
Abstract
Background
Effectiveness of pharmacist-led educational interventions on self-care activities and glycemic control of type 2 diabetes mellitus (T2DM) patients is vague. The purpose of this review is to appraise the effect of pharmacist-led educational interventions on self-care activities and levels of glycated hemoglobin of T2DM patients.
Methods
Five electronic databases were searched from date of database inception to September 2017. Randomized clinical trials examining the effectiveness of pharmacist-led educational interventions, directed at T2DM patients only, were included for systematic review and meta-analysis. The protocol is available with PROSPERO (CRD42017078854).
Results
Eleven studies, involving n=1,544 T2DM patients, were included in this systematic review. Meta-analysis demonstrated that pharmacist-led interventions had a significant effect on lowering of the levels of glycated hemoglobin (−0.66; 95% CI [−0.83, −0.50]; I2=58.3%; P=0.008), in comparison to usual care. Self-care activities were assessed by using Summary of Diabetes Self-care Activities tool in eight studies. Overall meta-analysis of self-care activities for included studies demonstrated a significant effect of pharmacist-led interventions on improvement of self-monitoring of blood glucose (1.62; 95% CI [0.92, 2.32]; I2=70.5%; P=0.005), foot care (1.20; 95% CI [0.49, 1.90]; I2=95.0%; P<0.001), and overall diet (1.16; 95% CI [0.38, 1.93]; I2=64.2%; P=0.094).
Conclusion
The findings of this review demonstrate a significantly positive effect of pharmacist-led educational interventions on HbA1c levels and self-care practices among T2DM patients.
Introduction
A steady and continuous growth in the number of reported cases of diabetes mellitus has been observed over the past decades.Citation1 According to the Global Diabetes Report by World Health Organization (WHO), there were approximately 422 million patients suffering from diabetes mellitus in 2014. The global prevalence of diabetes mellitus in the adult population has nearly doubled since 1980, rising from 4.7% to 8.5% in 2014. Diabetes prevalence is increasing more rapidly in low- and middle-income countries than in high-income countries. As such, the South-East Asian Region of WHO has seen a substantial increase in diabetes with roughly 96 million of diabetes patients in the region.Citation2,Citation3 In Ethiopia, 0.8 million diabetes cases were reported in 2000 and the figure is expected to skyrocket to 1.8 million by year 2030.Citation4
Keeping in view this massive increase in the number of diabetes cases, most of the diabetes foundations are emphasizing on the need to educate the patients about diabetes self-care which will further help in improving the clinical outcomes of the diabetes patients. Diabetes self-care is undertaken by individuals with or at risk of diabetes. It is a process in which necessary information and skills are acquired by the patients to successfully self-manage the disease and its complications for better health outcomes.Citation5 According to American Association of Diabetes Educators, there are seven key self-care activities in order to produce positive and efficacious outcomes. These activities include, proper diet, being physically active (regular exercising), monitoring of blood glucose level, adherence and compliance of medications, problem-solving skills, healthy coping skills, and finally, risk reducing behaviors.Citation6 Positive correlation has been proven between all seven activities with favorable glycemic control, significant reduction in late complications, and improved quality of life.Citation7 In other words, nonadherence to self-care activities can lead to lower health-related quality of life.Citation8,Citation9
Additionally, it is noticed that diabetes self-care also assists in improving adherence to the medications, which assists in controlling the medication cost and morbidity and mortality rates. In acknowledgement to this problem, the involvement of different health care professionals in interdisciplinary health care approach is seen to be a useful strategy to educate the public about the importance of adherence and subsequently improving overall health outcomes especially in patients with diabetes.Citation10 Health care providers can collaborate with public health agencies and come out with programs to assist diabetic patients and their families.Citation11 In the United States, programs such as state Diabetes Control Program and Living with Type 2 Diabetes Program assist health care professionals to implement diabetes interventions, increase access to quality diabetes care, and promote public awareness about diabetes.Citation12
In the last few years with the emergence of pharmacist’s role in direct patient care, clinical pharmacists with pharmacotherapeutic knowledge are playing a vital role in educating patients during dispensation process. Accurate directions for use of medicines and self-care advises incorporated into the counseling process are essential in educating people with diabetes. According to American College of Clinical Pharmacy, one of the key roles of clinical pharmacists is to educate the patients by giving them advises on important strategies for best possible treatment outcomes so as to improve or maintain their health.Citation13
Pharmacist-led interventions include variety of services, ranging from education on diabetes, complications associated with diabetes, self-management, medication adherence, telemedicine, and pharmaceutical care planning. Clinically significant effect of pharmacy-based interventions have been reported by few systematic reviews.Citation14–Citation19 The positive impact of pharmacist-led interventions is directly associated with reductions in micro- and macrovascular complications associated chronic diabetes.Citation16 Systematic reviews have previously been conducted to appraise the effect of pharmacy-based interventions on clinical and nonclinical parameters of people with diabetes.Citation14,Citation16 However, to date, there is hardly any summative evidence in the form of meta-analysis that scrutinize the impact of pharmacist-led educational interventions on self-care activities and glycemic control of type 2 diabetes patients. This systematic review will assess the impact of pharmacist-led educational interventions on patients’ self-care practices and glycated hemoglobin (HbA1c) levels.
