
Abstract
Purpose
Worldwide, stroke is a leading cause of disease burden. Many survivors have unmet needs after discharge from hospital. Electronic communication technology to support post-discharge care has not been used for patients with stroke. In this paper, we describe the development of a novel electronic messaging system designed for survivors of stroke to support their goals of recovery and secondary prevention after hospital discharge.
Participants and methods
This was a formative evaluation study. The design was informed by a literature search, existing data from survivors of stroke, and behavior change theories. We established two working groups; one for developing the electronic infrastructure and the other (comprising researchers, clinical experts and consumer representatives) for establishing the patient-centered program. Following agreement on the categories for the goal-setting menu, we drafted relevant messages to support and educate patients. These messages were then independently reviewed by multiple topic experts. Concurrently, we established an online database to capture participant characteristics and then integrated this database with a purpose-built messaging system. We conducted alpha testing of the approach using the first 60 messages.
Results
The initial goal-setting menu comprised 26 subcategories. Following expert review, another 8 goal subcategories were added to the secondary prevention category: managing cholesterol; smoking; physical activity; alcohol consumption; weight management; medication management; access to health professionals, and self-care. Initially, 455 health messages were created by members of working group 2. Following refinement and mapping to different goals by the project team, 980 health messages across the health goals and 69 general motivational messages were formulated. Seventeen independent reviewers assessed the messages and suggested adding 73 messages and removing 16 (2%). Overall, 1,233 messages (18 administrative, 69 general motivation and 1,146 health-related) were created.
Conclusion
This novel electronic self-management support system is ready to be pilot tested in a randomized controlled trial in patients with stroke.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
Globally, stroke is the third most common cause of disability with >10 million strokes occurring annually and almost 30 million people living with a history of stroke.Citation1,Citation2 For most survivors, integrating back into the community and managing the consequences of stroke is difficult. Survivors of stroke liken the experience of going home from hospital to “falling into a black hole”.Citation3 This situation arises because stroke can have a profound impact on quality of life, with approximately one-quarter of survivors reporting their situations as equivalent to, or worse than, death.Citation4 Factors that complicate return to the community after stroke include the presence of physical disability, cognitive changes, loss of employment, inability to participate in pre-stroke activities, social isolation, anxiety and depression.Citation5 Survivors also have an increased risk of vascular events,Citation6 and many have modifiable risk factors that are poorly managed.
Despite clear recommendations for discharge preparation in national guidelines for stroke care,Citation7 discharge care is poorly implemented in hospitals. Only half of the patients with stroke receive a formal care plan at the time of discharge or lifestyle education to support moderating their future risk of vascular disease.Citation8 In an Australian survey of 765 survivors one or more years following stroke, 84% reported unmet recovery and secondary prevention needs, particularly in aspects of health such as cognition, memory, emotion and fatigue.Citation9 The short length of hospital stay of ~5 days in AustraliaCitation10 may contribute to the lack of adequate self-management tools and support provided to patients in hospital. Approximately 40% of survivors of stroke, and >60% of their caregivers, report being dissatisfied with the information they received while in hospital.Citation11 Patients also want to be actively involved in setting their goals to positively influence their recovery.Citation12 However, there are often mismatches between what clinicians and patients consider to be patient-centered goal setting.Citation13
Comprehensive management and goal setting after discharge is aimed at addressing the self-management needs of each patient, including their return to usual activities in their home environment, addressing personal concerns and mini-mizing the risk of future stroke.Citation14 However, providing these patients with the necessary support to continue with their recovery and secondary prevention once they have been discharged home is challenging, particularly in those with limited mobility or who live a long distance from hospitals/services. Simple, innovative and cost-effective strategies could be used to help survivors attain their secondary prevention goals, adjust to their altered functional and emotional abilities, and promote community participation.Citation7 Because of the exponential increase in use of electronic devices, for example, mobile phones, tablets and personal computers in the community, these electronic communication technologies could be used to promote changes in lifestyle behavior and self-management.
