
Abstract
Missed care, defined as any aspect of patient care that is omitted or delayed, is receiving increasing attention. It is primarily caused by the imbalance between patients’ nursing care needs and the resources available, making it an ethical issue that challenges nurses’ professional and moral values. In this scoping review, conducted using the five-stage approach by Arksey and O’Malley, our aim is to analyze the patients’ perspective to missed care, as the topic has been mainly examined from nurses’ perspective. The search was conducted in April 2019 in PubMed, CINAHL, PsycINFO, Web of Science, ProQuest and Philosophers Index databases using the following terms: omitted care, unfinished nursing care, care undone, care unfinished, missed care, care left undone, task undone and implicit rationing with no time limitation. The English-language studies where missed care was examined in the nursing context and had patients as informants on patient-reported missed care or patients’ perceptions on nurse-reported missed care were selected for the review. Thirteen studies were included and analyzed with thematic content analysis. Twelve studies were quantitative in nature. Patients were able to report missed care, and mostly reported missed basic care, followed by missed communication with staff and problems with timeliness when they had to wait to get the help they needed. In statistical analysis, missed care was associated with patient-reported adverse events and patients’ perceptions of staffing adequacy, and in patients’ perception, it was mainly caused by lack of staff and insufficient experience. Furthermore, patients’ health status, as opposed to gender, predicted missed care. The results concerning patients’ age and education level were conflicting. Patients are able to identify missed care. However, further research is needed to examine patient-perceived missed care as well as to examine how patients identify missed care, and to get a clear definition of missed care.
Introduction
Literature related to missed care has increased over the last decade,Citation1 providing evidence of its prevalence and the threat it poses.Citation2,Citation3 The primary cause of missed care seem to be limited nursing resources.Citation4 Missed care is an international problem as most nurses report at least one task left undone in a shift, based on an international review.Citation3 However, little is known about patients’ views on this timely topic. Patients’ perspective in this review is viewed as patients’ personal perception about missed care as well as patients’ perception of their care environment where care is missed based on nurses’ reports. Missed care has been associated with decreased nurse-reported care quality, job satisfaction and patient satisfaction, as well as increased adverse events, turnover and intent to leave.Citation3 Furthermore, an association has been found between missed care and nursing work environment and patient safety culture.Citation5 Predictors of missed care include nurse’s shift type, resource allocation, health professional communication and workload intensity, and predictability.Citation6 Therefore, the worldwide prediction of a nurse shortage underlines the importance to understand the phenomenon.Citation7
The terminology referring to missed care varies in literature, as some studies view missed care as an implicit rationing of nursing care, referring to nurses’ bedside decision-making, leading to failure to carry out all needed nursing interventions because of inadequate resources.Citation8 In addition, the terms care left undone,Citation9,Citation10 nursing task left undone,Citation11 task incompletionCitation12, and unmet nursing care needsCitation13 have been used. The first report on this topic was from the International Hospital Outcomes Research (IHORC), using the term nursing care left undone.Citation9 The term missed care was first used in 2006 by Kalisch in her identification of nine elements of regularly missed nursing care and the reasons for them.Citation14
Missed care occurs when any aspect of required patient care is omitted (in part or whole) or delayed,Citation15 including all aspects of clinical, emotional and administrative nursing care.Citation3 There are some conceptualization of missed careCitation16 including the Missed Nursing Care Model, which is a middle-range theory developed by Kalisch (2009).Citation15 This model identifies external antecedents for missed care, such as resources and communication and relationships among staff, that have an effect on the nursing process. If nurses lack resources, they must prioritize how to best use the resources available. This decision-making interacts with the internal processes of nurses (including staff norms, the prioritization of the care, personal values and behavior). All these factors contribute to missed care, which has adverse outcomes for patients. The model identifies organizational characteristics as factors that facilitate or constrain nurses’ practice.Citation15 Another conceptual model, Implicit Rationing developed by Schubert (2007), is mainly used with cost reduction and the allocation of inadequate resources. This model also recognizes nurses as decision-makers, as they must prioritize, and acknowledges both individual and organizational factors contributing to rationing of nursing care. The number of omitted nursing activities measures the extent of the rationing and is an important indicator of the quality of care.Citation8 The conceptual framework of The Task Undone was originally described by Lucero et al (2009) using the Process of Care and Outcome model. In this model, the necessary care activities that are left undone reflect the quality of provided nursing care as they have negative outcomes for patients.Citation17
