 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
The impact of fixed-dose combination (FDC) products on adherence to other, non-fixed regimen components has not been examined. We compared adherence to a third antiretroviral (ART) component among patients receiving a nucleoside reverse transcriptase inhibitor (NRTI) backbone consisting of the FDC Epzicom®, GlaxoSmithKline Inc, Research Triangle Park, NC (abacavir sulfate 600 mg + lamivudine 300 mg; FDC group) versus NRTI combinations taken as two separate pills (NRTI Combo group) using data from a national sample of 30 health plans covering approximately 38 million lives from 1997 to 2005. Adherence was measured as the medication possession ratio (MPR). Multivariate logistic regression compared treatment groups based on the likelihood of achieving ≥95% adherence, with sensitivity analyses using alternative thresholds. MPR was assessed as a continuous variable using multivariate linear regression. Covariates included age, gender, insurance payer type, year of study drug initiation, presence of mental health and substance abuse disorders, and third agent class. The study sample consisted of 650 FDC and 1947 NRTI Combo patients. Unadjusted mean adherence to the third agent was higher in the FDC group than the NRTI Combo group (0.92 vs 0.85; P < 0.0001). In regression analyses, FDC patients were 48% and 39% more likely to achieve 95% and 90% third agent adherence, respectively (P ≤ 0.03). None of the other MPR specifications achieved comparable results. Among managed care patients, use of an FDC appears to substantially improve adherence to a third regimen component and thus the likelihood of achieving the accepted standard for adherence to HIV therapy of 95%.
Introduction
Mortality and morbidity associated with HIV disease are dramatically reduced through the use of combination antiretroviral therapy (ART), commonly comprised of two nucleoside reverse transcriptase inhibitors (NRTIs) and either a non-NRTI (NNRTI) or a protease inhibitor (PI).Citation1,Citation2 The latter is often “boosted” with a low-dose of the PI, ritonavir (Norvir, Abbott Laboratories, Abbott Park, IL). ART regimens containing a boosted PI may consist of up to four separate pills, with several dosing frequencies and requirements. However, more compact ART regimens can be created by taking advantage of fixed-dose combination (FDC) products which consist of two or more antiretroviral drugs in a single tablet.
Since the introduction of the first FDC antiretroviral product, FDCs have become a mainstay in the treatment of HIV. The chief advantage of FDCs lies in simplifying a patient’s regimen. In addition to reducing pill burden, many FDCs also have reduced dosing frequency and/or dosing requirements compared to other drugs in the FDC’s therapeutic class. These factors work together to increase the likelihood of adherence.Citation3 To date, most FDC introductions for HIV treatment have consisted of combinations of NRTIs which form the backbone of the ART regimen.Citation4 Patients receiving an NRTI FDC would require a separate NNRTI or PI component.
In HIV, perhaps more than other chronic diseases, regimen adherence is a critical and necessary component of successful treatment. Previous studies have documented that adherence rates in excess of 95% are required in order to achieve a high likelihood of reaching an undetectable plasma HIV RNA level (viral load), a primary objective of ART.Citation4–Citation6 This high level of adherence is needed throughout the course of therapy to maintain undetectable viral load and to protect against the development of viral resistance to regimen components. Poor adherence and the subsequent development of resistance is a primary cause of regimen failure.Citation4
FDCs have been associated with improved adherence compared to their separate components in both clinical trial and observational studies. For example, adherence to the FDC containing lamivudine 150 mg + zidovudine 300 mg (Combivir®, GlaxoSmithKline Inc, Research Triangle Park, NC) has been shown to be higher than adherence to its individual components.Citation7,Citation8 Similar results have been documented for FDCs in other therapeutic areas.Citation9 In addition, it has been shown that a reduction in the total number of pills prescribed can improve adherence to the overall HIV regimenCitation10–Citation12 and suggested that improved adherence to an ART backbone also may result in improved regimen adherence.Citation13–Citation15 Yet, specific evidence of a spillover adherence effect on the remaining regimen components among individuals receiving FDC-based ART regimens is lacking. We compared adherence to the remaining regimen component among individuals receiving ART including an NRTI backbone containing an FDC of abacavir sulfate (ABC) 600 mg + lamivudine (3TC) 300 mg (Epzicom, GlaxoSmithKline Inc, Research Triangle Park, NC) versus NRTI combinations given as two separate pills.
