
Abstract
Purpose
Although warfarin has historically been the standard of care for preventing ischemic stroke in patients with nonvalvular atrial fibrillation (NVAF), the use of direct oral anticoagulants (DOACs) is rapidly increasing. In this study, we examined the demographic and clinical characteristics of patients continuing warfarin therapy and investigated reasons for warfarin continuation.
Patients and methods
Each study site consecutively registered 10 patients with NVAF who had been taking warfarin for at least 12 months. Demographic and clinical characteristics and international normalized ratio (INR) values were collected from medical records. Physicians responded to questionnaires exploring reasons for continuing warfarin therapy.
Results
Overall, 313 patients treated with warfarin were registered at 33 sites. Mean ± SD age was 76.4±9.6 years; 62.9% of patients were male. The proportion of patients with INR values in the therapeutic range was 74.6% and 48.8% among patients aged ≥70 years and <70 years, respectively. Over half of the patients (51.4%) had been advised to switch from warfarin to DOACs; the primary physician-reported reason for this recommendation was superior safety and effectiveness. However, patients reported continuing warfarin because of the high price of DOACs (47.2%) and long-term positive experiences with warfarin (31.7%). The remaining 48.6% of patients with NVAF had never been counseled by their physicians about DOACs as an alternative to warfarin. For 76% of these patients, physicians favored warfarin for medical reasons, such as impaired renal function and controlled INR, but in the remaining patients, medical reasons for continuing warfarin were lacking.
Conclusion
Approximately half of the patients in this study were informed of warfarin alternatives primarily for improved efficacy and safety, but elected not to change regimens because of the high price of DOACs and long-term positive experiences with warfarin. In the remaining half, physician preference or specific patient characteristics prevented a change in therapy.
Plain language summary
Although warfarin has historically been the standard of care for preventing ischemic stroke in patients with nonvalvular atrial fibrillation, the use of direct oral anticoagulants (DOACs) is rapidly increasing. We examined the demographic and clinical characteristics of patients continuing warfarin therapy and investigated reasons for warfarin continuation in the era of DOACs. More than half of the patients (51.4%) had been advised to switch from warfarin to DOACs; the primary physician-reported reason was “better safety and effectiveness profile of DOACs compared with warfarin”. However, patients reported continuing warfarin because of the high price of DOACs (47.2%) and long-term positive experiences with warfarin (31.7%). The remaining 48.6% of patients had never been counseled by their physicians about DOACs as an alternative to warfarin. For 76% of these patients, physicians favored warfarin for medical reasons (eg, impaired renal function and controlled international normalized ratio), but in the remaining patients, medical reasons for continuing warfarin were lacking.
Introduction
Atrial fibrillation (AF) is a common arrhythmia in elderly populations and a major risk factor for cardioembolic stroke, which can lead to serious disability and diminished quality of life.Citation1–Citation4 The incidence of AF is on the rise, and major cardiovascular risk factors, including age, male gender, hypertension, heart failure, and obesity, are known to increase the risk of developing AF.Citation5–Citation7 Current AF treatment guidelines recommend the use of an oral anticoagulant (OAC) for prevention of cardioembolic stroke in patients with AF when additional risk factors are present.Citation8,Citation9 Historically, warfarin has been the OAC of choice in AF. However, patients taking warfarin must monitor their anticoagulation status with regular measurements of international normalized ratio (INR) values. Even with routine testing, therapeutic INR values are difficult to maintain and are prone to fluctuations outside of the relatively narrow therapeutic range. Deviations in INR values may lead to serious outcomes including thrombosis and bleeding. In addition to regular monitoring, patients on warfarin must carefully regulate their diet and concomitant medications, avoiding antiplatelet drugs, nonsteroidal anti-inflammatory drugs, and other medications that may increase bleeding or interact with warfarin, thus imposing an additional burden on patients. Furthermore, it has been suggested that warfarin therapy may be associated with increased arterial stiffness.Citation10
Recently, direct oral anticoagulants (DOACs), also known as non–vitamin K antagonist OACs, have been introduced for stroke prevention in patients with AF. DOACs – dabigatran, rivaroxaban, apixaban, and edoxaban – have shown superior or noninferior safety and efficacy compared to warfarin in large randomized controlled trialsCitation11–Citation13 and in real-world settings.Citation14–Citation20 Although many patients with nonvalvular AF (NVAF) have switched to DOAC therapy, a significant proportion of patients are still treated with warfarin. The AGAIN studyCitation38 was a prospective observational study conducted in Japanese patients with NVAF that investigated patient-reported satisfaction with apixaban after switching from warfarin (UMIN000018970). In this study, most physicians switched patients to apixaban in compliance with treatment guidelines,Citation21 but many patients remained on warfarin for reasons unsubstantiated by scientific evidence, including higher prices of DOACs compared to warfarin, lack of pressing reasons to switch (INR stably controlled within the therapeutic range), and fear of the potential risks of bleeding or ischemic events during the transition, either due to an overlap or a gap between warfarin and DOAC coverage. A further analysis of these reasons, as well as the characteristics of patients who remained on warfarin, was not explored in the study.
