for rapid progression of symptoms. Administration of bisphosphonate therapy as a monthly infusion to patients with bone metastases prevents or delays the onset and reduces the frequency of SREs and provides clinically meaningful improvements in bone pain and QOL. In addition to administration of therapy, the monthly infusion visit allows a dedicated team of healthcare professionals to regularly assess SREs, response to therapy, adverse events (AEs), QOL, and adherence to oral medications and supplements. The continuity of care that occurs during the monthly infusion visit provides oncology nurses with an opportunity to educate patients about effective strategies to manage SREs and AEs. In addition, regular interaction provides oncology nurses with an opportunity to recognize and proactively address subtle changes in the patients’ medical condition. Using a multidisciplinary medical team also eliminates barriers between the various healthcare professionals involved in patient management. Consequently, the monthly infusion visit can result in effective patient management and improved clinical outcomes in patients with malignant bone disease.
Introduction
Bone metastases are common in patients with advanced solid tumors, with estimates ranging from 20% to 25% for renal cell carcinoma (RCC) and 65% to 75% for breast or prostate cancer.Citation1 Moreover, bone lesions are almost inevitable in patients with refractory multiple myeloma. Malignant bone disease is associated with considerable morbidity and can result in skeletal-related events (SREs) such as pathologic fractures, spinal cord compression, the requirement for surgery or palliative radiotherapy to bone, and hypercalcemia of malignancy.Citation1 Approximately 50% of patients with bone metastases develop SREs, with patients experiencing an average of 1.5 to 4.0 events per year, depending on the primary cancer.Citation2,Citation3 Each type of SRE is associated with reductions in patient quality of life (QOL), and fractures are also associated with decreased survival.Citation4,Citation5
Current options for preventing the development of SREs from bone metastases in patients with advanced cancer include chemotherapy, radiotherapy, surgery, and bisphosphonates. Although management of the primary malignancy is the cornerstone of therapy, bone metastases represent a long-term challenge and often result in symptoms despite effective anticancer therapies.Citation1 Bisphosphonates are potent inhibitors of osteoclast-mediated bone resorption that can lower SRE risks throughout the disease course. Among the bisphosphonate agents, pamidronate and zoledronic acid are approved for multiple myeloma; pamidronate, zoledronic acid, clodronate (outside the United States), and ibandronate are approved for breast cancer; and zoledronic acid is approved for managing bone lesions secondary to a broad range of solid tumors, including prostate and lung cancer.Citation6–Citation9 Bisphosphonate therapy not only reduces the risk of SREs, but can also decrease bone pain and improve QOL in patients with malignant bone disease.Citation1,Citation10
Bisphosphonate therapy is generally administered as a monthly intravenous infusion in a hospital or infusion clinic, with infusion times ranging from 15 minutes for zoledronic acid to 120 minutes for pamidronate and up to 150 minutes for ibandronate.Citation6,Citation7,Citation9 In our facility, we take advantage of the monthly infusion visit to earmark time for interaction between patients and a dedicated team of healthcare professionals. This interaction provides the opportunity to regularly assess SREs, response to therapy, adverse events (AEs), QOL, and treatment adherence. Regular patient interaction is important because the effects of cancer and cancer treatments can vary greatly over the course of only a few weeks. A monthly infusion visit, such as that for bisphosphonates, provides a well-timed window of opportunity for proactive patient management.
Personalized treatment plans are becoming an increasingly common approach for managing bone metastases in patients with advanced cancer. At King’s College Hospital, one of the largest teaching hospitals in London, the Urology Department is a major referral center that cares for many patients with genitourinary cancers (eg, prostate, kidney, bladder, testicular, and penile cancer). Personalized treatment plans are developed for each patient by members of a dedicated multidisciplinary team, and suggested treatment options are discussed with the patient before the treatment plan is finalized. Nurses play a key role in implementing treatment plans. Based on the experience at King’s College Hospital, personalized treatment plans can improve patient care and clinical outcomes of malignant bone disease.
This review article discusses the opportunities afforded by the monthly infusion visit for managing bone metastases secondary to advanced cancer. Selected case studies demonstrating how the monthly infusion visit can be used to improve patient management are also presented.
Benefits of the monthly infusion visit
Regular interaction between patients and a dedicated healthcare professional team results in more effective patient management, and a monthly infusion visit can be used for patient follow-up assessments. In a managed-care setting, the allocation of nursing resources for infusional medicine provides an opportunity for structured follow-up. In particular, the continuity of care that occurs during the monthly infusion visit establishes a relationship of trust between the patient and the oncology nurse, fostering open and effective communication. Regularly scheduled visits are especially conducive to establishing this relationship because of allocated infusion chair occupancy time, in contrast with the typical time constraints during regular office visits with a physician. In the case of the patient with advanced cancer attending for a monthly bisphosphonate infusion visit, the oncology nurse can also evaluate the patient’s condition and educate the patient regarding the importance of SRE management, potential AEs, and the importance of taking calcium and vitamin D supplements and remaining hydrated. As a result of this regular interaction, the oncology nurse becomes the “expert” on a specific patient and will recognize subtle changes in the patient that could easily be missed by other healthcare professionals. The multidisciplinary nature of the medical team also promotes a more effective working relationship between the various cancer specialists in the infusion clinic. For example, in our facility, the absence of formal barriers between team members allows the oncology nurse to speak directly to the radiation oncologist about a patient needing palliative radiotherapy instead of seeking a referral. This helps to reduce treatment delays and can have a positive effect on patient care and clinical outcomes. The monthly infusion visit can also reduce outpatient appointments and provide an opportunity for oncology nurses to interact with family members and caregivers.
