
Abstract
Purpose
This study aimed to assess awareness of glycated hemoglobin (A1C) testing and targets, perceived level of glycemic control and risk of complications, attitudes toward medications and self-management, and regimen-related distress in an international sample of patients with type 2 diabetes (T2D).
Methods
The descriptive study used a single time-point survey of adults in online health communities in the USA, Canada, the UK, Germany, Spain, and Mexico, who self-reported T2D diagnosed by a physician.
Results
In total, 661 patients participated. Awareness of their A1C value at last test varied considerably between countries (42%–89%), as did awareness of having an A1C target (26%– 70%). Self-reported A1C values were similar across US, Canadian, and European respondents (mean, 6.8%–7.3%). Approximately two-thirds of respondents from these countries (66%–71%) reported that their T2D was very or fairly well controlled, and few (5%–15%) expected to experience serious complications within 1 year. However, many respondents expected to experience microvascular (rather than macrovascular) complications in this time frame (eg, nerve pain, 5%–47%). Self-reported adherence to oral medication was generally high, with most respondents (86%–98%) taking their pills or tablets as directed by their healthcare provider, although for insulin injections adherence was lower in the USA (71%) and Mexico (78%) than in the other countries (86%–95%). The majority of respondents across countries (71%–79%) reported that taking injectable medications was not at all or a little burdensome. Respondents across countries appeared to be reasonably confident that they could adequately manage their blood sugar levels; despite this, a sizeable minority (21%–35%) had clinically significant levels of regimen-related distress.
Conclusion
Limited patient awareness of their A1C value and the potential complications of poorly controlled T2D, particularly regarding cardiovascular complications, may be a widespread problem. Furthermore, greater patient support may be needed to improve self-management of T2D and to reduce regimen-related distress.
Introduction
Adequate glycemic control is crucial to reducing the risk of complications from type 2 diabetes (T2D), which can include myocardial infarction, stroke, peripheral artery disease, lower limb amputation, vision loss, heart failure, nephropathy, retinopathy, and neuropathy.Citation1 Evidence-based guidelines for management of T2D recommend a combination of lifestyle changes and medication (insulin and oral hypoglycemic agents) to control blood glucose, as well as medication to control the cardiovascular disease risk and regular screening for early detection of complications.Citation1,Citation2 These guidelines typically stipulate that patients with T2D should have an individualized glycated hemoglobin (A1C) target, often aiming for as low as 7.0% or 6.5%, depending on additional patient-specific factors such as age, duration of diabetes, comorbidities, and risk of hypoglycemia.Citation2–Citation5 However, despite the availability of these guidelines, patients’ glycemic control appears to remain suboptimal to various degrees worldwide,Citation6,Citation7 including in both high-incomeCitation8,Citation9 and low to medium-income countries.Citation10 In the MOSAIc study, for example, a multinational, longitudinal, observational study of adults with T2D using insulin, the mean participant A1C value across 18 countries at baseline was 8.2%, despite a mean target A1C of 6.9%.Citation7 This study also showed that there is considerable variation among countries in terms of patients’ demographic characteristics, medical histories, drug treatment regimens, and self-reported knowledge of, and distress about, diabetes.Citation7
Patient self-management is a critical aspect of T2D care. Patients’ knowledge and perceptions of their glycemic control and T2D medication can impact treatment adherence and diabetes outcomes. Several studies have shown that limited numbers of patients are aware of their current and target A1C levels.Citation11–Citation13 In addition, patients’ adherence to their T2D medication can be limited by critical beliefs about their medications (such as perceived treatment inefficacy), and the perceived burden regarding obtaining and taking their medication (including treatment complexity, out-of-pocket costs, and hypoglycemia).Citation14,Citation15 Patients with elevated A1C levels who display poor self-management behavior are less likely to receive treatment intensification,Citation16,Citation17 thereby prolonging or exacerbating their inadequate glycemic control. However, it is not clear what patients perceive to be the consequences of poor glycemic control, or how this may vary between countries.