Therefore, the aim of this study was to investigate the reasons for continuing warfarin rather than switching to DOACs. Additionally, we examined the demographic and clinical characteristics of patients who continued warfarin treatment compared with patients who switched to DOACs.
Methods
Statement of ethics
This multicenter, retrospective study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by each hospital’s ethics committee or by a central ethics committee (Supplementary materials, Table S1). The study is registered with UMIN-CTR, a clinical trial registry in Japan (study ID: UMIN000024531).
Study design
This study consisted of retrospective data collection of the patient’s medical record and a questionnaire on the physician’s perception on warfarin use in general. Physicians and investigators made a contract involving provisions and usage of the data for this study. Patient-level data, including patients’ clinical and demographic characteristics and INR values, were retrospectively collected from medical records. To obtain the reasons why patients chose to continue the use of warfarin though they were advised to switch to DOAC, physicians, not patients, completed a questionnaire retrospectively based on a medical chart of each patient. Data including evaluations of physicians’ knowledge and beliefs of warfarin-based anticoagulant therapy and general treatment strategies for NVAF were also collected. All data provided from physicians were de-identified. In this study, as no primary data collection of patient data was conducted, written informed consent was not required for this study according to local regulations in Japan.
Study sites
In total, 33 sites (10 hospitals and 23 clinics) were randomly selected from the institutions participating in the AGAIN study. Of these 33 institutions, 28 specialized in cardiology. Ten or more patients were registered consecutively at each site.
Study population
Adult Japanese patients with NVAF who had been treated with warfarin for prevention of cardioembolic stroke and systemic embolism for at least 12 months before the index date (defined as the date of contract execution between Pfizer Japan and the study site) and who had never been treated with DOACs were eligible for the study. At each institution, the first 10 consecutive patients to meet enrollment criteria were selected retrospectively from the index date to eliminate selection bias. A total of 313 patients were ultimately enrolled in the study.
Data collection
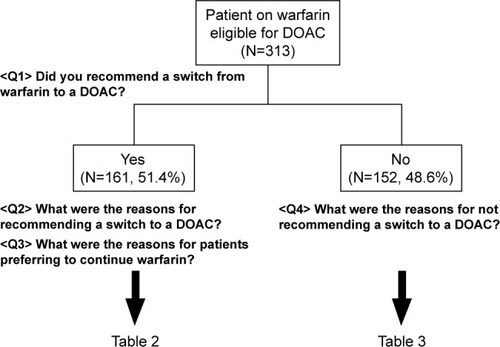
Patient demographic and clinical characteristics were retrospectively collected from the medical record to construct a dataset for the 1-year period preceding each patient’s most recent hospital visit. Each patient’s physician received a questionnaire regarding the reasons for recommending or not recommending switching from warfarin to a DOAC (, Q2 and Q4) and the reasons the patient declined to comply with this recommendation (, Q3). Additionally, with the assistance of a contract research organization (Mebix Inc., Tokyo Japan), we sent a second questionnaire to the same group of physicians that addressed their general (non–patient-specific) strategies and beliefs regarding anticoagulant therapy with warfarin and DOACs (Supplementary materials, Figure S1).
Figure 1 Flowchart of questions about physician recommendations to switch to DOACs or continue warfarin.
Abbreviation: DOAC, direct oral anticoagulant.
