
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose
This study aimed to determine the factors that influence patient satisfaction with ecdemic medical care.
Materials and methods
Eight hundred and forty-four face-to-face interviews were conducted between October and November 2017 in two high-profile hospitals in Nanchang, China. Patient satisfaction was divided into lowest and highest satisfaction groups according the 80/20 rule. Demographic factors associated with patient satisfaction were identified by logistic regression models.
Results
Respondents’ main reasons for choosing a non-local hospital were “high level of medical treatment” (581/844), “good reputation of the hospital” (533/844), and “advanced medical equipment” (417/844). The top three items that dissatisfied the ecdemic patients were “long time to wait for treatment” (553/844), “complicated formalities” (307/844), and “poor overall service attitude” (288/844). Fewer female patients (adjusted odds ratio [AOR] =1.47, 95% confidence interval [CI] =1.03–2.11), patients with a family per-capita monthly income (FPMI) between 3,001 and 5,000 CNY (AOR =1.40, 95% CI =1.01–2.17), inpatients (AOR =1.46, 95% CI =1.01–2.13), and more patients with an FPMI >7,000 CNY (AOR =0.43, 95% CI =0.20–0.92) were detected in the lowest satisfaction group. Fewer patients with an associate’s or bachelor’s degree (AOR =2.40, 95% CI =1.37–4.20) and patients with an FPMI >7,000 CNY (AOR =3.02, 95% CI =1.10–8.33) were detected in the highest satisfaction group. Moreover, more inpatients (AOR =0.70, 95% CI =0.54–0.97) and those aged 46–65 years (AOR =0.63, 95% CI =0.33–0.98) were detected in the highest satisfaction group.
Conclusion
Findings suggested that managers of the medical facilities should note the importance of increasing their publicity through a rapidly developing media, as well as the necessity of creating a more patient-friendly medical care experience. Hospitals should also focus on the medical care experience of patients with relatively lower and higher income levels, male ecdemic patients, and ecdemic outpatients.
Introduction
The distribution of health resources among different areas and cities varies greatly in China.Citation1–Citation3 High-quality health resources are mainly allocated in megacities such as Beijing, Shanghai, Guangzhou and major provincial capitals such as Wuhan, Chengdu, and Nanjing.Citation1,Citation3 Therefore, facing such an uneven distribution of health resources leaves no choice but to travel to big cities in order to access high-quality health resources for residents living in areas where health resources are relatively scarce.Citation4 These patients are termed as “ecdemic patients” in China, and this care-seeking behavior is called “the ecdemic medical care/treatment” in China. Since the economic reform in the 1970s, many changes have taken place in China. The disease spectrum of Chinese people and general attitudes toward health have transformed.Citation5–Citation7 The demand for better health services of Chinese nationals is still increasing with greatly improved living standards.Citation4,Citation8 Consequently, such alterations have increased the prevalence of the ecdemic medical care/treatment.
The ecdemic medical care in this article specifically refers to a patient who receives medical services in any place outside an individual’s officially registered residence location.Citation4 The recent completion of the high-speed railway and expressway network have expedited intercity travel and have made the ecdemic medical care much easier. Moreover, according to the 2017 Report on China’s Migrant Population Development, 292 million residents had lived in a location away from their officially registered location of residence for more than 6 months in 2016.Citation9 Meanwhile, the 2016 Statistical Communiqué of the People’s Republic of China on National Economic and Social Development records a number of 169.34 million migrant rural workers living in Chinese urban areas.Citation10 An evident result of this is that when those migrant rural workers seek medical treatment, they are most likely to turn to the hospitals nearby instead of the hospitals in their hometown, which is most likely their formally registered location of residence.Citation4 Hence, there are a large number of people who have had previous experience of the ecdemic medical care in China.