Materials and methods
Data and patients
Data were taken from the Integrated Health Care Information Services (IHCIS, Waltham, MA) Managed Care Benchmark Database, which contains medical (inpatient, outpatient, physician, other ancillary) and pharmacy claims from a national sample of 30 managed care health plans covering approximately 38 million lives in the United States over the period 1997 to 2005.Citation16 The IHCIS database has a representative distribution of age and gender compared with national enrollment in managed care plans. Geographic representation, however, is biased toward the East Coast. Patient-level records in the IHCIS database include demographics and information on benefits eligibility, and periods of health plan enrollment. Claims records in the IHCIS database contain detailed information on diagnoses, hospitalizations, diagnostic testing, therapeutic procedures, inpatient and outpatient physician services, prescription drug use, and cost data in the form of standardized managed care reimbursed amounts for each service. All claims in the IHCIS database were linked using unique patient identifiers and arranged in chronological order, thereby providing a detailed longitudinal file of all medical and pharmacy services utilized by each patient.
All patients in the IHCIS database with at least one pharmacy claim for Epzicom or for two or more components of an NRTI backbone as separate pills were eligible for study inclusion. For each patient, the date of the first prescription claim for any of these agents was designated the index date. Patients initiating Epzicom were designated the FDC group, while subjects receiving separate NRTI components on the index date were designated the NRTI Combo group. Patients in the NRTI Combo group were subject to the additional requirement that the first prescription for each drug be received within 7 days of the other in order to capture the intent to treat with a combination of separate pills. Patients in the FDC group were required to have at least one Epzicom refill within 60 days following the index date. Likewise, patients in the NRTI Combo group were required to have at least one refill for each agent within 60 days following initial receipt of the agent. Individuals in both treatment groups were excluded from the analysis if they met any of the following conditions: receipt of both Epzicom and one or more of its components on the index date; receipt of alternative therapy (ie, NRTI combo for the FDC group, or Epzicom for the NRTI Combo group) prior to the index date; failure to receive a third regimen component within 7 days of the index date; less than 6 months of continuous health plan enrollment prior to the index date; less than 60 days of continuous health plan enrollment after the index date; and/or age less than 18 years on the index date. The analysis was not limited to ART-naïve individuals because such patients may not accurately reflect the clinical populations using these drugs. However, because experienced and naïve patients may differ in their adherence behaviors, we control for prior ART exposure in the statistical analysis.
For each patient, a follow-up period was defined as the period beginning with the index date and ending with expiration of the days’ supply for the last observed refill for the study therapy of interest, receipt of alternative study therapy (eg, Epzicom for the NRTI Combo group or vice versa), a gap of more than 180 days in study therapy, end of health plan enrollment, or end of the IHCIS database, whichever occurred first. Adherence to the remaining regimen component(s), as well as to the overall ART regimen, was assessed for each patient within the follow-up period. The remaining regimen components were categorized by class as PI, NRTI (excluding the NRTI backbone agents), NNRTI, entry inhibitor (EI), or a boosted PI. For simplicity, we refer to the remaining regimen component as the third agent. For patients who received more than three agents, one class among the non-NRTI backbone antiretrovirals in the regimen was randomly selected as the third agent for analysis purposes.
Adherence measure
The primary outcome evaluated in this study was treatment adherence to the non-NRTI-backbone regimen component as measured by the medication possession ratio (MPR). A recent systematic literature review found MPR to be the most widely adopted measure in published claims-based analyses of medication adherence (57% of all studies).Citation17 MPR is generally defined as the proportion of days within an observation period covered by the total days’ supply obtained for a particular study drug within the observation period:
As noted in Andrade et al,Citation17 a common observation period used in the MPR calculation is the number of days between the first dispense date and end of the days’ supply of the last refill for the study therapy of interest. The same observation period was employed here.Citation17
Total days supplied for the third agent was calculated as the combined days’ supplied for all PIs, NNRTIs, EIs, and third NRTIs utilized during the follow-up period. We allowed patients to switch drugs within the same class for the third agent as the class in which that component was initiated (eg, PI to PI, NNRTI to NNRTI, etc) and control for this in the multivariate regressions. presents the percentage of patients in each treatment group who switched within the third agent class (37% of the FDC group, 27% of the NRTI combo group). Follow-up for third component adherence evaluation ended upon third agent switch to a drug outside of the class initiated (eg, upon switch from PI to NNRTI, NNRTI to PI). Days covered by both the NRTI backbone and the third agent were assessed by evaluating overlapping days’ supply for the respective agents.