Online health communities aim to bring patients together to share their experiences and offer support for living with conditions such as diabetes. These communities offer an opportunity to exchange information outside of the clinic environment. The aims of this survey-based international study of patients with T2D in online health communities were to assess the level of patient awareness of A1C testing and targets, to uncover patient attitudes toward, and preferences for, T2D pharmacological treatments, and to determine patient-perceived consequences of poor glycemic control. Patients from Canada, Germany, Mexico, Spain, the UK, and the USA were surveyed. The prevalence of diabetes among adults in these countries ranges from 5.9% in the UK to 14.0% in Mexico (Table S1).Citation18 The general target A1C value for most adults with T2D stipulated by each country’s national T2D management guidelines is 7.0% or below, with the exception of the German guidelines that recommend a target range of 6.5%–7.5% (Table S1), and all advise that the target should be tailored to the individual patient.Citation3,Citation19–Citation23
Methods
Study population and conduct
Patients aged 18 years or older who resided in Canada, Germany, Mexico, Spain, the UK, or the USA and who self-reported that they had been diagnosed with T2D by a physician were eligible to participate in the study. Patients also had to be able to read and understand the language in which the survey was presented, which was the official language of the country (ie, English, German, or Spanish). Those patients who were diagnosed with T2D within the previous 6 months were excluded, because they may not have had sufficient experience of their diabetes to answer the questions in an informed manner.
Approval to field the survey in the USA and Canada was granted by the Western Institutional Review Board (Puyallup, WA, USA; Vancouver, BC, Canada) and was not required in the other countries. The appropriate regulatory bodies in the UK (Health Research Authority) and Spain (Agencia Española de Medicamentos y Productos Sanitarios), and local colleagues in Germany and Mexico, confirmed that approval was not required to field the survey in these countries. Participants gave their informed consent by completion of an online form before taking the survey.
Data source
Data for this descriptive study were obtained by surveying patients who were members of online health communities hosted by PatientsLikeMe (for patients resident in the USA and Canada), Carenity (for patients resident in Germany, Spain, and the UK), or HealthUnlocked (for patients resident in Mexico). Eligible members of the PatientsLikeMe platform were invited to participate through a private message sent to their account, directing them to the study on the PatientsLikeMe website. Users who did not complete the survey received up to three reminders. Eligible members of T2D communities hosted by Carenity and HealthUnlocked were sent pop-up invitations, weekly for Carenity members and once only for HealthUnlocked members, that directed them to internal landing pages for the study within the Carenity or HealthUnlocked platforms. Invitations were sent in members’ native languages. The survey was fielded for 2 weeks, or until a sample of 100 respondents per country was achieved.
Survey instrument
The single time-point survey was designed to assess patient perceptions and attitudes about A1C and its impact on health outcomes (Appendix S1). The survey also included a series of questions on goal-setting, management of diabetes, treatments, and adherence, as well as demographic and health history information (Table S2).
Survey items were derived from the results of targeted literature reviewsCitation6,Citation7,Citation11,Citation14,Citation24–Citation26 and the relevant experience of the authors. Perceived diabetes control was assessed as in a previous cross-national study:Citation25 participants were asked whether they believed that their last A1C test result meant that they were doing well or poorly on a four-point Likert scale (very well, fairly well, fairly poorly, very poorly), or they could select “I don’t know.” In addition, participants were asked to rate the distress associated with taking their diabetes medication, using the Regimen-Related Distress domain of the Diabetes Distress Scale (DDS).Citation27
The survey was prepared in English and translated into the official language of each country from which participants were drawn. A series of iterative survey language checks among investigators, and electronic pretesting for design elements, question ordering, and survey flow, were conducted before the survey launch.
Statistical analyses
All nonresponse options were treated as missing values and coded as null. Multisite data were aggregated and cleaned in RStudio version 1.0.143, with R version 3.0.0, utilizing the packages “dplyr” and “lubridate.” Analyses were conducted using SAS Enterprise Guide version 7.13 (SAS Institute Inc., Cary, NC, USA). Descriptive statistics were generated for variables of interest.
Results
Participant demographics and characteristics
The response rate for the survey ranged from below 1% in Mexico to 39% in Canada (Table S3). In total, 661 respondents were included in the study (). There were slight differences between countries in the age of study participants, with German participants being older than American, Canadian, and Mexican participants. A slightly higher proportion of women than men participated in the study overall (53% vs 47%); the difference in proportions was most pronounced in the USA. The spread of responses for time since T2D diagnosis was similar across all countries, with most participants being diagnosed between 1 and 15 years previously. Respondents across countries typically saw a primary care physician/general practitioner for their T2D care, with other commonly seen healthcare providers (HCPs) being diabetologists for German respondents, endocrinologists for Spanish respondents, and nurse practitioners for UK respondents.