The Chinese government has realized the fact that there are a large number of patients who get medical treatment away from home and that the numbers are still rising rapidly. Therefore, the Chinese government has been trying to solve this issue, including establishing a direct medical insurance payment system for the ecdemic patients, building a national network for basic health care insurance, and strengthening the cooperation among administration departments of health care in different cities.Citation11–Citation14 These measures had effectively lessened the medical economic burden on ecdemic patients, met the demand for the ecdemic medical care to some extent, and increased the degree of satisfaction with health care services among ecdemic patients.Citation11,Citation13,Citation14
Patient satisfaction is a key measurement of the quality of medical service, as it directly assesses medical service from the perspective of patients toward health care.Citation15,Citation16 The National Health Service system can affect patient satisfaction.Citation17,Citation18 However, as the direct provider of medical service, hospitals have the ability to promote patient satisfaction by improving the quality of medical services on their side.Citation19–Citation23 Government and the related policies, on the other hand, have a more limited impact on the improvement of patient satisfaction. In response to the severity of the conflict between doctors and patients,Citation24,Citation25 Chinese hospitals are now attempting to provide services in all aspects using the principles for patient-centered care, which may improve their service quality and efficiency, and enhance the timeliness and rationality of their decision-making on health care.Citation26–Citation28 In this process, patients, especially the ecdemic patients, can provide valuable opinions and suggestions that are crucial toward the development of hospitals. Therefore, a large number of medical facilities have added great importance to the evaluation of patient satisfaction with their medical experience, and have conducted many routine satisfaction surveys and initiatives.
Current studies on patient satisfaction have been conducted primarily to focus on the general population or groups with certain diseases, such as cancer patients.Citation15–Citation17,Citation19–Citation23,Citation25–Citation27,Citation29 Some empirical studies are conducted in developed countries, focusing on patient mobility and its influencing factors.Citation30–Citation32 However, few research studies have specifically targeted the ecdemic patients in China. Therefore, this study considered such a population group as its object and aimed to investigate the reasons underlying their preference for specific hospitals, to determine the causes of unsatisfactory experiences in the medical facilities, and to explore differences in satisfaction between patients with different demographic statistics. Moreover, this study can also provide references for hospitals to improve their service and for policymakers to establish or adjust relevant policies.
Materials and methods
Material sources
The present survey was conducted in Nanchang – the capital city of Jiangxi province as well as being one of the megacities located in the economic belt of middle reach of Yangtze River. Nanchang is a major transportation hub connecting the prosperous coastal areas of Southeast China. Convenient transportation provides access for residents from other places to seek high-quality medical care services in Nanchang. We selected the First Affiliated Hospital of Nanchang University and Jiangxi Zhonghuan Hospital, because these two comprehensive hospitals are a good representation of the high-profile public hospitals and private hospitals in Jiangxi province, respectively. They accept the largest number of patients living outside of Nanchang city.
Data collection and sampling
According to the study design, patients (or their caregivers) from other areas who were aged ≥18 years were considered to be within the inclusion criteria of survey participants. The qualified participants (non-local household registration – known as “hukou” in Chinese) were briefly told about our study and were asked about their willingness to participate in the study. Convenience sampling strategy was used to carry out the investigation. Between October and November 2017, trained public health graduate students collected the data by means of face-to-face interviews. Our survey was conducted from 9 AM to 4 PM each day, excluding Saturday afternoons and Sundays (the hospitals provide services only to inpatients and do not operate during these times).
Questionnaire
The questionnaire used in this study was based on the Improvement and Assessment of Patient Satisfaction Questionnaire in General Hospitals.Citation29 There was sufficient evidence for reliability and construct validity of this questionnaire; the Cronbach’s alpha coefficient of the questionnaire was 0.912, and the Cronbach’s alpha coefficients of all dimensions ranged from 0.669 to 0.801. We also designed the basic social demographic characteristic questionnaire based on local circumstances and specific needs of this study. Participants were also asked to list their main reasons for choosing a non-local hospital and the most unsatisfactory items for the hospital that served them. The majority of the questions in the original edition used a 5-point Likert scale. It is hard to differentiate patient satisfaction, as most respondents may choose “neutral” (scored 3) if using the 5-point Likert scale.Citation29 In the current study, we used a 9-point Likert scale, where a higher score indicated higher patient satisfaction. We also measured the internal reliability of our questionnaire, and the Cronbach’s alpha coefficient was 0.902.
Sample size calculation
The sample size for this study was determined according to the formula for the cross-sectional survey study as follows: ,Citation33 where n is the sample size, π is the over all satisfaction rate, and δ is the desired level of precision. The overall satisfaction rate was obtained from pre-survey (n=87), and it was 78.67%. Meanwhile, we desired a 95% confidence level and 5% precision; hence the sample size was calculated to be:
, rounded to 258. However, we got 844 valid questionnaires, which was far more than expected. Hence, there should be adequate power for analyses.