Statistical methods
For continuous variables, the mean ± SD, median, minimum, and maximum were calculated. Proportions are presented as percentages. Differences in patient characteristics between patients treated with warfarin in the current study and those who switched from warfarin to apixaban in the AGAIN study were compared using the paired t-test or chi-square test. Statistical analyses were conducted using SAS version 9.4 software (SAS Institute Inc., Cary, NC, USA).
Results
Patient characteristics
In total, 313 patients who met inclusion criteria were registered at 33 institutions. Patient demographic and clinical characteristics were collected retrospectively. Thirty-eight physicians answered questions regarding patient-specific reasons for continuing warfarin therapy, as well as additional questions addressing their knowledge and beliefs about anticoagulant therapy with warfarin and DOACs.
Patient demographic and clinical characteristics are shown in . Mean ± SD age was 76.4±9.6 years (73.5% of patients were ≥70 years old); 62.9% of patients were male. Mean ± SD CHADS2, CHA2DS2-VASc, and HAS-BLED scores were 2.3±1.2, 4.1±1.8, and 2.6±1.2, respectively. Baseline INR values were within the recommended therapeutic range for 74.6% of patients aged ≥70 years and 48.8% of patients aged <70 years.
Table 1 Patient demographic and clinical characteristics
The mean ± SD annual number of INR measurements was 9.2±3.9 in patients aged ≥70 years and 8.2±3.6 in those aged <70 years; 43.0% and 36.1% of patients had changed warfarin dosages during the 52 weeks before the index date among patients aged ≥70 years and <70 years, respectively.
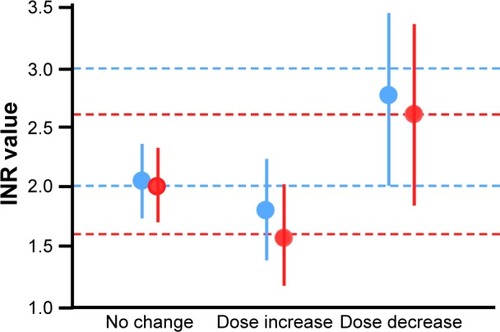
There was no significant difference in INR values between patients <70 years old and those ≥70 years old (2.0±0.5 and 2.0±0.4, respectively; P=1.000) (). Additionally, shows mean ± SD INR values at times when warfarin doses were increased (1.59±0.42 in patients aged ≥70 years and 1.82±0.43 in patients aged <70 years) and those at times when doses were decreased (2.60±0.77 in patients aged ≥70 years and 2.78±0.72 in patients aged <70 years). The timing of dose changes was similar between the two groups.
Figure 2 INR values when doses of warfarin were increased or decreased in patients <70 years old and ≥70 years old.
Abbreviation: INR, international normalized ratio.
Reasons for switching to DOACs or continuing warfarin
shows a flowchart of the questions presented to physicians regarding switching from warfarin to DOACs and patients’ reasons for continuing warfarin despite physician recommendations. Approximately half of all patients (51.4%) who continued warfarin treatment had been advised to switch from warfarin to a DOAC. The primary reason among physicians for recommending DOACs was “a better safety and effectiveness profile for DOACs compared with warfarin” (55.3%), as shown in . However, although these patients had been advised to switch to DOACs, they chose to continue warfarin therapy primarily due to “much higher drug prices of DOACs” (47.2%) and their “long-term experience with warfarin without any trouble” (31.7%). Among the remaining half of the patients who were not advised to switch from warfarin to DOACs, leading reasons for continuing warfarin treatment were “INR stably controlled” (37.5%) and “decreased renal function” (25.7%) ().
Table 2 Reasons physicians recommended switching to DOACs (N=161)
Table 3 Reasons in favor of continued warfarin therapy (N=152)
Questionnaire results: physicians’ insight into anticoagulation therapy
and show physicians’ responses to general questions of patient suitability for warfarin versus DOAC treatment (refer to Figure S1 for the questionnaire). In response to the question “Which patients do you think are suitable for warfarin treatment?”, 81.6% of physicians selected “patients with decreased renal function”, and 68.4% selected “patients who are satisfied with warfarin”. A large majority of physicians responded that switching to DOACs is appropriate for patients with fluctuating INR levels (89.5%) and for patients with INR values consistently outside of the therapeutic range (76.3%).