Skeletal-related events
King’s College Hospital has developed a patient-management process to leverage regular infusion visits as an opportunity to more effectively monitor patients. Early identification of new or worsening skeletal morbidity is crucial in patients with malignant bone disease, in whom symptoms may progress very rapidly. Effective treatment to prevent or delay onset and to minimize the severity of SREs plays an important role in the supportive care of patients with bone metastases.
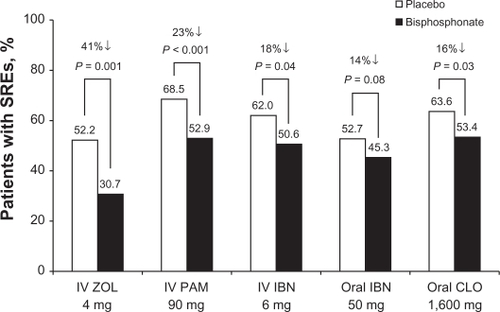
In facilities that treat patients with advanced malignancies, infusion nurses become very familiar with treatment options that span a large range of cancer types. Bisphosphonates are an established component of therapy for patients with bone metastases, which are common in most advanced malignancies.Citation11 Among bisphosphonates approved in the UK for preventing SREs from bone metastases in patients with breast cancer (ie, clodronate, ibandronate, pamidronate, and zoledronic acid), zoledronic acid generated the largest reduction in SRE risk relative to placebo ().Citation10,Citation12–Citation19 Furthermore, zoledronic acid significantly reduced the cumulative mean incidence of SREs in patients with bone metastases from breast cancer (17.8%; P = 0.05 vs pamidronate), prostate cancer (35.3%; P = 0.002 vs placebo), or lung cancer or other solid tumors (26.9%; P = 0.025 vs placebo).Citation20 These results illustrate the benefit of therapy with bisphosphonates in patients with malignant bone disease.
Figure 1 Overall risk of skeletal-related events in patients with bone metastases from breast cancer treated with bisphosphonates.Citation12–Citation19 Hypercalcemia was not included as a skeletal-related event (SRE) in this analysis.
Copyright © 2005. Reproduced with permission of Cochrane Collaboration. Pavlakis N, Schmidt R, Stockler M. Bisphosphonates for breast cancer. Cochrane Database Syst Rev. 2005(3):CD003474.Citation10
As part of each monthly bisphosphonate infusion visit, the patient is thoroughly evaluated for the development of new or worsening SREs, and effective management strategies should be discussed if any are detected. Bone pain is one of the most common complications of bone metastases and tends to occur throughout the course of the disease.Citation21 Managing bone pain generally involves concomitant administration of focal radiotherapy and analgesic medications, especially steroids and nonsteroidal anti-inflammatory agents, although effective pain management may require opioids in some cases.Citation22 Radiotherapy to bone is standard therapy for palliation of malignant bone pain refractory to standard pharmacologic interventions. Nonpharmacologic interventions may include heat and cold applications, massage, relaxation exercises, and therapeutic mattresses.Citation23 Spinal cord compression presents initially as back pain and may cause irreversible paraparesis or paraplegia if left untreated. Early diagnosis, administration of high-dose corticosteroids, and urgent referral for radiotherapy or decompression and spinal stabilization are key for successful rehabilitation.Citation21 Pathologic fractures and hypercalcemia of malignancy are relatively late complications of bone metastases that may require urgent treatment.Citation21,Citation24 Pathologic fractures occur because of loss of bone integrity, thereby resulting in increased bone pain and the need for surgical intervention.Citation21 Identifying weakened weight-bearing bones at high risk for fracture can allow proactive treatment and fixation, sparing patients from potentially life-threatening fractures. Hypercalcemia of malignancy frequently remains undiagnosed and, left untreated, may result in acute renal failure, cardiac arrest, or death.Citation24
The beneficial effects of the monthly infusion visit on SRE management are illustrated by a recent patient case study from King’s College Hospital. A 72-year-old man initially presented to his general practitioner with lower urinary tract symptoms including nocturia. The patient had an abnormal prostate on rectal examination and elevated prostate-specific antigen levels (207.3 ng/L). Biopsy results revealed prostate adenocarcinoma (Gleason score 5 + 5). Based on a multidisciplinary team review of the patient’s histology and radiology results, hormone therapy was initiated, and intravenous bisphosphonate therapy was recommended. During a subsequent monthly visit to the nurse-led bone support clinic for consideration of bisphosphonate therapy, the patient complained to the clinical nurse specialist of experiencing pain in his left hip, which he described as a “constant ache” when walking that was relieved by sitting. The patient was diagnosed with an osteoblastic lesion in the peritrochanter-proximal femur that was associated with mechanical pain. Subsequent assessment by the clinical nurse specialist using the Mirels assessment tool for diagnosis of impending pathologic fracture risk resulted in a score of 9 out of a possible total of 12, and the patient was estimated to have a 33% risk of incurring a pathologic fracture. The clinical nurse specialist referred the patient directly to an orthopedic surgeon, who admitted the patient the same day under their care and performed prophylactic surgical fixation of the femoral neck. A radiation oncologist also recommended palliative radiotherapy to relieve bone pain.