Statistical analysis
The IBM SPSS version 22.0 for Windows (IBM Corporation, Armonk, NY, USA) was used to perform all the analyses in this study. An initial descriptive analysis was first conducted. The frequencies and proportions were used to summarize the respondents’ demographic characteristics, their main reasons for choosing a non-local hospital, and the most unsatisfactory items for the hospital that served them. The demographic information of the participants is summarized in . The main reasons for choosing a non-local hospital are shown in , and their most unsatisfactory items are shown in . Patient satisfaction was divided into lower and higher satisfaction groups according the 80/20 rule (also known as Pareto principle).Citation34 The 80/20 rule states that, for many events, roughly 80% of the effects come from 20% of the causes. We believe that these 20% of patients who gave the highest and lowest satisfaction score are the target population that the managers of hospitals should especially focus on. The population with the highest and lowest scores was selected. Then, by using binary logistic regression models, we distinguished the diverse patient satisfaction in different population subgroups. The crude odds ratios (CORs) and adjusted odds ratios (AORs) with 95% confidence interval (CI) obtained from univariate and multivariable logistic regression models are summarized in and , respectively. The p-value of <5% was considered to be statistically significant.
Figure 1 Patients’ main reasons for choosing the hospital.
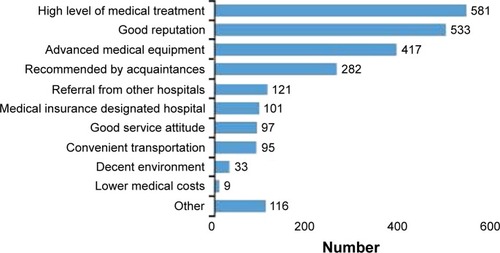
Figure 2 Patients’ most unsatisfactory items regarding hospital services.
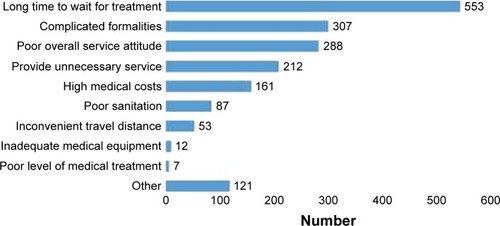
Table 1 Demographic information of the participants (N=844)
Table 2 Logistic regression analysis of influencing factors associated with patient satisfaction (for lowest score group)
Table 3 Logistic regression analysis of influencing factors associated with patient satisfaction (for highest score group)
Quality control
First, the questionnaire was inspected and edited by relevant domestic and international scholars and experts in this field based on the local circumstances and specific needs of this study. Second, the interviewees who carried out the investigation received strict training, and only qualified personnel were eligible for a face-to-face interview. The interviewees were very conscientious and diligent in this survey, because most of them were going to use the data for their graduation thesis. Third, pre-investigations of the target population were conducted to ensure the face validity and comprehension of the survey paper. In addition, we had a meeting every 5 days to discuss the difficulties and improvement suggestions for the interview. Finally, by using Excel 2010 (Microsoft Corporation, Redmond, WA, USA) each completed questionnaire was separately imported into two different databases by two students, and then it was cross-verified. Only the variables that were exactly the same in the two databases were considered accurate and the rest were further compared with the original questionnaire.
Ethical statement
The study protocol was reviewed and approved by the Research Ethics Board of Provincial Postgraduate Innovation Projects and School of Health Sciences of Wuhan University (IRB No YC2015-S039). Informed consent information was attached on the top of each questionnaire and presented before the surveys. The participants completed and signed the informed consent documents.
Results
Demographic information of the participants
A total of 844 patients participated in our study with 402 males (47.63%) and 442 females (52.37%), of whom most were outpatients (60.07%). Participants aged ≤25, 26–45, 46–65, and >65 years accounted for 32.35%, 34.24%, 25.47%, and 7.94% of the total sample size, respectively. Most of the participants (65.76%) were from rural areas. The participants’ education level was classified as ≤elementary school, middle or high school, associate’s or bachelor’s degree, and ≥master’s degree, accounting for 38.03%, 24.17%, 24.88%, and 12.91% of the total sample size, respectively. Participants’ family per-capita monthly income (FPMI) <3,000 CNY (48.34%) and 3,001–5,000 CNY (38.15%) accounted for the majority of the sample. The largest proportion of the participants’ health insurance type was new-type rural cooperative medical insurance, with 49.53% of the participants insured, followed by medical insurance for urban residents (MIUR), with 28.32% of the participants insured. The demographic information of the survey participants is summarized in .
