
Abstract
Purpose
Rosacea is a chronic inflammatory dermatosis mainly involving facial skin, leading to physical and emotional problems, which greatly affect the quality of life (QoL) of patients. Dermatology Life Quality Index (DLQI) and willingness to pay (WTP) are well-established instruments assessing the health-related quality of life (HRQoL), while very few studies have been focused on this topic about rosacea in China. The present study investigated HRQoL in Chinese rosacea patients.
Patients and Methods
This cross-sectional study was conducted on 973 patients with rosacea. Sociodemographic data, clinical features and DLQI were collected, and WTP was assessed by three standardized items. Multivariable logistic analysis was performed to investigate independent factors influencing QoL.
Results
A total of 921 questionnaires were accomplished by participants. The mean DLQI score was 11.6 (median 11). Patients were willing to pay an average of € 896.2 (median € 368.1) for complete cure. 33.3% would like to pay more than 20% of their monthly income to achieve sustainable control. There were positive correlations between WTP with DLQI (P < 0.05). DLQI could be independently impacted by age (21–30 and 31–40 relative to > 50, OR = 3.242 and 3.617, respectively), the occupational requirement of appearance (high, OR = 4.410), disease duration (< 2 years, OR = 1.582), edema (OR = 1.844) and severity of flushing, burning, stinging and pruritus (severe, OR = 2.003, 1.981, 2.491, 2.249, respectively). There were no significant associations between WTP and most of the clinical factors.
Conclusion
The QoL was greatly impaired and should not be ignored among rosacea patients in China. Patients aged 21–40y, having occupational requirement of appearance, with the disease duration less than 2 years, and suffering severe flushing and related sensitive symptoms were more likely to have severe or very severe limitation of QoL.
Introduction
Rosacea is a chronic inflammatory dermatosis that primarily affects the convexities of central face. Manifestations of rosacea include flushing, persistent erythema, papules and pustules, telangiectasia and phymatous changes as well as plaque and edema.Citation1 The global prevalence of rosacea is 5.46%,Citation2 while in China the prevalence was reported as 3.48%,Citation3 and not lower than 3.35% even in the population of adolescents.Citation4
Since rosacea predominantly presents in the facial region and affects patients’ cosmetic appearance, it frequently interferes with social and occupational interactions.Citation5 Besides, the accompanying subjective symptoms of rosacea (such as burning, stinging and pruritus) may also reduce patients’ quality of life (QoL) or even sleep quality.Citation6 Another disturbance is the long course of recurrent exacerbations and remissions,Citation1 which may make patients lose confidence in treatment. Plenty of triggers could cause rosacea to relapse, so patients have to be very careful to modify their productivity and behavior to avoid the recurrence.Citation2,Citation7 As a result, rosacea may not be life-threatening, but still result in significant psychosocial and emotional problems due to its unsightly suffering and embarrassing appearance.Citation8,Citation9 Patients with rosacea often have feelings of stigmatization and stress, more severely, have a higher probability of social phobia, anxiety and depression.Citation9–Citation11 Nonetheless, clinicians often overlook these problems perceived by patients and focus more on the visible and objective symptoms. This discrepancy may interfere with the treatment satisfaction as the patients usually care more about subjective feelings and psychosocial impact.Citation12,Citation13 To eliminate this discrepancy, QoL should be considered when the therapy strategy is made.
Generally, the QoL can be evaluated comprehensively with several kinds of instruments, including descriptive and detailed health status instruments such as DLQI, and preference-based methods composing of willingness-to-pay (WTP) and utilities.Citation14 The Dermatology Life Quality Index (DLQI) is the most extensively used health status instrument in dermatologyCitation20 and is recommended by the ROSacea COnsensus to assess the patient’s burden and refer for psychological consultation of rosacea patients.Citation21 WTP is another well-used health economic method, which can afford complementary information to that revealed by DLQI. WTP is expressed in monetary terms, so it is relatively easier and more intuitive for patients to consider paying certain amounts of money. For those disorders considered to be minor health states, WTP is especially suitable to assess the QoL.Citation22 As for rosacea, researchers have used DLQI to evaluate HRQoL over the last two decades, and there were a few studies focused on WTP. For specific, Beikert et al used DLQI and WTP to evaluate HRQoL in Germany and found a moderate WTP and mild QoL reduction in patients with rosacea.Citation23 However, there is lack of research in this area in China so far.
To evaluate the effects of rosacea on the QoL in China, in this study we investigated DLQI and WTP among 921 rosacea patients, and tried to find out the factors associating closely with QoL.