Table 4 Physicians’ perspective on patients suitable for warfarin treatment (N=38)
Table 5 Physicians’ perspective on patients suitable for switching to DOACs (N=38)
A comparison of patients on warfarin therapy (current study) versus patients who switched to apixaban (AGAIN study)
shows the demographic and clinical characteristics of patients continuously treated with warfarin and those who switched from warfarin to a DOAC. There were significant differences between the two groups in the self-pay ratio of medical costs (P<0.0001), duration of warfarin treatment (P<0.0001), and the percentage of patients aged ≥70 years whose baseline INR values were within the therapeutic range (P<0.0001).
Table 6 Demographic and clinical characteristics of patients receiving continued warfarin therapy (current study) and patients who switched to apixaban (AGAIN studyCitation38)
Discussion
This study surveyed patient characteristics, INR values, and physicians’ and patients’ reasons for continuing warfarin therapy rather than switching to DOACs in a population of patients with NVAF treated with warfarin. We found that ~50% of patients on warfarin were never counseled by their physician about DOACs as an alternative treatment option, and therefore continued warfarin therapy primarily as a result of physicians’ medical judgment. Additionally, we found that the percentage of patients with therapeutic INR values was notably high among patients aged ≥70 years.
In our investigation into the reasons for continuing warfarin rather than switching to DOACs, we found that about half of the patients remaining on warfarin therapy had never been advised by their physicians to switch therapies, nor had they been informed about DOACs as a potential alternative to warfarin. Medical rationales for continuing warfarin outweighed reasons related to patient convenience, including “INR stably controlled by warfarin”, as reported by 37.5% of physicians (). When asked in general terms about which patients are suitable for continuing warfarin treatment, 52.6% of physicians responded, “patients whose INR is controlled within the recommended therapeutic range” (). In contrast, 76.3% of physicians stated that patients should be switched to DOACs “when INR values are not consistently within the therapeutic range of warfarin recommended by the guidelines”. Correspondingly, 89.5% of physicians replied that “patients with fluctuations in INR” are appropriate for DOACs ().
Physicians reported that patients with large visit-to-visit INR fluctuations may carry a higher risk of bleeding and ischemic stroke. However, the opposite may not always be true, as patients receive the maximum benefit of stable INR only when INR is maintained within the optimal therapeutic range. Furthermore, results from previous randomized controlled trials suggest that patients treated with DOACs may experience fewer bleeding and/or ischemic events compared to patients on warfarin with INR levels stably maintained inside the therapeutic range. Hemorrhage has also been observed in patients with INR <3.0 in real-world settings.Citation22,Citation23 Therefore, stably controlled INR may not always be a logical reason to forgo transitioning to DOACs, although many physicians reportedly believe that control status of INR is the most critical factor for deciding to continue warfarin therapy.
The second most common reason for not recommending DOACs was “reduced renal function”, reported by 25.7% of physicians (). Warfarin is metabolized in the liver, whereas all DOACs have some degree of renal excretion; dabigatran is the highest at 80%, followed by edoxaban (50%), rivaroxaban (33%), and apixaban (27%).Citation24–Citation28 Therefore, warfarin can be expected to provide more stable anticoagulation than DOACs in patients with reduced renal function. However, patients with impaired renal function were excluded from the large-scale randomized Phase III trials that investigated the efficacy and safety of DOACs in comparison to warfarin.Citation11–Citation13,Citation29 In one study comparing apixaban and warfarin, apixaban reduced the rate of stroke, death, and major bleeding, regardless of renal function.Citation30 Further studies are needed to evaluate the efficacy and safety of DOACs compared with warfarin in patients with impaired renal function.
As previously mentioned, 51.4% of patients taking warfarin had been advised by their physician to switch to a DOAC. Although it is not entirely clear why warfarin therapy was continued in these patients, patient preference likely affected this decision. Our results revealed that patients elected to continue warfarin therapy primarily due to the “much higher drug prices of DOACs” (reported by 47.2% of patients) and a “long-term experience of warfarin without any trouble” (31.7%). AF commonly occurs in the elderly, as reflected in this survey population (73.5% of patients were ≥70 years old). Consequently, many patients with AF have a limited income – often solely pension – and may not be able to afford more expensive medications. This may explain why drug price was the leading reason for continuing warfarin, the least expensive OAC.