Table 1 Patient characteristics at baseline by treatment group
Statistical analysis
Patient characteristics were measured at the index date and included age, gender, geographic region, insurance payer type (eg, commercial, self, or government-sponsored), insurance product type (eg, health maintenance organization [HMO], preferred provider organization [PPO]), prior exposure to antiretroviral therapy, and eligibility for mental health benefits coverage. We also assessed the presence of substance abuse and mental health disorders that have been linked to poor ART adherence during the 6-month period prior to therapy initiation. ICD-9 diagnostic and CPT-4 procedural codes appearing in medical records were used to identify these conditions and were based on algorithms set forth by the US Substance Abuse and Mental Health Services Administration (SAMHSA).Citation18
Descriptive analyses of patient characteristics and unadjusted adherence measures were conducted as mean values and standard deviations for continuous variables of interest and frequency distributions for categorical variables of interest. The statistical significance of descriptive differences in adherence outcomes between the FDC and NRTI Combo groups, as well as between patients who are adherent and not adherent with each study therapy based on relevant MPR thresholds, were measured using t-tests and χ2 tests as appropriate, with results reported as P values.
To assess differences in adherence to the third agent between the FDC and NRTI Combo groups, multivariate regressions of the following general forms were estimated:
In EquationEquation 1(1) , continuous MPR was estimated in a linear model as a function of a dichotomous indicator FDC equal to one for patients who initiated Epzicom and zero for patients who initiated an NRTI backbone as separate components, and a vector of baseline patient characteristics (Xi). EquationEquation 2
(2) was a logistic model with the same covariate structure as EquationEquation 1
(1) . The dichotomous outcome, ADHERENT, was set equal to one for patients meeting one of four MPR thresholds (MPR ≥ 0.80, 0.85, 0.90, and 0.95) and zero for patients not meeting the threshold. This range of values was chosen based on previous evidence suggesting that lower risk of virologic failure is associated with maintaining adherence of at least 95%.Citation5,Citation6
All analyses were carried out using SAS® (v 9; SAS Institute, Cary, NC) statistical software.
Results
After applying inclusion and exclusion criteria as described previously, there were 650 individuals in the FDC group and 1947 in the NRTI Combo group (). In both groups, the proportions of patients receiving an NNRTI or a PI as the third agent of their regimens were similar (). Roughly 59%, 42%, and 37% of patients in the NRTI group received lamivudine, tenofovir, or stavudine, respectively. Median duration of follow-up for the FDC group was 272 days; for the NRTI Combo group, 338 days.
Figure 1 Sequential application of study inclusion and exclusion criteria to the IHCIS sample.
Abbreviations: FDC, fixed-dose combination; IHCIS, Integrated Health Care Information Services; NRTI, nucleoside reverse transcriptase inhibitor.
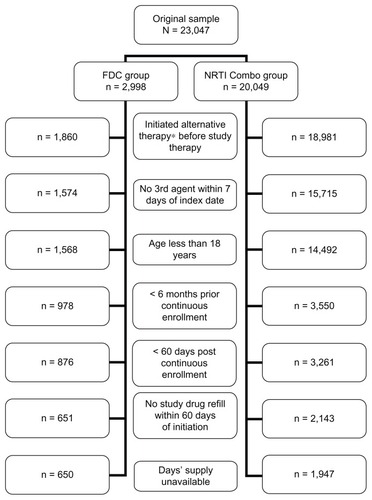
Table 2 Antiretroviral therapy use by treatment group
The distribution of baseline (index date) characteristics for patients in the FDC and NRTI Combo groups is shown in . The majority of study subjects were aged 35–54 years, and 82.7% were men. FDC group patients had an unadjusted mean adherence of 0.88 (standard deviation [SD] = 0.17) versus 0.82 (SD = 0.20) for the NRTI Combo, with median adherence of 0.96 (range: 0.26–1.00) versus 0.89 (range: 0.08–1.00), respectively (P < 0.0001 for mean comparisons). Mean adherence to the third agent was 0.923 (SD = 0.17) for the FDC group and 0.85 (SD = 0.25) for the NRTI Combo group (P < 0.0001).