Response to therapy
The monthly infusion visit also provides healthcare professionals with an opportunity to regularly assess how the patient is responding to the current treatment regimen. Decreases in the patient’s well-being can be rapidly reported to other members of the multidisciplinary team so that adjustments to dose and/or schedule as well as modification of the individual components in the treatment regimen can be rapidly implemented to optimize clinical outcomes.
Adverse events
Intravenous therapy is generally administered by the nursing staff in most hospitals and infusion centers. As a result, the nursing staff play a central role in the safety and comfort of patients receiving intravenous therapy. For example, in addition to ensuring that bisphosphonates are administered in a safe and consistent manner, the monthly infusion visit allows the oncology nurse to educate the patient about potential AEs associated with therapy. Improved communication stemming from the regular interaction between the patient and the oncology nurse also encourages early reporting of AEs and implementation of effective management strategies.
There are key monitoring steps for the administration of any intravenous medication that provide important insight into the patient’s well-being. For example, before administering the intravenous infusion, the nursing staff must ensure that the patient is adequately hydrated ().Citation2,Citation25,Citation26 For agents cleared by renal filtration, such as bisphosphonates, serum creatinine levels should be within acceptable ranges to minimize the possibility of renal deterioration. Renal impairment is common among the elderly, and many cancer therapies can adversely affect renal function. Therefore, the monthly visit provides an excellent opportunity for ongoing monitoring of renal function. This is also a good time to remind patients to take recommended supplements (such as calcium or vitamin D for bisphosphonate-treated patients) or to follow dietary restrictions.Citation25,Citation26
Table 1 Guidelines for administering bisphosphonate therapy
During an infusion, patients can be counseled on proactive AE management. For example, bone pain, nausea, fatigue, and fever are the most common AEs reported in bisphosphonate-treated patients.Citation27 Acute flu-like symptoms, which commonly occur after initial exposure to bisphosphonate agents, are related to activation of γδ T cells and the subsequent release of pyrogenic cytokines such as tumor necrosis factor-alpha and interleukin-6.Citation28 Because acute flu-like symptoms are associated with immune system activation, their occurrence may be predictive of response to therapy. These symptoms are generally mild, transient, and manageable with standard analgesic medications.Citation27,Citation29 Because all intravenous bisphosphonates are associated with dose- and infusion-rate–dependent effects on renal function, serum creatinine should be assessed before each infusion. The baseline serum creatinine clearance rate should be measured before the first intravenous bisphosphonate infusion, and the dose adjusted if needed. Treatment should be administered in no less than the recommended infusion times. Shorter infusion times and higher doses of bisphosphonates may increase the risk of renal AEs.Citation27,Citation29 Osteonecrosis of the jaw (ONJ), characterized by exposed bone in the maxillofacial area that occurs spontaneously or after dental surgery in the absence of metastatic disease in the jaw or osteoradionecrosis, with no evidence of healing after 6 weeks of appropriate dental care, has been reported as an uncommon AE in patients receiving complex treatment regimens including bisphosphonates. Approximately 1% of patients in the advanced cancer setting and 0.2% of patients in the adjuvant cancer setting develop ONJ.Citation30–Citation34 Implementing proactive dental surveillance and completing necessary dental work before administering bisphosphonate therapy reduces the incidence of ONJ, and early identification and management of this condition may improve healing.Citation35,Citation36 The monthly visit allows follow-ups on dental health issues. Recommended supportive care measures for managing AEs associated with bisphosphonate therapy are presented in .Citation2,Citation25,Citation26
Quality of life
Inadequate pain management may result in reductions in patient mobility, functional independence, and QOL. Interactions during the monthly infusion visit allow the oncology nurse to conduct regular QOL assessments that monitor the patient’s well-being and ability to function during daily activities. Any QOL deterioration or performance status reduction should prompt evaluation of whether modification of palliative therapy is necessary.
