Abstract
Background:
As important users of health care, adolescents with chronic conditions deserve to be consulted about their experiences and expectations. This study aimed to explore chronically ill adolescents’ preferences regarding providers’ qualities, and outpatient and inpatient care. Furthermore, suggestions for improvement of service delivery were collected.
Methods:
This research was a sequential mixed methods study in adolescents aged 12–19 years with various chronic conditions treated in a university children’s hospital. Methods comprised 31 face-to-face interviews at home, a hospital-based peer research project in which nine adolescents interviewed 34 fellow patients, and a web-based questionnaire (n = 990). Emerging qualitative themes were transformed into questionnaire items.
Results:
Having “a feeling of trust” and “voice and choice” in the hospital were central to these adolescents. Regarding providers’ qualities, “being an expert” and “being trustworthy and honest” were ranked highest, followed by “being caring and understanding”, “listening and showing respect”, and “being focused on me”. Regarding outpatient consultations, preferences were ranked as follows: “answering all questions”; “attending to my and my parents’ needs”; and “clear communication”, while “limited waiting times” and “attractive outpatient surroundings” scored lowest. Regarding hospitalization, adolescents most preferred to “avoid pain and discomfort”, “keep in touch with home”, and “be entertained”, while “being hospitalized with peers” and “being heard” were least important. Regarding priorities for improvement, 52% of the respondents felt that more attention should be paid to older children, followed by enabling more contact with family and friends (45%), shorter waiting times (43%), and more activities to meet fellow patients (35%).
Conclusion:
Adolescents prefer technically competent providers, who are honest and trustworthy, and attend to their needs. As they gradually grow out of the pediatric environment, they desire staff attitudes to become less childish and more age-appropriate, and welcome being treated as an equal partner in care. Health care professionals should inquire into preferences and adjust their communication style accordingly.
Introduction
Children with chronic conditions are frequent users of health care services, yet they are rarely included in the evaluation of such services.Citation1,Citation2 Satisfaction with pediatric care is usually only measured in parents,Citation3–Citation7 whereas children act as silent users of these facilities.Citation8 However, having parents evaluate children’s care may not accurately represent children’s views.Citation9–Citation11 For example, Farrant and Watson found adolescents to be more critical about the received care than their parents, even though they identified the same qualities for good health care providers.Citation9
Direct input from children and adolescents on their health care experiences, preferences, and priorities is helpful for service evaluation and a prerequisite for improving patient-centeredness of pediatric health care.Citation12 This is especially relevant for young patients with chronic conditions, who may offer a valuable source of data with which to improve the overall effectiveness of the health care delivery system for adolescents.Citation12 Making services more responsive to their needs may have a positive effect on their adherence with treatment and appointments.Citation13
Reasons for not involving children in the evaluation of services may be related to the idea that they are not interested in this or are incompetent.Citation14 Both assumptions have been contested in studies that have included children as young as 4–6 years.Citation15–Citation17 Children like to be seen as partners in medical care and in the planning, development, and evaluation of services.Citation18,Citation19 The older they get, the more capable they are of providing rich and detailed descriptions of their preferences.Citation15
The first studies of children’s preferences for care focused on the factors affecting healthy adolescents’ decision to seek preventive care.Citation20–Citation22 Provider characteristics proved more important than site or system characteristics,Citation20 and issues of hygieneCitation21 and confidentialityCitation22 were of crucial importance. Chronically ill adolescents, on the other hand, may have different needs and experiences, because they have more frequent and often critical health care interactions. Also, these children and their families build long-lasting relationships with (the same) providers, which may affect their evaluation of care.Citation7
Several studies (mostly in the US, UK, and Canada) have explored experiences and preferences of adolescents with chronic conditions in three major domains, ie, communication with health professionals,Citation9,Citation12,Citation23–Citation26 outpatient facilities,Citation10,Citation11,Citation27 and inpatient services.Citation2,Citation15,Citation28–Citation30 Some studies focused on themes related to privacyCitation31 or adolescents’ decision-making preferences.Citation32 The various studies applied either qualitativeCitation2,Citation15,Citation23–Citation26,Citation31,Citation33 or quantitativeCitation9,Citation10,Citation12,Citation30 methodologies. In the Netherlands, an estimated 14% of all children under 18 years have a chronic condition.Citation34 So far, only one study has explored their perspectives on hospital care.Citation35
The aim of this paper was to explore the preferences of chronically ill Dutch adolescents (12–19 years of age) for health care professionals and outpatient and inpatient service delivery. We also aimed to collect their suggestions for improvement of adolescent health care.
Materials and methods
Study design
In a project entitled “On Your Own Feet” (2004–2008) we mapped preferences for hospital care and competencies required for self-management in adolescents with chronic conditions. These adolescents were treated in one Dutch university children’s hospital. The research team consisted of social scientists, nurse researchers, and a doctor. Here, we report on three substudies exploring their preferences for health care. Data about competencies and readiness for transfer were published elsewhere.Citation36,Citation37
We chose a mixed methods design to account for the complexity of a multiparty context. Mixed methods research is defined as a single study in which qualitative data collection and/or analysis is combined with quantitative data collection and/or analysis.Citation38 Reasons for applying a mixed methods design were, first, comprehensiveness, ie, using different methods to address different aspects of the overall research question to provide a more complete insight. Second, better validity and generalizability; by combining qualitative and quantitative methods, inherent weaknesses of each methodology could be compensated for.Citation38,Citation39 Third, because we wished to give adolescents a voice, patient-centeredness was another justification for including qualitative and participatory research.Citation39 Therefore, in one of the substudies we experimented with a participatory approach, inviting young people with chronic conditions to participate as coresearchers.Citation40
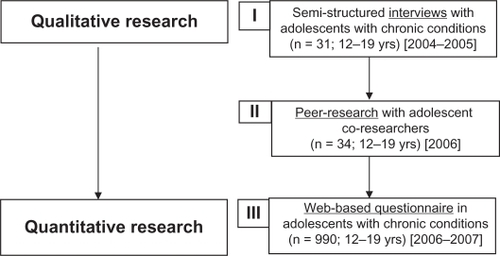
Although mixed methods research has become popular in health research, integration of different strands of research is a methodological challenge because there are no clear procedures for this.Citation41 To enhance the transparency and quality, we followed the guidelines of O’Cathain et al, for good reporting of mixed methods studies.Citation42 We employed a sequential strategy of inquiry,Citation36 which implies that the studies were conducted in three consecutive steps, as presented in . The qualitative studies preceded and guided the development of the quantitative survey. Design, execution, and analysis of each step is presented below.