Materials and Methods
Study Design
This non-interventional, cross-sectional study was performed among patients with rosacea in Xiangya Hospital of Central South University (Changsha, China) from October 2017 to May 2018. All the patients met the diagnostic criteria based on the National Rosacea Society Expert Committee,Citation1,Citation24 and were diagnosed independently by two board-certified dermatologists. Patients with other concurrent facial skin diseases such as acne, eczema, seborrheic dermatitis and systemic lupus erythematosus were excluded.
Questionnaire
In the first part of the questionnaire, sociodemographic and clinical data were recorded. For sociodemographic data, age, gender, income, the occupational requirement of appearance, education, marital status and residential location were collected. In terms of clinical data, the symptoms and signs recorded included flushing, persistent erythema, papules and pustules, angiotelectasis, phymatous changes, plaque, edema, dry sensation, burning sensation, stinging sensation as well as pruritus. For the severity of rosacea, persistent erythema, papules and pustules, angiotelectasis were evaluated by two professional doctors independently and rated as absent, mild, moderate and severe. Patients would be required to report the feeling of flushing, dry sensation, burning sensation, stinging sensation and pruritus rating as 11-point scale (0–10) and ultimately divided into three levels before analysis: absent to mild, moderate and severe.
To measure the HRQoL, Dermatology Life Quality Index (DLQI)Citation25 and WTP were evaluated. DLQI in Chinese version was used, which contains 10 questions covering six aspects of life including symptoms, feelings, daily activities, leisure time, work or school, personal relationships and treatment. It depends on the patients’ perception during the previous week, and total score ranges from 0 to 30. The score can be divided into five classes: 0–1 (no effect), 2–5 (small effect), 6–10 (moderate effect), 10–20 (very large effect), 20–30 (extremely large effect).Citation26
To assess WTP, three standard questions were inquired to obtain the amount of money they were willing to pay for a hypothetical drug to control or cure rosacea as previous studies reported.Citation14,Citation17,Citation23,Citation27 For the disease control question, patients were asked about the amount per month and the percentage of monthly income they were willing to spend. Then, patients were asked to name a total amount of money they would pay at once to achieve the complete cure of rosacea.
Statistical Analysis
For continuous variables, mean, standard deviation (SD), median and interquartile range (IQR) were described. And for categorical variables, absolute and percentage frequencies were presented. Mann-Whitney U-tests and Kruskal-Wallis H-tests were used to compare the independent groups of continuous variables. Statistical correlation analysis was conducted using Spearman’s rank test (rs). Multivariate binary and ordinal logistic regression analyses were used to elicit the predictors for DLQI. Multivariate linear regression analysis was applied to assess the association between WTP and income (controlling for age, gender, the occupational requirement of appearance, education, marital status and residential location). The level of significance was two-sided and considered to be significant (P < 0.05) or highly significant (P < 0.001). All analyses were performed with IBM SPSS version 21 for Windows.
Results
Total Subject Population
A total of 973 patients were recruited into our study, 921 questionnaires were collected for analysis of DLQI and 594 participants fulfilled the WTP questionnaire. The sociodemographic and clinical characteristics were displayed in and , respectively. The mean ± SD age of our study population was 32.4 ± 11.1 years (median 30, IQR 23–41). And females accounted for 91.0% of all patients.
Table 1 DLQI Scores According to Sociodemographic Characteristics and Clinical Characteristics
Table 2 DLQI Scores According to Adjusted Clinical Characteristics
Almost all patients had a flushing manifestation (n = 916, 99.5%). Of patients with phymatous change, 34.9% (29/83) were male. The mean disease duration was 4.8 ± 5.7 years with those over 2 years accounting for 58.3% (537/921). Almost half of the patients (436/921,47.3%) had three or more facial regions involved. And 11.6% (107/921) of the participants had a family history.
DLQI
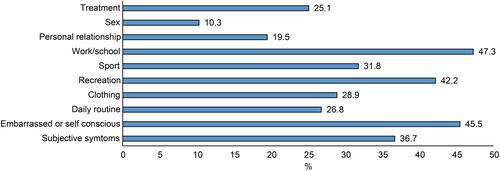
The mean DLQI total score of the patients was 11.6 ± 7.2 (median 11, IQR 6–16). About half (496/921,50.9%) of them thought the impact of rosacea on HRQoL was large to extremely large. Especially prominent impairment in HRQoL was observed in the items of “work/school” and “embarrassed or self conscious” in DLQI ().
Figure 1 Percentage of patients by DLQI items rated moderately or severely affected.