Oncology nurses can use various instruments, including QOL questionnaires and patient diaries, to assess the QOL of patients with advanced cancer. The European Organisation for Research and Treatment of Cancer (EORTC) QOL Questionnaire Group Bone Metastases Module (QLQ-BM22) is a newly developed QOL questionnaire that captures symptoms and morbidities specific to bone metastases that were not included in the previous QOL questionnaire (EORTC QLQ-C30).Citation37,Citation38 The new questionnaire consists of 22 items, rated on a scale from 1 (not at all) to 4 (very much), that evaluate a patient’s experience during the previous week regarding painful sites and pain characteristics, as well as functional limitations and psychosocial concerns associated with pain ().Citation38 The EORTC QLQ-BM22, which is currently undergoing additional clinical validation, will enable bone-metastasis–related QOL outcomes to be compared across treatment regimens and will assist in selecting appropriate treatment interventions.
Table 2 Issues included in the Bone Metastases Quality of Life Questionnaire (EORTC QLQ-BM22)
Use of a patient diary for recording pain scores, changes in mobility, and AEs may also facilitate interaction between the patients and the oncology nurse during the monthly infusion visit.Citation25 As part of an ongoing record of patient progress, information should be recorded in the patient diary before or during each infusion visit and should be compared with baseline information obtained before treatment was initiated. Research-based evidence highlights the importance of using a patient diary for assessing and managing pain. Regular use of a patient diary heightens a patient’s awareness of pain patterns, guides pain management behavior, confers a sense of control over pain, and facilitates communication with healthcare professionals.Citation23,Citation39 Use of a patient diary may also assist patients in recognizing early, more subtle benefits of therapy, resulting in improved treatment adherence. Patient diaries may also help oncology nurses to identify when appropriate interventions are necessary to enhance QOL.
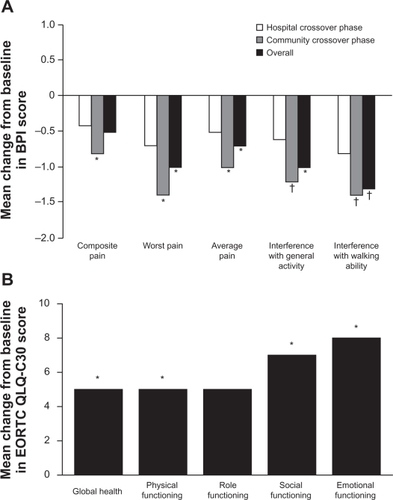
During the monthly infusion visit, the oncology nurse can recommend several interventions to reduce pain and maintain QOL. As previously described, managing bone pain generally involves administering analgesic medications or palliative radiotherapy to patients with refractory bone pain. Bisphosphonate therapy is also associated with clinically meaningful palliation of bone pain. Administering zoledronic acid as a monthly infusion to patients with bone metastases from breast cancer is associated with reduced pain and improved QOL.Citation40,Citation41 In a cross-over study wherein zoledronic acid was administered to patients with cancer, either in a hospital or community setting, pain and QOL were prospectively evaluated by trained nurses. Analysis of Brief Pain Inventory scores revealed that zoledronic acid improved scores from baseline for composite pain, worst pain, and average pain; zoledronic acid also reduced the overall extent to which pain interfered with general activities and walking ability (N = 101; P ≤ 0.05; ).Citation40 Significant improvements from baseline in global health and in physical, social, and emotional functioning, as assessed using EORTC QLQ-C30, were also observed in patients receiving zoledronic acid therapy (N = 101; P < 0.05 vs baseline; ).Citation40 The observed QOL improvements suggest that administration of zoledronic acid as a monthly intravenous infusion has the ability to maintain patient mobility and functional independence. A Cochrane meta-analysis of 30 randomized clinical studies of bisphosphonates for relief of pain secondary to bone metastases recommended their use for diffuse, painful metastases, especially when analgesics with or without radiotherapy failed to provide adequate pain relief or produced unacceptable adverse drug reactions (N = 3682).Citation42 Indeed, bisphosphonate therapy should be considered for pain management in all patients with bone metastases because they are the only approved class of supportive pharmacotherapy capable of relieving pain and affecting the underlying pathophysiology of bone metastases–malignant osteolysis.Citation2 Oncology nurses can also educate patients about how to modify their lifestyle to reduce the risk of a fracture (eg, incorporating modifications in their environment to prevent falls).Citation25,Citation26
Figure 2 A) Effect of monthly infusion of zoledronic acid on pain. *P < 0.05; †P < 0.005 versus baseline. B) Effect of monthly infusion of zoledronic acid on quality of life. *P < 0.05 versus baseline.
