
Abstract
Objectives
Our aim was to study whether the acute care of frail elderly patients directly admitted to a comprehensive geriatric assessment (CGA) unit is superior to the care in a conventional acute medical care unit in terms of patient satisfaction.
Design
TREEE (Is the TReatment of frail Elderly patients Effective in an Elderly care unit?) is a clinical, prospective, controlled, one-center intervention trial comparing acute treatment in CGA units and in conventional wards.
Setting
This study was conducted in the NÄL-Uddevalla county hospital in western Sweden.
Participants
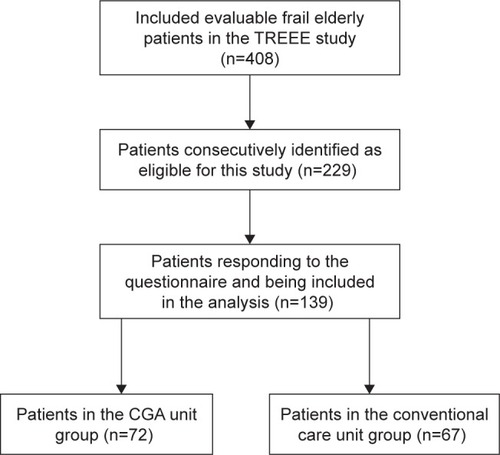
In this follow-up to the TREEE study, 229 frail patients, aged ≥75 years, in need of acute in-hospital treatment, were eligible. Of these patients, 139 patients were included in the analysis, 72 allocated to the CGA unit group and 67 to the conventional care group. Mean age was 85 years and 65% were female.
Intervention
Direct admittance to an acute elderly care unit with structured, systematic interdisciplinary CGA-based care, compared to conventional acute medical care via the emergency room.
Measurements
The primary outcome was the satisfaction reported by the patients shortly after discharge from hospital. A four-item confidential questionnaire was used. Responses were given on a 4-graded scale.
Results
The response rate was 61%. In unadjusted analyses, significantly more patients in the intervention group responded positively to the following three questions about the hospitalization: “Did you get the nursing from the ward staff that you needed?” (p=0.003), “Are you satisfied with the information you received on your diseases and medication?” (p=0.016), and “Are you satisfied with the planning before discharge from the hospital?” (p=0.032). After adjusted analyses by multiple regression, a significant difference in favor of the intervention remained for the first question (p=0.027).
Conclusion
Acute care in a CGA unit with direct admission was associated with higher levels of patient satisfaction compared with conventional acute care via the emergency room.
Introduction
Background
Frailty is a biological syndrome reflecting vulnerability to stressors and reduced physiological reserves.Citation1 It is associated with functional decline, activity limitations, prolonged recovery, and a high risk of being institutionalized and dying.Citation2–Citation5 Among older persons, the prevalence of frailty is estimated to be 10%–60%, depending on the frailty assessment instrument used and the population studied.Citation6,Citation7 Most of these patients have multiple chronic diseases and recurring episodes of acute illness.
Frail elderly individuals constitute a high percentage of emergency patients in every hospital. The current organization of acute care is often poorly adapted to the specific needs of these patients. To meet these needs, in 2008, the NU (NÄL-Uddevalla) hospital group in the Västra Götaland Region of Sweden introduced two acute elderly care comprehensive geriatric assessment (CGA) units (MÄVAs).Citation8 The basic aims were to optimize the clinical treatment and thereby utilize health care resources in the best way. This form of care is characterized by direct admission and a structured, systematic multi- and interdisciplinary CGA and care performed in the ward, including an early rehabilitation strategy involving physicians, occupational therapists, physiotherapists, and nurses as active team members.