Main reasons for choosing the hospital
recorded the respondents’ main reasons for choosing the hospital. The top four reasons were: high level of medical treatment, good reputation of the hospital, advanced medical equipment, and recommended by acquaintances.
The most unsatisfactory items for the hospital that served them
records the respondents’ most unsatisfactory items for the hospital that served them. The top four items were: long time to wait for treatment, complicated formalities, poor overall service attitude, and provided unnecessary service.
Analysis of the demographic factors affecting patient satisfaction
The population with the highest and lowest satisfaction was selected according to the 80/20 rule. We found that 20.14% of the respondents scored 1–5 points (lowest satisfaction) and 29.62% scored 8–9 points (highest satisfaction). In order to better understand the bivariate and multivariate associations of patient satisfaction versus demographic factors such as age, gender, education level, marital status, FPMI, household registration, type of patient, and type of health insurance, we obtained the CORs and AORs by implementing univariate and multivariable logistic regression models, respectively.
Analysis of the lowest score group showed that in the univariate logistic regression model, there was a higher proportion of patients with lowest satisfaction who had an associate’s or bachelor’s degree (COR =0.69, 95% CI =0.45–0.99), as compared to those with a ≤elementary school educational background, and a lower proportion of patients with a middle or high school educational background (COR =1.71, 95% CI =1.04–2.80). Compared to those with an FPMI ≤3,000 CNY, more patients with an FPMI >7,000 CNY were detected in the lowest satisfaction group (COR =0.36, 95% CI =0.19–0.69). Besides, a lower proportion of inpatients (COR =1.41, 95% CI =1.01–2.01) was also found in the lowest satisfaction group. Multivariable logistic regression model reported that a lower proportion of female patients (AOR =1.47, 95% CI =1.03–2.11), patients with an FPMI between 3,001 and 5,000 CNY (AOR =1.40, 95% CI =1.01–2.17), and inpatients (AOR =1.46, 95% CI =1.01–2.13) scored 1–5 points. In addition, a higher proportion of patients with the highest FPMI >7,000 CNY showed the lowest satisfaction (AOR =0.43, 95% CI =0.20–0.92) ().
On the other hand, in terms of the analysis for the highest score group, both univariate logistic regression model and multivariable logistic regression models demonstrated that inpatients were more satisfied with the received medical service (COR =0.68, 95% CI =0.51–0.92; AOR =0.70, 95% CI =0.54–0.97) as compared to outpatients. When compared to younger individuals aged ≤25 years, patients aged 46–65 years (OR =1.61, 95% CI =1.39–2.98) were more satisfied with the received medical service (COR =0.54, 95% CI =0.37–0.79; AOR =0.63, 95% CI =0.33–0.98). However, those with an associate’s or bachelor’s degree showed a lower proportion of the highest satisfaction (COR =2.52, 95% CI =1.65–3.86; AOR =2.40, 95% CI =1.37–4.20). Top earners with an FPMI >7,000 CNY also showed a lower proportion of the highest satisfaction (COR =3.80, 95% CI =1.46–9.87; AOR =3.02, 95% CI =1.10–8.33) ().
Discussion
The present study found that the top four reasons why migrant patients prefer a certain hospital are: high level of medical treatment, good reputation, advanced medical equipment, and recommendation from a friend or family member. The most significant criteria for patients when choosing a hospital were its service and its reputation. The better a facility’s service is and the greater its reputation, the more patients were willing to receive medical treatment there. Improvement of the quality of medical service remains the core part of a hospital’s development, which may be further facilitated by better medical equipment.Citation35,Citation36 Only through expanding a hospital’s medical treatment capabilities, can more people actually be cured and be more satisfied with their medical experience, thereby attracting more patients to visit. Managers of medical facilities should also note the importance of increasing their publicity through a rapidly developing media, as well as the necessity of creating a more patient-friendly medical experience, which will lead to more recommendations from patients to potential patients.