Table 1 Participant self-reported demographics and characteristics
Awareness of diabetes tests, A1C test results, and A1C targets
There was variation between countries in the routine tests that respondents reported their HCPs performed regularly (). Most respondents across countries were aware that their A1C level had been assessed in the past. Respondents from Mexico and Spain reported the lowest rates of A1C testing on a regular basis, with 18% of Mexican respondents believing that their HCP had never tested their A1C level. By contrast, almost all US respondents were aware that their A1C level had been tested, and 97% reported regular testing.
Table 2 Participant-reported diabetes tests, A1C test results, and A1C targets
Of respondents who reported having their A1C tested, the majority across countries reported that their most recent test occurred within the last 3 months (). Respondents’ ability to recall their A1C value at last test varied considerably between countries, with more respondents from the USA, Germany, and Spain providing a response than those from Canada and the UK. The mean (SD) self-reported A1C value at last test was largely consistent across countries (6.8 [1.3]–7.3 [1.6]%), with over half of respondents (57%) reporting an A1C level of at least 7.0%. Two-thirds of respondents (68% overall) reported that their last A1C test result indicated that they were doing very or fairly well.
Approximately two-thirds of North American and German respondents reported that they had an A1C target, but this proportion was only 38% for Spanish respondents and 26% for UK respondents (). Of those respondents who reported having an A1C target, the highest mean value was reported by UK respondents (6.9 [1.0]%) and the lowest was reported by Spanish respondents (6.1 [1.4]%). The A1C test result that respondents felt would make them ask their HCP to change their treatment plan ranged from a mean of 7.6 (2.1)% for UK respondents to 8.6 (1.3)% for Canadian respondents.
Perceptions of diabetes control and complications
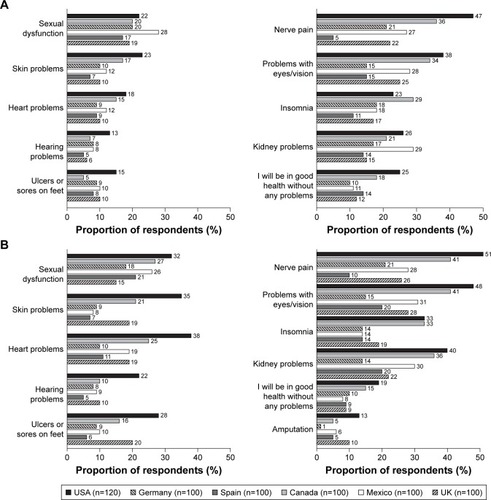
Respondents’ perceptions of their level of diabetes control were fairly consistent across countries, with approximately two-thirds (60%) of respondents, other than those in Mexico (43%), reporting that their diabetes was very well or fairly well controlled (). Spanish respondents were the most likely to indicate that, if they stayed at their current level of diabetes control, they did not expect any future diabetes-related complications (). Almost half of US and Canadian respondents expected complications within 5 years, compared with about one-quarter of respondents from the other countries. North American respondents also anticipated a higher number of different complications, both within the next year and after 5 years, than European respondents, assuming that their diabetes remained at the same level of control (). Nerve pain, eye problems, sexual dysfunction, skin problems, and kidney problems were the most common complications that respondents reported they were likely to experience.
Figure 1 Participant perceptions of diabetes control and complications (part 1).
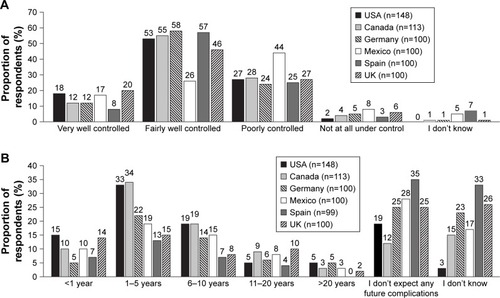
Figure 2 Participant perceptions of diabetes control and complications (part 2).