Methods
This systematic review and meta-analysis was performed according to PRISMA guidelines.
Database and search strategies
An online search was made from date of database inception till September 2017, from five databases, namely, PubMed, ProQuest, Scopus, EBSCOhost, and Ovid, by using the following search strategy: Diabetes Mellitus, Type 2 OR T2DM OR Non-insulin dependent diabetes mellitus OR NIDDM OR Type 2 diabetes AND Pharmaceutical care OR Clinical pharmacy OR Community pharmacy OR Pharmacist* OR Pharmaceutical services OR Education OR Intervention OR “Self-care” OR Self-management OR Medication Management AND Knowledge OR Haemoglobin A, Glycosylated OR HbA1c OR glycemic control OR Behavior change.
Outcomes
The outcomes of interest were glycemic control, which was measured by HbA1c, and self-care activities, such as, diet control, physical activity, and self-monitoring of blood glucose (SMBG).
Selection criteria
The studies were included in this systematic review if they were 1) randomized controlled trials (RCTs); 2) evaluating the effectiveness of educational interventions delivered by pharmacists (alone or in collaboration with other health care professionals); 3) conducted on patients with type 2 diabetes only; 4) reporting both self-care activities and HbA1c; and 5) available in English language. Conference abstracts, review articles, and non-RCT interventional studies were excluded.
Data extraction
After completion of the literature search, two researchers (AB and TMK) reviewed the titles and abstracts of all identified studies and selected the articles that fulfilled the study selection criteria. One researcher (AB) independently extracted the data from each identified study and recorded on a standardized data extraction form. The data extraction form was piloted on a selection of included studies in order to check whether it is adequate to capture all relevant information.
The data extracted from the selected studies in this review included the following: author names, year of publication, study design, health care setting and country where this study was conducted, duration of study, patient characteristics (number of participants, gender, and age), contents of the intervention, and outcome measures. AB extracted the data, which was checked and verified by another researcher (TMK); inconsistencies in the extracted data were resolved by discussion and consensus.
Risk of bias (quality) assessment
Quality assessment of the included studies was done by two reviewers (AB and XT) by using Cochrane risk of bias (ROB) tool. This quality assessment was checked by a third researcher (TMK). The criteria that were used for quality assessment included the following: biasness associated with random sequence generation, allocation concealment, blinding for outcome evaluation, the extent of outcome data completeness, selective reporting, and other sources of bias. Each item of tool was rated, either as “low risk” (if it was unlikely that a bias would seriously alter the results), or “unclear” (if it was likely that a bias would raise some doubt about the results), or “high risk” (if it was likely that a bias would seriously alter the results). Disagreements were resolved through discussion.
Data analysis
Meta-analysis was performed by using STATA version 14®. Weighted mean difference (WMD) was estimated to calculate the overall comparative effect of all interventions using random-effects model. For the meta-analysis, WMD < 0 will indicate an improvement in the self-care activities (specific diet, general diet, overall diet, physical activity, SMBG and foot care), however WMD < 0 will represent reduction of HbA1c levels. All the P-values were set to be <0.05 with 95% CIs (according to whether the confidence interval included the null value) to assess significance. Subgroup analyses were performed on the basis of quality of the studies, in order to explain the heterogeneity among the studies. Inconsistency among the included studies was quantified by using I2 statistic, which was appraised by the following criteria: 0%–40%, might not be important; 30%–60%, may represent moderate heterogeneity; 50%–90%, may represent substantial heterogeneity, and 75%–100%, considerable heterogeneity.Citation20
Sensitivity analysis was done to check the robustness of the results by performing subgroup analysis regarding baseline HbA1c levels (<8% and ≥8%), duration of interventions, and geographical areas of the studies and their influence on HbA1c.
Study protocol registration
The study protocol is registered with PROSPERO (Registration No CRD42017078854).