Moreover, the results of our study showed that the top four reasons why ecdemic patients were dissatisfied with their experience at a hospital were long waiting times, complicated formalities and paperwork, poor overall service attitude, and provision of unnecessary services. Among these factors, long waiting times is the most significant one; the number of respondents who selected this option exceeds that of respondents who chose the other ones to a very large degree. The significance of this factor may be explained by the fact that ecdemic patients are already burdened with non-medical costs including travel and accommodation during their trip, and long waiting times will increase such costs.Citation4,Citation7,Citation26,Citation37 The uneven distribution of health care resources, with the best medical facilities and equipment concentrated in large cities and large hospitals, may be the primary cause for long queues.Citation26 Another reason for long waiting times may be that the increased specialization of medical services into professional clinical departments has complicated and elongated the treatment processes. A possible solution to this is the incorporation of Internet technology into medical service. Moreover, studies have shown that job satisfaction of medical staff affects the quality of their service and subsequently patient satisfaction, especially when the staff works under fatigue.Citation38,Citation39 Managers of health care facilities should incentivize their employees and improve their working experience through discreet management and the prevention of working overloads.Citation40,Citation41
Using the 80/20 rule, we especially examined the highest and lowest 20% groups of satisfaction scores. Because the distribution of satisfaction scores skewed in a direction such that it was concentrated around 6 and 7 points, we found 20.14% of the respondents scored 1–5 points (lowest score group), and 29.62% scored 8 or 9 points (highest score group). We investigated whether there were patterns in the demographic information of respondents in the lowest and highest score groups, such that we may identify population groups that the managers of hospitals should especially focus on.
It was found that patients with an FPMI between 3,001 and 5,000 CNY had a higher degree of satisfaction than those with an income below 3,000 CNY. Patients with an FPMI above 7,000 CNY reported an even lower satisfaction score than the population group with an income below 3,000 CNY. Moreover, female patients and inpatients were more satisfied with their medical experience than male patients and outpatients, respectively. The low degree of satisfaction among low-income patients may be due to the fact that constraints in their financial resources make it difficult to pay high treatment costs. Those with higher income are more likely to be dissatisfied, as they have higher demands for health care. In several previous related studies, researchers have demonstrated that female patients had a lower degree of satisfaction than males.Citation19,Citation21,Citation22,Citation26,Citation42,Citation43 This study, however, detected fewer female patients in the lowest satisfaction group, and yet statistically significant differences between male and female groups were also not found in the highest satisfaction group.
Inpatients were more contented with the medical care that they received, partly due to pronounced effects that they experienced during their long-term stay at a hospital, and partly due to the formation of cordial relationships with staff and increased familiarity with the facility. Therefore, hospitals should focus on the medical experience of patients with relatively lower and higher income levels. Some practical measures include: simplifying procedures for claiming reimbursements, providing guidance for low-income patients on such formalities, avoiding prescribing unnecessary treatments to decrease their financial burden, and identifying the expectations and demands of patients with higher income in advance. Moreover, the information desk in each hospital should be fully utilized such that the service for patients is proactive rather than passive. Hospitals should provide navigation for patients to receive examinations or treatments and guide them through any complicated procedures.
Finally, the following limitations can be identified in this study. The confounding factors of patient satisfaction are possibly more than those we investigated. Other factors that may be examined include the distance between the hometown and destination location of ecdemic patients, the type of disease, duration of disease, comorbidities, different clinical department in which a patient receives their treatment, and so on. Since the study was based on a strategy of convenience sampling, such a design may be affected to some extent by sampling bias. Thus, data should be weighted using variables related to the population of reference to achieve better representativeness of the population. However, there were no related previous survey experiences with the sampling frame among this population in China, and the general population characteristics remained unknown. Therefore, we did not weight the data in the present study. Furthermore, the geographic scope of the study was limited. Moreover, the biases related to the face-to-face interviews and non-response bias were not assessed, as only those agreeing to participate were included. Thus, application of the findings to other areas throughout China needs to be done with caution.
Conclusion
This study has clearly shown that the ecdemic patients were more willing to receive the ecdemic medical care in a certain hospital with a high level of medical treatment, good reputation, and advanced medical equipment. Ecdemic patients were mainly dissatisfied with the long waiting times for care, complicated formalities, a poor overall service attitude, and provision of unnecessary services. Fewer female patients, patients with an FPMI between 3,001 and 5,000 CNY, and inpatients were found in the lowest satisfaction group. Fewer patients with an associate’s or bachelor’s degree, and top earners with an FPMI >7,000 CNY, were detected in highest satisfaction group. Those aged 46–65 years were mainly detected in the highest satisfaction group. The findings from this study suggested that managers of the medical facilities should note the importance of increasing their publicity through a rapidly developing media, as well as the necessity of creating a more patient-friendly medical care experience. Hospitals should also focus on the medical care experience of patients with relatively lower and higher income levels, male ecdemic patients, and ecdemic outpatients. The information desk in the hospital should be fully utilized such that the service for patients is proactive rather than passive. The information desk should provide navigation for patients to receive examinations or treatments and guide them through any complicated procedures. Hospitals and the physicians should actively and truly practice patient-centered care to improve the patients’ clinical outcomes, quality of the doctor–patient relationship, and patient satisfaction.