Partial results for the multivariate regression models of third agent adherence, as described below, are shown in ; full results are available upon request from the authors. In multivariate logistic analyses, the presence of an FDC NRTI backbone consistently improved the likelihood of adherence at the four thresholds examined, and this impact was statistically significant at the 90% and 95% adherence thresholds. Patients in the FDC group were 47% more likely to achieve a clinically meaningful adherence level of 95% to the third agent compared to the NRTI Combo group. When the threshold for adherence was considered at the lower 90% level, the likelihood of achieving that level of adherence to the third agent was 40% higher among FDC patients. Similarly, when adherence was defined as a continuous variable, use of an FDC provided a small improvement in adherence to the third agent compared to the use of separate pills (NRTI Combo), but the magnitude of the effect did not reach statistical significance.
Table 3 Results of multivariate regression analyses on third component adherence
Relative to the PI class, third agents that were from the NRTI or boosted PI classes were associated with a higher likelihood of adherence (or better odds of achieving a certain level of adherence) in all three models shown in . In the continuous MPR model, NRTIs were associated with an absolute increase in adherence of 11.6%; boosted PIs, 7.3%. Entry inhibitors were consistently associated with reduced adherence compared to PIs, but the effect reached only near statistical significance in the continuous MPR model. Switching of the third agent within the same class was also consistently associated with improved adherence in all three models. Prior ART experience in the 6-month, pre-index period was insignificant across all models.
Discussion
Evidence from clinical trials and observational studies in a variety of therapeutic applications supports the ability of FDC products to improve adherence to therapy, compared to separate pills.Citation7,Citation9,Citation19,Citation20 To our knowledge, this is the first study to empirically quantify the spillover effect of FDCs in improving adherence to another regimen component. Our results confirm the hypothesis that use of an FDC as the backbone of an ART regimen improves adherence to the third agent, compared to a regimen that utilizes separate pills as a regimen backbone. This improvement in adherence is in addition to the increase associated solely with the backbone component of the regimen.
While some evidence suggests that newer antiretrovirals and ART combinations may be more “forgiving” of poor adherence than older agents and un-boosted regimens, the standard for adherence in HIV remains high.Citation4 In our population of managed care enrollees, patients receiving an FDC backbone were nearly 50% more likely to achieve an adherence rate of 95% or better to the third agent in the regimen. Even at the lower 90% threshold, FDC backbone use was associated with a nearly 40% increase in the likelihood of third-agent adherence. The magnitude of the FDC spillover adherence effect observed in our sample, while smaller than the approximately 300% direct effect estimated by Legorreta et al,Citation8 is nonetheless statistically and clinically meaningful.
Results for adherence thresholds of 80% and 85% and for continuous adherence were also positive, but did not reach statistical significance. The inability to detect a spillover effect in these other model specifications may reflect the adherence behavior of our sample. Mean regimen adherence among the patients in this study was 88%, relatively high compared to other reports, though not unprecedented.Citation21 Examination of adherence effects from FDCs in patient populations with lower baseline levels of adherence is needed to fully understand the spillover phenomenon.
Across the spectrum of available antiretrovirals, adherence is positively correlated with virologic suppression.Citation4 FDC backbones, then, may play an important role in improving adherence and likelihood of suppression for the remaining regimen component(s), regardless of drug class. Additionally, adherence plays an important role in the development of drug resistance, although the specific relationships may differ across drug classes.Citation22 As such, the spillover adherence effect of FDCs may be especially clinically meaningful for PI-based regimens. Studies examining the relationship between adherence and resistance suggest that the development of primary and secondary PI mutations peaks at levels of adherence just below those required to maintain virologic suppression.Citation22,Citation23 For example, among patients with relatively high overall adherence, even small, absolute improvements in PI adherence of only a few percentage points may be sufficient to substantially reduce mutation development. The use of an FDC backbone may be one tool for achieving such an improvement in PI adherence.