Results
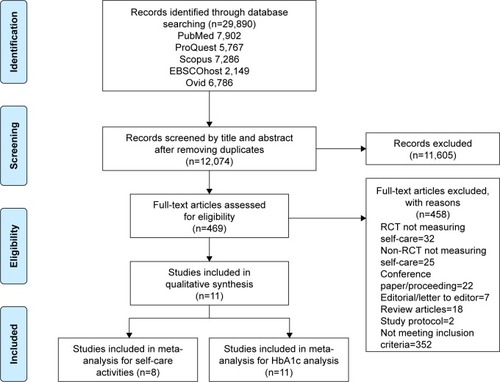
In total, 29,890 articles were identified initially from five electronic databases. After removing duplication and performing title and abstract screening, 469 articles were identified. Full-text assessment of these 469 articles resulted in identification of 11 articles meeting our inclusion criteria; the details are presented in PRISMA flow diagram of .
Figure 1 PRISMA flow diagram of the study selection.
Description of the included studies
Among the n=11 included studies, parallel-group design of RCTs was adopted.Citation21–Citation31 The study duration of all studies ranged from 4 months to 12 months. Three studies had a study duration <6 months,Citation28,Citation30,Citation31 n=6 studies’ duration was 6 months,Citation21,Citation23,Citation24,Citation26,Citation27,Citation31 and n=2 studies’ duration was 12 months.Citation22,Citation25 All of the included studies (n=11) were conducted on type 2 patients (n=1,544). Some studies imposed certain criteria on the type 2 patients’ recruitment, such as patients who were using oral hypoglycemic medications,Citation28 and poorly controlled type 2 diabetes.Citation24 Majority of the studies included in this review (n=5) were conducted in Asia subcontinent,Citation23,Citation24,Citation28,Citation29,Citation31 followed by North America (n=4),Citation21,Citation22,Citation25,Citation30 and Europe (n=2).Citation26,Citation27
Description of pharmacist-led educational interventions
In most of the studies (n=8), educational intervention was performed by the pharmacist alone,Citation22,Citation23,Citation25–Citation29,Citation31 whereas, in rest of the studies (n=3) it was performed by a multidisciplinary health care team, such as nurses, physicians, dieticians, involving pharmacist as a member of team.Citation21,Citation24,Citation30 Summary of Diabetes Self-care Activities (SDSCA) was the most frequently used tool (n=8) in the included studies for assessment of the impact of educational interventions on self-care behaviors of the diabetes patients.Citation21–Citation23,Citation25–Citation28,Citation31 This eleven items tool is comprised of five domains of self-care, which include, diet (first four items), exercise (two items), blood glucose testing (two items), foot care (two items), and smoking (one item). This tool requires the respondents to rate their diabetes-related self-care activates of past 7 days on eight-point Likert scale. The diet domain (overall diet) of the tool is further composed of two subdomains, namely, General diet (first two items of the scale) and Specific diet (items three and four of the tool).Citation32
One study used Diabetes self-care (DSC) scale,Citation24 and the other two studies used nonvalidated diabetes self-care assessment tool.Citation29,Citation30 Details of contents of pharmacist-led educational interventions are presented in .
Table 1 Characteristics of the included studies (n=11)
Risk of bias assessment
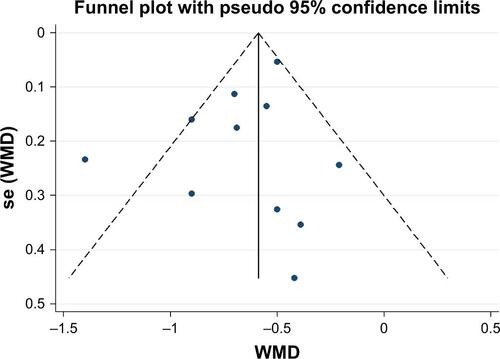
The ROB of the included RCTs (n=11 studies) by using Cochrane ROB tool is presented in (ROB summary) and (ROB graph). Most of the studies (<80%) were free from attrition bias, selection bias, performance bias, detection bias, and reporting bias. Publication bias was checked by using funnel plot, and the Egger test was performed to check the funnel-plot asymmetry in meta-analysis.
Outcomes
Self-care activities
Effect of pharmacist-led educational intervention on self-care activities was measured by using a validated SDSCA tool in majority of the studies (8 out of 11). The results of eight studies that used SDSCA tool were pooled together for meta-analysis. Overall, a significant effect of pharmacist-led interventions was observed on different domains of patients’ self-care practices, such as overall diet (1.16; 95% CI [0.38, 1.93]; I2=64.2%; P=0.094), foot care (1.20; 95% CI [0.49, 1.90]; I2=95.0%; P<0.001), and SMBG (1.62; 95% CI [0.92, 2.32]; I2=70.5%; P=0.005).