Author contributions
All authors have approved the content of the submitted manuscript. Dr Xiaojun Liu and Prof Zongfu Mao conceived and designed the study; Dr Xiaojun Liu and research team partners from other units collected data; Dr Xiaojun Liu, Hanson Lu, Yanan Wang, Wenjie Wang, Anran Tan, and Zhaoxun Hou contributed to data analysis and wrote the manuscript; Prof Zongfu Mao, Dr Xiaojun Liu, and Hanson Lu revised the manuscript.
Acknowledgments
This study was supported by an internal grant from Wuhan University and the Postgraduate Innovation Project (No YC2015-S039). We wish to thank Dr Mingyang Wu from Tongji Medical College, Huazhong University of Science and Technology, and Prof Dr Zhaokang Yuan, Fei Xie, Xiaoqing Jiang, and other graduate students from the Medical School of Nanchang University for their specific contributions in data collection. We also gratefully acknowledge the assistance and cooperation from the related hospitals and the research participants who contributed their time and effort for this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- AnandSFanVYZhangJChina’s human resources for health: quantity, quality, and distributionLancet200837296511774178118930528
- HouJLWangZFLuoYHMengQYHealth professional educational system in China from 1998 to 2012: a time-series analysisLancet2015386OctS51
- ZhangXZhaoLCuiZWangYStudy on equity and efficiency of health resources and services based on key indicators in ChinaPLoS One20151012e014480926679187
- ChenJInternal migration and health: re-examining the healthy migrant phenomenon in ChinaSoc Sci Med20117281294130121435765
- ZhangXZhouXHuangXThe analysis of the disease spectrum in ChinaBiomed Res Int2014201460186924967381
- LamCLKWhat are the important health concepts for the Chinese?Qual Life Res199877620
- FangPDongSXiaoJLiuCFengXWangYRegional inequality in health and its determinants: evidence from ChinaHealth Policy2010941142519735959
- Powell-JacksonTYipWCHanWRealigning demand and supply side incentives to improve primary health care seeking in rural ChinaHealth Econ201524675577224807650
- National Health and Family Planning Commission of People’s Republic of China Available from: http://www.nhfpc.gov.cn/zhuz/xwfb/201711/6a9007b7754a477a8109fd572853b02a.shtmlAccessed February 28, 2018
- National Bureau of Statistics of China Available from: http://www.stats.gov.cn/tjsj/zxfb/201702/t20170228_1467424.htmlAccessed February 28, 2018
- National Health and Family Planning Commission of People’s Republic of China Available from: http://www.nhfpc.gov.cn/zhuz/mtbd/201709/6c8a18d7990b4adcaf05d7c38707e2b7.shtmlAccessed February 28, 2018
- National Health and Family Planning Commission of People’s Republic of China Available from: http://www.nhfpc.gov.cn/jws/xnhzcwj/201708/170add2740ad473b81d45c8af79ca629.shtmlAccessed February 28, 2018
- National Health and Family Planning Commission of People’s Republic of China Available from: http://www.nhfpc.gov.cn/tigs/s9660/201412/09c02e4b429d405fadf798d94c7caa66.shtmlAccessed February 28, 2018
- National Health and Family Planning Commission of People’s Republic of China Available from: http://www.nhfpc.gov.cn/jws/xnhydjy/xnhydjy.shtmlAccessed February 28, 2018
- SitziaJWoodNPatient satisfaction: a review of issues and conceptsSoc Sci Med19974512182918439447632
- LyuHWickECHousmanMFreischlagJAMakaryMAPatient satisfaction as a possible indicator of quality surgical careJAMA Surg2013148436236723715968
- KatoKO’MalleyKJRelationships between the eligibility process, trust in the U.S. health care system, and patient satisfaction with the Houston Veterans Affairs Medical CenterMil Med2007172881817803072
- GothUSHammerHLClaussenBUtilization of Norway’s emergency wards: the second 5 years after the introduction of the patient list systemInt J Environ Res Public Health2014113375338624662997