Diabetes medications and self-management
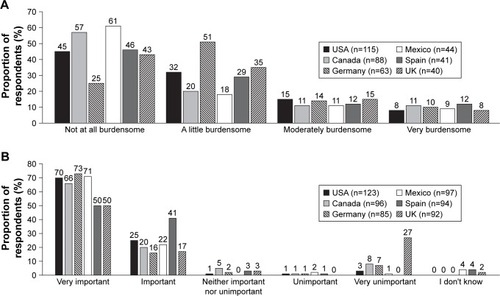
Overall, approximately two-thirds of respondents reported that they never missed medical appointments regarding their diabetes, although in Mexico this figure dropped to about half (). Participants across countries reported that they were frequently told by their doctor to take oral medications, to increase their levels of exercise, and to change their diet in order to improve their diabetes control (). Self-reported adherence to oral medication and insulin treatment was generally high, although adherence to insulin treatment appeared to be lower in the USA and Mexico than in the other countries (). The majority of respondents across countries reported that taking injectable medications was not at all burdensome or was a little burdensome (). When asked how important medications for T2D are in helping them achieve their diabetes goals, the vast majority (89%) of respondents across countries rated them as very important or important (); however, 27% of UK respondents said they were a very unimportant factor.
Figure 3 Participant behaviors relating to diabetes management.
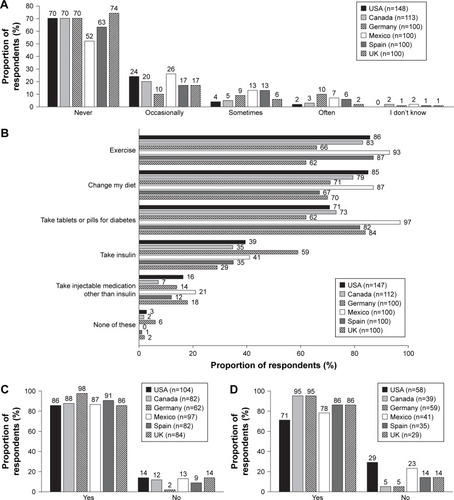
Figure 4 Participant perceptions of diabetes medications.
Regimen-related diabetes distress and attitudes toward diabetes self-management
Overall, approximately one-quarter to one-third of respondents’ scores met or exceeded the clinical threshold for the Regimen-Related Distress domain of the DDS, with the highest proportion above the threshold being Canadian respondents and the lowest being German respondents (). The majority of respondents were confident that they could avoid serious problems due to low blood sugar when alone, and did not feel that worrying about the possibility of a low blood sugar episode interfered with their ability to do the things they wanted to do (). Responses across countries were similar regarding managing blood sugar to avoid hypoglycemic episodes, with approximately one-third of patients keeping their blood sugar levels higher than they should ().
Figure 5 Participant attitudes toward diabetes self-management.
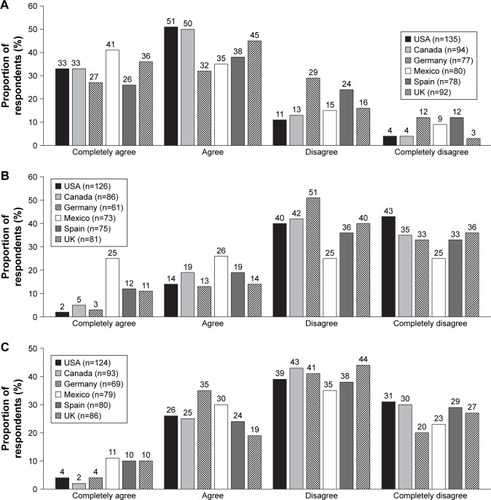
Table 3 Participant scores for the Regimen-Related Distress domain of the Diabetes Distress Scale
Discussion
Individualized A1C targets, self-monitoring of blood glucose, and adherence to treatment are key pillars of T2D management guidelines. This survey-based study of patients with T2D in online health communities revealed several insights into patients’ awareness of A1C testing and targets, their perceptions of their glycemic control, and their attitudes toward diabetes management.
Previous studies indicate that limited numbers of patients are aware of their current and target A1C levels.Citation11–Citation13 The participants in our study who were aware of having an A1C target, approximately half of the total number, generally reported targets that were in line with national guidelines,Citation3,Citation19–Citation23 with a mean A1C value of 6.1%–6.9%. However, about half of participants who reported an A1C level at last test gave a value greater than 7.0%, generally considered to be a sign of uncontrolled glycemia,Citation2,Citation3 although it should be noted that patient recollections of their last A1C test result may not be accurate.Citation11,Citation12 Participant self-reported target A1C and last A1C test results were largely consistent between countries, suggesting that any slight differences between the national guidelines do not seem to have a great impact on patients’ target and actual A1C values.