Whereas, among rest of the three studies, which did not use SDSCA tool, statistically insignificant change (P=0.61) in the self-care behaviors was reported by Kang et al, in type 2 diabetes patients, after 6 months of the intervention.Citation24 On the other hand, significantly improved compliance was observed by Samtia et al, among intervention group patients, toward foot care (P<0.001) and SMBG (P=0.001).Citation29 Similar findings were also observed by Taveira et al, where a significant improvement (P=0.01) in adherence toward self-care behaviors was observed, especially for SMBG (P=0.01).Citation30
Exercise
By using SDSCA tool, n=8 studies measured the effect of pharmacist-led educational intervention on exercise for type 2 diabetes patients, which is one of the key factors for diabetes self-care. The results of an overall meta-analysis favored the pharmacist-led education on exercise (WMD =0.94; 95% CI [0.72, 1.16]; I2=17.9%; P=0.288), as shown in .
Figure 2 Overall meta-analysis of all categories of Summary of Diabetes Self-care Activities.
Abbreviation: WMD, weighed mean difference.
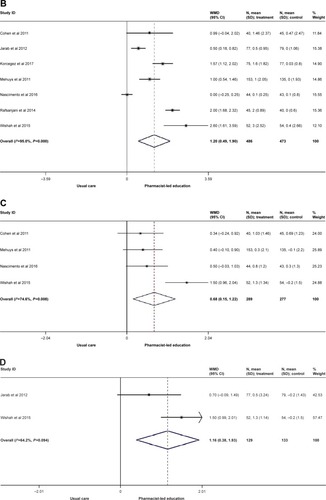
Foot care
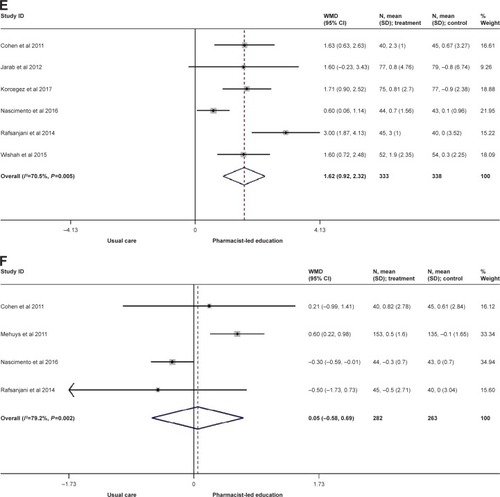
Foot care was examined by n=7 studies, and the results of an overall meta-analysis favored pharmacist-led education (WMD =1.20; 95% CI [0.49, 1.90]; I2=95.0%; P<0.001; ). Due to significant heterogeneity among these (n=7) studies (I2=95.0%), subgroup analyses were performed based on the ROB (unclear, low, and high) of the seven studies. It was found that the heterogeneity of the unclear ROB groupCitation21,Citation27 notably decreased from 95.0% to 70.2%. However, the studies in low ROB groupCitation23,Citation26,Citation28,Citation31 showed only a slight decrease in heterogeneity (I2=94.1%; ). There was no I2 value for the high ROB group, as there was only one study with high ROB,Citation25 thus there was no comparison of data to obtain I2 value. Significantly high effect of interventions was observed by the studies with low ROB (WMD =1.46; 95% CI [0.58, 2.35]; I2=94.1; P<0.001), when compared with the studies with unclear ROB (WMD =0.36; 95% CI [−0.57, 1.30]; I2=70.2%; P=0.067).
Figure 3 Subgroup meta-analysis for different categories of Summary of Diabetes Self-care Activities scale.
Abbreviation: WMD, weighed mean difference.

General diet
Effect of pharmacist-led educational interventions on general diet was examined by n=4 studies. Results of overall meta-analysis were in favor of the pharmacist-led education (WMD =0.68; 95% CI [0.15, 1.22]; I2=74.6%; P=0.008), however the overall heterogeneity was high, as shown in . Therefore, a subgroup analysis based on the ROB of each study was performed. The studies with low ROBCitation26,Citation31 showed greater effect on general diet (WND =0.94; 95% CI [−0.13, 2.02]; I2=88.4%; P=0.003) when compared with the studies with unclear ROBCitation21,Citation27 (WMD =0.43; 95% CI [0.04, 0.82]; I2=0%; P=0.688); details are presented in .
Overall diet
Another analysis was performed with two studies for overall diet. The results favored the pharmacist-led intervention, toward overall diet in type 2 diabetes patients (WMD =1.16; 95% CI [0.38, 1.93]; I2=64.2%; P=0.094; ).