A recent case study illustrates how incorporating individual patient preferences into management plans for malignant bone disease may preserve QOL. Two patients with RCC presented with bone metastases on the lower leg; surgical amputation was recommended based on an orthopedic evaluation. The first patient underwent leg amputation and subsequently required ambulatory support for the rest of his life. The second patient, a 68-year-old woman with bone metastases on the right tibia, refused amputation and instead elected to receive radiotherapy, zoledronic acid, dexamethasone, and opioid analgesics. After 4 weeks, she reported reduced pain and was able to walk with the assistance of crutches instead of a walking frame. After 12 weeks, the patient’s N-telopeptide of type I collagen levels normalized, indicating a reduction in malignant osteolysis. Notably, the patient sustained no fractures and did not require increased analgesic use before succumbing to her disease approximately 7 months after initiation of radiotherapy and zoledronic acid.Citation43 The potential of radiotherapy plus zoledronic acid to restore function in bone affected by aggressive tumors is an important consideration for preserving mobility and QOL in patients with limited therapeutic options.
Treatment adherence
One concern with long-term therapies is patients’ ongoing adherence to dosing protocols. Indeed, this is especially challenging when there is limited tracking of treatment effects. For example, because bisphosphonate therapy is a preventive intervention in patients with bone metastases, patients may lose interest in taking their medication because of the lack of any outward sign of benefit. Administering bisphosphonate therapy as an intravenous infusion improves treatment adherence versus oral therapy and provides an assurance that the patient is receiving the prescribed agent.Citation44 The oncology nurse can also educate the patient about the relationship between treatment adherence, improved clinical outcomes, and prevention of SREs.
Numerous studies have demonstrated that both overall compliance and persistence with oral bisphosphonate therapy are poor among women with osteoporosis. Extending the dosing interval increased adherence; however, gains remained suboptimal. Notably, low compliance and persistence rates consistently resulted in increased fracture rates.Citation45 Intravenous bisphosphonate therapy is generally associated with improved adherence compared with oral bisphosphonate therapy in patients with advanced cancer. A retrospective analysis of a German health-claims database reported that persistency rates (defined as continuous prescription refill without an interruption lasting longer than 30 days) were significantly higher with intravenous bisphosphonates (92%) compared with oral bisphosphonates (36.4%; P = 0.0012).Citation44 A prospective study of 79 women with metastatic breast cancer conducted in the United Kingdom reported that although self-reported adherence to oral bisphosphonate therapy was high, 21% of patients had chosen not to take their medications at some time. Twenty-four percent of patients expressed dissatisfaction with constraints associated with oral bisphosphonate administration, especially the time required to remain upright after taking their medication. In contrast, an overwhelming majority of patients receiving intravenous bisphosphonate therapy were generally satisfied with the frequency (91%) and the convenience (88%) of their medications, especially when administered concurrently with chemotherapy.Citation46
Adherence to intravenous bisphosphonate therapy is associated with improved clinical outcomes among patients with advanced cancer. Analysis of a national medical claims database of patients with solid tumors and bone metastases revealed that administering zoledronic acid according to the recommended continuous dosing regimen (4 mg every 3 to 4 weeks) provided the greatest protection against SREs (0.16 SREs/month vs 0.43 SREs/month with no bisphosphonate therapy). Patients who received zoledronic acid according to less frequent dosing schedules were only partially protected against SREs (0.31 SREs/month; ).Citation47 Administration of zoledronic acid according to the recommended dosing schedule was also associated with a significantly longer duration of follow-up (17.11 months) compared with administration according to nonrecommended dosing schedules (9.93 months) or no treatment (8.68 months; P < 0.001).Citation47 Therefore, administering zoledronic acid based on the recommended continuous dosing schedule reduced the skeletal morbidity rate and increased follow-up duration, suggesting increased survival among patients with malignant bone disease.
Table 3 Effect of zoledronic acid on skeletal morbidity rate in patients with solid tumors and bone metastases
Regular interaction between the patient and the oncology nurse in the infusion center fosters adherence to therapy protocols. The oncology nurse is uniquely positioned to educate the patient and his/her caregivers and to reinforce the importance of continuous therapy for managing metastatic bone disease and associated SREs. Patient education is especially important because poor adherence to bisphosphonate therapy is frequently caused by the patient not understanding how the medication works or why it needs to be taken on a continuous basis. The oncology nurse should explain that prematurely discontinuing bisphosphonate therapy leaves the patient at risk for painful and debilitating SREs, which reduce functional independence and impair activities of daily living.Citation48 By highlighting the benefits of administering bisphosphonates according to recommended dosing schedules and enacting established supportive care protocols to ensure patient safety and comfort, oncology nurses may increase patients’ persistence with and adherence to bisphosphonate therapy.