Figure 1 Overview of mixed methods research on preferences for care from “On Your Own Feet”.
Participants and setting
All studies were performed at the Erasmus MC University Medical Center in Sophia Children’s Hospital, Rotterdam, the largest tertiary referral center in the Netherlands. This hospital treats over 3500 adolescents with chronic conditions, but has no specialized adolescent inpatient facilities and offered, at the time of the study, only a handful of outpatient youth clinics. We enrolled 12–19-year-old patients with chronic somatic conditions who had had at least one consultation in the past six months and had been under continuous treatment for the past three years. Adolescents with intellectual disabilities and those already transferred to adult care were excluded.
Qualitative research
Interviews
Two age groups were created, ie, younger adolescents aged 12–15 years and older adolescents aged 16–19 years. Equal numbers of random cases in both groups were drawn from the hospital database to facilitate purposive sampling.Citation38 Next, we aimed at sampling equal numbers of participants, even distributions of gender, hospital experience, and nature of the condition (ie, congenital or recently acquired, physically disabling or not) within both age groups. Our intent was to interview at least 15 adolescents in each age group.
Pairs of purpose-trained nursing and paramedical students or a researcher (SJ) conducted the interviews in the participants’ homes. The semistructured interviews collected background information about their condition, their understanding of their condition, its impact on their day-to-day lives, and assessed their preferences for service delivery. This included asking about their experiences with hospital staff, the attributes of a good doctor, what they liked and disliked about hospital consultations, and their experiences with hospital admissions. Interviews lasted between 45–90 minutes, were audiotaped and transcribed verbatim. The data were analyzed in combination with those from the peer research.
Peer research
For the participatory research project, adolescents were sought who were both motivated to act as coresearchers and willing to give their opinion about the care they received. Because a hospital is not an ideal setting for community-based research, we organized a disco party in a real discotheque during which the coresearchers were to interview their fellow patients. A representative sample of adolescents was not intended. More information on the design and execution of the peer research study is provided elsewhere.Citation40
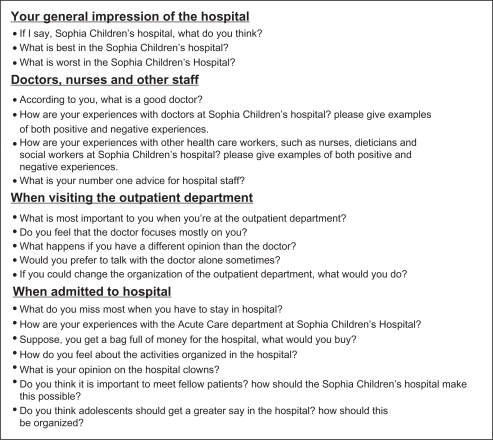
The nine coresearchers (all over 15 years of age) were recruited by nurse specialists in the hospital. They were briefly trained in interview techniques, and we discussed the themes and topics to be included in the interview protocol with them. The research team presented some open-ended questions inspired by the previous interview study and by a child-friendly questionnaire designed and tested in another Dutch pediatric hospital.Citation35 The coresearchers rephrased the questions where needed and added new topics. The interview protocol was finalized in several discussion rounds with the coresearchers via email. The questions related to adolescents’ care experiences and preferences are shown in .Citation40 Data on sociodemographic characteristics were also collected.
Figure 2 Questions related to preferences in the interview protocol for the peer research interviews.Citation40
Copyright © 2010, John Wiley and Sons. Reproduced with permission from van Staa et al.Citation40
Although we intended to involve the coresearchers in the data analysis, setting up a “real-life” meeting proved impossible. Instead, the research team analyzed the anonymous transcripts and invited coresearchers to comment on draft versions of the report via email.
Combined qualitative analysis
Because the topics discussed during the interviews and the peer research project were very similar, all qualitative data were analyzed together, using the qualitative software package ATLAS.ti 5.5. Thematic analysis was chosen for its flexibility and theoretical freedom, and was applied in several phases.Citation43 As a first step, AvS and SJ read the interviews repeatedly to familiarize themselves with the data. They independently formulated initial codes (subthemes). Together, the researchers examined codes and reached consensus on the initial codes. Subsequently, these were modified, expanded, or merged as new issues emerged. The third step was collating subthemes to identify potential themes; emerging themes were checked iteratively in other interviews. Possible relationships between patients’ preferences and relevant demographic characteristics were identified. The research team examined the coding process, and the emerging themes were discussed continually until consensus was reached.
Quantitative research
Questionnaire
All adolescents who met our aforementioned inclusion criteria on July 1, 2006 (n = 3648) were invited by letter to complete an online questionnaire accessible with a unique code on a secured Internet site. Response postcards were included in the invitation letter to encourage adolescents to state reasons for refusal. All received a written reminder after three weeks.
The questionnaire measured sociodemographic characteristics, disease-related and health care-related variables, competencies, and preferences for care. Data on gender, age, ethnicity, and hospital visits (outpatient departments, admissions) were retrieved from the electronic hospital database, and all other data were self-reported. The questionnaire had been pilot-tested in face-to-face interviews with five chronically ill adolescents and four parents. Information on the measures has been published elsewhere.Citation37
Because there were no short and reliable measures available to assess preferences for health care providers, outpatient consultations, and inpatient care, we transformed the final themes of the qualitative studies into questionnaire items. Adolescents were asked to indicate what they considered to be the most important quality for a good doctor or nurse, and what is most important to them when coming to an outpatient appointment, and during hospitalization. Respondents were invited to rank-order five statements related to each topic from 1 to 5 (number 1 being the most important quality or issue and number 5 the least important).