Missed care is associated with patient safety culture,Citation5 which has been examined in different theoretical frameworks. Groves et alCitation18 recommend structuration theory of safety culture, which is a middle-range theory that is widely used to examine different organizational topics. It views safety culture as a system that involves individual actions as well as organizational structures. Nurses share values regarding patient safety and enact them in their practice. Organizational structures, such as resources and rules, both enable and constrain nurses’ action to keep patients safe.Citation18 This model could also be adapted to examine missed care. However, there is currently a lack of a theoretical framework and common terminology to describe missed care as it remains unclear whether an understanding exists about how it occurs or whether the causation and response to missed care are similar across different health-care environments; development of a theoretical framework to describe and understand missed care is thus highly needed.Citation19
Missed care is an ethical issue challenging nurses’ professional and moral values, consequently leading to imbalance between patients’ needs and available and/or scarce resources. Therefore, nurses need to prioritize their work, and missed care is an outcome of this prioritization process.Citation20 Missed care is an error of omission, meaning failure to do the right thing, which potentially leads to adverse outcomes to patients, impacting the quality of care negatively. Higher missed care has been associated with a greater risk of patient falls, while missed ambulation can cause pressure ulcers, pneumonia, delayed wound healing, and increased pain and suffering.Citation21 Thus, missed care has been associated with lower patient safety.Citation22,Citation23
The research emphasis of this topic has mainly been on nurses’ perspectiveCitation3,Citation10 Thus, the aim of this scoping review is to analyze the patients’ perspective to missed care as it has not received adequate research interest. Today, patients are recognized as partners in health care and experts on their situation, working alongside professionals, with their own rights as well as responsibilities.Citation24 This view is associated with the empowerment philosophy to health, which aims to increase patient autonomy and freedom of choice, encouraging patients to oversee their own health values, needs and goals.Citation25 Therefore, patients should be involved in the discussion about the requirements of nursing care and the prioritization process where nurses are unable to respond to patients’ needs.Citation20 This paper adds to the existing literature by examining how patients’ perceptions on missed care have been examined, how patients are able to identify missed care, what care has been mostly identified as missing by patients, and how patients experience the received care when nurses report missed care. In this review, the term missed care expresses patients’ perception that something is missing, delayed or not done during their health-care treatment. The goal of the analysis is to deepen our understanding of the concept of missed care and to provide a basis for further studies in the field.
Materials and Methods
This scoping review was conducted using the five-stage approach by Arksey and O’Malley (2006).Citation26 In the next paragraph, the five stages of analysis are described in more detail.
Stage 1: Identifying the Research Question
The following research questions were identified to guide the scoping review:
How have patients’ perceptions of missed care been studied?
What instruments were used to measure patients’ perceptions on missed care?
What were the main findings of the studies?
What are the implications and suggestions for further research in the studies?
Stage 2: Identifying Relevant Studies
Six electronic databases (PubMed, CINAHL, PsycINFO, Web of Science, ProQuest/Scholarly Journals and Philosophers Index) were searched in April 2019 using the terms omitted care, unfinished care, care undone, care unfinished, missed care, care left undone, task undone and implicit rationing. No time limitation was used in the search. The search phrases, chosen in collaboration with the university library information specialist, followed the guidelines of each database. In addition to the systematic database search, a manual search of the reference lists of the included articles as well as scanning through Google Scholar and Academic Search Premier databases was conducted; however, no new articles were identified. In total, the search produced 2145 hits ().
Stage 3: Study Selection
Study selection started by determining the inclusion criteria for the articles.Citation26 After the search was conducted, two research approaches in studies of missed nursing care from the patient perspective were identified. The first approach used validated instruments for measurement of missed nursing care from the patient perspective. The second used validated instruments to measure missed nursing care from the nurse’s perspective, linking it to patient data. In these studies, mostly patient satisfaction was measured. These studies have proven that patient satisfaction is linked to missed nursing care from the nurses’ perspective.Citation27 Therefore, it is important to include these studies in this review because they give us important answers of patients’ perspective of their care in an environment where nurses report missed care. Hence, articles were eligible for inclusion if they: 1. Examined missed care in the nursing context; 2. Had patients as participants to provide full or partial data, so that at least some data were collected from patients (patient-reported missed care or patients’ perceptions on nurse-reported missed care); and 3. Were empirical study reports in English. Studies conducted solely from the nurses’ perspective were excluded. Records were first screened by title and afterwards by abstract, leading to exclusion of 1994 articles. Full-text articles (n=18) were finally read among those that were selected based on abstract. Finally, 13 articles were included in the analysis ().