- BjertnaesOASjetneISIversenHHOverall patient satisfaction with hospitals: effects of patient-reported experiences and fulfilment of expectationsBMJ Qual Saf20122113946
- TsaiTCOravEJJhaAKPatient satisfaction and quality of surgical care in US hospitalsAnn Surg201526112824887985
- KleefstraSMKoolRBZandbeltLCHaesJDAn instrument assessing patient satisfaction with day care in hospitalsBMC Health Serv Res201212112522624677
- LiMHuangCLuXChenSZhaoPLuHEvaluation of medical staff and patient satisfaction of Chinese hospitals and measures for improvementBiosci Trends20159318218926166371
- CanoSJHobartJCThe problem with health measurementPatient Prefer Adherence2011527929021792300
- JinTA transformative tale of patients and doctors in ChinaLancet201137797721144
- WangGXieJHuYDoctor-outpatient communications in Chinese public hospitals: a cross-sectional surveyLancet2016388S38
- PanJLiuDAliSPatient dissatisfaction in China: what mattersSoc Sci Med201514314515326356826
- LeeYYLinJLDo patient autonomy preferences matter? Linking patient-centered care to patient-physician relationships and health outcomesSoc Sci Med201071101811181820933316
- XieBWangMFeldmanRZhouLInternet use frequency and patient-centered care: measuring patient preferences for participation using the health information wants questionnaireJ Med Internet Res2013157e13223816979
- LiDRImprovement and evaluation of patient satisfaction scale in general hospitalSouthern Medical UniversityGuangzhou, China2007 Available from: http://kns.cnki.net/KCMS/detail/detail.aspx?dbcode=CMFD&dbname=CMFD2008&filename=2007223146.nh&uid=WEEvREcwSlJHSldRa1FhdkJkVWI3Nkp6bjhkeTlrVzlnd1lrSUpSRDIrST0=$9A4hF_YAuvQ5obgVAqNKPCYcEjKensW4ggI8Fm4gTkoU-KaID8j8gFw!!&v=MDcyNzViUElSOGVYMUx1eFlTN0RoMVQzcVRyV00xRnJDVVJMS2ZZT2RvRnlybVU3L01WMTI3R2JHNkh-kRElxWkU=Accessed July 19, 2018 Chinese
- LegidoquigleyHGlinosIBaetenRMckeeMPatient mobility in the European UnionBMJ2007334758618819017255612
- AndritsosDATangCSIntroducing competition in healthcare services: the role of private care and increased patient mobilityEur J Oper Res20142343898909
- BrekkeKRLevaggiRSicilianiLStraumeORPatient mobility and health care quality when regions and patients differ in incomeJ Health Econ20165037238727344297
- SunZQXuYYMedical Statistics3rd edBeijing, ChinaThe People’s Medical Publishing House2010508509
- CuadrasCMCuadrasDLahlouYPrincipal directions of the general Pareto distribution with applicationsJ Stat Plan Infer2006136825722583
- LyDPGliedSAVariations in the service quality of medical practicesAm J Manage Care20131911378385
- TukeyMHWienerRSThe impact of a medical procedure service on patient safety, procedure quality and resident training opportunitiesJ Gen Intern Med201429348549024272831
- LiuYSkupMLinJChaoJImpact of non-medical switching on healthcare costs: a claims database analysisValue Health2015183A252
- WengHHungCLiuYAssociations between emotional intelligence and doctor burnout, job satisfaction and patient satisfactionMed Educ201145883584221752080
- MiaoYLiLBianYGender differences in job quality and job satisfaction among doctors in rural western ChinaBMC Health Serv Res201717184829282049
- FuJSunWWangYYangXWangLImproving job satisfaction of Chinese doctors: the positive effects of perceived organizational support and psychological capitalPublic Health20131271094695124094359
- YuWLiMChenXDeterminants and influencing mechanism of outpatient satisfaction: a survey on tertiary hospitals in the People’s Republic of ChinaPatient Prefer Adherence201610160161227143865
- ChenHLiMWangJFactors influencing inpatients’ satisfaction with hospitalization service in public hospitals in Shanghai, People’s Republic of ChinaPatient Prefer Adherence201610146947727110101
- PaulSHerrmannFRHallerDMIs patient satisfaction with organizational aspects of their general practitioner’s practice associated with patient and doctor gender? An observational studyBMC Fam Pract201617112027729018