Previous clinical studies have indicated that frail elderly patients could benefit from a CGA.Citation9–Citation14
Patient satisfaction is an important patient-reported experience measure, and it can also be seen as an outcome in itself and as an integrated part of the results of every type of health care organization. It has been described as crucial for the evaluation of health care quality.Citation15,Citation16 In accordance with the consumer model, satisfaction can be regarded as a difference between expectations and assessed performance.Citation17 On the other hand, it has been argued that it might be problematic to treat elderly patients as consumers.Citation18 Patient satisfaction can also be defined as measuring the needs and wants,Citation19 and it influences patient compliance as well as continuity of care.Citation20,Citation21
Importance
In acute care settings, there is, however, a lack of knowledge regarding the effects of CGA on health-related quality of life (HRQoL) and even more so on patient satisfaction. In the TREEE study (Is the TReatment of frail Elderly patients Effective in an Elderly care unit?), the results on HRQoL, activities of daily living (ADLs), mortality, and re-hospitalizations were favorable for the CGA units as described previously.Citation14
In severely frail elderly patients with poor prognosis who need emergency care, the satisfaction with the received hospital care may be particularly important.
Goals of the investigation
Our aim in this follow-up of the TREEE study was to evaluate whether the acute care of frail elderly patients directly admitted to a CGA unit is superior to conventional acute medical care in terms of patient satisfaction. We hypothesized that a higher proportion of patients cared for in a CGA unit would report satisfaction compared with patients treated in a conventional care unit.
Patients and methods
Study design and setting
This study on patient satisfaction used data from the TREEE study, a clinical, prospective, controlled intervention trial with two parallel groups performed at the NU hospital group between March 2013 and July 2015. Details of TREEE have been described earlier.Citation14 The total primary population of the NU health care system is 280,000 inhabitants. The TREEE study was approved by the Independent Ethics Committee at the Sahlgrenska University Hospital in Gothenburg (8883-12, 20121212) and registered at the Swedish National Database of Research and Development (identifier: 113021). Written informed consent was obtained from the patients or from a member of their next of kin. All data were computerized and handled in accordance with legislation and Good Clinical Practice.
Selection of participants
TREEE included patients aged ≥75 years, in need of in-hospital treatment, and who fulfilled the foundation of frailty in accordance with the recently validated FRESH (FRail Elderly Support researcH group) screening instrument,Citation22 that is, two or more of the following criteria: tiredness from a short walk, general fatigue, frequent falls/anticipation of falls, dependence in shopping, and three or more visits to the emergency ward during the last 12 months. Patients were excluded if they were clearly suited for care in a conventional acute medical care unit due to the type or severity of the acute illness.
When the ambulance nurse, or the primary care physician, had identified a patient who could fulfill the inclusion criteria, a MÄVA doctor was contacted via telephone. If he/she agreed, and there was a bed available at MÄVA, the patient was allocated to the intervention group and admitted directly to MÄVA. If bed was not available, the patient was allocated to the control group and admitted to a conventional acute medical care unit through the emergency room.
In the TREEE study, 408 patients were included between March 2013 and July 2015. For practical and resourcing reasons, we could not start the distribution of the questionnaire on patient satisfaction until February 2014. Between February 2014 and July 2015, 229 patients were consecutively considered to be eligible in this part of the TREEE study ().
Figure 1 Flowchart of participant selection and assessment.
Intervention and control
Intervention group
In addition to care in accordance with national and international guidelines, the CGA units are characterized by a structured, systematic interdisciplinary CGA and care via direct admittance to the wards (). The CGA involves physicians, nurses, occupational therapists, and physiotherapists as active team members. This implies a broad focus on physiological, psychological, and social factors via validated instruments, focusing on somatic and mental health, medication review, functional and activity ability including early rehabilitation, social situation, and early discharge planning. This also includes care guidance, adjusted to the needs of frail elderly patients. In order to individualize the assessment and treatment, the team has a person-centered approach. There are educational sessions in the intervention, including advice regarding physical exercise after discharge. There is a specially trained nurse responsible for the planning before discharge, with established contacts in primary care, home health care, and other types of support facilities.