Figure 1 Flowchart on the article selection process.
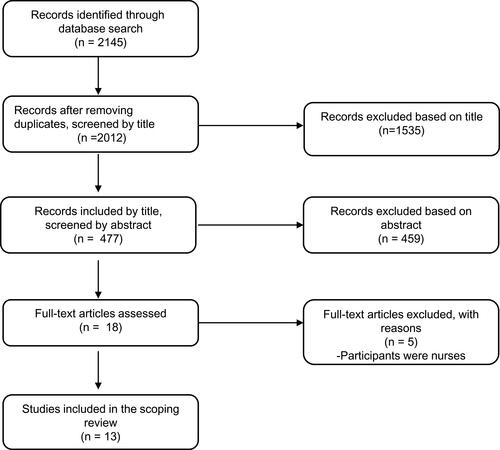
Table 1 Articles Included in the Analysis
Stage 4: Charting the Data
The data chart () included the following topics: Authors, Publication year, Country, Purpose, Methods and Sample, Instruments, Main Results, Validity/Reliability, and Implications for Further Research. These variables were central in answering the research questions.
Stage 5: Collating, Summarizing and Reporting the Results
Stage five included descriptive numerical summary analysis as well as thematic analysis. Descriptive numerical summary included basic numerical analysis of the extent and nature of the included studies.Citation26,Citation28 Thematic analysis in scoping review resembles qualitative data analysis; researchers may thus consider using qualitative content analytical techniques. Therefore, the data were analyzed with content analysis, where it was organized thematically and presented according to the research questions.Citation28 Themes were not preconceived but emerged inductively from the included articles,Citation29 as scoping review does not seek to synthesize evidence on a particular topic, but rather, to describe the account of available research.Citation26,Citation28 The PRISMA-Sco checklist for scoping review was used to guide the reporting of the results.Citation30
Results
Studies Involving Patients’ Perceptions About Missed Care
Description of Studies and Methods Used
The included studies (n=13), published between 2008 and 2018, were from the USA (n=5), Switzerland (n=3), South Korea (n=1), Cyprus (n=1), Mexico (n=1), and the UK (n=1), and one combined data from eight countries (n=1, ).
The data included one qualitative study using phenomenological approach with data collected using in-depth, semi-structured interviews of 38 patients.Citation31 Other studies (n=12) were quantitative in nature. Five studies inquired about missed nursing care directly from the patients. Sample sizes in these varied between 160 and 1555.Citation32–Citation36 Seven studies collected data about patients’ satisfaction with care and compared it to missed care data collected from nurses. The sample size in these varied between 352 and 66,348 patientsCitation27,Citation37–Citation42 Quantitative studies (n=12) were descriptive cross-sectional studies using structured questionnaires and statistical analysis.
All participants were adults and the studies were conducted in different clinical hospital settings: medical (n=11), surgical (n=11), rehabilitation unit (n=2), mixed unit (n=1), intensive care unit (n=1), gynecological unit (n=2), and maternity care (n=1).
Instruments Used to Measure Patients’ Perceptions on Missed Care
In the included studies, three different instruments were used to examine patients’ perceptions on missed care: the MISSCARE Survey – Patient,Citation32–Citation34 MISSCARE Survey,Citation35 and Hospital Consumer Assessment of Health Providers and Systems survey (also known as the HCAHPS®).Citation36
The MISSCARE Survey – Patient, developed by Kalisch (2014), was used in three studies.Citation32–Citation34 In these studies, patients were asked to identify whether nursing care was provided during their hospitalization. This instrument contains three sections: 1. Demographic characteristics and health status (including patient age, sex, race, education, marital status, hospitalized days, health status, diagnosis, and disease history), 2. Elements of nursing care, and 3. Adverse events. The section of elements of nursing care contains 13 items and uses 5-point Likert-type scales for measurement of communication and basic care (1 = never, 2 = rarely, 3 = sometimes, 4 = usually, and 5 = always) and for measurement of timeliness (from 1 to 30 mins). The mean of all 13 items is used as a total score for the scale, and the potential range of scores is 1 to 5.Citation32–Citation34
The MISSCARE survey, originally developed to measure missed nursing care and the reasons for it from nurses’ perspective, was used to measure patients’ perspective of missed care in one study.Citation35 It contains two parts. Part A consists of 24 listed elements of nursing care. Nurses are asked to indicate how frequently each nursing care element was missed in their unit by all staff, including themselves, using the scale “rarely”, “occasionally”, “frequently”, “always”, or non-applicable. Part B consists of 17 reasons listed for missed care. Nurses are asked to rate each item using the scale “significant factor”, “moderate factor”, “minor factor”, or “not a reason for unmet nursing care”. In addition, demographic/background data contain characteristics of the respondent’s gender, years of working experience, highest nursing degree, current employment status and unit.Citation35
One study used the HCAHPS survey,Citation36 which was originally developed for measuring patients’ perceptions of their hospital experienceCitation41 and includes 32 items consisting of nine-key domains pertaining to patient care. The survey has items that ask whether and at what frequency patients experienced a critical aspect of hospital care, rather than whether they were satisfied with their care. The survey also includes four screener items directing patients to relevant questions, five items to adjust for the mix of patients across hospitals, and two items supporting Congressionally-mandated reports.Citation36