Although short message service (SMS) and internet-based programs have been trialled in several populationsCitation15 their use in survivors of stroke is less common and limited to improving medication adherence or reducing depression in men.Citation16,Citation17 Given the broad impact stroke has on survivors, the aim of our project was to develop a comprehensive, electronic self-management support program designed for attaining patient-centered goals.
Materials and methods
The Inspiring Virtual Enabled Resources following Vascular Events (iVERVE) pilot establishment project was achieved through collaboration between the Faculty of Medicine, Nursing and Health Sciences and the Faculty of Engineering at Monash University, Australia. Leading academics with an interest in self-management programs for chronic conditions from other institutions were also involved. We undertook a literature review of electronic health interventions to ensure our program design was based on the latest evidence. We then used a formative program evaluation to ensure the system was robust. Formative evaluation enables development and modification of a program within a feedback loop to promote successful future implementation.Citation18
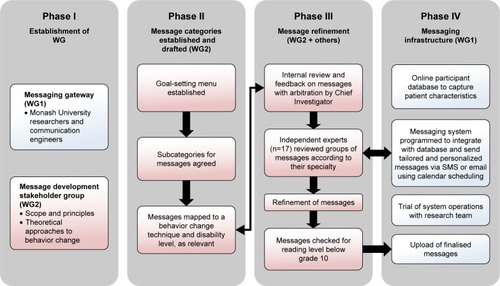
The iVERVE pilot project was established in four phases. Phase I involved establishment of two working groups: working group 1 for the technical application/infrastructure; and working group 2 for the content and refinement of messages. In Phase II, we developed a goal-setting menu comprising broad categories of recovery and secondary prevention categories. These categories were then subcategorized to enable the formulation of messages. Phase III comprised refinement of messages, using internal and external review, while Phase IV comprised establishing and trialling the concurrently developed iVERVE messaging system (). Further detail is provided in the following sections.
Figure 1 Project phases and activities.
The working groups were comprised of investigators based on their relevant expertise, clinicians, project staff and consumer representatives or engineers, as relevant. The lead principal investigator (DAC), project coordinators (JC and DB), and MFK, AGT and NEA from Monash University were members of both working groups to ensure that concurrent work was complementary and that the experience gained in one area could be used to inform the other area.
Ethical approval for this project was provided by Monash University Human Research Ethics Committee (CF16/1920-2016000979). As this was early development phase research, the testing of the system by researchers was considered to not require written informed consent.
Messaging infrastructure development and testing (working group 1)
Telecommunications engineers from the Faculty of Engineering at Monash University were responsible for creating the specified electronic messaging system and web interface. The system was developed during several meetings to fulfil our requirements to incorporate scheduling, personalization (ie, ability to include first, last name or preferred names), and tailoring of the support messages to align with a patient’s disability level and their specified health and recovery goals.
A participant database was created to enter patient demographic information and severity of stroke. Information obtained from patients about their preferred scheduling frequency or mode of communication (eg, by SMS or email) was also incorporated into this database. The messaging system was programmed for integration with the database used for storing a much larger range of variables for each participant. This was to avoid double data entry of patient information. For future use in clinical trials, the participant database was created using Research Electronic Data Capture (REDCap) tool hosted at Monash University. REDCap is a secure, web-based application designed to support data capture for research studies, providing: 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.Citation19 We designed the database to be partitioned for different users, whereby only the project coordinator could access all information. The system also incorporates an inbuilt electronic randomization program.
Messages were bundled, with the iVERVE messaging system programmed to randomly select a message from a themed predetermined bundle until all messages from that bundle had been sent at least once. This provides a large range of message options for each goal that can be pre-assigned for each patient for each of their specified goals. This process was developed to reduce the labor intensity in pre-assigning messages for each specific personalized goal. Individual messages within the bundle were categorized into those more appropriate during the first weeks of participation (ie, “early”) and for more advanced stages of goal attainment (“late”; “Theoretical basis for message development” section). The system was also designed so that electronic messages could be sent via email if this was the participant’s preferred mode of receiving messages. The ability to delete, edit or add messages was also built into the system.