Sociodemographic Characteristics Associating with DLQI
Statistically significant differences in DLQI score were observed in age, gender, the occupational requirement of appearance (). Females rated a significantly higher DLQI score (P < 0.001). For different age groups, we observed the most severe HRQoL impairment in patients aged 31–40 years, which was significantly different from patients aged 41–50 years (P = 0.008) and over 50 years (P < 0.001). The occupational requirement of appearance was positively correlated with DLQI (rs = 0.148, P < 0.001). Those with high occupational requirements of appearance had significantly higher DLQI score () than the other three groups. No significant differences were observed in marital status, residential location and education ().
Clinical Characteristics Associating with DLQI
Regarding phymatous changes, patients with phymatous changes exhibited a significantly lower DLQI score (, P = 0.004). Patients with the signs including angiotelectasis (P = 0.033), plaque (P = 0.021) and edema (P < 0.001) rated significantly higher DLQI scores than the corresponding negative counterparts (). Patients with shorter disease duration tended to have higher DLQI score (, P = 0.001).
We next divided the severity of rosacea into four or three levels as mentioned earlier, flushing, erythema, dry sensation, burning sensation, stinging sensation and pruritus displayed a positive correlation with DLQI level (rs = 0.106, P = 0.001; rs = 0.109, P = 0.001; rs = 0.120, P < 0.001; rs = 0.234, P < 0.001; rs = 0.212, P < 0.001; rs = 0.199, P < 0.001; respectively) (). Also, patients with different severity of the above symptoms had significantly different DLQI total scores (H-test: P < 0.01). Corresponding with the correlation between DLQI score and the severity of flushing, patients with longer daily flushing duration also had higher DLQI scores ().
Factors Independently Associating with DLQI
In a binary logistic regression model predicting HRQoL reduction, DLQI score was independently related to age, gender, occupational requirement of appearance, disease duration, the presence of edema, the severity of certain symptoms (ie, flushing, burning sensation, stinging sensation and pruritus) (). With ordinal logistic regression analysis, we observed the same factors independently affected DLQI, with the exclusion of gender ().
Table 3 Factors Independently Associating with DLQI Total Score
Willingness to Pay
When participants were asked to name a monthly cost that they were willing to spend for controlling the disease, the average amount was € 106.5 ± 6.7 (median €61.3, IQR €36.8–122.7). Concerning the percentage of monthly income (relative WTP), patients accepted to spend 23.2% ± 0.97% (median 15.5%, IQR 10–30%) on average. 198 out of 594 participants (33.3%) would like to pay more than 20% of their monthly income to achieve sustainable control. As to one-time payment for a complete cure of rosacea, the average amount patients willing to pay was €896.2 ± 68.5 (median €368.1, IQR €0-1227). We observed a negative correlation between relative WTP and age (rs = −0.230, P < 0.001). And income was significantly associated with the one-time WTP (B = 0.031, P < 0.001) and monthly WTP (B = 0.005, P < 0.001) after adjusting other sociodemographic characteristics.
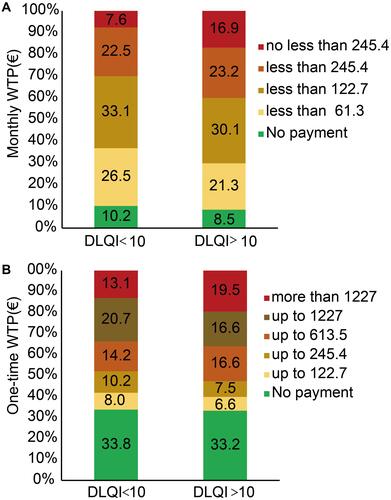
Additionally, among participants who were willing to invest some money for controlling or completely curing of the disease, we observed positive correlations between DLQI total score and the one-time WTP (rs = 0.130, P = 0.01), monthly WTP (rs = 0.139, P = 0.001) as well as relative WTP (rs = 0.110, P = 0.01). For patients with DLQI total score more than 10, 16.9% (54/319) of them were willing to pay no less than €245.4 monthly, and 19.5% (62/319) of them were willing to pay more than €1227 one-time (DLQI < 10: 7.6% (21/275) and 13.1% (36/275), respectively) (). When the participants were divided into two group according to the WTP (one-time WTP: ≤ €2454 and > €2454; monthly WTP: <€122.7 and ≥ €122.7; relative WTP: < 20% and ≥ 20%), the high WTP groups always have significantly higher DLQI score (U-test: one-time WTP, P = 0.001; monthly WTP, P < 0.001; relative WTP, P = 0.009) than the corresponding low WTP groups (data not shown).
Figure 2 Monthly WTP (A) and one-time WTP (B) distribution in DLQI<10 and >10. The euro symbol (€) represents the euro currency.