The Main Findings of the Studies
Missed Care Reported by Patients
Patients can recognize and report several aspects of missed care.Citation31 MISSCARE Survey – Patient divides missed care into three domains: missed basic care, missed communication, and timeliness. In studies using this questionnaire,Citation32–Citation34 patients (n=210-729) reported mostly missed basic care (mean 2.29–3.57, SD 1.06–1.23), followed by missed communication (mean 1.69–2.02, SD 0.71–0.83) and timeliness (mean 1.29–1.52, SD 0.54–0.64).Citation32–Citation34
MISSCARE Survey – Patient views missed care as unperformed nursing activities. To begin with missed basic care, mouth care (missed 32.1–50.3% of the time), ambulation (missed 20.3–41.3% of the time), lifting to a chair (missed 38.8% of time), bathing (missed 26.9% of time), assistance with hand washing (missed 29.4% of time) and support for chancing position (missed 17% of time) were recognized as missed.Citation32 Moreover, activities categorized as missed communication included nurses providing necessary information to patients and families (missed 11.9–27% of the time), discussing the treatment plan with patients (missed 26.5% of time), considering patient’s opinions (missed 20.4% of time), patient knowing who their assigned nurse was (missed 11.2% of time), and listening to patient (missed 7.8% of time).Citation32 Finally, activities related to timeliness were listed, including timely help to the bathroom (missed 10.1–10.9% of the time), fulfilling call light requests (missed 10.3–16.4% of time) and responding to beeping monitors (missed 8.8% of time) as well as call lights (missed 8.6% of time).Citation32
In the study using MISSCARE Survey,Citation35 patients (n=160) also mostly reported missed basic care, followed by missed individual needs, which included activities such as emotional support for the patient or family (reported as missing by 43.7% of patients), visits for assessments by other professional such as physician or nutritionist (reported as missing by 26.2% of patients), and evaluating the effectiveness of drugs (reported as missing by 16.7% of patients), as well as patient education during hospitalization (reported as missing by 36% of patients) and discharge plan (reported as missing by 73.7% of patients).Citation35 Furthermore, one-third (38%) of the patients (n=1125) reported at least one nursing activity from the HCAHPS survey as missed during their hospital stay.Citation36
Factors Associated with Missed Care
Several patient-related and staff-related factors were associated with missed care. Among patient-related factors, patients with poorer health status and patients with mental health problems reported more missed care,Citation32,Citation36 as did patients who experienced adverse events during hospitalization compared to those who did not; a significant positive association was thus found between patient-reported missed care and patient-reported skin breakdown, medication error, new infection, intravenous infusion (IV) running dry and IV leaking.Citation32 Dabney & Kalisch (2015) found patients’ older age to be a predictor of missed timeliness,Citation33 as opposed to Orique et al (2107).Citation36 Similarly, Kalisch et al (2014) found that patients with lower education level reported more missed care,Citation32 whereas Orique et al (2017) found no significant association between patient’s education level and missed care.Citation36 Patient’s gender did not predict missed care.Citation32,Citation36
Staff-related factors contributing to missed care perceived by patients (n=160) included lack of staff (18.1%), staff with insufficient experience (13.8%), lack of teamwork (7.5%), lack of staff communication between shifts and the attitude of staff members (5%).Citation35
Patient-reported missed care was also associated with nurse staffing levels. The total number of productive hours worked by registered nurses, total number of productive hours worked by all nursing staff members, and the proportion of registered nurses in the total number of nursing staff members had a significant negative correlation with missed patient reported timeliness as opposed to patient-reported missed basic care or communication.Citation33 However, in another studyCitation34 the actual patient-to-nurse ratio was not significantly associated with patient-reported missed care while patients’ perceptions of staffing adequacy had a significant positive association with patient-reported missed communication and patient-reported missed basic care. Nurse-perceived staffing adequacy had a significant inverse relationship with patient-reported missed communication but no significant relationship with patient-reported missed basic care.Citation34
Patients’ Satisfaction
Missed care was also connected with the outcomes of care, the outcome mostly being patient satisfaction. In the studies reviewed, patient-reported satisfaction with the nurses’ care showed a significant negative association with nurse-reported missed care.Citation27,Citation37–Citation41 Even low levels of nurse-reported missed care associated significantly with low patient satisfaction.Citation40 Furthermore, a significant negative association was found between nurse-reported missed care and patients rating their care as excellent,Citation37 as well as between nurse-reported missed care and patient-reported patient-centered care.Citation42