Table 1 Comparison of the management in the intervention group (CGA) and the control group (conventional acute medical care)
A formal discussion with the patient and relatives and a total medicine treatment evaluation are included in the routine.
Control group
Patients are admitted to a conventional acute medical care unit via the emergency room, using standard clinical care and procedures in accordance with national and international guidelines. For both the groups, bedside medical examinations, electrocardiograms (ECGs), medical referrals, laboratory testing, X-ray examinations, blood transfusions, nutritional therapy, and drug treatment are included.
Methods and measurements
The data collection has previously been described in detailCitation14 and is therefore only briefly repeated here.
Clinical and demographic characteristics
These data were collected at the index hospitalization: age, gender, housing, diabetes mellitus, renal function, heart failure, other comorbidities, mini nutritional assessment (MNA-short form), and numbers of in-hospital care days.
The Charlson index score
Charlson’s comorbidity index (CCI) is a measurement of the total morbidity.Citation23 It consists of 19 comorbidities, each of which is given a severity weighting depending on the risk of dying associated with this condition. The CCI was completed from medical records by the assessing physician.
The FRESH screening instrument
Frailty was assessed using the FRESH screening instrument,Citation22 which is a validated screening instrument for frailty shown to be appropriate in an emergency hospital setting. It consists of five questions (see the “Selection participants” section). The FRESH screening instrument was performed by a physician or a nurse at the time of inclusion.
ADL
ADL independence/dependence was assessed by using the ADL Staircase before discharge.Citation24 This instrument consists of five personal ADL (PADL) items (ie, feeding, transferring, going to the toilet, dressing, and bathing), extended by four instrumental ADL (IADL) items (ie, cooking, shopping, cleaning, and transportation). The ADL Staircase was administered through interview and, if possible, observation.
The satisfaction questionnaire
From February 2014 to July 2015, the patients were provided with a confidential satisfaction questionnaire to be filled in shortly after discharge from hospital by the patient alone, or with the help of relatives. The patient satisfaction questions were based on the experience with physicians and other team members in the MÄVA units and on questions and topics often brought up by patients and relatives. The aim was to create simple, clinically relevant questions, easy to respond to by ticking one of four options. The questions were carefully discussed internally, and we consulted broadly with geriatric expertise. Questions of the same kind have been used before,Citation25–Citation27 but not previously been formally validated in an acute care context.
The questionnaire included four questions regarding patient satisfaction during the hospitalization period:
Did you get help from the doctors with the medical problems you came in for? (1)
Did you get the nursing from the ward staff that you needed? (2)
Are you satisfied with the information you received on your diseases and medication? (3)
Are you satisfied with the planning before discharge from the hospital? (4)
The alternatives for answers to the questions were: (1) Great help, fairly great help, little help and very little help; (2) Yes always, yes often, no not often, and no seldom; (3) and (4) Very satisfied, fairly satisfied, fairly unsatisfied, and very unsatisfied.
Outcomes
The primary outcome was the level of satisfaction on each question reported by the patient after the index hospitalization.
Analysis
For the TREEE study, it was estimated that 200 evaluable patients should be included in each study group.Citation14 The two first response alternatives to each of the four questions were considered as positive, the remaining two responses to each question were considered as negative, that is, for each question, the responses were dichotomized before analysis. The data were computerized and analyzed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, Version 22.0; IBM Corporation, Armonk, NY, USA). Student’s t-test was used to compare the continuous, parametric data between the groups, and the χ2 test or Fisher’s exact test was used to compare the categorical data. Adjustments for possible differences at baseline were made, using a logistic regression model including age, gender, and CCI score as covariates.
Results
Characteristics of study subjects
In this follow-up to the TREEE study, 229 frail patients were consecutively identified to be eligible. Of these patients, 139 patients being allocated to the CGA unit group (n=72) or conventional ward group (n=67) responded to the questionnaire and were included in the analysis. The response rate was 61%.