A dedicated phone number was purchased through a commercial bulk SMS provider. This ensured that patients would only receive messages from a unique iVERVE phone number. To ensure appropriate and efficient documentation of activity, the system was designed with an automated log record of all electronic messages sent to individual participants (date, time, copy of message), including any that had failed to send. Bi-directional communication was required to permit simple responses (eg, Yes or No) to incoming messages when requested, as well as the option to send a “STOP” message to opt out of receiving some or all the electronic messages.
Alpha testing of the system, by the project team, was conducted throughout the various development stages, similar to an agile method.Citation20 Once an initial 60 messages had been developed, they were uploaded onto the electronic website and members of the research team were scheduled to receive SMS or email messages for various health/recovery goals. Revisions were made following feedback on the wording of messages, spelling errors, or failure of the shortened URL Web links. All other technical issues were also recorded and rectified.
Development of the goal-setting menu and self-management support messages (working group 2)
We established a working group consisting of clinicians, behavioral and social scientists, psychologists, and epidemiologists with experience in conducting research using SMS or e-health interventions in stroke or similar chronic conditions.Citation21–Citation23 A representative from the Stroke Foundation and a consumer (ie, survivor of stroke) also contributed to this working group. Terms of reference were established, and monthly or bi-monthly meetings were arranged via teleconference or in person.
In the first stage, consensus agreement from the working group was sought to provide feedback on a draft standardized goal-setting menu (). Setting goals for recovery based on “needs” can be highly effective and use of a standardized goal-setting menu can reduce subjectivity, ensure goals are measurable, and reduce the time taken to set goals.Citation24 For this aspect, we used existing data from observational studies to ensure we included all relevant areas important for achieving a patient-centered approach to meeting identified recovery or secondary prevention goals. In particular, we relied on data from the Australian Stroke Survivor and Carer Needs assessment survey that was based on a similar survey conducted in the UK.Citation9,Citation25 In the Australian version, 88% of the N=765 respondents felt that the scope of the survey questions covered their needs.Citation26
Table 1 Goal-setting menu developed for the iVERVE program
The components of the draft goal-setting menu used in this project were then mapped to the International Classification of Functioning Disability and Health (health and body functions, activities and participation, environment)Citation27 by NEA within the context of unmet needsCitation9 to ensure that all relevant aspects of recovery were covered. Secondary prevention of future stroke is very important to survivors and forms part of best-practice clinical guidelines.Citation7 Therefore, a secondary prevention category was added to the menu.
Following consensus on the goal-setting menu and subcategories for each main goal, this menu was used as the basis for developing the support/educational messages. Members of the working group volunteered to develop preliminary health messages selected from a subcategory that matched their area of expertise. As part of this process, contributors were asked to draw upon reputable and current clinical guidelines for management of stroke or prevention of cardiovascular disease and provide appropriate and trusted Web links of the source information.
Contributors were asked to follow set criteria for developing messages. Messages were required to be applicable to people of any age or sex, cater for different levels of impairment (disability), and allow for progression over a 12-week period of support. The maximum message length was set at 160 characters to allow messages to be sent as a single SMS. Use of commonly accepted abbreviations was permitted. Messages were also required to be developed using plain language that could be understood by someone with a reading level below grade ten (equivalent to a reading level of people aged 15–16 years). Each working group member was asked to develop a minimum of 8 messages for their subcategory. This was to enable a sufficient number of messages to be produced for a 12-week program of support.
Theoretical basis for message development
The messages targeted at attaining stroke recovery goals or maintaining motivation for secondary prevention goals were designed on the basis of 21 behavior change techniques (BCTs) that are underpinned by up to 7 behavior change theories (). This approach was used because of the evidence that attainment of individual goals is more likely when the messages are targeted at specific behavior change constructs.Citation28,Citation29 Specifically, working group members were asked to match each message to a specific BCT as reported by Abraham and Michie et alCitation29 () and adapted by Redfern et al.Citation22 This taxonomy of BCTs has been developed to standardize and characterize the content of behavior change interventions that have been linked to mediating processes informed by the relevant behavior change theories. Similar to Redfern et al,Citation22 messages were developed with a positive reinforcement stance. This has been shown to be more effective in producing lasting behavior change. For example, messages targeted positive reinforcement in the form of social reward such as encouragement, feelings of mastery from goal attainment, or experiencing benefits from improvements in health ().