Implications and Suggestions for Further Research in the Studies
In most of the studies, the authors reported suggestions for further studies. There is variation in this as well. Suggestions for future research referring to patients’ perspective of missed care are limited. Authors agree that data should be collected from both nursing staff and patients, which would permit comparison of the reports of missed nursing care.Citation33 Future research is also needed to explore the effect of engaging patients and families more extensively in their nursing care,Citation32 and to study the expectations of patients regarding professional hospital care.Citation39
Discussion
Patients’ perspective in missed care literature is very limited, as studies were only included in the review if they had patients providing missed care data or examined patients’ perceptions of nurse-reported missed care and yet, in the search with no time limit, only 13 studies, published 2008–2018, were identified. The selected studies included mostly data about patients’ satisfaction compared to nurse-reported missed care whereas direct information on patients’ perceptions on missed care is extremely scarce: only six studies included these data.
Research on this field has mainly focused on the amount and nature of missed care as tasks experienced by patients and the factors associated with it whereas no causal conclusions can be made about these relationships. In the reviewed studies, patients mostly reported missed basic care, followed by missed communication and missed timeliness.Citation32–Citation34 The studies are from several countries and the results on the amount of missed care experienced by patients are similar, potentially indicating an international problem. The estimation of a shortage of two million nurses by 2030Citation7 suggests an increasing amount of missed care requiring attention since patient-reported missed care is associated with patient-reported adverse events during hospitalization.Citation32
Some patient- and nurse-related background factors were associated with missed care. However, the results about patients’ education level and age as predictors of missed care were conflicting,Citation32,Citation36 as were the results about an association between staffing level and missed care, highlighting the need for further research. The determination of staffing level varies between studies, making it more difficult to combine these results. Cho et al (2017) used patient-to-nurse ratio (the average number of patients at midnight over the past 7 days divided by the average number of nurses per shift) to determine staffing level, and this was not significantly associated with patient-reported missed care,Citation34 whereas Dabney & Kalisch (2015) used three variables to measure nurse staffing: RNHPPD (the total number of productive hours worked by RNs in a designated inpatient unit during a specific calendar month, divided by the total number of patient days for the corresponding unit and month), NHPPD (total number of productive hours worked by all nursing staff members in an inpatient unit during a designated calendar month, divided by the total number of patient-days for the corresponding unit and month), and RN SKILL MIX (the proportion of RNs in the total number of nursing staff members). These variables were not associated with patient-reported communication and basic care, as opposed to missed timeliness,Citation33 which runs counter to previous studies that highlight the association between lower staff levels and increased amount of missed care.Citation1,Citation21 Nurse-reported missed care was significantly associated with patients’ satisfaction with care, potentially indicating the mediating effects of missed care on the relationship between nurse staffing and patients’ experiences.Citation34
Patient-perceived staffing adequacy was, however, significantly associated with patient-reported missed care, and lack of staff was named as the primary factor contributing to missed care perceived by patients, which raises the questions of how patients recognize missed care and how patients perceive staffing adequacy. Patients may not be able to separate nurses from other health-care professionals or they may not recognize care needs with the same scope as professionals; in addition, each patient also has their individual expectations for nursing care. Among the studies reviewed, different questionnaires were used to measure missed care perceived by patients. The questionnaires included different numbers of listed nursing care tasks, and patients were asked whether or not this task was performed during their hospitalization. This, however, does not say what is important to patients or what nursing care they and their family members value the most; further research would thus be useful to examine how patients identify missed care, what activities they consider that nurses perform, and how they define care that is completed in correspondence with their views on their care needs.