As shown in , there were minimal differences in clinical and demographic background between patients on warfarin (from the current study) and patients who switched to apixaban (from the AGAIN study). Only three significant differences in background were observed between the two groups: 1) duration of warfarin treatment, 2) percentage of patients aged ≥70 years with therapeutic INR levels, and 3) self-pay ratio of medical costs. Not coincidentally, these differences between warfarin users and apixaban users correspond with the reasons that patients reported a preference for continuing warfarin therapy, namely, that patients on long-term warfarin have had positive experiences, that patients have been able to maintain stable INR with warfarin, and that patients with higher self-pay ratios tend to choose the more affordable OAC.
The aim of this study was to explore the reasons for continued warfarin use from the perspective of both physicians and patients. However, the most critical element in this scenario, regardless of the type of OAC, is patient compliance with medications as prescribed by physicians. Patient satisfaction with and preference for a given pharmaceutical regimen may have a significant impact on medication adherence.Citation31 The importance of patient adherence to anticoagulant therapy for prevention of stroke cannot be overstated; a single missed dose may lead to stroke.Citation32,Citation33 Therefore, patient preference for anticoagulation therapy should be taken into consideration to maintain optimal medication adherence. Equally important is a healthy doctor–patient relationship that includes discussion of all treatment options and frequent communication about patient satisfaction with anticoagulation therapy.
As shown in , mean INR values were comparable between patients aged <70 years and ≥70 years, indicating that physicians are not always strictly adherent to the Japanese Circulation Society’s 2013 Guidelines for Pharmacotherapy of Atrial Fibrillation; these guidelines recommend that INR levels in patients with NVAF should be maintained between 2.0 and 3.0 in patients aged <70 years old, and between 1.6 and 2.6 in patients aged ≥70 years old.Citation21 As shown in , physicians may be targeting the INR range of 1.6–2.6 even in younger patients, despite Japanese guideline recommendations for a therapeutic range of 2.0–3.0. Similar results have been reported by investigators from the Fushimi Registry, a community-based survey of patients with AF in Japan that primarily consists of private clinics of general practitioners,Citation34,Citation35 and the J-RHYTHM Registry, a nationwide registry of patients with AF recruited from hospitals and clinics specializing in cardiology.Citation36,Citation37 This finding implies that physicians may treat patients of all ages with relatively low doses of warfarin to maintain INR values between 1.6 and 2.6 regardless of guideline recommendations, likely out of concern related to the development of bleeding events. Taken together, these results suggest that INR is suboptimally controlled in patients aged <70 years, regardless of the specialty of the physician managing care.
Limitations
This study has several limitations because of its design and methodology. The study was conducted at a limited number of institutions that were chosen at random from the AGAIN study; therefore, the results may not be suitable for extrapolation to general practice in Japan or other countries. Additionally, the questionnaires used in this study have not been validated linguistically and psychometrically, and methods for using them have not been standardized.
Conclusion
Approximately half of the patients in this study received a recommendation from their physician to switch from warfarin to a DOAC, primarily on the basis of improved efficacy and safety, but elected not to change regimens because of the high price of DOACs. In the remaining half of the study population, physician preference or specific patient characteristics prevented a change of therapy. From the physician’s perspective, stable INR control was the most important reason to continue warfarin, even if INR values were below the therapeutic range. For patients, lower cost and long-term positive experiences with warfarin constituted the rationale for warfarin preference. Ultimately, a healthy doctor–patient relationship that includes discussion of all treatment options and frequent communication about patient satisfaction with anticoagulation therapy is crucial for achieving medication adherence.
Author contributions
All authors contributed toward study design, data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Acknowledgments
The authors would like to thank the doctors participating in this study. We would like to acknowledge the contribution of Mebix, Inc. to this study, including site selection, site monitoring, study management, data management, and statistical analysis. We thank Ms Pearl Gomes from Cactus Communications KK for editing the manuscript. The study and editing of the manuscript were supported by Bristol-Myers Squibb KK and Pfizer Japan Inc.