Furthermore, respondents were asked to mark three out of nine items as priorities for improvement in the Sophia Children’s Hospital. This list was adapted from a seven-item “improvement indicator” that had been constructed after consultation with 225 children aged 7–16 years in another Dutch children’s hospital.Citation35 Because half of their population was below 12 years of age, we added two items that had proved relevant in the peer research project, ie, “I wish they would pay more attention to the needs of older children” and “I wish I could do more things with fellow patients”.
Quantitative analysis
Questionnaire data were analyzed using SPSS 17.0 (SPSS Inc, Chicago, IL). Descriptive statistics were applied. Ratings for preferences for providers, outpatient visits, and hospital admissions were recoded (the most important preference receiving 5 points and the lowest 1 point) and then summated. Analysis of variance was used to test differences between the means on preference scores and priority listing between boys and girls, between older and younger adolescents, between higher and lower educated adolescents, those who visited the hospital more than four times a year versus those who came less frequently, and those who had, or had not been hospitalized in the past three years.
Validation and integration
Validation of the findings was primarily realized by method triangulation and peer review. For example, preliminary analyses of interviews and peer research were discussed within the research group, with the coresearchers, and with health care providers (data reported elsewhere).Citation36 Integration of the findings of the different study parts occurred at two stages. First, to establish the additional value of the participatory approach, results from the peer interviews were compared with those from the home interviews.Citation40 All qualitative findings were thematically summarized in a popular book.Citation44 The qualitative findings also provided direct input for questionnaire development by transforming qualitative themes into questionnaire items. Second, for the present paper interpretations from the qualitative studies were systematically compared with the quantitative findings.
Ethics
All study procedures were approved by the institutional review board at the Erasmus MC University Medical Center. The researchers had no access to participants’ medical records. Participants were assured of confidentiality and data were processed anonymously. Eligible adolescents and their parents received written information about the study and gave informed consent. The interviewees were rewarded with a €20 gift voucher. The coresearchers involved in the peer research received €75 remuneration for their input, while participants attended the disco party for free. Adolescents who completed the questionnaire were entered into a lottery for 2 iPods and a cell phone.
Results
Response
Characteristics and medical diagnoses of the participants in the substudies are presented in .
Table 1 Adolescents’ socio-demographic and disease-related characteristics in preference studies in the research project ‘On Your Own Feet’
Interviews
Thirty-one of the 66 invited adolescents (47%) consented to an interview. Data on responders and nonresponders have been published elsewhere, revealing no significant differences in the selected variables for purposive sampling.Citation45 Five adolescents presented with surgical conditions, two were chronically disabled, and the others had a variety of chronic illnesses.
Peer research
Twenty-five adolescents, predominantly younger girls (12–15 years), attended the disco party. The nine coresearchers also interviewed each other, adding up to a total of 34 peer interviews. Compared with the visitors, the coresearchers were older (P < 0.05) and visited the hospital more frequently (P < 0.01).
Questionnaire
The study population for the questionnaire consisted of 3648 adolescents. Of the 1087 questionnaires received (response rate 29.8%), 97 were excluded because they were incomplete, leaving a total of 990 valid questionnaires. An analysis of response and nonresponse has been published elsewhere.Citation37 Nonresponders tended to be males with non-Dutch surnames; in addition, they were older and had fewer consultations than responders (P < 0.05). presents participants’ characteristics. All major chronic conditions were represented, and the majority suffered from life-long chronic conditions.
Adolescents’ preferences
Below, we first present the qualitative themes (summarized in ) in each domain of care-related preferences, followed by the results from the questionnaire items developed from them.
Table 2 Qualitative themes and sub themes related to preferences for health care providers, outpatient consultations and hospital care, and overall quality
Preferences for interactions with providers
Qualitative results
Adolescents regarded health care professionals as the most valuable asset in the hospital. Five themes emerged, ie, being trustworthy and honest, being caring and understanding, listening and showing respect, focusing on me, and being competent. One of the coresearchers summarized these attributes as follows: “A good doctor is someone who is child-friendly. Someone who consults with you and with your parents; who doesn’t treat you like a toddler. He doesn’t need to tell you that you’re ill, that’s obvious. Furthermore, he or she should be able to listen well and to solve your problems” (16-year-old girl).
The adolescents wanted a doctor who is trustworthy, ie, one whom they trust and who trusts them. This is why they preferred continuity in providers: “There is some sort of trust that you feel with this doctor and not with someone else” (16-year-old boy). It is also a matter of convenience: “Having to explain everything every time is rather irritating” (13-year-old girl). However, it is predominantly related to confidentiality: “My own doctor knows all about me and that is confidential information” (16-year-old girl). A 17-year-old boy saw his familiar providers as “... more than just interested, you have the feeling you can tell them everything, they are not just passers-by, but confidantes”. It is vital that health care providers keep this information confidential. It also takes time to build a trusted relationship, and it requires “getting to know each other”. The concept of trust seems closely intertwined with that of provider honesty. Therefore, we combined “trust and honesty” in one theme. Many adolescents claimed to prefer honesty even when it implies being given unpleasant information. A 19-year-old boy thought: “They should tell you what’s going on and tell you straight in the face what the consequences of your behavior are, because that’s in your best interests.” Mainly older adolescents did not fear confrontations: “It startles me when they confront me. That helps me to correct my behavior; I guess I need that once in a while” (18-year-old girl). Although not all adolescents wanted to be confronted directly with the consequences of sloppy adherence, they all felt that doctors should tell honestly “what’s up and what they’re going to do” (14-year-old girl). Withholding information or being overprotective was considered to be “childish”.