Table 2 Behavior change techniques used to create health educational and motivational messages for the iVERVE program
To enable logical scheduling, messages were developed and grouped into early (contemplation/preparation) and late (action/maintenance) stages based on the Transtheoretical model of health behavior change (TTM), as outlined above. We acknowledge the relationships associated with behavior are complex and may be non-linear. However, the TTM is particularly helpful when developing interventions that address multiple behaviors within one program. The TTM has been used successfully in several settings for behavior change relating to stroke and cardiovascular risk reduction, whereby specific strategies have been applied to address the individual’s readiness to change.Citation30–Citation33 Considering that individuals who receive the self-management messages will have set their own health and recovery goals, they will have passed the pre-contemplation stage. On this basis, members of the working group were asked to map each message to either the contemplation/preparation, or action/maintenance phase.
To assist in tailoring messages to individual ability, potential barriers to self-management were assessed based on application of the Theoretical Domains Framework.Citation34,Citation35 These domains provide wide coverage of potential barriers to achieving behavior change and include: knowledge; skills; social role and identity; beliefs about capabilities; optimism; beliefs about consequences; reinforcement; intentions; goals; memory, attention and decision processes; environmental context and resources; social influences; emotion; and behavioral regulation. The working group members were asked to consider developing messages that addressed these potential barriers to self-management. For example, to overcome lack of knowledge, messages were developed with links to reputable websites from where more information could be accessed regarding a specific behavior or goal.
Where appropriate, messages were further categorized to cover a range of disability/functional levels, for example, slight or moderate disability and severe disability. In this manner, health messages could be tailored to the individual’s level of disability on the basis of using the modified Rankin scale, a disability measure commonly used in stroke populations. Finally, Google URL (https://goo.gl/) was used to create shortened Web links.
Internal review of health messages
Two investigators (DB and JC) reviewed all the messages returned by members of the working group. As bundles of messages were completed, they were reviewed by the principal investigator (DAC) who made editorial changes, suggested new messages, or wrote additional messages, when required. Where the character limit permitted, it was decided that all messages would be personalized with a first name.
Validation of messages via independent review
Health professionals and stroke researchers not contributing to iVERVE working groups were identified and invited to independently review the initial set of messages based on their field of expertise. The messages were sent via email with instructions on the review process. Specifically, they were asked to review the appropriateness and wording of messages, the stage(s) of change classification and, where relevant, the level of (dis)ability targeted for each message. They were also asked to consider providing additional messages appropriate to their allocated topic when they considered that an important message had been overlooked.
Confirmation of final bank of messages
Feedback from the independent panel was initially reviewed by 2 investigators (JC and DB) and the principal investigator (DAC) arbitrated to achieve consensus, as required. The final-ized messages were then checked for reading level, below grade 10, using an online software (http://www.webpagefx. com/tools/read-able/). The authors of this software consider that if the text has an average grade level of about 10, it should be easily understood by people aged 15–16 years.
Results
The initial draft goal setting menu based on the Australian Stroke Survivor Needs Survey items, consisted of 26 subcategories. Following input from the expert panel, the household chores subcategory was further categorized to inside chores and outside chores, whereas the subcategories of emotions, concentration and memory were combined into a single subcategory. Eight additional subcategories were identified by the panel. The additional goals were: managing cholesterol; smoking; physical activity; alcohol consumption; weight management; medication management; access to health professionals, for example, General Practitioner; and self care (eg activities of daily living). Overall, this resulted in 32 subcategories for the 4 main categories of the goal-setting menu ().