Clinical outcomes
An infusion visit also allows for discussion of the latest clinical news about the patient’s regimen, such as identification of new potential risks or benefits. Patients often enquire about new data from the common media or information on their current medications that their family members access on the Internet. For example, bisphosphonates have been in the news recently because of an association with improved clinical outcomes among patients with early or advanced cancer. In the AZURE trial, the effects of adding zoledronic acid to standard neoadjuvant and adjuvant chemotherapy for early breast cancer are being evaluated. In the subgroup of patients who received neoadjuvant chemotherapy, adding monthly zoledronic acid reduced residual invasive tumor size compared with chemotherapy alone (P = 0.006; n = 205).Citation49 The pathologic complete response rate (breast and axilla) was also higher among patients treated with zoledronic acid plus chemotherapy (11.7%) compared with chemotherapy alone (6.9%; P = 0.146). Several studies reported that zoledronic acid improved overall survival among patients with various types of advanced cancer including multiple myeloma, bladder cancer, and lung cancer.Citation50–Citation52 In the largest of these studies, the Medical Research Council Myeloma IX study, zoledronic acid significantly improved overall survival (P = 0.0118) and progression-free survival (P = 0.0179) versus clodronate in patients with newly diagnosed multiple myeloma (N = 1960).Citation50 Furthermore, subset analyses of 2 phase III clinical studies revealed that zoledronic acid prolonged survival compared with placebo among patients with solid tumors who had high baseline N-telopeptide of type I collagen levels.Citation53,Citation54 Survival benefits appeared to be independent of SRE prevention, suggesting that zoledronic acid may improve survival via anticancer activity.Citation50,Citation53,Citation54
Recently, administering zoledronic acid with endocrine therapy for early breast cancer also resulted in apparent anticancer benefits. In this low-disease-burden setting, zoledronic acid was administered every 6 months. In the ABCSG-12 study, adding zoledronic acid to adjuvant endocrine therapy resulted in a relative reduction of 36% in the risk of disease progression compared with endocrine therapy alone in premenopausal women with early breast cancer (hazard ratio [HR] = 0.64; P = 0.01; N = 1803).Citation55 Patients treated with zoledronic acid experienced fewer events of locoregional and distant recurrence, bone metastases, and disease in the contralateral breast. In the ZO-FAST (N = 1065) and Z-FAST (N = 602) studies, immediate addition of zoledronic acid to adjuvant letrozole reduced disease recurrence in postmenopausal women with early breast cancer (HR = 0.59 [P = 0.0176] and HR = 0.8 [P = not significant] for immediate vs delayed zoledronic acid, respectively).Citation34
Moreover, recent retrospective database analyses revealed that administration of bisphosphonates for postmenopausal osteoporosis is associated with lower rates of invasive breast cancer.Citation56–Citation58 Therefore, discussion of these new results of bisphosphonate therapy may also provide a positive outlook for patients who may be experiencing challenges with their concomitant anticancer therapies.
Conclusion
Administering bisphosphonate therapy as a monthly intravenous infusion provides healthcare professionals with an opportunity to adopt a holistic approach toward managing malignant bone disease in patients with advanced cancer. During each infusion visit, healthcare professionals can assess SREs, response to therapy, AEs, QOL, and treatment adherence. Proactive management of new or worsening SREs is extremely important in patients with malignant bone disease because symptoms may progress very rapidly. Skeletal morbidity may limit patient mobility, reduce functional independence, and impair QOL. Effective management of SREs plays an important role in the supportive care of patients with bone metastases. Bisphosphonates prevent or delay the onset and decrease the frequency of SREs, thereby reducing bone pain and improving QOL. Administering bisphosphonate therapy as an intravenous infusion is also associated with improved treatment adherence and clinical outcomes compared with oral bisphosphonate therapy in patients with malignant bone disease.Citation50
Regular interaction between patients and a dedicated team of healthcare professionals results in effective management of bone metastases. The continuity of care that occurs during the monthly infusion visit establishes trust between the patient and the oncology nurse, leading to more open and effective communication. As a result of regular interaction, the oncology nurse is uniquely positioned to recognize and respond to subtle changes in the patient’s condition. The monthly infusion visit also provides the oncology nurse with an opportunity to educate the patient about effective strategies to manage SREs and AEs and to maintain QOL. Incorporation of patient preferences into personalized treatment plans is likely to improve patient care and clinical outcomes of malignant bone disease.
Acknowledgements
Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals. I thank Ann Marie Fitzmaurice, PhD, ProEd Communications, Inc., for her medical editorial assistance with this manuscript.
Disclosure
Advisor to Novartis Pharmaceuticals Corporation, Amgen Inc., Ferring, sanofi-aventis, and AstraZeneca.