These results support the conceptual models developed to understand missed care, as there were organization-related factors, such as resources and lack of teamwork, identified as contributors to missed care perceived by patients. Moreover, missed care was associated with adverse events and lower patient satisfaction, thus resulting in negative patient outcomes, which could be an indicator of care quality. In these conceptual models, nurses are decision-makers who, in situations that require prioritization, make a choice about what activities to perform and what to leave out. In addition to conceptual models, these results could also be viewed through the framework of structuration theory.Citation15,Citation17 In this framework, nurses would be acknowledged as agents who, based on their education and experience, have knowledge about the necessary nursing activities they should provide, and are able to reflect upon how they carry out these activities. Nurses as agents must also make choices on whether or not to perform a specific task. Nurses carry out their work intentionally, based on their knowledge and the expected outcomes of these activities to patients or themselves. In addition to personal choices, nurses practice their work in a specific social environment and structural system which, for example, provides the resources available.Citation18 Based on these results, basic care was mostly missed; this would indicate that nurses mostly decide that the expected outcome of missed basic care would not be as severe as that of some other nursing activities. However, based on these articles reviewed, no conclusions can be drawn about nurses’ decision process.
The imbalance between patients’ care needs and the resources available forces nurses to prioritize between patients and different nursing tasks, making it an ethical challenge.Citation20 Prioritization has consequences for nurses as well as patients as it may cause nurses to experience moral distress as well as feelings of frustration and powerlessness. The consequences for patients include missed care, dissatisfaction and loss of trust,Citation43 as the prioritization process leaves patients vulnerable to unmet care needs.Citation3 However, the ethical perspective on missed care was not adduced in the reviewed articles, and further research is needed on this topic.
This study has strengths and limitations. The strengths include that the search was comprehensive, using six databases, and conducted in collaboration with an information specialist. In addition, the PRISMA-ScR checklist for scoping reviews was used to guide the reporting of the results.Citation30 The limitation is that only English-language articles were included in the review, and it is therefore possible that relevant articles in languages other than English were left out. However, the studies in the selected articles were conducted internationally in different countries and cultures. The term “patient perspective” was left out of the search phrases because of possible difficulties of including all the terms describing it, as a result of which something relevant might be left out. Even without this, it was possible to go through all the found articles by title.
Further research is needed to form a clear definition of missed care and to state what the definition includes, as it is challenging to examine something that does not exist. In addition, further research is needed to gain a deeper understanding of missed care as perceived by patients and the factors influencing it, including different organizational structures, as the literature on this topic is limited and the existing results were partly conflicting. Based on this review, it is not possible to identify a specific nursing context that encloses missed care, which is why future research is needed within a variety of patient groups and health-care contexts, as so far, all the participants have been adult patients in clinical hospital setting. Missed care has been investigated in aged care from the nurses’ perspective, and one study showed that additional unplanned careCitation44 was most frequently missed, whereas basic care was mostly missed among the medical patients in the studies reviewed. As populations age in many parts of the world, prioritization might also increase in older people care in the future.Citation45 Furthermore, in the future it would be useful to examine how patients identify missed care and to explore the ethical perspective on missed care, as it was not addressed in the articles reviewed.
Conclusion
Research about missed care from patients’ perspective is scarce, although anticipated to be an extremely common phenomenon. Patients mostly report missed basic care, followed by missed communication and timeliness. The included articles pointed out that researchers can investigate patient’s perspective of missed nursing care using validated instruments; however, we suggest also asking patients’ views more broadly. In addition, patients’ perception on some of the missing nursing tasks and areas had strong correspondence with previously studied nurses’ perception. However, since identification of missed care is not simple, it presents, and will continue to present, a great challenge for researchers, clinicians and patients.
Acknowledgments
The authors would like to thank Anna Vuolteenaho for the language check of this article.
Disclosure
The authors report no conflicts of interest in this work.