For the initial stage of message development, 455 health messages were created by members of working group 2 ( shows examples of messages). These were then refined by project staff and additional messages created based on suggestions for addressing gaps that had been identified by the working group. Messages were then mapped to other goals and duplicated, where appropriate. For example, the message “Activity burns calories and helps maintain weight. Climbing stairs, parking further away, or walking to the office add up quickly to 30 min a day” was suitable for a weight loss and physical activity goal. This internal review process resulted in 980 health messages related to health and recovery goals and 69 general motivational messages.
Figure 2 Sample messages for a fictitious person.

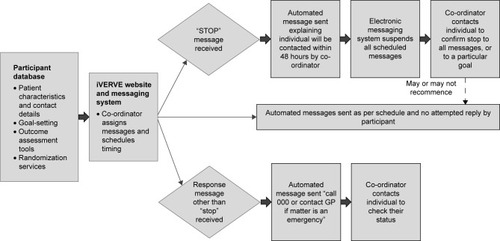
During alpha testing of the messaging system, we identified that we needed to program an automated message as a response to all “STOP” messages. This standard automatic message from the iVERVE project staff would indicate to the participant that they will be contacted within 48 hours regarding their request to STOP. In this circumstance, the system would temporarily suspend all other messages that had been scheduled for this participant until the iVERVE team clarified with them the reason for wanting to stop messages (). In the event that a message other than “Yes/No/STOP” was to be received, an automated message was programmed to be sent with instructions to “Call 000 or contact a GP, if the matter is an emergency”. We also identified that several other administrative messages would be needed, including a “welcome” message.
Figure 3 Messaging system and responses to messages.
Independent review
Seventeen independent reviewers, including health professionals and researchers, agreed to review bundles of messages. The independent reviewers disagreed with only 16 of the messages (2%) and suggested 73 additional messages (). Following the independent review process, all health and motivational messages were assessed for level of readability, whereby 96% (1,097/1,215) met our objective with a reading level of Grade 10 or below. Moreover, 79% were at a readability level of Grade 8 and below (equivalent to a reading level of adolescents aged 13–14 years).
Table 3 Independent review of developed health and motivational messages
Overall, we developed a final set of 1,233 messages (1,146 health or recovery-related, 18 administrative and 69 general motivational messages), with several duplicated across goals where relevant (). Shortened URL Web links were created on 27% (333/1,215) of the non-administrative messages using the Google URL: https://goo.gl/. In addition, more than one-third of the developed messages could be personalized.
Table 4 Overview of number of messages developed for each potential goal as part of the iVER VE program
Discussion
Our findings add to the limited literature on the process of developing an electronic self-management support messaging program to promote health behavior change. Most importantly, we have developed a bank of health messages and infrastructure that can be used to promote secondary prevention and recovery from stroke. Most messages were designed for 1-way communication. However, some 2-way messages were included as this format has been shown to encourage greater patient engagement.Citation15 Combined with the fact that messages were informed by behavioral theories, these bidirectional messages may enhance the potential for successful behavior change in the targeted population.
Our iVERVE intervention, which comprises a goal-setting menu that can be used by clinicians with aligned support messages, will address many of the aforementioned barriers to discharge planning such as poor communication from clinicians with patients by augmenting the current support offered to patients in the post-discharge period for up to 12 weeks. Our plan now is to test the effectiveness potential of this novel intervention for stroke by undertaking Phase I (proof-of-concept), II (acceptability and feasibility) and III (powered for health outcome effects) randomized controlled trials. In these trials, we will recruit patients with stroke and use the goal-setting menu to standardize and pri-oritize mutually agreed recovery and secondary prevention goals. Patient data and agreed goals will be entered into an electronic Case Report Form (eCRF), which will automatically prepopulate the iVERVE system. A clinician researcher can then link appropriate bundles of messages to each of the goals for a specified period (eg, 12 weeks). It is our intention to contact patients in the intervention group at least 3 times per week; the maximum number of contacts will be daily. Messages will be scheduled according to the priority of the goals, and stage of readiness for change, with a focus on only 1 goal in week 1 and then gradual introduction of other goals. This staggered approach was chosen to avoid overwhelming participants. In addition, 1 or 2 administrative or general motivational messages will be sent each week. This future work will provide essential information for determining the practicalities of implementing this new intervention and its potential effectiveness (eg, fewer readmissions to hospital, increased self-efficacy, and persistence with secondary prevention) and cost-effectiveness.