The use of administrative records to examine the spillover effect of FDCs offers several advantages over other data sources. First, these data reflect the experiences of patients in actual clinical practice, potentially avoiding the adherence bias associated with clinical trials.Citation24 Second, these observational data allow for a relatively large sample size, thereby increasing the ability to detect differences between study groups. Additionally, while not a nationally representative sample, the IHCIS data include individuals from all regions of the US. To the extent that heterogeneity in adherence is correlated with regional heterogeneity in HIV risk, demographic characteristics, and other factors that may affect adherence, the generalizability of our results is improved relative to smaller studies of more homogeneous cohorts.
There are differences between the IHCIS sample, and the US HIV population as a whole. In 2006, approximately 73% of individuals living with a diagnosis of HIV or AIDS in the US in 2006 were males, compared to nearly 83% in our study.Citation25 During the same time period, roughly 38% of persons living with HIV/AIDS were aged 18–34 years, compared to less than 15% in our sample. The older age and increased proportion of males observed in our sample may reflect an increased access to health insurance for this group compared to other individuals diagnosed with HIV/AIDS. It is possible that spillover effects measured in different populations may differ from those seen in the IHCIS sample, especially if factors associated with insurance status, such as education and income (which are unobserved in the IHCIS sample), also influence adherence behavior. While socioeconomic status does appear to be associated with adherence in many chronic diseases, such relationships have not been documented conclusively for HIV.Citation26
As with other observational studies, this work is subject to limitations which should be considered when evaluating the results. The retrospective nature of the data source raises the possibility of selection bias because the assignment of patients to study groups is not random, as in a clinical trial. For example, if individuals who received Epzicom were more likely to be adherent to a third regimen component than those who received a backbone of separate NRTIs, the impact of FDCs on spillover adherence would be overestimated. Conversely, if physicians who were particularly concerned with patient adherence tended to prescribe FDCs to that end, then the spillover effect observed here may be underestimated. It should be noted that the study inclusion requirement of at least one refill in the 60 days following the index prescription – necessary to capture the intent to treat with a specific agent – may bias the sample toward more adherent patients. In such a case, the ability of the FDC to improve adherence even among those already adherent is notable. Still, further efforts are needed to understand adherence among very poor adherers.
As noted in , subjects in the two study groups were similar in terms of age and gender, but other differences did exist. We controlled for all the factors listed in in our statistical analysis. We did not have access to subjects’ complete HIV treatment histories and could not definitively identify those who were completely naïve to treatment. While there is some evidence that adherence differs between treatment-experienced and treatment-naïve patients,Citation27 the likelihood that the marginal adherence effect estimated here would differ between these two groups of patients was less likely and, indeed, was what we observed. There may exist other factors for which we were unable to control. If those factors were associated with adherence differentially by study group, the study results may be biased.
Epzicom dosing is labeled as once per day, while most other NRTI combinations used during the study period were dosed twice per day, per product labeling. Thus, some of the spillover attributed to the FDC group may be due to reduced dosing frequency. However, some of the combinations in the NRTI Combo group included one or two agents that could be dosed once per day. Interestingly, patients in the NRTI Combo were more likely to receive an NNRTI as the third regimen component. Compared to PIs, NNRTIs have been associated with improved adherence.Citation28
The approach we use to construct the follow-up period over which adherence was assessed is subject to the inherent limitation that some patients may discontinue study therapy before expiration of the last observed refill. Since discontinuation in that case cannot be observed in automated pharmacy claims, our method may lead to follow-up durations that are slightly overestimated for some patients. Similarly, no gold standard for measurement of adherence exists. Adherence levels measured from pharmacy records have been shown to be higher than those measured by electronic monitoring, although the two measures are highly correlated.Citation29 Importantly, any overestimation of adherence would be attributable to both study groups, minimizing its effect.
This study examines only the use of an FDC containing two antiretrovirals and intended to be combined with at least one additional agent. Due to sample size constraints, we were unable to assess whether spillover effects extend to all components of regimens that consist of an FDC plus two or more antiretrovirals taken as separate pills. FDCs containing three antiretrovirals are also available and can be used alone or as part of a larger regimen in combination with other antiretrovirals. It is unclear, a priori, whether such effects would be greater or lesser than those seen with two-agent FDCs in a typical, three-agent regimen. We have shown that adherence to a third regimen component is increased with the use of an FDC backbone and that this adherence level is high. As a result, in populations where medication-taking behavior is relatively high, triple-agent FDCs may not offer much of an adherence advantage over dual-agent FDCs. Additional research on the direct and spillover adherence effects of dual-agent and triple-agent FDCs as components of regimens consisting of more than three antiretrovirals is warranted.