The majority of respondents across countries believed that their last test result indicated that they were doing very or fairly well, and that their diabetes was very or fairly well controlled. However, respondents did not feel that any change to their treatment plan was needed unless their A1C levels hit 7.6%–8.6% on average. This could suggest that patients may overestimate the extent of their diabetes control, considering the A1C target set by their HCP to be an ideal target only and not feeling that action is required unless their A1C is considerably higher than this. Alternatively, HCPs may consider guideline A1C targets to be an ideal, with changes to patient treatment not being required until their A1C reaches a higher threshold.
Of further concern regarding patient adherence to A1C targets is that only about half of Canadian, Spanish, and UK respondents to our survey could recall their last A1C value, and only about one-third of UK and Spanish respondents were aware that they had an A1C target. In addition, the majority of respondents in Spain and Mexico did not think that their A1C levels were tested regularly by their HCP. By contrast, almost all US respondents reported regular A1C testing, with almost 90% able to recall their last A1C value and over two-thirds aware that they had an A1C target. These findings suggest that A1C tests may be carried out more regularly in some countries than in others, which may be due to economic reasons, or that there may be variation in doctor–patient communication among these countries. In Spain and Mexico, for example, physicians may adopt a more paternalistic model of care than physicians in the USA, Canada, and northern Europe, and may therefore be less likely to communicate in detail about laboratory test results. Indeed, in a survey of patients in European countries, Spain had the lowest patient support for shared decision-making, favoring a doctor-led process;Citation28 while in Mexico, doctors are required only to give verbal (rather than written) summaries of medical records to patients.Citation29 By contrast, it has been the official policy of the US Department of Health and Human Services since 2014 to give patients direct access to their own test results;Citation30 this initiative seems to be reflected in our survey data. Our findings suggest that there is room for improvement in communication of A1C test results and targets between HCPs and patients in many countries. Patients’ awareness of their A1C levels could also be improved by increased remote monitoring feedback via mobile devices and other telehealth technologies, as well as a broader implementation of continuous glucose monitoring with long-term sensors.
Although the majority of respondents across countries (other than in Mexico) had similar perceptions of their level of glycemic control, North American respondents expected to experience more diabetes-related complications in the future than their European counterparts, especially those from Spain. This finding may be explained by cultural and regulatory differences between North America and Europe. The high prevalence of T2D and widespread advertising of diabetes medication in North America is likely to increase awareness of T2D and its consequences.Citation31 Although few respondents expected to experience serious complications in general during the next year, when asked about specific complications many did expect to experience one or more of these in this time frame, particularly microvascular issues, such as neuropathy, retinopathy, sexual dysfunction, and skin problems, rather than cardiovascular issues. There are several potential explanations for this response. It may be that patients do not perceive microvascular complications to be “serious,” as was found in a telephone-based survey of patients with diabetes in the USA,Citation32 or that microvascular outcomes are more apparent in the shorter term. Alternatively, these patients may not associate diabetes with cardiovascular issues, as has been found in previous studies.Citation32,Citation33 A recent systematic review of studies investigating the perceptions of diabetes-related complication risks in populations with T2D found that patients’ perceptions are generally biased, characterized by optimism and low risk awareness.Citation34 In line with our findings, the review found that patients were less aware of their risk of experiencing macrovascular vs micro-vascular complications. Given that half of people with T2D die prematurely from cardiovascular disease,Citation35 it appears that patients may not be realistically evaluating their personal risk of developing macrovascular complications.