A caring and understanding attitude was also much appreciated. Doctors and nurses should be “kind, patient, and understanding” (14-year-old boy). They should not treat adolescents “... like a number” (15-year-old boy). Questions about their social life were appreciated: “I like it when doctors and nurses take interest in the things I do in my free time” (17-year-old girl). Some liked jokes or small talk from doctors. This could even be useful, suggested a 16-year-old boy: “Children should be made to feel at ease, so they don’t withhold information”. But others wanted a doctor to be “serious, taking his time” (12-year-old girl). A 15-year-old girl recommended that health care staff should “try to think from the patient’s perspective – how would you like to be treated? Ask them if they can cope!”
Adolescents wanted doctors to listen to them and consider their opinion. “If I don’t like something, they should respect that” (17-year-old girl). Not considering their opinion was experienced as a breach of confidence: “Just one time the doctor did not take my opinion into account and then I got very upset” (12-year-old girl). In contrast, being given a choice in treatment options is appreciated: “My doctor usually says that she only gives advice but that I have to decide for myself. That’s fine.” (12-year-old girl).
Adolescents preferred health care professionals to focus on them rather than on their parents. Some complained that their parents were asked for information, rather than them themselves. A 16-year-old girl wished “... they would talk more to the children and ask their permission if they want to change treatment. For example, they could ask children whether they would like to talk to the doctor alone. That would give you the opportunity to share things you would otherwise never tell.” Doctors “should really talk to me and co-decide with me” thought a 16-year-old girl. Being focused on the adolescent patient was often related to a preference for being treated like an adult: “They should treat teenagers in a less childish way, according to their age” (15-year-old girl). A 12-year-old girl complained: “The doctor always says: “so, you have grown a lot” – that is so childish! They never talk to me in an adult way, like my parents talk to me. I don’t like that. I wish they wouldn’t treat me like a small child”. Only a minority of the adolescents, especially those who labeled themselves as “... still being a child” (12-year-old boy), did not prefer an adult approach, for example because “... it would be too difficult for me” (15-year-old girl). But a 14-year-old girl said that, even though she could not handle everything the way grownups do, she still wanted to be treated in an adult way.
Competence and professional expertise were valued highly. This was defined in terms of knowledge, attitude, and practical skills: “A good doctor is someone who knows exactly what he’s doing and also takes into account that children find jabs very scary” (12-year-old girl). It is “someone who helps you and always tries to make you better and doesn’t give up” (14-year-old girl). Professionals should have the skill to explain matters in a way children can understand: “A doctor should be able to explain everything very well, what it means and what you can expect” (16-year-old girl).
Quantitative results
The five themes were transformed into items. presents the mean scores, standard deviations, and priority listing (number of times this item was selected as being most important) of the questions on preferences for provider qualities. The most important attribution for a good doctor or nurse was being an expert and knowing what (s)he is doing, while issues related to honesty and trustworthiness came in second place. Significant differences were found between the genders and age groups. Boys attached more importance to providers’ expertise (F[1, 986] = 5.48; P = 0.02) and trustworthiness and honesty (F[1, 986] = 7.24; P < 0.01) than did girls; girls rated the importance of careful listening (F[1, 986] = 5.53; P = 0.02) and being kind (F[1, 986] = 9.06; P < 0.01) higher than did boys. Younger adolescents found providers’ kindness and ability to reassure them more important than did older adolescents (F[1, 986] = 13.36; P < 0.001). The latter found it more important that health care providers are focused on them and consider their opinion (F[1, 986] = 8.54; P < 0.01).
Table 3 Top 5: most important qualities of health care providers and most important issues related to hospital consultations and inpatient care (n = 988)
Preferences for outpatient consultations
Qualitative results
Five themes relating to effective and efficient consultations emerged from the thematic analysis, ie, answering all my questions, attending to my and my parents’ needs, clear and concise communication, short waiting times, and attractive outpatient surroundings.
Adolescents wanted consultations to be meaningful and helpful, ensuring that all their questions were being answered: “The doctor must listen to what is being said. He should answer all your questions without using difficult words” (15-year-old boy). Doctors should “talk steadily, not too fast” (12-year-old girl). Some adolescents found consultations “... boring, always the same”. Perhaps this is because they feel left out of the conversation: “With all these difficult words, I don’t understand what’s going on and that is boring” (12-year-old boy).
Both their own and their parents’ needs should be attended to: “They should explain things to me and to my parents as well. So that they too understand” (17-year-old girl). Their parents’ presence is important for many adolescents, especially the younger ones: “It is convenient that my parents are there because I do not always understand everything” (14-year-old boy). Still, many feel it would be a good idea to see the doctor alone sometimes: “Certain things I can’t discuss with my parents” (16-year-old boy). In any case: “Doctors should not only address my parents, but me in the first place” (15-year-old girl).
Adolescents preferred clear and concise communication: “They should come to the point straight away and not tell you nice stories” (17-year-old girl). A 16-year-old boy was irritated by his doctor beating around the bush: “If you ask my doctor a question, he spins a tale around it, but doesn’t give an answer!” Another 15-year-old boy was most concerned with the consultation “... going quick and smooth, without long silences”. Clear communication also implied avoiding jargon or difficult words.
Short waiting times for outpatient consultations were also thought to be important. Many complained: “I wished I wouldn’t have to wait so long!” (16-year-old boy). Inefficient planning also bothered them: “Consultations should be planned in one day, after each other” (17-year-old girl).
Attractive outpatient surroundings also mattered: “It should be cozy and pleasant” (18-year-old girl). The waiting room should offer distraction and be an age-appropriate environment that is not too noisy: “It should be quiet in the waiting area, so you won’t get stressed out and can concentrate yourself ” (16-year-old girl). Unfortunately, this was not always the case because adolescents complained about “... screaming young kids scooting about on tricycles”.