None of the prior research on SMS and email messaging support has offered a comprehensive solution to addressing the complexity of living with stroke. Appropriately designed trials in stroke are urgently needed.
The large and comprehensively developed bank of iVERVE messages is, to our knowledge, the first of its kind and is of great importance in interventions targeted at secondary prevention and recovery in survivors of stroke. Additionally, the novelty of our study is that the health messages have been specifically designed with a patient-centered focus to promote attainment of individual patient goals. An advantage of using text messages as the basis of interventions is that they can be used with almost all mobile phones, can be personalized, and take advantage of the widespread use of texting in most populations globally.Citation36,Citation37 The uptake of this technology in survivors of stroke is likely to increase in the future with the predicted increases in use of technology in older populations.
A robust process was used in the development of our program and messages were based on a range of complementary theoretical frameworks. These messages were mapped to various BCTs to promote beneficial behavior. Additionally, messages were based on evidence-based information and Stroke Clinical GuidelinesCitation7 since we did not seek to recreate reliable education material or content. In particular, a main principle was that the strategies or suggestions we provided would encourage and empower patients to seek out the information as part of their self-management.
Another strength is the ability to use SMS or email to communicate with participants. While availability of Internet-based resources does not necessarily mean they will be used, uptake of technology is greater when it is based on tools/devices already in everyday use,Citation38 and there is evidence of willingness to learn new technologies and skills.Citation36 In Australia, in 2016, 85% of the total population used the Internet.Citation39 Furthermore, 79% of adults aged >65 years used the Internet, with most (85%) accessing it daily, and 74% owning a mobile phone.Citation39 Therefore, participants who have suffered a stroke (generally aged over 65 years) are likely to have access to, and use, technology.
A limitation of this study is that messages developed were written in English and further research is needed to develop text messages that are suitable for culturally and linguistically diverse groups, or those with communication disorders. This limitation notwithstanding, a strength of our study is that messages were developed using evidence-based methods. Importantly, feedback from the independent review demonstrated essential consensus to the messages that we had developed with requests mainly being for minor changes.
Conclusion
We have described the development of a novel electronic self-management support system designed for survivors of stroke after hospital discharge. The intervention addresses the full scope of potential needs for patients through a comprehensive goal-setting menu and includes an online database to capture participant characteristics with automatic integration of selected data into the purpose-built iVERVE messaging system. The platform has >1,200 electronic messages ready for testing for acceptability in clinical use. The messages were developed using evidence-based theory, clinical guidelines, and independent review. There is a growing body of evidence about the use and potential effectiveness of messaging-based interventions for reducing behavioral risk factors and improving cardiovascular disease management. The iVERVE intervention has the potential to promote secondary prevention and recovery in survivors of stroke and may help avoid unplanned readmissions. Since effectiveness data for e-Health are limited in stroke, future randomized controlled clinical trials are planned to use the iVERVE intervention.
Author contributions
All authors have contributed to various or all aspects of conception, design, drafting or revising of the article, final approval for publication and agree to be accountable for the accuracy and integrity of the work.
Acknowledgments
We thank Frank Lan (engineer) for his contributions to the iVERVE messaging system. We also acknowledge Mariko Carey and Amy Waller (University of Newcastle) for their contributions to working group 2 and also the independent review panel members who provided their time in giving feedback on the messages or offering suggestions for additional messages. This study was funded by a Monash University Faculty Strategic Grant (SG516-0431). The following authors were also supported by fellowships from the National Health and Medical Research Council: DAC (1063761 co-funded by Heart Foundation), NEA (1072053), AGT (1042600), MFK (1109426), and the Heart Foundation MLH (100034). Some prevention messages were adapted with permission from the National Heart Foundation of Australia (Managing High blood Pressure [2013]; Measuring your blood pressure at home [2016]; Blood Cholesterol; Replace unhealthy fats; Be active every day [2016]; Walking; Am I active enough? [2016]; Get active. Melbourne: National Heart Foundation of Australia). Several of the messages were also adapted from educational materials from the Stroke Foundation and EnableMe websites.