Patient-reported adherence to diabetes medications in the present study was generally high, albeit somewhat lower for insulin than for oral medications among respondents in the USA and Mexico, where patients may face higher out-of-pocket costs of treatment relative to income than in other countries.Citation36,Citation37 Surprisingly, while the majority of respondents across countries believed that taking medications for T2D was an important or very important factor in achieving their diabetes goals, over one-quarter of respondents in the UK felt that it was very unimportant. This may suggest that, in comparison with their counterparts in other countries, UK physicians put more emphasis on lifestyle changes than on medication use when communicating with patients. When assessing self-management of their diabetes, respondents across countries appeared to be reasonably confident that they could adequately manage their blood sugar levels. Despite this confidence, a sizeable minority of respondents across countries had clinically significant levels of regimen-related distress. Diabetes distress has been linked with poor adherence and poor glycemic control;Citation38,Citation39 however, greater levels of HCP support can decrease diabetes distress.Citation40,Citation41 Improvement in HCP support for patients regarding their treatment, for instance by offering guidance on how often to test blood sugar levels and by providing, or referring patients to, nutrition support, may therefore reduce patient distress and improve diabetes outcomes.
Strengths and limitations
The major strength of this study is that it assessed data obtained directly from a network of patients with T2D in a real-world setting, offering context that cannot be observed in medical records. Use of an anonymous online survey may improve willingness to disclose sensitive information, such as medication nonadherence. Finally, direct access to patients through online communities enabled a potentially more diverse sample to be reached than could be reached through physicians’ offices alone.
Several limitations of this work are noted, the first being sample generalizability and selection bias. The participants were a self-selecting population of patients who were concerned enough with their disease to become members of online health communities, therefore this group may overrepresent patient knowledge of T2D compared with the general T2D population. It may be expected that respondents to online surveys are likely to be younger, more computer-literate, and better educated than the general population. In addition, more participants in this study were female than male. These factors may also impact the generalizability of results to the general population of patients with T2D. A second limitation is that, because the study utilized a convenience sample, the populations from each country were not matched for variables such as age and duration of diabetes, and so were not homogeneously distributed, which may influence the interpretation of study results. A third limitation is that the accuracy of patients’ perceptions could not be compared with their clinical data, introducing the possibility of recall bias. A fourth limitation is that participants may have had difficulties understanding the questions posed; some Mexican respondents appeared to conflate A1C and glucose levels when giving answers to A1C-based questions, providing responses that were clearly out of range for A1C tests, which led us to exclude these data. The questionnaire was not pretested in each country and we did not send a follow-up survey to assess comprehension.
Conclusion
Patients’ knowledge of their glycemic control and targets, and the potential outcomes of poor control, varied between countries. Awareness of A1C testing and targets was high in the USA but considerably lower in Spain and the UK, and North American respondents anticipated a higher number of complications than European respondents. The majority of respondents across countries felt that their T2D was very or fairly well controlled, and few expected to experience serious complications within 1 year; however, many respondents expected to experience microvascular (rather than macrovascular) complications in this time frame. Our findings highlight the need for clear communication between HCPs and patients to ensure that the latter are aware of their A1C levels and targets and to understand what is needed to achieve those targets. The potential consequences of poor glycemic control should also be communicated clearly to patients, including the possibility of macrovascular disease, of which they appear to be less aware. Furthermore, while patient self-reported adherence to medication was generally high and most respondents across countries felt that taking injectable medications was not overly burdensome, a sizeable minority still have regimen-related distress: HCPs should work with patients to support self-management, reduce distress, and improve diabetes outcomes.
Author contributions
Kristina Simacek – conception and design of the study, acquisition and interpretation of data, and drafting and revising of the manuscript. Christopher Curran – conception and design of the study, acquisition and interpretation of data, and revising of the manuscript. Peter Fenici and Ricardo Garcia-Sanchez – conception and design of the study, interpretation of data, and revising of the manuscript. All authors gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Acknowledgments
We thank all of the study participants for their time in responding to our survey. We also thank Cathy Emmas and Lynn Hagger of AstraZeneca for their contributions to this work. Medical writing support for the manuscript was provided by Richard Claes PhD of Oxford PharmaGenesis, funded by AstraZeneca. This work was supported by AstraZeneca, who provided financial sponsorship for the conduct of the study and prepa ration of the manuscript.
Disclosure
Kristina Simacek and Christopher Curran are employees of PatientsLikeMe, Inc. and hold stock options in Patients-LikeMe, Inc. They have received research funding (including conference support and consulting fees) from Abbvie, Accorda, Actelion, Alexion, Amgen, AstraZeneca, Avanir, Biogen, Boehringer Ingelheim, Celgene, EMD, Genentech, Genzyme, Janssen, Johnson & Johnson, Merck, Neuraltus, Novartis, Otsuka, Sanofi, Takeda, and UCB. They have received research grant funding from Kaiser Permanente, the Robert Wood Johnson Foundation, Sage Bionetworks, the AKU Society, and the University of Maryland. Peter Fenici and Ricardo Garcia-Sanchez are current and former employees of AstraZeneca, respectively and may own shares in AstraZeneca.