Baseline clinical and demographic characteristics are presented in . The two groups did not differ significantly in terms of age, gender, scores of ADL and MNA, and percentage living in residential care (all p>0.05). The intervention group presented with higher scores of frailty (p=0.046) and Charlson comorbidity index (p<0.001). Both the groups were heavily affected by diseases, particularly cardiovascular disease. Furthermore, dependence or difficulty carrying out PADL or IADL were common among the participants in both the groups.
Table 2 Baseline clinical and demographic characteristics of the intervention and control group patients who responded to the satisfaction questionnaire
Main results
The responses to the four questions of the satisfaction questionnaire are reported in . For each question, the proportions of chosen alternatives on the 4-graded scale are referenced. In the intervention group, the responses were given by the patient alone in 36 cases, a next-of-kin in 11 cases, and a combination in 25 cases. In the control group, the responses were given by the patient alone in 28 cases, a next-of-kin in 11 cases, and a combination in 28 cases.
Table 3 The responses of patients in each group to the four questions of the satisfaction questionnaire, n (%)
Unadjusted analysis of the dichotomized responses of the questionnaire is shown in . Significantly more patients in the intervention group responded positively to the following three questions: “Did you get the nursing from the ward staff that you needed?” (p=0.003), “Are you satisfied with the information you received on your diseases and medication?” (p=0.016), and “Are you satisfied with the planning before discharge from the hospital?” (p=0.032). There was no difference between the groups in response to the question “Did you get help from the doctors with the medical problems you came in for?” (p=0.120).
Table 4 Unadjusted analysis of the dichotomized responses
After adjusting for age, gender, and Charlson’s index in multiple regression analyzes, a statistically significant difference in favor of the intervention remained for the second question “Did you get the nursing from the ward staff that you needed?” (p=0.027). Neither regarding the question “Are you satisfied with the information you received on your diseases and medication?” (p=0.059), nor for the responses of the other two questions (both p>0.05), there were any statistically significant differences in favor of the intervention group. For the questions “Are you satisfied with the information you received on your diseases and medication?” and “Are you satisfied with the planning before discharge from the hospital?” there was a correlation between satisfaction and higher age (both p<0.05).
Discussion
Our study shows that acute care of elderly, frail patients directly admitted to a CGA unit was associated with significantly higher levels of patient satisfaction compared with conventional acute care for three of the four components registered.
This difference in favor of the intervention remained partly also after adjusting for age, gender, and comorbidity with a statistically significant difference for the question “Did you get the nursing from the ward staff that you needed?”
In both the study groups, a broad majority of the patients reported overall positive satisfaction scores. Furthermore, for two of the questions, there was an association between positive answers and high age. This harmonizes with previous studies, indicating an association between patient satisfaction and age,Citation28,Citation29 particularly among female elderly patients.Citation19 In the current study, the mean age was 85 years, and the majority were females.
There is a growing evidence in favor of CGA units for frail elderly patients. The CGA and related care can be considered a complex intervention. Consequently, there may be several critical differences compared to conventional care, which may interact and benefit frail elderly patients with accompanying higher patient satisfaction.
The previously reported results of the broader study indicates that well-structured team-based acute care for frail elderly patients in a CGA unit is superior to the care in a conventional acute medical care unit in terms of several clinically meaningful outcomes. The satisfaction results might be linked to these positive outcomes from the TREEE study.Citation14
Moreover, in recent studies, it has been emphasized that patient involvement, participation, and communicating with patients about motivations and expectations might lead to higher satisfaction.Citation19,Citation30,Citation31 A person-centered approach in order to individualize the assessment and treatment, which was applied by the team in the intervention group, might have facilitated these values.