References
- Griffiths P, Recio-Saucedo A, Dall’Ora C, et al. The association between nurse staffing and omissions in nursing care: a systematic review. J Adv Nurs. 2018;74:1474–1487. doi:10.1111/jan.13564
- Recio-Saucedo A, Dall’Ora C, Maruotti A, et al. What impact does nursing care left undone have on patient outcomes? Review of the Literature. J Clin Nurs. 2018;27:2248–2259. doi:10.1111/jocn.14058
- Jones T, Hamilton P, Murry N. Unfinished nursing care, missed care, and implicitly rationed care: state of the science review. Int J NursStud. 2015;52:1121–1137. doi:10.1016/j.ijnurstu.2015.02.012
- Schubert M, Ausserhofer D, Desmedt M, et al. Levels and correlates of implicit rationing of nursing care in Swiss acute care hospitals e a cross sectional study. Int J Nurs Stud. 2013;50(2):230–239. doi:10.1016/j.inurstu.2012.09.016
- Kim KJ, Yoo MS, Seo EJ. Exploring the influence of nursing work environment and patient safety culture on missed nursing care in Korea. Asian Nurs Res. 2018;12:121–126. doi:10.1016/j.anr.2018.04.003
- Blackman I, Henderson J, Willis E, et al. Factors influencing why nursing care is missed. J Clin Nurs. 2014;24:47–56. doi:10.1111/jocn.12688
- Drennan V, Ross F. Global nurse shortages-the facts, the impact and action for change. Br Med Bull. 2019;1–13. doi:10.1093/bmb/ldz014
- Schubert M, Glass T, Clarke S, et al. Validation of the Basel extent of rationing of nursing care instrument. Nurs Res. 2007;56(6):416–424. doi:10.1097/01.NNR.0000299853.52429.62
- Aiken L, Clarke S, Sloane D, et al. Nurses’ reports on hospital care in five countries. Health Affairs. 2001;20(3):43–53. doi:10.1377/hlthaff.20.3.43
- Ausserhofer D, Zander B, Busse R, et al. Prevalence, patterns and predictors of nursing care left undone in European hospitals: results from the multicountry cross-sectional RN4CAST study. BMJ Qual Saf. 2014;23(2):126–135. doi:10.1136/bmjqs-2013-002318
- Sochalski J. Is more better? The relationship between nurse staffing and the quality of nursing care in hospitals. Med Care. 2004;42(2):II67–II73. doi:10.1097/01.mlr.0000109127.76128.aa
- Al-Kandari F, Thomas D. Factors contributing to nursing task incompletion as perceived by nurses working in Kuwait general hospitals. J Clin Nurs. 2009;18(24):3430–3440. doi:10.1111/j.1365-2702.2009.02795.x
- Lucero R, Lake E, Aiken L. Nursing care quality and adverse events in US hospitals. J Clin Nurs. 2010;19(15–16):2185–2195. doi:10.1111/j.1365-2702.2010.03250.x
- Kalisch B. Missed nursing care: a qualitative study. J Nurs Care Qual. 2006;14(4):306–313. doi:10.1097/00001786-200610000-00006
- Kalisch B, Landstrom G, Hinshaw A. Missed nursing care: a concept analysis. J Adv Nurs. 2009;65(7):1509–1517. doi:10.1111/j.1365-2648.2009.05027.x
- Kalánková D, Zianková K, Kurucová R. Approaches to understanding the phenomenon of missed/rationed/unfinished care – a literature review. Central Eur J Nurs Midwifery. 2019;10(1):1005–1016. doi:10.15452/CEJNM.2019.10.0007
- Lucero RJ, Lake ET, Aiken LH. Variations in nursing care quality across hospitals. J Adv Nurs. 2009;65(11):2299–2310. doi:10.1111/j.1365-2648.2009.05090.x
- Groves PS, Meisenbach RJ, Scott-Cawiezell J. Keeping patients safe in healthcare organizations: a structuration theory of safety culture. J Adv Nurs. 2019;76(8):1846–1855. doi:10.1111/j.1365-2648.2011.05619.x
- Jones T, Willis E, Amorim-Lopes M, Drach-Zahavy A. Advancing the science of unfinished nursing care: exploring the benefits of cross-disciplinary exchange, knowledge integration and transdisciplinarity. J Adv Nurs. 2019;75:905–917. doi:10.1111/jan.13948
- Suhonen R, Scott A. Missed care: a need for careful ethical discussion. Nurs Ethics. 2018;25(5):458–551. doi:10.1177/0969733018790837
- Kalisch B, Xie B. Errors of omission: missed nursing care. Western J Nurs Res. 2014;36(7):875–890. doi:10.1177/0193945914531859
- Cho S-H, You SJ, Song KJ, Hong KJ. Nurse staffing, nurses prioritization, missed care, quality of nursing care, and nurse outcomes. Int J Nurs Pract. 2019;e12803. doi:10.1111/ijn.12803
- Hessels AJ, Wurmser T. Relationship among safety culture, nursing care and Standard Precautions adherence. Am J Infect Control. 2019. doi:10.1016/j.ajic.2019.11.008