Successful HIV therapy requires individuals to maintain nearly perfect adherence, and clinical practice guidelines have long recommended that physicians consider adherence when selecting regimen components. This study highlights an additional adherence advantage associated with the use of FDCs that has not previously been identified: a spillover effect on a non-fixed regimen component. While additional efforts are needed to assess the extent of adherence spillover associated with other FDCs, our work supports the use of fixed-dose NRTI backbones as a means of encouraging adherence to the entire ART regimen.
Acknowledgments
The authors thank Christopher M Blanchette for his contributions to this study. This work was funded by GlaxoSmithKline Inc (Research Triangle Park, NC). The individual authors’ contributions to the work are as follows: TLK led the study design, interpretation of results, and writing. As corresponding author, TLK takes full responsibility for the entirety of the content of the manuscript. KLD conducted all data analysis and contributed to the interpretation of results and writing. SRE assisted with study design and contributed to the interpretation of results. EAD provided the data source for the study and contributed to the study design.
Disclosures
This study was funded by a contract between GlaxoSmithKline Inc (Research Triangle Park, NC), which manufactures abacavir sulfate, zidovudine, lamivudine, and various combinations of these drugs, and RTI Health Solutions (Research Triangle Park, NC), an independent contract research organization that has received research funding for this and other studies from GlaxoSmithKline and other pharmaceutical companies that market drugs for use in HIV patients and other medical conditions. KLD and SRE are employees of RTI Health Solutions. At the time of the study, EAD was an employee of GlaxoSmithKline. TLK is an Associate Professor of Pharmaceutical Outcomes and Policy at the University of Florida. She has provided consultancy to RTI Health Solutions and has received funding for other studies from GlaxoSmithKline and other pharmaceutical companies that market drugs for use in the treatment of HIV patients.
References
- MocroftALedergerberBKatlamaCEuroSIDA study groupDecline in the AIDS and death rates in the EuroSIDA study: an observational studyLancet20033629377222912853195
- PalellaFJJrDelaneyKMMoormanACDeclining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study InvestigatorsN Engl J Med1998338138538609516219
- StoneVEHoganJWSchumanPHERS studyAntiretroviral regimen complexity, self-reported adherence, and HIV patients’ understanding of their regimens: survey of women in the her studyJ Acquir Immune Defic Syndr200128212413111588505
- Panel on Antiretroviral Guidelines for Adults and AdolescentsGuidelines for the use of antiretroviral agents in HIV-1-infected adults and adolescentsDepartment of Health and Human ServicesOctober 1420111167 Available from: http://www.aidsinfo.nih.gov/Content-Files/AdultandAdolescentGL.pdfAccessed on October 31, 2011
- PatersonDLSwindellsSMohrJAdherence to protease inhibitor therapy and outcomes in patients with HIV infectionAnn Intern Med20001331213010877736
- Low-BeerSYipBO’ShaughnessyMVHoggRSMontanerJSAdherence to triple therapy and viral load responseJ Acquir Immune Defic Syndr200023436036110836763
- EronJJrYeniPGatheJJrKLEAN study teamThe KLEAN study of fosamprenavir-ritonavir versus lopinavir-ritonavir, each in combination with abacavir-lamivudine, for initial treatment of HIV infection over 48 weeks: a randomised non-inferiority trialLancet2006368953447648216890834
- LegorretaAYuAChernicoffHGilmoreAJordanJRosenzweigJCAdherence to combined lamivudine + zidovudine versus individual components: a community-based retrospective medicaid claims analysisAIDS Care200517893894816176890
- BangaloreSKamalakkannanGParkarSMesserliFHFixed-dose combinations improve medication compliance: a meta-analysisAm J Med2007120871371917679131
- GardnerEMBurmanWJMaraviMEDavidsonAJSelective drug taking during combination antiretroviral therapy in an unselected clinic populationJ Acquir Immune Defic Syndr200540329430016249703