References
- ColemanREBisphosphonates: clinical experienceOncologist20049Suppl 4142715459426
- FitchMMaxwellCRyanCLothmanHDrudge-CoatesLCostaLBone metastases from advanced cancers: clinical implications and treatment optionsClin J Oncol Nurs200913670171019948468
- LiptonABisphosphonate therapy in the oncology settingExpert Opin Emerg Drugs20038246948814662000
- ColemanREMetastatic bone disease: clinical features, pathophysiology and treatment strategiesCancer Treat Rev200127316517611417967
- LiptonATreatment of bone metastases and bone pain with bisphosphonatesSupport Cancer Ther2007429210018632473
- Aredia [package insert]East Hanover, NJNovartis Pharmaceuticals Corporation2008
- Zometa [package insert]East Hanover, NJNovartis Pharmaceuticals Corporation2009
- Ostac [package insert]Nutley, NJHoffmann-La Roche2004
- Bondronat [summary of product characteristics]Welwyn Garden City, UKRoche Products Ltd2007
- PavlakisNSchmidtRStocklerMBisphosphonates for breast cancerCochrane Database Syst Rev20053CD00347416034900
- AaproMAbrahamssonPABodyJJGuidance on the use of bisphosphonates in solid tumours: recommendations of an international expert panelAnn Oncol200819342043217906299
- KohnoNAogiKMinamiHZoledronic acid significantly reduces skeletal complications compared with placebo in Japanese women with bone metastases from breast cancer: a randomized, placebo-controlled trialJ Clin Oncol200523153314332115738536
- HortobagyiGNTheriaultRLPorterLEfficacy of pamidronate in reducing skeletal complications in patients with breast cancer and lytic bone metastases. Protocol 19 Aredia Breast Cancer Study GroupN Engl J Med199633524178517918965890
- HortobagyiGNTheriaultRLLiptonALong-term prevention of skeletal complications of metastatic breast cancer with pamidronate. Protocol 19 Aredia Breast Cancer Study GroupJ Clin Oncol1998166203820449626201
- BodyJJDielIJLichinitserMRIntravenous ibandronate reduces the incidence of skeletal complications in patients with breast cancer and bone metastasesAnn Oncol20031491399140512954579
- BodyJJDielIJBellROral ibandronate improves bone pain and preserves quality of life in patients with skeletal metastases due to breast cancerPain2004111330631215363874
- KristensenBEjlertsenBGroenvoldMHeinSLoftHMouridsenHTOral clodronate in breast cancer patients with bone metastases: a randomized studyJ Intern Med19992461677410447227
- PatersonAHPowlesTJKanisJAMcCloskeyEHansonJAshleySDouble-blind controlled trial of oral clodronate in patients with bone metastases from breast cancerJ Clin Oncol199311159658418243
- Tubiana-HulinMBeuzebocPMauriacL[Double-blinded controlled study comparing clodronate versus placebo in patients with breast cancer bone metastases]Bull Cancer200188770170711495824
- MajorPPCookRJChenBLZhengMSurvival-adjusted multiple-event analysis for the evaluation of treatment effects of zoledronic acid in patients with bone metastases from solid tumorsSupport Cancer. Ther20052423424018628179
- ColemanRESkeletal complications of malignancyCancer1997808 Suppl158815949362426
- PayneRPharmacologic management of bone pain in the cancer patientClin J Pain19895Suppl 2S43S49 discussion follows.2520440
- ReichCDAdvances in the treatment of bone metastasesClin J Oncol Nurs20037664164614705479
- BarnettMLHypercalcemiaSemin Oncol Nurs199915319020110461704
- MaxwellCRole of the nurse in preserving patients’ independenceEur J Oncol Nurs200711Suppl 2S38S4117768093
- MaxwellCSwiftRGoodeMDoaneLRogersMAdvances in supportive care of patients with cancer and bone metastases: nursing implications of zoledronic acidClin J Oncol Nurs20037440340812929273
- RosenLSGordonDKaminskiMZoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trialCancer J20017537738711693896
- DielIJBergnerRGrotzKAAdverse effects of bisphosphonates: current issuesJ Support Oncol200751047548218240669
- BerensonJRRosenLSHowellAZoledronic acid reduces skeletal-related events in patients with osteolytic metastasesCancer20019171191120011283917
- HoffAOTothBBAltundagKFrequency and risk factors associated with osteonecrosis of the jaw in cancer patients treated with intravenous bisphosphonatesJ Bone Miner Res200823682683618558816
- McArthurHLEstiloCHurynJOsteonecrosis of the jaw (ONJ) among intravenous (IV) bisphosphonate- and/or bevacizumab-treated patients (pts) at Memorial Sloan-Kettering Cancer Center (MSKCC). [abstract]J Clin Oncol200826Suppl 15523s Abstract 9588.
- HenryDvon MoosRVadhan-RajSA double-blind, randomized study of denosumab versus zoledronic acid for the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. [abstract]Eur J Cancer Suppl20097311 Abstract 20LBA.
- StopeckATLiptonABodyJJDenosumab Compared With Zoledronic Acid for the Treatment of Bone Metastases in Patients With Advanced Breast Cancer: A Randomized, Double-Blind StudyJ Clin Oncol2010118 [Epub ahead of print].
- ColemanRBundredNde BoerRImpact of zoledronic acid in postmenopausal women with early breast cancer receiving adjuvant letrozole: Z-FAST, ZO-FAST, and E-ZO-FAST. [abstract]Cancer Res200969Suppl 24733s Abstract 4082.