Self-monitoring of blood glucose
By using SDSCA scale, n=6 studies examined the effect of pharmacist-led interventions on SMBG. The results of overall meta-analysis were in favor of pharmacist-led education on better practices toward SMBG, when compared with usual care (WMD =1.62; 95% CI [0.92, 2.32]; I2=70.5%; P=0.005; ). A subgroup analysis was performed according to the ROB of each study. The heterogeneity of the unclear ROB subgroupCitation21,Citation23,Citation27 decreased significantly compared with the previous overall I2 value (I2=46.8%). There was only n=1 study in the high ROB subgroup;Citation25 therefore, the I2 value cannot be obtained, but the result was still in favor of the pharmacist-led education. For the low ROB subgroup, the I2 value increased slightly to 72.9%. Also, the studies with low ROB showed significantly better effect (WMD =2.25; 95% CI [0.88, 3.62]; P=0.055) when compared with the studies with Unclear ROB (WMD =1.08, 95% CI [0.30, 1.87]; P=0.153; ).
Specific diet
Effect of pharmacist-led educational interventions on specific diet was examined by n=4 studies. The results of overall meta-analysis showed no effect on specific diet (WMD =0.05; 95% CI [−0.58, 0.69]; P=0.002; ). However, the heterogeneity was high (I2=79.2%). A subgroup analysis was performed according to the ROB of each study. The studies with low ROBCitation26,Citation28 (WMD =0.21; 95% CI [−0.82, 1.24]; I2=64.4%; P=0.094) as well as with unclear ROBCitation21,Citation27 (WMD =−0.27; 95% CI [−0.56, 0.01]; I2=0%; P=0.417) showed insignificant effect on specific diet ().
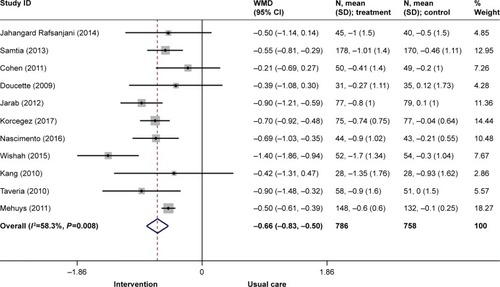
Glycated hemoglobin
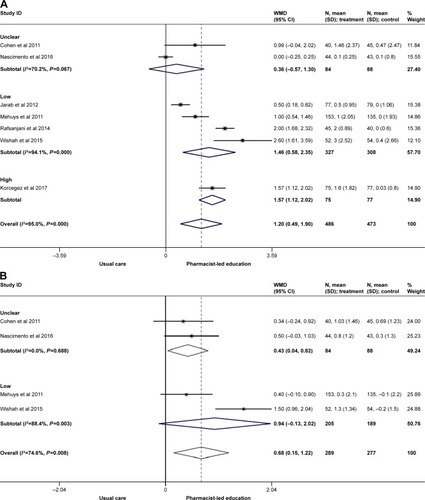
Glycemic control of the all the included studies (n=11) was measured by HbA1c. WMD was estimated for overall meta-analysis of the included studies. The meta-analysis showed an overall effect in favor of the pharmacist-led educational interventions on HbA1c, where the levels of HbA1c reduced with a mean difference of −0.66% (95% CI [−0.83, −0.50]; I2=58.3%; P=0.008), as shown in .
Figure 4 Overall meta-analysis for glycated hemoglobin of the included studies (n=11).
Abbreviation: WMD, weighed mean difference.
Moderation of effectiveness of intervention and study features on HbA1c
The findings of subgroup meta-analysis revealed that the studies that were conducted in Asian countries (n=5) showed a comparatively larger effect on HbA1c level reduction (WMD =−0.80; 95% CI [−1.14, −0.46]; I2=66.3%; P=0.018) when compared with the studies (n=4) that were conducted in North America (WMD =−0.58; 95% CI [−0.86, −0.31]; I2=35.1%; P=0.201) and Europe n=2 (WMD =−0.52; 95% CI [−0.64, −0.40]; I2=7%; P=0.300; ). When self-care education was provided by pharmacist alone, comparatively more reduction in HbA1c level was examined (WMD =−0.70; 95% CI [−0.88, −0.52]; I2=65.5%; P=0.005) in comparison to the intervention where education was given by pharmacist in a team (WMD =−0.50; 95% CI [−0.95, −0.04]; I2=38.3%; P=0.198; ). No significant difference on WMD of HbA1c was observed when other features of the studies, such as, duration of invention and baseline HbA1c levels were examined ( and , respectively).