- MaggioloFRavasioLRipamontiDSimilar adherence rates favor different virologic outcomes for patients treated with nonnucleoside analogues or protease inhibitorsClin Infect Dis200540115816315614706
- PortsmouthSDOsorioJMcCormickKGazzardBGMoyleGJBetter maintained adherence on switching from twice-daily to once-daily therapy for HIV: a 24-week randomized trial of treatment simplification using stavudine prolonged-release capsulesHIV Med20056318519015876285
- CrémieuxACKatlamaCGillotinCAZl10002 Study GroupA comparison of the steady-state pharmacokinetics and safety of abacavir, lamivudine, and zidovudine taken as a triple combination tablet and as abacavir plus a lamivudine-zidovudine double combination tablet by HIV-1-infected adultsPharmacotherapy200121442443011310515
- LamarcaAClumeckNPlettenbergAEfficacy and safety of a once-daily fixed-dose combination of abacavir/lamivudine compared with abacavir twice daily and lamivudine once daily as separate entities in antiretroviral-experienced HIV-1-infected patients (CAL30001 Study)J Acquir Immune Defic Syndr200641559860616652033
- MooreKHShawSLaurentALLamivudine/zidovudine as a combined formulation tablet: bioequivalence compared with lamivudine and zidovudine administered concurrently and the effect of food on absorptionJ Clin Pharmacol199939659360510354963
- IngenixIntegrated Health Care Information Services Available from: http://www.ingenix.com/AboutUs/Businesses/ihcis/
- AndradeSEKahlerKHFrechFChanKAMethods for evaluation of medication adherence and persistence using automated databasesPharmacoepidemiol Drug Saf200615856557416514590
- FinkelsteinEBrayJLarsonMMental healthManderscheidRWHendersonMJPrevalence of, and payments for, mental health and substance abuse disorders in public and private sector health plansRockville, MarylandUnited States Department of Health and Human Services, Center for Mental Health Services2002 Available from: http://store.samhsa.gov/product/Mental-Health-United-States-2002/SMA04-3938Accessed on June 19, 2009
- MelikianCWhiteTJVanderplasADeziiCMChangEAdherence to oral antidiabetic therapy in a managed care organization: a comparison of monotherapy, combination therapy, and fixed-dose combination therapyClin Ther200224346046711952029
- VanderpoelDRHusseinMAWatson-HeidariTPerryAAdherence to a fixed-dose combination of rosiglitazone maleate/metformin hydrochloride in subjects with type 2 diabetes mellitus: a retrospective database analysisClin Ther200426122066207515823770
- MaitlandDJacksonAOsorioJMandaliaSGazzardBGMoyleGJSwitching from twice-daily abacavir and lamivudine to the once-daily fixed-dose combination tablet of abacavir and lamivudine improves patient adherence and satisfaction with therapyHIV Med20089866767218631255
- BangsbergDRAcostaEPGuptaRAdherence-resistance relationships for protease and non-nucleoside reverse transcriptase inhibitors explained by virological fitnessAIDS200620222323116511415
- KingMSBrunSCKempfDJRelationship between adherence and the development of resistance in antiretroviral-naive, HIV-1-infected patients receiving lopinavir/ritonavir or nelfinavirJ Infect Dis2005191122046205215897990
- WhiteHDAdherence and outcomes: it’s more than taking the pillsLancet200536695021989199116338439
- Centers for Disease Control and PreventionHIV/AIDS Surveillance Report 2006 Available from: http://www.cdc.gov/hiv/surveillance/resources/reports/2006report/Accessed on January 23, 2009
- FalagasMEZarkadouliaEAPliatsikaPAPanosGSocioeconomic status (SES) as a determinant of adherence to treatment in HIV infected patients: a systematic review of the literatureRetrovirology200851318241330
- HorbergMSilverbergMHurleyLDelorenzeGQuesenberryCInfluence of prior antiretroviral experience on adherence and responses to new highly active antiretroviral therapy regimensAIDS Patient Care STDS200822430131218338961
- MartinMDel CachoCECodinaCRelationship between adherence level, type of the antiretroviral regimen, and plasma HIV type 1 RNA viral load: a prospective cohort studyAIDS Res Hum Retroviruses200824101263126818834323
- HansenRAKimMMSongLTuWWuJMurrayMDComparison of methods to assess medication adherence and classify nonadherenceAnn Pharmacother200943341342219261962