Furthermore, patients in the intervention group were directly admitted to the CGA care unit. In a previous study in an emergency context, long waiting times at the reception were associated with dissatisfaction.Citation32–Citation34 It can also be hypothesized that longer hospital stay in the intervention group made it possible to optimize the medical treatment, to inform the patients and relatives in more detail and to perform a more extensive care planning in cooperation with other care-givers. This might be another part of the explanation for the higher satisfaction in the CGA group.
Elderly patients are so severely affected by frailty and multi-morbidity as our study patients generate a large part of everyday hospital care consumption in most western countries. There is therefore a particular need to build evidence relating to the treatment and care of this important patient group. Patient satisfaction is an integrated and important part of that work. This study was integrated in the standard daily clinical context and included a wide spectrum of diagnoses, which enhances the generalizability of the study results. Moreover, we studied very frail elderly patients in need of acute care, which adds complementary knowledge to former studies focusing on patients in a more stable and chronic phase.
The MÄVA form of care can serve as one example of how acute care for frail elderly people can be organized. More research is needed to identify the most appropriate organizational forms adapted to the varying needs of the frail elderly patients, for example, stable chronic disease and acute illness. This further research should include evaluations of primary and municipal care, ambulant geriatric care, and specialized hospital care. In every such study, the evaluation of patient satisfaction should be an important part.
Limitations
Our patient satisfaction study has some limitations, the main one being that the questions used in this survey are not formally validated. However, we wanted to take the opportunity to capture the opinions of our patients on these few, short, and clinically relevant questions. In addition, we did not find any validated instrument that fulfilled the needs of the TREEE study. The questions were based on available literature and intense discussions and broad consultations with experts. Another limitation is the low number of patients. However, the response rate of 61% is in the range of what has previously been reported in this kind of population.
Conclusion
Acute care in a CGA unit with direct admission was associated with higher levels of patient satisfaction compared with conventional acute care via the emergency room.
Acknowledgments
This study was funded by grants from the Healthcare subcommittee, Region Västra Götaland; Department of Research and Development, NU Hospital Group; and the Fyrbodal Research and Development Council, Region Västra Götaland, Sweden.
Disclosure
The authors report no conflicts of interest in this work.
References
- BergmanHFerrucciLGuralnikJFrailty: an emerging research and clinical paradigm. Issues and controversiesJ Gerontol A Biol Sci Med Sci20076273173717634320
- FriedLPTangenCMWalstonJFrailty in older adults: evidence for a phenotypeJ Gerontol A Biol Sci Med Sci200156146156
- RockwoodKSongXMacKnightCA global clinical measure of fitness and frailty in elderly peopleCan Med Assoc J200517348949516129869
- ShamliyanTTalleyKMCRamakrishnanRKaneRLAssociation of frailty with survival: a systematic literature reviewAgeing Res Rev20121271973622426304
- ButaBJWalstonJDGodinoJGFrailty assessment instruments: Systematic characterization of the uses and contexts of highly-cited instrumentsAgeing Res Rev201626536126674984
- AfilaloJKarunananthanSEisenbergMJAlexanderKPBergmanHRole of frailty in patients with cardiovascular diseaseAm J Cardiol20091031616162119463525
- CollardRMBoterHSchoeversRAOude VoshaarRCPrevalence of frailty in community-dwelling older persons: a systematic reviewJ Am Geriatr Soc2012601487149222881367
- JohanssonMJohanssonPMultisjuka äldre med upprepade vårdtillfällen bör läggas in direktLäkartidningen201210910221023 Swedish22741406