Disclosure
The authors report no conflicts of interest in this work.
References
- Barker-ColloSLBennettDAKrishnamurthiRGBD 2013 Writing GroupGBD 2013 Stroke Panel Experts GroupSex differences in stroke incidence, prevalence, mortality and DALYs: results from the global burden of disease study 2013Neuroepidemiology201545320321426505984
- FeiginVLNorrvingBMensahGAGlobal burden of strokeCirc Res2017120343928154096
- National Stroke FoundationWalk in Our Shoes. Stroke Survivors and Carers Report on Support After StrokeMelbourneNational Stroke Foundation2007
- SturmJWDonnanGADeweyHMQuality of life after stroke: the North East Melbourne Stroke Incidence Study (NEMESIS)Stroke200435102340234515331799
- HankeyGJStroke Treatment and Prevention: An Evidence-Based ApproachMelbourneCambridge University Press2005
- MohanKMWolfeCDARuddAGHeuschmannPUKolominsky-RabasPLGrieveAPRisk and cumulative risk of stroke recurrence: a systematic review and meta-analysisStroke20114251489149421454819
- National Stroke FoundationClinical Guidelines for Acute Stroke ManagementMelbourneNational Stroke Foundation2010
- National Stroke FoundationNational Stroke Audit: Acute Services Report 2015MelbourneNational Stroke Foundation2015
- AndrewNEKilkennyMNaylorRNational Stroke FoundationUnderstanding long-term unmet needs in Australian survivors of strokeInt J Stroke20149Suppl A10010611225042019
- CadilhacDLanninNAAndersonCKimJAndrewNEKilkennyMThe Australian Stroke Clinical Registry Annual Report 2014Melbourne, AustraliaThe Florey Institute of Neuroscience and Mental Health2015
- ForsterABrownLSmithJInformation provision for stroke patients and their caregiversCochrane Database Syst Rev201211CD00191923152210
- RosewilliamSRoskellCAPandyanADA systematic review and synthesis of the quantitative and qualitative evidence behind patient-centred goal setting in stroke rehabilitationClin Rehabil201125650151421441308
- D’CruzKUnsworthCRobertsKEngaging patients with moderate to severe acquired brain injury in goal settingInt J Ther Rehabil2016231213
- GrimmerKMossJFalconJKindnessHIncorporating patients and carer concerns in discharge plan: the development of a practical patient-centered checklistInternet Journal of Allied Health Sciences and Practice2006418
- PietteJDListJRanaGKTownsendWStriplinDHeislerMMobile health devices as tools for worldwide cardiovascular risk reduction and disease managementCirculation2015132212012202726596977
- KamalAKShaikhQPashaOA randomized controlled behavioral intervention trial to improve medication adherence in adult stroke patients with prescription tailored Short Messaging Service (SMS)-SMS4Stroke studyBMC Neurol20151521226486857
- SmithGCEgbertNDellman-JenkinsMNannaKPalmieriPAReducing depression in stroke survivors and their informal caregivers: a randomized clinical trial of a Web-based interventionRehabil Psychol201257319620622946607
- DeharM-ACasswellSDuignanPFormative and process evaluation of health promotion and disease prevention programsEval Rev1993172204220
- HarrisPATaylorRThielkeRPayneJGonzalezNCondeJGResearch electronic data capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics supportJ Biomed Inform200942237738118929686
- KaneDWHohmanMMCeramiEGMcCormickMWKuhlmmanKFByrdJAAgile methods in biomedical software development: a multi-site experience reportBMC Bioinformatics2006727316734914
- ChowCKRedfernJHillisGSEffect of lifestyle-focused text messaging on risk factor modification in patients with coronary heart disease: a randomized clinical trialJAMA2015314121255126326393848
- RedfernJThiagalingamAJanSDevelopment of a set of mobile phone text messages designed for prevention of recurrent cardiovascular eventsEur J Prev Cardiol201421449249922605787