- DimopoulosMAKastritisEBamiaCReduction of osteonecrosis of the jaw (ONJ) after implementation of preventive measures in patients with multiple myeloma treated with zoledronic acidAnn Oncol200920111712018689864
- RipamontiCIManiezzoMCampaTDecreased occurrence of osteonecrosis of the jaw after implementation of dental preventive measures in solid tumour patients with bone metastases treated with bisphosphonates The experience of the National Cancer Institute of MilanAnn Oncol200920113714518647964
- ChowEBottomleyAUnderstanding the EORTC QLQ-BM22, the module for patients with bone metastasesExpert Rev Pharmacoecon Outcomes Res20099546146519817529
- ChowEHirdAVelikovaGThe European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire for patients with bone metastases: the EORTC QLQ-BM22Eur J Cancer20094571146115219097882
- SchumacherKLKoresawaSWestCThe usefulness of a daily pain management diary for outpatients with cancer-related painOncol Nurs Forum20022991304131312370700
- WardleyADavidsonNBarrett-LeePZoledronic acid significantly improves pain scores and quality of life in breast cancer patients with bone metastases: a randomised, crossover study of community vs hospital bisphosphonate administrationBr J Cancer200592101869187615870721
- CostaLBadiaXChowELiptonAWardleyAImpact of skeletal complications on patients’ quality of life, mobility, and functional independenceSupport Care Cancer200816887988918392862
- WongRWiffenPJBisphosphonates for the relief of pain secondary to bone metastasesCochrane Database Syst Rev20022CD00206812076438
- Drudge-CoatesLThompsonPMMuirGHBurden of bone metastases from renal cell carcinoma: zoledronic acid and functional independence[poster]Societe Internationale d’Urologie (SIU) World Uro-Oncology Update2008 Nov 19–22Santiago, Chile Abstract UP-18.
- MangiapaneSHoerAGotheHBarghoutVHaeusslerBHigher persistency with i.v. bisphosphonates in patients with bone metastasis. [abstract]J Clin Oncol200624Suppl 18698s Abstract 18623.
- RabendaVHiligsmannMReginsterJYPoor adherence to oral bisphosphonate treatment and its consequences: a review of the evidenceExpert Opin Pharmacother200910142303231519640210
- FallowfieldLStebbingJBraybrookeJLangridgeCJenkinsVThe preferences and experiences of different bisphosphonate treatments in women with breast cancerPsycho-oncology2010524 [Epub ahead of print].
- HatoumHTLinSJSmithMRBarghoutVLiptonAZoledronic acid and skeletal complications in patients with solid tumors and bone metastases: analysis of a national medical claims databaseCancer200811361438144518720527
- FitchMIMaxwellCBisphosphonate therapy for metastatic bone disease: the pivotal role of nurses in patient educationOncol Nurs Forum200835470971318591175
- ColemanREWinterMCCameronDThe effects of adding zoledronic acid to neoadjuvant chemotherapy on tumour response: exploratory evidence for direct anti-tumour activity in breast cancerBr J Cancer201010271099110520234364
- MorganGDaviesFGregoryWEvaluating the effects of zoledronic acid (ZOL) on overall survival (OS) in patients (Pts) with multiple myeloma (MM): Results of the Medical Research Council (MRC) Myeloma IX study. [abstract]J Clin Oncol201029Suppl 15578s Abstract 8021.
- ZaghloulMSBoutrusREl-HossienyHKaderYAEl-AttarINazmyMA prospective, randomized, placebo-controlled trial of zoledronic acid in bony metastatic bladder cancerInt J Clin Oncol201015438238920354750
- ZarogoulidisKBoutsikouEZarogoulidisPThe impact of zoledronic acid therapy in survival of lung cancer patients with bone metastasisInt J Cancer200912571705170919521984
- BodyJ-JCookRCostaLPossible survival benefits from zoledronic acid treatment in patients with bone metastases from solid tumors and poor prognostic features. [poster]The IX International Meeting on Cancer Induced Bone Disease2009 Oct 28–31Arlington, VA Poster 71.
- CostaLCookRBodyJ-JZoledronic acid treatment delays disease progression and improves survival in patients with bone metastases from solid tumors and elevated levels of bone resorption. [poster]The IX International Meeting on Cancer Induced Bone Disease2009 Oct 28–31Arlington, VA Poster 50.
- GnantMMlineritschBSchippingerWEndocrine therapy plus zoledronic acid in premenopausal breast cancerN Engl J Med2009360767969119213681
- RennertGPinchevMRennertHSUse of bisphosphonates and risk of postmenopausal breast cancerJ Clin Oncol201028223577358120567021
- NewcombPATrentham-DietzAHamptonJMBisphosphonates for osteoporosis treatment are associated with reduced breast cancer riskBr J Cancer2010102579980220160722
- ChlebowskiRTChenZCauleyJAOral bisphosphonate use and breast cancer incidence in postmenopausal womenJ Clin Oncol201028223582359020567009