- Coulter A. Paternalism or partnership? Patients have grown up- and there’s no going back. Br Med J. 1999;319:719–720. doi:10.1136/bmj.319.7212.719
- Feste C, Anderson RM. Empowerment: from philosophy to practice. Patient Educ Counsel. 1995;26:139–144. doi:10.1016/0738-3991(95)00730-N
- Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol. 2005;8(1):19–32. doi:10.1080/1364557032000119616
- Lake E, Germack H, Viscardi M. Missed nursing care is linked to patient satisfaction: a cross-sectional study of US hospitals. BMJ Qual Saf. 2016;25:535–543. doi:10.1136/bmjqs-2015-003961
- Levac D, Colquhoun H, O’Brien KK. Scoping studies: advancing the methodology. Implementation Science. 2010;5(69). doi:10.1186/1748-5908-5-69
- Kastner N, Tricco A, Soobiah C, et al. What is the most appropriate knowledge synthesis method to conduct a review? Protocol for a scoping review. BMC Med Res Methodol. 2012;12(144). doi:10.1186/1471-2288-12-114
- Tricco A, Lillie E, Zarin W, et al. PRISMA extension for Scoping Reviews (PRISMA.ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/M18-0850
- Kalisch B, McLaughlin M, Dabney B. Patient perceptions of missed nursing care. Jt Comm J Qual Patient Saf. 2012;38(4):161–167. doi:10.1016/S1553-7250(12)38021-5
- Kalisch B, Xie B, Dabney B. Patient-reported missed nursing care correlated with adverse events. Am J Med Qual. 2014;29(5):415–422. doi:10.1177/1062860613501715
- Dabney B, Kalisch B. Nurse staffing levels and patient-reported missed nursing care. J Nurs Care Qual. 2015;30(4):306–312. doi:10.1097/NCQ.0000000000000123
- Cho S, Mark B, Knafl G, et al. Relationships between nurse staffing and patients’ experiences, and the mediating effects of missed nursing care. J Nurs Scholarship. 2017;49(3):347–355. doi:10.1111/jnu.12292
- Moreno-Monsiváis M, Moreno-Rodríguez C, Interial-Guzmán MG. Missed nursing care in hospitalized patients. Aquichan. 2015;15(3):318–328. doi:10.5294/aqui.2015.15.3.2
- Orique S, Patty C, Sandidge A, et al. Quantifying missed nursing care using the hospital consumer assessment of healthcare providers and systems (HCAHPS) survey. J Nurs Admin. 2017;47(12):616–662. doi:10.1097/NNA.0000000000000556
- Shubert M, Glass T, Clarke S, et al. Rationing of nursing care and its relationship to patient outcomes: the Swiss extension of the International Hospital Outcomes Study. Int J Qual Health Care. 2008;20(4):227–237. doi:10.1093/intqhc/mzn017
- Schubert M, Clarke S, Glass T, et al. Identifying thresholds for relationships between impacts of rationing of nursing care and nurse- and patients-reported outcomes on Swiss hospitals: A correlational study. Int J Nurs Stud. 2009;46(7):884–893. doi:10.1016/j.inurstu.2008.10.008
- Bruyneel L, Li B, Ausserhofer D, et al. Organization of hospital nursing, provision of nursing care, and patient experiences with care in europe. Med Care Res Rev. 2015;72(6):643–664. doi:10.1177/1077558715589188
- Papastavrou E, Andreou P, Tsangari H, et al. Linking patient satisfaction with nursing care: the case of care rationing – a correlational study. BMC Nurs. 2014;13:26. doi:10.1186/1472-6955-13-26
- Aiken L, Sloane D, Ball J, et al. Patient satisfaction with hospital care and nurses in England: an observational study. BMJ Open. 2018;8. doi:10.1136/bmjopen-2017-019189
- Bachnick S, Ausserhofer D, Baernholdt M, et al. Patient-centered care, nurse work environment and implicit rationing of nursing care in Swiss acute care hospitals: A cross-sectional multi-centered study. Int J Nurs Stud. 2018;81:98–106. doi:10.1016/j.inurstu.2017.11.007
- Suhonen R, Stolt M, Habermann M, et al. Ethical elements in priority setting in nursing care: A scoping review. Int J Nurs Stud. 2018;88:25–42. doi:10.1016/j.nurstu.2018.08.006
- Henderson J, Willis E, Xiao L, et al. Missed care in residential aged care in Australia: an exploratory study. Collegian. 2017;24:411–416. doi:10.1016/j.colegn.2016.09.001
- Amalberti R, Vincent C, Nicklin W, et al. Coping with more people with more illness. Part 1: the nature of the challenge and the implications for safety and quality. Int J Qual Health Care. 2019;31(2):154–158. doi:10.1093/intqhc/mzy235