Quantitative results
presents the priority listing of preferences for outpatient visits. All questions being attended to and appointments starting on time were ranked as most important. Least importance was given to the waiting room environment. Only educational level accounted for differences in priorities: the more highly educated adolescents found it more important that their questions were being answered (F[1, 939] = 9.47; P < 0.01), whereas the less educated ones attached more importance to distraction in the waiting room area (F[1, 939] = 5.13; P = 0.02).
Preferences for hospital admissions
Qualitative results
Not all adolescents interviewed had been hospitalized. Five themes associated with inpatient care emerged, ie, avoiding pain and discomfort, keeping in touch with home, being entertained, being hospitalized with peers, and being heard.
Avoiding pain and discomfort is important because hospital admission is associated with pain and unpleasant invasive procedures. Other associations included being locked up, being bored, and being alone. Adolescents missed their family, friends, and pets.
Therefore, keeping in touch with family and friends during hospitalization was important to them and availability of a laptop with an Internet connection was highly appreciated for that reason.
Being entertained and being offered distraction (game computers and recreational activities) was also mentioned regularly: “You should be entertained so you won’t think of your illness all the time” (18-year-old girl). These activities were not always age-appropriate. “I would like more activities for older children – they are a little boring now, more for small kids” (12-year-old girl). Also: “the hospital clowns are nice for younger kids, but they should ask you if you want to be entertained by them. When you get older, you really do not have a need for that sort of entertainment anymore” (17-year-old girl). While younger adolescents thought the clowns were “... very funny, they cheered everything up” (12-year-old girl), a 16-year-old girl thought they were “stupid and boring. I am too old for that kind of humor, but it’s good that they are there for the kids”.
Those with extensive hospital experience complained about being with younger children on the ward and favored being hospitalized with peers. Meeting fellow patients through activities offered by the hospital was important to about half of the attendants of the disco party, whereas the adolescents interviewed at home seemed less interested in meeting fellow patients. A 16-year-old-girl at the disco party said: “That’s very important. You can support each other in difficult times, exchange advice and hear stories about how others experience things”. Suggested ways to meet fellow patients were chat rooms, group sessions, and activities outside the hospital. Not all adolescents were interested in such activities: “I don’t feel like there’s something wrong with me, so I prefer to hang out with people who have nothing wrong with them” (15-year-old-girl), and a 15-year-old boy thought he would “go crazy” if he would have to talk about hemophilia “all the time”.
Being heard and being empowered to participate in decisions formed the last theme. Some adolescents wanted more involvement in treatment decisions: “I wish they would ask me more often to say what I really want. If only you should get the opportunity” (14-year-old boy). On the other hand, not all participants felt the need to have a greater say in hospital matters because “they already listen to you and I do not have any bad experiences”. However, some did, especially the coresearchers: “It’s a children’s hospital, so it should be child-friendly. Who can better judge whether it’s a good or bad hospital than children themselves?” (15-year-old girl). She suggested that a youth council be formed that could advise the hospital board how to improve services further.
Quantitative results
It was most important to adolescents that they suffer the least possible pain and discomfort when being hospitalized (). Keeping contact with family and friends was also highly valued, and being hospitalized with peers was least important. However, girls found the latter more important than did boys (F[1, 986] = 4.91; P < 0.03), whereas boys rated distraction as more important than did girls (F[1, 986] = 36.88; P < 0.001). Keeping in touch with family and friends was more important for younger adolescents (12–15 years) than it was for the older ones (F[1, 986] = 4.99; P ≤ 0.03). The latter rated the importance of staff listening higher than the younger group (F[1, 986] = 18.07; P < 0.001).
Those admitted to the hospital in the past three years attached more importance to experiencing the least possible pain and discomfort (F[1, 986] = 6.41; P = 0.01) and staff listening to them than did those who had no inpatient experience (F[1, 986] = 4.16; P < 0.05). The latter rated maintaining contact with family and friends as more important than did the ones with inpatient experience (F[1, 986] = 7.75; P < 0.01).
Quality of care and priorities for change
Qualitative results
The adolescents were very positive about the quality of care provided in the children’s hospital. They pointed at the warm atmosphere, the caring attitude of the staff, and the child-friendly facilities: “It is really a place for children. They help you and it’s very beautiful there” (13-year-old girl). “They are really focused on children. They do their best to make your visit as pleasant as possible. I love the colors in the central hall. The hospital gives me a feeling of trust” (15-year-old girl). “The nurses are really nice. They have good computers there” (12-year-old-girl). “There are qualified doctors who listen to me” (17-year-old-girl).
Having a feeling of trust was a central theme in the interviews and peer research. The fact is that many have come here often from a very young age: “The doctors are very nice, the building is nice and I’ve been coming here all my life, so it is all familiar” (17-year-old girl). To the question what should be improved, quite a few adolescents responded “Nothing, everything is OK”. However, others identified several areas for improvement, ie, lack of involvement in treatment decisions, staff attitude toward teenagers, and the lack of adolescent-focused services and facilities. Therefore, the other central theme related to the quality of adolescent care was having voice and choice.
Quantitative results
displays adolescents’ priorities for improvement based on the “improvement indicator”. The item selected most often (by 52.2% of all adolescents) was paying more attention to the needs of older children. Having more contact with family and friends through the Internet (44.6%), shorter waiting times (43.3%), and more activities with fellow patients (34.5%) came next. Only 14.6% of all adolescents wished that doctors and nurses would listen to them more often.
Figure 3 Priorities for improvement in the children’s hospital: Percentage of adolescents that selected this item in the survey (n = 990).