References
- World Health OrganizationGlobal Report on DiabetesGenevaWorld Health Organization2016 Available from: http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdfAccessed January 17, 2018
- International Diabetes FederationGlobal guideline for type 2Diabetes2012 Available from: https://www.idf.org/e-library/guidelines/79-global-guideline-for-type-2-diabetesAccessed January 17, 2018
- American Diabetes AssociationStandards of medical care in diabetes – 2017Diabetes Care201740Suppl 1S1S13227979885
- GarberAJAbrahamsonMJBarzilayJIAACE/ACE comprehensive diabetes management algorithm 2015Endocr Pract201521443844725877012
- QaseemAHumphreyLLSweetDEStarkeyMShekellePClinical Guidelines Committee of the American College of PhysiciansOral pharmacologic treatment of type 2 diabetes mellitus: a clinical practice guideline from the American College of PhysiciansAnn Intern Med2012156321823122312141
- KilpatrickESDasAKØrskovCBerntorpKGood glycaemic control: an international perspective on bridging the gap between theory and practice in type 2 diabetesCurr Med Res Opin20082492651266118691443
- PolinskiJMKimSCJiangDGeographic patterns in patient demographics and insulin use in 18 countries, a global perspective from the multinational observational study assessing insulin use: understanding the challenges associated with progression of therapy (MOSAIc)BMC Endocr Disord20151514626353820
- Stark CasagrandeSFradkinJESaydahSHRustKFCowieCCThe prevalence of meeting A1c, blood pressure, and LDL goals among people with diabetes, 1988–2010Diabetes Care20133682271227923418368
- StoneMACharpentierGDoggenKQuality of care of people with type 2 diabetes in eight European countries: findings from the Guideline Adherence to Enhance Care (GUIDANCE) studyDiabetes Care20133692628263823628621
- ChanJCGagliardinoJJBaikSHMultifaceted determinants for achieving glycemic control: the International Diabetes Management Practice Study (IDMPS)Diabetes Care200932222723319033410
- HarwellTSDettoriNMcdowallJMDo persons with diabetes know their (A1c) number?Diabetes Educ20022819910511852748
- TrivediHGrayLJSeiduSSelf-knowledge of HbA1c in people with type 2 diabetes mellitus and its association with glycaemic controlPrim Care Diabetes201711541442028684227
- WillaingIRogviSABøgelundMAlmdalTSchiøtzMRecall of HbA1c and self-management behaviours, patient activation, perception of care and diabetes distress in type 2 diabetesDiabet Med2013304e139e14223331258
- García-PérezLEÁlvarezMDillaTGil-GuillénVOrozco-BeltránDAdherence to therapies in patients with type 2 diabetesDiabetes Ther20134217519423990497
- PolonskyWHHenryRRPoor medication adherence in type 2 diabetes: recognizing the scope of the problem and its key contributorsPatient Prefer Adherence2016101299130727524885
- GrantRAdamsASTrinactyCMRelationship between patient medication adherence and subsequent clinical inertia in type 2 diabetes Glycemic managementDiabetes Care200730480781217259469
- ReachGPatient non-adherence and healthcare-provider inertia are clinical myopiaDiabetes Metab200834438238518706843
- International Diabetes FederationIDF Diabetes Atlas8th ed2017 Available from: http://www.diabetesatlas.orgAccessed January 17, 2018
- National Institute for Health and Care ExcellenceNICE guideline: type 2 diabetes in adults: management1222015 Available from: https://www.nice.org.uk/guidance/ng28Accessed November 14, 2018
- AWMFProgramm für Nationale VersorgungsLeitlinienTherapie des Typ-2-Diabetes. Version 42013 Available from: http://www.deutsche-diabetes-gesellschaft.de/fileadmin/Redakteur/Leitlinien/Evi-denzbasierte_Leitlinien/dm-therapie-1aufl-vers4-lang.pdfAccessed November 14, 2018
- GuiaSaludWorking group of the Clinical Practice Guideline for type 2 DiabetesClinical Practice Guideline on type 2 Diabetes52013 Available from: http://www.guiasalud.es/egpc/traduccion/ingles/diabetes/completa/index.htmlAccessed November 14, 2018