- CameronJLuggEFrancisKDevelopment of SMS text messages for heart failure patients promoting self-care (abstract)Australian Cardiovascular Health and Rehabilitation Annual Scientific MeetingAugust 8–10; 2016Adelaide, Australia
- YipAMGormanMCStadnykKMillsWGMacPhersonKMRockwoodKA standardized menu for Goal Attainment Scaling in the care of frail eldersGerontologist19983867357429868853
- McKevittCFudgeNRedfernJSelf-reported long-term needs after strokeStroke20114251398140321441153
- AndrewNEKilkennyMFLanninNACadilhacDAIs health-related quality of life between 90 and 180 days following stroke associated with long-term unmet needs?Qual Life Res20162582053206226847339
- World Health OrganizationICF: International Classification of Functioning, Disability and HealthGenevaWorld Health Organization2001
- ProchaskaJODiClementeCCStages and processes of self-change of smoking: toward an integrative model of changeJ Consult Clin Psychol19835133903956863699
- AbrahamCMichieSA taxonomy of behavior change techniques used in interventionsHealth Psychol200827337938718624603
- EamesSHoffmannTWorrallLReadSStroke patients’ awareness of risk and readiness to change behaviorsTop Stroke Rehabil201118548148922082699
- GarnerCPageSJApplying the transtheoretical model to the exercise behaviors of stroke patientsTop Stroke Rehabil2005121697515736002
- GongJChenXLiSEfficacy of a Community-based physical activity program KM2H2 for stroke and heart attack prevention among senior hypertensive patients: a cluster randomized controlled Phase-II trialPLoS One20151010e013944226426421
- WhiteNDLenzTLSmithKTool guide for lifestyle behavior change in a cardiovascular risk reduction programPsychol Res Behav Manag20136556323983496
- FrancisJJO’ConnorDCurranJTheories of behaviour change synthesised into a set of theoretical groupings: introducing a thematic series on the theoretical domains frameworkImplement Sci201273522531601
- FrenchSDGreenSEO’ConnorDADeveloping theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the Theoretical Domains FrameworkImplement Sci201273822531013
- Cole-LewisHKershawTText messaging as a tool for behavior change in disease prevention and managementEpidemiol Rev2010321566920354039
- FjeldsoeBSMarshallALMillerYDBehavior change interventions delivered by mobile telephone short-message serviceAm J Prev Med200936216517319135907
- JimisonHGormanPWoodsSBarriers and Drivers of Health Information Technology Use for the Elderly, Chronically III, and UnderservedRockvilleAgency for Healthcare Research and Quality2008
- Australian Communications and Media AuthorityDigital Lives of Older Australians: Research SnapshotsCanberraACMA2016
- World Health OrganisationThe International Classification of Functioning, Disability and Health (ICF)2001 Available from: http://apps.who.int/classifications/icfbrowser/Accessed June 8, 2018
- CarverCSScheierMFControl theory: a useful conceptual framework for personality–social, clinical, and health psychologyPsychol Bull19829211111357134324
- FisherJDFisherWAChanging AIDS-risk behaviorPsychol Bull199211134554741594721
- BanduraASelf-efficacy: toward a unifying theory of behavioral changePsychol Rev1977842191215847061
- FishbeinMA theory of reasoned action: some applications and implicationsNebr Symp Motiv198027651167242751
- AjzenIThe theory of planned behaviourOrgan Behav Hum Decis Process1991502179211
- RollnickSMillerWRWhat is motivational interviewing?Behav Cogn Psychother1995234325334
- WilsonJTLHareendranAGrantMImproving the assessment of outcomes in stroke. Use of a structured interview to assign grades on the modified Rankin ScaleStroke20023392243224612215594