Disclosure
TI received research grants from Bristol-Myers Squibb KK, Daiichi Sankyo KK, Nippon Boehringer Ingelheim, honoraria and consulting fees (for speaker, writer and/or adviser) from Bayer Yakuhin Ltd., Bristol-Myers Squibb KK, Daiichi Sankyo KK, Nippon Boehringer Ingelheim, and Pfizer Japan Inc. MY received a research grant from Nippon Boehringer Ingelheim, honoraria and consulting fees from Bayer Yakuhin Ltd., Bristol-Myers Squibb KK, Daiichi Sankyo KK, Nippon Boehringer Ingelheim, and Pfizer Japan Inc. MK is an employee of Bristol-Myers Squibb KK. MI is an employee of Pfizer Japan Inc. The authors report no other conflicts of interest in this work.
References
- HataJTanizakiYKiyoharaYTen year recurrence after first ever stroke in a Japanese community: the Hisayama studyJ Neurol Neurosurg Psychiatry200576336837215716529
- PereraKSVanasscheTBoschJESUS Global Registry Investigators. Global survey of the frequency of atrial fibrillation-associated stroke: embolic stroke of undetermined source global registryStroke20164792197220227507860
- PrystowskyENBensonDWJrFusterVManagement of patients with atrial fibrillation. A statement for healthcare professionals. From the subcommittee on electrocardiography and electrophysiology, American Heart AssociationCirculation1996936126212778653857
- WolfPAAbbottRDKannelWBAtrial fibrillation: a major contributor to stroke in the elderly. The Framingham StudyArch Intern Med19871479156115643632164
- BenjaminEJLevyDVaziriSMD’AgostinoRBBelangerAJWolfPAIndependent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart StudyJAMA1994271118408448114238
- KokuboYWatanabeMHigashiyamaANakaoYMKusanoKMiyamotoYDevelopment of a basic risk score for incident atrial fibrillation in a Japanese general population – the Suita StudyCirc J201781111580158828539563
- WangTJPariseHLevyDObesity and the risk of new-onset atrial fibrillationJAMA2004292202471247715562125
- JanuaryCTWannLSAlpertJS2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm SocietyJ Am Coll Cardiol20146421e1e7624685669
- KirchhofPBenussiSKotechaD2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTSEuropace201618111609167827567465
- MozosIStoianDLucaCTCrosstalk between vitamins A, B12, D, K, C, and E status and arterial stiffnessDis Markers20172017878497128167849
- GrangerCBAlexanderJHMcMurrayJJApixaban versus warfarin in patients with atrial fibrillationN Engl J Med20113651198199221870978
- PatelMRMahaffeyKWGargJRivaroxaban versus warfarin in nonvalvular atrial fibrillationN Engl J Med20113651088389121830957
- ConnollySJEzekowitzMDYusufSDabigatran versus warfarin in patients with atrial fibrillationN Engl J Med2009361121139115119717844
- LarsenTBRasmussenLHSkjøthFEfficacy and safety of dabigatran etexilate and warfarin in “real-world” patients with atrial fibrillation: a prospective nationwide cohort studyJ Am Coll Cardiol201361222264227323562920
- LaliberteFCloutierMNelsonWWReal-world comparative effectiveness and safety of rivaroxaban and warfarin in nonvalvular atrial fibrillation patientsCurr Med Res Opin20143071317132524650301
- HernandezIBaikSHPineraAZhangYRisk of bleeding with dabigatran in atrial fibrillationJAMA Intern Med20151751182425365537
- LauffenburgerJCFarleyJFGehiAKRhoneyDHBrookhartMAFangGEffectiveness and safety of dabigatran and warfarin in real-world US patients with non-valvular atrial fibrillation: a retrospective cohort studyJ Am Heart Assoc201544e00179825862791
- BouillonKBertrandMMauraGBlotierePORicordeauPZureikMRisk of bleeding and arterial thromboembolism in patients with non-valvular atrial fibrillation either maintained on a vitamin K antagonist or switched to a non-vitamin K-antagonist oral anticoagulant: a retrospective, matched-cohort studyLancet Haematol201524e150e15926687957