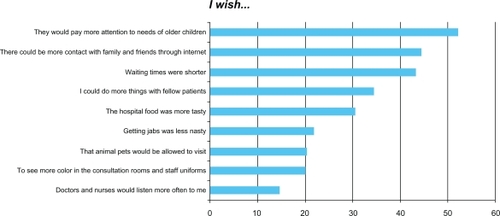
Here, we also tested for differences between those who did and did not select an item as priority for improvement. Girls more often than boys mentioned that more attention should be paid to older children (F[1, 988] = 10.97; P = 0.001) and that there should be more color in the hospital (F[1, 988] = 10.37; P = 0.001). Boys more often than girls mention that the hospital food should be tastier (F[1, 988] = 4.54; P = 0.03) and that waiting times should be shorter (F[1, 988] = 5.78; P = 0.02). More of the younger ones wished that pets would be allowed to visit in the hospital (F[1, 988] = 8.17; P < 0.01); that more contact with family and friends through the Internet would be possible (F[1, 988] = 6.11; P < 0.01), and that getting jabs would be less unpleasant (F[1, 988] = 14.58; P < 0.001). The older ones were more concerned about the hospital paying greater attention to older children (F[1, 988] = 20.45; P < 0.001). For those with lower education, having more activities with fellow patients (F[1, 940] = 9.98; P < 0.01) and having more contact with family and friends while in hospital (F[1, 940] = 3.95; P < 0.05) were higher priorities than for those with higher education. In reverse, the more highly educated adolescents were more concerned about shorter waiting times in the hospital (F[1, 940] = 7.25; P < 0.01). Finally, those who have been hospitalized in the past three years were more keen on having tastier hospital food (F[1, 988] = 8.88; P < 0.01], while shorter waiting times were more important to those without inpatient experience (F[1, 988] = 6.82; P < 0.01).
Discussion
This mixed methods study explored chronically ill adolescents’ preferences for health care providers’ attributes and for service delivery in outpatient clinics and during hospitalization in a children’s hospital. Their suggestions for improved delivery of care were also collected. The adolescents were generally very satisfied with the care provided and felt at home in the children’s hospital, but they recommended paying more attention to the needs of older children and improving the age-appropriateness of providers’ attitudes and services. Technical competence and good communication skills and attitudes were regarded as important qualities of health care providers. The adolescents were concerned about having their questions and needs attended to in outpatient consultations as well as being seen on time. Having as little pain and discomfort as possible, as well as maintaining contact with family and friends, were considered most important during hospitalization. Environmental aspects were rated as less important.
Preferences
The themes we uncovered and those from other qualitative studies exploring adolescents’ preferences for (communication with) providers share many similarities (). Honesty, respect, a caring and friendly attitude, being focused on adolescents, and technical competence are all important.Citation9,Citation23,Citation26,Citation33,Citation46 Trustworthiness seems a core attribute for professionals and is related to good communication skills and respect for teenagers’ opinions and privacy.Citation20,Citation25,Citation31 Other studies have confirmed that adolescents favor direct communication with them (and not with their parents) and dislike being patronized or being approached in a condition-centered manner.Citation26,Citation47 In our study, the importance of receiving explanations and information did not emerge as a separate theme. We placed this under the theme “being competent”. Receiving appropriate information during consultations was seen as very important. In contrast with some other studies, our respondents did not mention preferring a provider of the same gender.Citation9,Citation26,Citation46 Some mentioned a preference for continuity in providers in relation to trust, but this did not emerge as a separate theme.Citation26,Citation46
Table 4 Comparison of themes in qualitative studies into adolescents’ preferences for their interactions with health care professionals
The qualitative findings were reinforced by the survey outcomes, both in our study and among chronically ill adolescents in the US, who rated the honesty of their physician, attention to pain, and items related to respect as very important, while technical aspects of care were also highly appreciated.Citation12 Our study adds that professional expertise is most important (41% indicated this as their number 1 concern), and honesty and kindness of the provider came in second and third place, respectively. An important theme in the qualitative studies, ie, providers “being focused on me”, proved to be less important than the other qualities in our survey.
For outpatient facilities, our findings correspond with those of other studies that also indicated the importance of good explanations and having a choice,Citation33 as well as of more efficient services and reduced waiting times.Citation27,Citation47 A study by Wray and Maynard also demonstrated that both streamlined care processes in the outpatient department and care interactions are important to young people with congenital heart conditions who move to adult services.Citation47 Making the outpatient area more teen-oriented and less child-centeredCitation27 was also a wish of our respondents, but they did not give it much priority.
With respect to clinic environment and inpatient care, our qualitative studies confirm the findings of others, ie, the interior design should be less child-centered and more teen-oriented, and feel more like home.Citation15,Citation27,Citation29 Adolescent inpatients would also appreciate more fun and distraction, more comfort, and attention to privacy.Citation15 Although few adolescents in our study complained of unsympathetic hospital staff,Citation30 friendliness was important to them. However, in our survey, they indicated that minimizing pain and discomfort was the most important aspect to them when hospitalized. Although our participants stressed the importance of being consulted and involved in their hospital care, as in the study by Coyne,Citation2 they did not give this a high priority in our survey. Only 15% indicated that they wished doctors and nurses would listen to them more often. Some adolescents, especially those involved in the peer research, would appreciate being hospitalized with peers,Citation30 or be offered activities enabling them to meet fellow patients (35% of survey participants indicated this was an area for improvement). An interesting but unexplained association was found between a lower level of education and a stronger preference for meeting fellow patients. However, our participants did not voice a strong need for a dedicated adolescent unit.Citation48
Differences between adolescents
Not all young people have the same preferences.Citation45 Our study confirmed some differences related to gender, age, inpatient experience, and educational level. Boys attached more importance to professional expertise and the honesty of providers than did girls, who wanted more attention to older children and rated listening as a more important provider quality. We cannot explain these differences, and they have not been reported before. A large survey of adolescent preferences found only one significant association for gender, ie, girls viewed the “power/control” factor as more important than did boys.Citation12 In that survey, higher age was strongly associated with a preference for communication directly with the teen versus the parent,Citation12 a finding confirmed in our survey, in which older adolescents had a stronger preference for staff being focused on them and listening to them than did the younger ones. Younger adolescents in our study were more concerned about staff kindness, pets’ visits, and the discomfort of painful procedures, like the participants in another Dutch hospital.Citation35 For adolescents with inpatient hospital experience, the quality of hospital food and staff listening to them was more important than for those who had not been admitted before, indicating that both a higher age and more hospital experience increases the desire of adolescents to be involved in decision-making.