- ClínicaGuía de PrácticaDiagnóstico y Tratamiento Farmacológico de la Diabetes Mellitus Tipo 2 en el Primer Nivel de Atención. Guía de Evidencias y RecomendacionesMéxicoInstituto Mexicano del Seguro Social2018 Available from: http://www.imss.gob.mx/sites/all/statics/guiasclinicas/718GER.pdfAccessed November 14, 2018
- Diabetes Canada2018 Clinical Practice Guidelines for the Prevention and Management of Diabetes in CanadaCan J Diabetes201842Suppl 1A1A18S11S326
- LopezJMKaticBJFitz-RandolphMJacksonRAChowWMullinsCDUnderstanding preferences for type 2 diabetes mellitus self-management support through a patient-centered approach: a 2-phase mixed-methods studyBMC Endocr Disord20161614127430259
- PeyrotMRubinRRLauritzenTResistance to insulin therapy among patients and providers: results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) studyDiabetes Care200528112673267916249538
- SkeieSThueGSandbergSInterpretation of hemoglobin A(1c) (HbA(1c)) values among diabetic patients: implications for quality specifications for HbA(1c)Clin Chem20014771212121711427451
- PolonskyWHFisherLEarlesJAssessing psychosocial distress in diabetes: development of the Diabetes Distress ScaleDiabetes Care200528362663115735199
- CoulterAJenkinsonCEuropean patients’ views on the responsiveness of health systems and healthcare providersEur J Public Health200515435536015975955
- Comité Consultivo Nacional de Normalización de Regulación y Fomento SanitarioNorma Oficial Mexicana del Expediente Clínico, NOM-168-SSA1-1998 (Section 5.5)Rev Mex Patol Clin2000474245253 Available from: http://www.medigraphic.com/pdfs/patol/pt-2000/pt004g.pdfAccessed April 3, 2018
- Centers for Medicare and Medicaid Services, H. H. S.; Centers for Disease, Control and Prevention, H. H. S.; Office for Civil Rights, H. H. SCLIA program and HIPAA privacy rule; patients’ access to test reports. Final ruleFed Regist201479257289731624605389
- SinghBMPrescottJJGuyRWalfordSMurphyMWisePHEffect of advertising on awareness of symptoms of diabetes among the general public: the British Diabetic Association StudyBMJ199430869296326368148713
- MerzCNBuseJBTuncerDTwillmanGBPhysician attitudes and practices and patient awareness of the cardiovascular complications of diabetesJ Am Coll Cardiol200240101877188112446074
- O’SullivanEPBhargavaAO’CallaghanMAwareness of diabetes complications in an Irish populationIr J Med Sci2009178440140619259760
- RouyardTKentSBaskervilleRLealJGrayAPerceptions of risks for diabetes-related complications in type 2 diabetes populations: a systematic reviewDiabet Med201734446747727864886
- van DierenSBeulensJWvan der SchouwYTGrobbeeDENealBThe global burden of diabetes and its complications: an emerging pandemicEur J Cardiovasc Prev Rehabil201017Suppl 1S3S820489418
- ArredondoABarcelóAThe economic burden of out-of-pocket medical expenditures for patients seeking diabetes care in MexicoDiabetologia200750112408240917879080
- SeuringTArchangelidiOSuhrckeMThe economic costs of type 2 diabetes: a global systematic reviewPharmacoeconomics201533881183125787932
- PanditAUBaileySCCurtisLMDisease-related distress, self-care and clinical outcomes among low-income patients with diabetesJ Epidemiol Community Health201468655756424489044
- van BastelaarKMPPouwerFGeelhoed-DuijvestijnPHLMDiabetes-specific emotional distress mediates the association between depressive symptoms and glycaemic control in Type 1 and Type 2 diabetesDiabet Med201027779880320636961
- WardianJSunFFactors associated with diabetes-related distress: implications for diabetes self-managementSoc Work Health Care201453436438124717184
- DelahantyLMGrantRWWittenbergEAssociation of diabetes-related emotional distress with diabetes treatment in primary care patients with type 2 diabetesDiabet Med2007241485417227324