Publication bias
The symmetrical presentation of the funnel plot for HbA1c for all studies (n=11) indicated slight publication bias, as the majority of the studies were with 95% CI () along with Egger test, where the bias was −0.86 (95% CI =−2.63, 0.90; P=0.298).
Discussion
Based on the evidence synthesized from the overall meta-analysis of RCTs (n=11), included in this review, it is evident that pharmacist-led educational interventions have clinically significant effect on glycated hemoglobin (−0.66; 95% CI [−0.83, −0.50]; I2=58.3%) and on various domains of self-care activities, such as, on SMBG (1.62; 95% CI [0.92, 2.32]; I2=70.5%), foot care (1.20; 95% CI [0.49, 1.90]; I2=95.0%), and overall diet (1.16; 95% CI [0.38, 1.93]; I2=64.2%).
The ROB of most of the included studies was low in different domains; however, there is still a significant percentage of unclear and low ROB in few studies. Among the included studies, Korcegez et al,Citation25 has the highest percentage of high ROB, whereas Samtia et al,Citation29 has the highest percentage of unclear ROB. These studies might lead to an overestimate or underestimate for the effect of pharmacist-led education toward the observed outcomes of people with diabetes. Slight evidence of publication bias was confirmed by funnel plot and Eggers test. To address the issue of high heterogeneity, subgroup meta-analysis was performed on the basis of quality of the studies. The findings of subgroup meta-analysis revealed that the studies with low ROB had a comparatively larger effect of pharmacist-led interventions on foot care (1.46; 95% CI [0.58, 2.35]; I2=94.1%), general diet (0.94; 95% CI [−0.13, 2.02]; I2=88.4%), SMBG (2.25; 95% CI [0.88, 3.62]; I2=72.9%), and specific diet (WMD =0.21; 95% CI [−0.82, 1.24]; I2=64.4%), when compared with studies with unclear or high ROB.
Similarly, clinically important reductions were observed in HbA1c levels when self-care education was provided by pharmacist (−0.70; 95% CI [−0.88, −0.52]; I2=66%), as evident from subgroup meta-analysis. A similar effect of pharmacist-led interventions on HbA1c levels was reported by van Eikenhorst et al,Citation15 (−0.70; 95% CI [−0.91, −0.51]) and Cranor et al.Citation33 Likewise, Pousinho et alCitation16 [−0.18% to −2.1%] and Machado et alCitation17 [1.00% ± 0.28%; P<0.001] in their systematic reviews also reported statistically significant reductions in HbA1c. Inclusion of pharmaceutical care component to the pharmacist-led educational intervention resulted in comparatively more reductions in HbA1c levels as shown by Wishah et alCitation31 [−1.40; 95% CI −1.86, −0.94]. Further research is required to examine the effect of components, cost and delivery of interventions on clinical and patient-reported outcomes of patients with type 2 diabetes, in order to design a cost-effective intervention.
Micro- and macrovascular complications in chronic patients with type 2 diabetes are directly associated with glycemic control. Effective diabetes self-care education provided by health care providers can minimize the chances of such complications, which occur as a consequence of poor glycemic control. Being an expert in pharmacotherapy and easily approachable, when compared with other overburdened health care providers, pharmacists can play an effective role by providing self-care education in addition to pharmaceutical care in a variety of health care settings. Especially, people with diabetes from low- and middle-income countries can rely more on pharmacists within the community and it will decrease dependence on the limited public hospitals and will facilitate in achieving favorable health outcome.
Limitations
One of the limitation of this systematic review is the relatively small sample size of the included studies, thus the results are subject to greater sampling variation and hence might be interpreted with care. In addition, heterogeneity among the included studies was another limitation to this study, which could be due to variability of patient populations and interventions. Despite the heterogeneity, most of the outcomes were in favor of the pharmacist-led education. To address the issue of high heterogeneity, subgroup analysis and funnel plot for publication bias were performed for the pooled results of HbA1c. The symmetrical shape of funnel plot indicated low risk of publication bias, but the heterogeneity remained same after subgroup analysis, which could possibly be due to varied population characteristics. Thus, the high heterogeneity values should not greatly affect the conclusion of this systematic review.
Conclusion
This systematic review demonstrates a positive impact of pharmacist-led educational interventions on glycemic control and diabetes-related self-care activities of type 2 diabetes patients, which are surrogate markers for disease progression and its related complications. Therefore, pharmacists should take an active role in providing diabetes self-care education in conjunction with euglycemic medicines, in order to improve patient outcomes.
Supplementary materials
Figure S1 Risk of bias summary of included studies (n=11).