Mixed methods
Combining qualitative and quantitative research methods in one study proved successful. In two domains, the quantitative findings confirmed the interpretations from the interviews and the findings could also be explained from them, strengthening the validity and generalizability of the results. Still, the qualitative data suggested that communication issues were more important than issues related to professional expertise. This was not confirmed in the survey. Being listened to was even given lowest priority for improvement, with all other issues being considered more important. These findings seem contradictory, because adolescents in the interviews clearly indicated that they liked to be consulted and wished to be involved in their own care. Perhaps this may be explained by adolescents’ assumption that “paying more attention to the needs of older children” (listed as top priority) also encompasses their preference to be seen as a partner in care. For example, in the interviews, the older adolescents highly valued “being treated as an adult”, which indicates a preference for direct communication, as well as for more voice and choice.Citation12
There were few differences between the preferences reported in the face-to-face interviews at the adolescents’ homes and in the peer-research interviews during the disco party. The most notable difference was that, in the peer research, adolescents were more convinced of the importance of meeting fellow patients and of being enabled to participate in hospital matters. Because the peer interviews lacked depth and did not yield substantial new insights, we realized that the participatory approach has its drawbacks. Adolescents with chronic conditions enjoy having a voice in the design and evaluation of health care services. However, the desirable extent of patient partnership (from patient perspective and in research) remains undefined.Citation40
Limitations of the study
Although the mixed methods approach may be seen as a strength, our study also had some weaknesses. The research was carried out in one university hospital in the Netherlands and the results may thus not apply to other settings and countries. Nevertheless, there are many similarities between countries in the reported care preferences of adolescents with chronic conditions.
We researched a wide range of health conditions and preferences, because all chronic patients have many tasks and challenges in common.Citation49 As a logical consequence, differences in experiences and preferences related to the chronic conditions themselves cannot be accounted for. Also, the nonresponse rate was fairly high for both the interview study and the questionnaire, while only a small number of adolescents attended the disco party, implying that the results may not be representative for the total population. Because girls and those with more extensive hospital experience were over-represented in the survey and among the peer research participants, this may have affected the outcomes.
Conclusion
Young people with chronic conditions are able and willing to express their views on the perceived quality of health care services provided to them. They have a strong preference for providers who are technically competent, honest, and straightforward. The older they are, the more concerned they are about providers focusing on them rather than on their parents and treating them like an adult. Adolescents grow out of pediatric care, and wish that the pediatric environment and staff attitudes would be less child-centered and more age-appropriate. Different needs according to gender, age, and educational level should also be acknowledged. Health care professionals should be aware of preferences, inquire into them, and adjust their communication style accordingly. This may strengthen adolescents’ competencies on their road to adulthood and help build positive, trusting relationships between professionals and their adolescent patients, which is a prerequisite of shared responsibility for treatment.
Acknowledgements
The “On Your Own Feet” project was funded by ZonMw, ie, the Netherlands Organization for Health Research and Development, and by Kinderpostzegels, a Dutch charity foundation. The disco party was made possible by Pekoenja, Leiden, and Sophia Kinderziekenhuis Fonds, Rotterdam, the Netherlands. We would like to express our gratitude to the hospital staff, students, young patients, and their parents for their collaboration in the studies. In particular, we gratefully acknowledge the commitment and enthusiasm of our adolescent coresearchers, the nurse specialists, and all others who participated in the “On Your Own Feet” research group, especially Jos Latour, Marijn Kuijper, and Andrea Rouland. Jane Sattoe, Annemiek Stoopendaal, and other colleagues are thanked for their constructive feedback, as well as Ko Hagoort for editorial assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
- HartCChessonRChildren as consumersBr Med J19983167144160016039596605
- CoyneIConsultation with children in hospital: Children, parents’ and nurses’ perspectivesJ Clin Nurs200615617116390525
- HomerCJMarinoBClearyPDQuality of care at a children’s hospital: The parent’s perspectiveArch Pediatr Adolesc Med1999153111123112910555712
- IreysHTPerryJJDevelopment and evaluation of a satisfaction scale for parents of children with special health care needsPediatrics19991045 Pt 21182119110545571
- YggeBMArnetzJEQuality of paediatric care: Application and validation of an instrument for measuring parent satisfaction with hospital careInt J Qual Health Care2001131334311330441
- CoJPFerrisTGMarinoBLHomerCJPerrinJMAre hospital characteristics associated with parental views of pediatric inpatient care quality?Pediatrics2003111230831412563056
- MackJWCoJPGoldmannDAWeeksJCClearyPDQuality of health care for children: Role of health and chronic illness in inpatient care experiencesArch Pediatr Adolesc Med2007161982883417768281
- CarterBChildren – silent consumers of health careJ Child Health Care1998225710474409
- FarrantBWatsonPDHealth care delivery: Perspectives of young people with chronic illness and their parentsJ Paediatr Child Health200440417517915009544