- EkdahlAWWirehnABAlwinJCosts and effects of an ambulatory geriatric unit (the AGe-FIT study): a randomized controlled trialJ Am Med Dir Assoc201516649750325703450
- PrestmoAHagenGSletvoldOComprehensive geriatric care for patients with hip fractures: a prospective, randomised, controlled trialLancet20153851623163325662415
- EllisGGardnerMTsiachristasAComprehensive geriatric assessment for older adults admitted to hospitalCochrane Database Syst Rev20117CD006211
- SBUComprehensive geriatric assessment and care of frail elderlyStockholmSwedish Council on Health Technology Assessment (SBU)2014 SBU report no 221 (in Swedish). Available from: http://www.sbu.se/upload/Publikationer/Content0/1/Akutvard_aldre.pdfAccessed May 7, 2016
- BaztánJJSuárez-GarcíaFMLópez-ArrietaJRodríguez-MañasLRodríguez-ArtalejoFEffectiveness of geriatric units on functional decline, living at home, and case fatality among older patients admitted to hospital for acute medical disorders: meta-analysisBMJ2009338b5019164393
- EkerstadNKarlsonBWDahlin IvanoffSIs the acute care of frail elderly patients in a comprehensive geriatric assessment unit superior to conventional acute medical care?Clin Interv Aging2017121928031704
- DanielsenKBjertnaesOGarrattAForlandOIversenHHHunskaarSThe association between demographic factors, user reported experiences and user satisfaction: results from three casualty clinics in NorwayBMC Fam Pract2010117320925930
- PrakashBPatient satisfactionJ Cutan Aesthet Surg20103315115521430827
- ClausenGBorcheltMJanssenCPatient satisfaction and geriatric care – an empirical studyZ Gerontol Geriatr200639485616502227
- OwensDJBatchelorCPatient satisfaction and the elderlySoc Sci Med19964211148314918771631
- ChumblerNROtaniKDesaiSPHerrmannPAKurzRSHospitalized older adults’ patient satisfactionSAGE Open2016617
- LinnLSFactors associated with patient satisfaction of healthcareMilbank Mem Fund Q Health Soc1975535315481044424
- XiaoHBarberJPThe effect of perceived health status on patient satisfactionValue Health20081171972518179667
- EklundKWilhelmsonKLandahlSIvanoff-DahlinSSynneveIDScreening for frailty among older emergency department visitors: validation of the new FRESH-screening instrumentBMC Emerg Med2016162727449526
- CharlsonMPompeiPAlesKLMacKenzieCRA new method of classifying prognostic comorbidity in longitudinal studies: development and validationJ Chronic Dis1987403733833558716
- SonnUHulter-ÅsbergKAssessment of activities of daily living in the elderlyScand J Rehabil Med1991231932021785028
- ArnetzJEArnetzBThe development and application of a patient satisfaction measurement system for hospital-wide quality improvementInt J Qual Health Care199685555669007605
- BroadbentEPetrieKJMainJWeinmanJThe brief illness perception questionnaireJ Psychosom Res20066063163716731240
- BerglundHWilhelmsonKBlombergSDunérAKjellgrenKHassonHOlder people’s views of quality of care: a randomized controlled study of continuum of careJ Clin Nurs2013222934294423808647
- BeneJListonRNelsonLElderly patients’ satisfaction with hospital careJ R Coll Physicians Lond19983221381419597630
- PeckBAge-related differences in doctor-patient interaction and patient satisfactionCurr Gerontol Geriatr Res2011201113749
- LiWWangSZhangYRelationships among satisfaction, treatment motivation, and expectations in orthodontic patients: a prospective cohort studyPatient Prefer Adherence20161044344727110100
- KeitaIAubin-AugerILalanneCAssessment of quality of life, satisfaction with anticoagulation therapy, and adherence to treatment in patients receiving long-course vitamin K antagonists or direct oral anticoagulants for venous thromboembolismPatient Prefer Adherence2017111625163429026288
- TaylorCBengerJRPatient satisfaction in emergency medicineEmerg Med J20042152853215333521
- HedgesJRTroutAMagnussonARSatisfied patients exiting the emergency department (SPEED) studyAcad Emerg Med20029152111772664
- RahmqvistMBaraACPatient characteristics and quality dimensions related to patient satisfactionInt J Qual Health Care201022869220133477