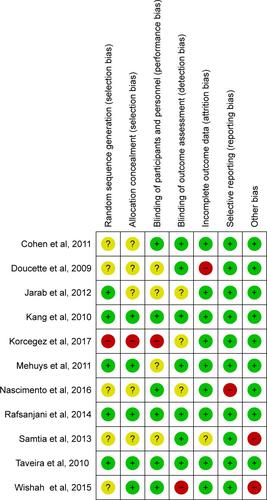
Figure S2 Risk bias graph of included studies (n=11).
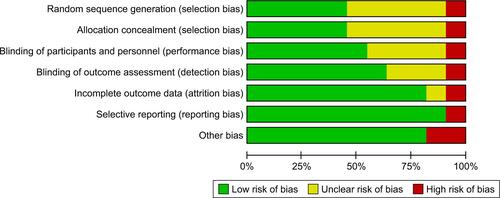
Figure S3 Sub-group meta-analysis for HbA1c on the basis of region (n=11). Weights are from random effects analysis.

Figure S4 Sub-group meta-analysis for HbA1c of included RCTs on the basis of intervention provider (n=11).
Note: Weight are from random effects analysis.
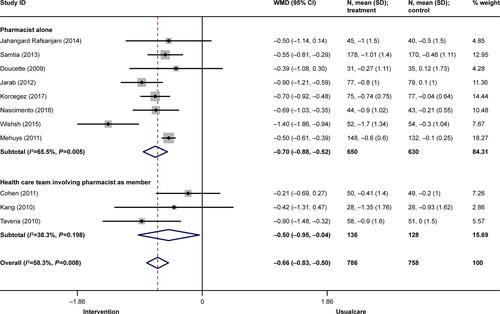
Figure S5 Sub-group meta-analysis for HbA1c of included RCTs on the basis of duration of study (n=11).
Note: Weights are from random effects analysis.

Figure S6 Sub-group meta-analysis for HbA1c of included RCTs on the basis of baseline HbA1c (n=11).
Note: Weights are from random-effects analysis.
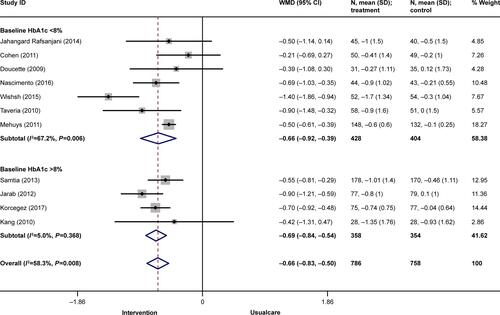
Figure S7 Funnel Plot of Publication Bias.
Disclosure
AB received a PhD Merit Scholarship from Monash University. KGC received a grant from the University of Malaya (PG089-2015B). The authors report no other conflicts of interest in this work.
References
- World Health OrganizationDiabetes [webpage on the Internet]. Key facts2017 Available from: http://www.who.int/news-room/fact-sheets/detail/diabetesAccessed April 24, 2018
- MohanVRuchiVGayathriRSlowing the diabetes epidemic in the World Health Organization South-East Asia Region: the role of diet and physical activityWHO South East Asia J Public Health20165151628604391
- CousinsSAddressing Asia’s fast growing diabetes epidemicBull World Health Organ20179555055128804165
- AnimawWSeyoumYIncreasing prevalence of diabetes mellitus in a developing country and its related factorsPLoS One20171211e018767029112962
- DeakinTMcShaneCECadeJEWilliamsRDGroup based training for self-management strategies in people with type 2 diabetes mellitusCochrane Database Syst Rev20052CD003417
- American Association of Diabetes EducatorsAADE Position Statement. AADE 7TM Self-Care BehaviorsDiabetes Educ200834344544918535317
- ShrivastavaSRShrivastavaPSRamasamyJRole of self-care in management of diabetes mellitusJ Diabetes Metab Disord20131211423497559
- SalehFMumuSJAraFHafezMAAliLNon-adherence to self-care practices & medication and health related quality of life among patients with type 2 diabetes: a cross-sectional studyBMC Public Health20141443124885315
- JannooZWahYBLazimAMHassaliMAExamining diabetes distress, medication adherence, diabetes self-care activities, diabetes-specific quality of life and health-related quality of life among type 2 diabetes mellitus patientsJ Clin Transl Endocrinol20179485429067270
- ErkuDAAyeleAAMekuriaABBelachewSAHailemeskelBTegegnHGThe impact of pharmacist-led medication therapy management on medication adherence in patients with type 2 diabetes mellitus: a randomized controlled studyPharm Pract20171531026
- American Association of Diabetes EducatorsPosition statement. Diabetes Education and Public Health. American Association of Diabetes EducatorsDiabetes Educ200026460760911142264
- MarathePHGaoHXCloseKLAmerican diabetes association standards of medical care in diabetesJ Diabetes20179432032428070960
- American College of Clinical Pharmacy [webpage on the Internet]About Clinical Pharmacists2017 Available from: https://www.accp.com/about/clinicalpharmacists.aspxAccessed December 1, 2017
- YaghoubiMMansellKVatanparastcHSteevesMZengWFaragMEffects of pharmacy-based interventions on the control and management of diabetes in adults: a systematic review and meta-analysisCan J Diabetes201741662864129224636