- ChesneyMLindekeLJohnsonLJukkalaALynchSComparison of child and parent satisfaction ratings of ambulatory pediatric subspecialty careJ Pediatr Health Care200519422122916010261
- MahJKToughSFungTDouglas-EnglandKVerhoefMAdolescent quality of life and satisfaction with careJ Adolesc Health2006385e601e607
- BrittoMTDeVellisRFHornungRWDeFrieseGHAthertonHDSlapGBHealth care preferences and priorities of adolescents with chronic illnessesPediatrics200411451272128015520107
- LittIFSatisfaction with health care: The adolescent’s perspectiveJ Adolesc Health199823259609714165
- AldersonPCompetent children? Minors’ consent to health care treatment and researchSoc Sci Med200765112272228317854964
- LindekeLNakaiMJohnsonLCapturing children’s voices for quality improvementMCN Am J Matern Child Nurs200631529029517013067
- PelanderTLeino-KilpiHQuality in pediatric nursing care: Children’s expectationsIssues Compr Pediatr Nurs200427313915115371112
- AldissSHorstmanMO’LearyCRichardsonAGibsonFWhat is important to young children who have cancer while in hospital?Children and Society20092328598
- AldersonPSutcliffeKCurtisKChildren as partners with adults in their medical careArch Dis Child200691430030316399782
- CoadJEShawKLIs children’s choice in health care rhetoric or reality? A scoping reviewJ Adv Nurs200864431832718990109
- GinsburgKRMenapaceASSlapGBFactors affecting the decision to seek health care: The voice of adolescentsPediatrics199710069229309374558
- GinsburgKRSlapGBCnaanAForkeCMBalsleyCMRouselleDMAdolescents’ perceptions of factors affecting their decisions to seek health careJAMA199527324191319187783300
- ChengTLSavageauJASattlerALDeWittTGConfidentiality in health care. A survey of knowledge, perceptions, and attitudes among high school studentsJAMA199326911140414078441216
- WoodgateRLHealth professionals caring for chronically ill adolescents: Adolescents’ perspectivesJ Soc Pediatr Nurs19983257689670167
- Dovey-PearceGHurrellRMayCWalkerCDohertyYYoung adults’ (16–25 years) suggestions for providing developmentally appropriate diabetes services: A qualitative studyHealth Soc Care Community200513540941916048529
- KlostermannBKSlapGBNebrigDMTivorsakTLBrittoMTEarning trust and losing it: Adolescents’ views on trusting physiciansJ Fam Pract200554867968716061053
- BeresfordBASloperPChronically ill adolescents’ experiences of communicating with doctors: A qualitative studyJ Adolesc Health200333317217912944007
- TivorsakTLBrittoMTKlostermannBKNebrigDMSlapGBAre pediatric practice settings adolescent friendly? An exploration of attitudes and preferencesClin Pediatr (Phila)2004431556114968893
- BattrickCGlasperEAThe views of children and their families on being in hospitalBr J Nurs200413632833615126966
- CoadJCoadNChildren and young people’s preference of thematic design and colour for their hospital environmentJ Child Health Care2008121334818287183
- UllánAMBelverMHSerranoIDelgadoJBadíaMPerspectives of youths and adults to improve the care of hospitalized adolescents in SpainJ Pediatr Health Care9202010 [Epub ahead of print]
- BrittoMTTivorsakTLSlapGBAdolescents’ needs for health care privacyPediatrics20101266e1469e147621098148
- KnopfJMHornungRWSlapGBDeVellisRFBrittoMTViews of treatment decision making from adolescents with chronic illnesses and their parents: A pilot studyHealth Expect200811434335419076663
- MoulesT‘They wouldn’t know how it feels ...’: Characteristics of quality care from young people’s perspectives: A participatory research projectJ Child Health Care200913432233219833668
- MokkinkLBvan der LeeJHGrootenhuisMAOffringaMvan PraagBMSHeymansHSAOmvang en gevolgen van chronische aandoeningen bij kinderen. [Extent and consequences of chronic conditions in children]Tijdschr Kindergeneeskd2007754138142 Dutch.
- SnelMCDokter, dit vind ik! Verbeterpunten voor een megacool ziekenhuis [Doctor, this is my opinion! Ideas for a megacool hospital]Kind en Ziekenhuis20062911822 Dutch.
- Van StaaALOn Your Own Feet Research GroupUnraveling triadic communication in hospital consultations with adolescents with chronic conditions: The added value of mixed methods researchPatient Educ Couns201182345546421194872
- van StaaALvan der StegeHAJedelooSMollHAHilberinkSReadiness to transfer to adult care of adolescents with chronic conditions: Exploration of associated factorsJ Adolesc Health201148329530221338902
- CreswellJWResearch Design: Qualitative, Quantitative, and Mixed Methods Approaches2nd edLondon, UKSage Publications2003
- O’CathainAMurphyENichollJWhy, and how, mixed methods research is undertaken in health services research in England: A mixed methods studyBMC Health Serv Res200778517570838
- Van StaaALJedelooSLatourJMTrappenburgMJExciting but exhausting: Experiences with participatory research with chronically ill adolescentsHealth Expect20101319510719682098
- BrymanABarriers to integrating quantitative and qualitative researchJ Mix Methods Res200711822
- O’CathainAMurphyENichollJThe quality of mixed methods studies in health services researchJ Health Serv Res Policy20081329298
- BraunVClarkeVUsing thematic analysis in psychologyQual Res Psychol20063277101
- Van StaaALJedelooSKuijperMLatourJMOp Eigen Benen. Jongeren met chronische aandoeningen: wat willen en kunnen zij in de zorg? [On Your Own Feet. Young people with Chronic Conditions: What are their Preferences and Competencies for Health Care?]Rotterdam, the NetherlandsHogeschool Rotterdam [Rotterdam University]2007
- JedelooSvan StaaALLatourJMvan ExelNJPreferences for health care and self-management among Dutch adolescents with chronic conditions: A Q-methodological investigationInt J Nurs Stud201047559360319900675
- FreakeHBarleyVKentGAdolescents’ views of helping professionals: A review of the literatureJ Adolesc200730463965316867305
- WrayJMaynardLSpecialist cardiac services: What do young people want?Cardiol Young200818656957418940027
- SmithSAdolescent units – an evidence-based approach to quality nursing in adolescent careEur J Oncol Nurs200481202915003741
- SawyerSMDrewSYeoMSBrittoMTAdolescents with a chronic condition: Challenges living, challenges treatingLancet200736995711481148917467519