- LipGYKeshishianAKambleSReal-world comparison of major bleeding risk among non-valvular atrial fibrillation patients initiated on apixaban, dabigatran, rivaroxaban, or warfarin. A propensity score matched analysisThromb Haemost2016116597598627538358
- LipGYPanXKambleSMajor bleeding risk among non-valvular atrial fibrillation patients initiated on apixaban, dabigatran, rivaroxaban or warfarin: a “real-world” observational study in the United StatesInt J Clin Pract201670975276327550177
- JCS Joint Working GroupGuidelines for Pharmacotherapy of Atrial Fibrillation (JCS 2013)Circ J20147881997202124965079
- YamaguchiTOptimal intensity of warfarin therapy for secondary prevention of stroke in patients with nonvalvular atrial fibrillation: a multicenter, prospective, randomized trial. Japanese Nonvalvular Atrial Fibrillation-Embolism Secondary Prevention Cooperative Study GroupStroke200031481782110753981
- YasakaMMinematsuKYamaguchiTOptimal intensity of international normalized ratio in warfarin therapy for secondary prevention of stroke in patients with non-valvular atrial fibrillationIntern Med200140121183118811813841
- BlechSEbnerTLudwig-SchwellingerEStangierJRothWThe metabolism and disposition of the oral direct thrombin inhibitor, dabigatran, in humansDrug Metab Dispos200836238639918006647
- StangierJRathgenKStähleHMazurDInfluence of renal impairment on the pharmacokinetics and pharmacodynamics of oral dabigatran etexilate: an open-label, parallel-group, single-centre studyClin Pharmacokinet201049425926820214409
- ParasrampuriaDATruittKEPharmacokinetics and pharmacodynamics of edoxaban, a non-vitamin K antagonist oral anticoagulant that inhibits clotting factor XaClin Pharmacokinet201655664165526620048
- WeinzCSchwarzTKubitzaDMueckWLangDMetabolism and excretion of rivaroxaban, an oral, direct factor Xa inhibitor, in rats, dogs, and humansDrug Metab Dispos20093751056106419196845
- FrostCWangJNepalSApixaban, an oral, direct factor Xa inhibitor: single dose safety, pharmacokinetics, pharmacodynamics and food effect in healthy subjectsBr J Clin Pharmacol201375247648722759198
- GiuglianoRPRuffCTBraunwaldEEdoxaban versus warfarin in patients with atrial fibrillationN Engl J Med2013369222093210424251359
- HohnloserSHHijaziZThomasLEfficacy of apixaban when compared with warfarin in relation to renal function in patients with atrial fibrillation: insights from the ARISTOTLE trialEur Heart J201233222821283022933567
- OsterbergLBlaschkeTAdherence to medicationN Engl J Med2005353548749716079372
- WangYKongMCLeeLHNgHJKoYKnowledge, satisfaction, and concerns regarding warfarin therapy and their association with warfarin adherence and anticoagulant controlThromb Res2014133455055424448058
- ShoreSCareyEPTurakhiaMPAdherence to dabigatran therapy and longitudinal patient outcomes: insights from the veterans health administrationAm Heart J2014167681081724890529
- AkaoMChunYHEsatoMFushimi AF Registry Investigators. Inappropriate use of oral anticoagulants for patients with atrial fibrillationCirc J20147892166217224976391
- AkaoMChunYHWadaHFushimi AF Registry Investigators. Current status of clinical background of patients with atrial fibrillation in a community-based survey: the Fushimi AF RegistryJ Cardiol201361426026623403369
- AtarashiHInoueHOkumuraKYamashitaTKumagaiNOrigasaHJ-RHYTHM Registry InvestigatorsPresent status of anticoagulation treatment in Japanse patients with atrial fibrillation: a report from J-RHYTHM RegistryCirc J20117561328133321467664
- AtarashiHInoueHOkumuraKYamashitaTOrigasaHJ-RHYTHM Registry InvestigatorsInvestigation of optimal anticoagulation strategy for stroke prevention in Japanse patients with atrial fibrillation – the J-RHYTHM Registry study designJ Cardiol2011571959920934857
- KoretsuneYIkedaTKozumaKPatient satisfaction after switching from warfarin to apixaban in patients with nonvalvular atrial fibrillation: AGAIN studyPatient Prefer Adherence2017111987199629290682