- van EikenhorstLTaxisKvan DijkLde GierHPharmacist-led self-management interventions to improve diabetes outcomes. A systematic literature review and meta-analysisFront Pharmacol2017889129311916
- PousinhoSMorgadoMFalcãoAAlvesGPharmacist interventions in the management of type 2 diabetes mellitus: a systematic review of randomized controlled trialsJ Manag Care Spec Pharm201622549351527123912
- MachadoMBajcarJGuzzoGCEinarsonTRSensitivity of patient outcomes to pharmacist interventions. Part I: systematic review and meta-analysis in diabetes managementAnn Pharmacother200741101569158217712043
- WubbenDPVivianEMEffects of pharmacist outpatient interventions on adults with diabetes mellitus: a systematic reviewPharmacotherapy200828442143618363526
- BukhshAKhanTMLeeSWHLeeLHChanKGGohBHEfficacy of pharmacist based diabetes educational interventions on clinical outcomes of adults with type 2 diabetes mellitus: a network meta-analysisFront Pharmacol2018933929692730
- DeeksJJHigginsJPAltmanDGAnalysing data and undertaking meta-analysesCochrane Handbook for Systematic Reviews of Interventions: Cochrane book seriesWest SussexWiley-Blackwell2008243296
- CohenLBTaveiraTHKhatanaSADooleyAGPirragliaPAWuWCPharmacist-led shared medical appointments for multiple cardiovascular risk reduction in patients with type 2 diabetesDiabetes Educ201137680181222021025
- DoucetteWRWitryMJFarrisKBMcDonoughRPCommunity pharmacist-provided extended diabetes careAnn Pharmacother200943588288919401477
- JarabASAlqudahSGMukattashTLShattatGAl-QirimTRandomized controlled trial of clinical pharmacy management of patients with type 2 diabetes in an outpatient diabetes clinic in JordanJ Manag Care Pharm201218751652622971205
- KangCMChangSCChenPLComparison of family partnership intervention care vs conventional care in adult patients with poorly controlled type 2 diabetes in a community hospital: a randomized controlled trialInt J Nurs Stud201047111363137320371056
- KorcegezEISancarMDemirkanKEffect of a pharmacist-led program on improving outcomes in patients with type 2 diabetes mellitus from northern cyprus: a randomized controlled trialJ Manag Care Spec Pharm201723557358228448779
- MehuysEvan BortelLde BolleLEffectiveness of a community pharmacist intervention in diabetes care: a randomized controlled trialJ Clin Pharm Ther201136560261321143256
- NascimentoaTBrazNGomesEFernández-ArcheAde La PuertaRSelf-care improvement after a pharmaceutical intervention in elderly type 2 diabetic patientsCurr Diabetes Rev201512212012826201426
- Jahangard-RafsanjaniZSarayaniANosratiMEffect of a community pharmacist-delivered diabetes support program for patients receiving specialty medical care: a randomized controlled trialDiabetes Educ201541112713525420946
- SamtiaAMRasoolMFRanjhaNMUsmanFJavedIA multifactorial intervention to enhance adherence to medications and disease-related knowledge in type 2 diabetic patients in Southern Punjab, PakistanTrop J Pharm Res2013125851856
- TaveiraTHFriedmannPDCohenLBPharmacist-led group medical appointment model in type 2 diabetesDiabetes Educ201036110911719966072
- WishahRAAl-KhawaldehOAAlbsoulAMImpact of pharmaceutical care interventions on glycemic control and other health-related clinical outcomes in patients with type 2 diabetes: randomized controlled trialDiabetes Metab Syndr20159427127625301007
- ToobertDJHampsonSEGlasgowREThe summary of diabetes self-care activities measure: results from 7 studies and a revised scaleDiabetes Care200023794395010895844
- CranorCWBuntingBAChristensenDBThe Asheville Project: long-term clinical and economic outcomes of a community pharmacy diabetes care programJ Am Pharm Assoc2003432173184