Discussion
Rosacea is a chronic inflammatory skin disorder mainly affects centrofacial areas resulting in physical disfigurement and emotional distress and impairs the patients’ quality of life. In this study, we evaluated the effects of rosacea on the QoL by investigating DLQI and WTP among 921 rosacea patients in China, which verified that rosacea could significantly impair QoL. Age, occupational requirement of appearance, disease duration, severity of flushing and the related symptoms were primary factors associated with the QoL. On the other hand, rosacea has been suggested to be considered a systemic disease, which was associated with some other diseases including psychiatric disorders.Citation28 Rosacea treatment remains challenging for dermatologists, so dermatologists should pay attention to patient experience and patient education.Citation29 QoL can, to some extent, reflect the patient individual experience. Our discovery donates a guide for clinicians to rapidly recognize patients whose QoL were severely impaired, to better manage these patients and improve treatment satisfaction. In turn, QoL can be an indicator to assess the treatment effectiveness.
DLQI is a classic instrument for evaluating HRQoL and widely used in studies regarding disease burden. An authorized DLQI in Chinese version has been widely used in skin diseases for research or clinical settings in China. A study conducted in 851 Chinese patients with psoriasis showed a mean DLQI score of 11.34.Citation19 As to alopecia areata and androgenetic alopecia, a relative low mean DLQI score of 6.3 was reported,Citation30 similar results were showed in another study which showed a DLQI score of 7.21 for alopecia areata and 8.30 for androgenetic alopecia.Citation31 Two studies focused on vitiligo conducted in the Chinese patients obtained the mean overall DLQI scores of 8.41 and 5.83, respectively.Citation16,Citation32 One study showed Chinese patients with lepromatous leprosy had a mean DLQI score of 18.78.Citation33 In this study, the mean score of DLQI for rosacea was 11.6, indicating the huge effect of rosacea on patients’ HRQoLCitation26 comparable with that in psoriasis patients,Citation19 and more severe than patients with other common dermatosis such as vitiligo,Citation16 alopecia.Citation30,Citation31
The DLQI score of rosacea obtained in the current study was in the range reported in a systematic review (4.1–17.3),Citation34 similar to the results of another study focused on rosacea in China,Citation35 but much higher than the published data from other countries.Citation7,Citation23,Citation36 It has been recognized that age is negatively correlated with DLQI score.Citation34 The mean age of our study population was relatively younger, which may, at least in part, explain our higher DLQI score. On the other hand, all our participants were recruited from the hospital which might lead to a select bias, contributing to their relatively high DLQI score. Based on our study, women were more likely to suffer greater impairment on HRQoL. This finding was consistent with the published researches conducted by Beikert et alCitation23 and Aksoy et al.Citation36 One possible reason was that women often paid more attention to their appearance. Concerns about the impaired appearance always cause some emotional problems like embarrassment or low self-esteem,Citation11 negatively affecting the HRQoL. In addition, occupational requirement of appearance was an independent factor associated with HRQoL, with higher requirement indicating more severe impairment of HRQoL. Accordingly, we observed that “work/school” and “embarrassed or self-conscious” contained in DLQI displayed as the most prominent affected items among rosacea patients. Thus, asking the occupational requirement of appearance is helpful to easily and rapidly assess the impact of rosacea on HRQoL.
As rosacea is a chronic disease, patients with long disease duration may be forced to fit this situation, and the impaired HRQoL may be restored or turn to be tolerable. In the current study, we observed that patients with shorter disease duration had more severe impairment on HRQoL, which is consistent with the results from other studies.Citation23,Citation37 In the multivariable analysis, we found the severity of flushing and the accompanied subjective feelings (ie, burning, stinging, dry sensation and pruritus) rather than objective signs could independently impact DLQI score, which is consistent with a previous study.Citation36 In addition to the severity level of flushing, the longer daily duration of flushing was also found to be associated with a higher DLQI score, although this association turned insignificant in multivariate analysis. These results indicate patients with more severe subjective symptoms were more likely to have severe impairment of HRQoL, just as the previous viewpoint mentioned, flushing and burning were the most disturbing symptoms of rosace.Citation38 Therefore, we suggest more frequent follow-up visits for patients who complains about severe subjective symptoms.
For other phenotypes of rosacea, we observed a potential association between edema and high DLQI score, which is consistent with a previous study.Citation7 Interestingly, patients with phymatous changes were related to a significantly low DLQI score, but the trend turned insignificant in a multivariable analysis model.
As for other visible signs including the presence of plaque and severity of persistent erythema, angiotelectasis, papules and pustules, we did not find any significant correlation with the DLQI score. It follows that the sensitive symptoms were associated more closely with the limitation of QoL than the common objective signs of rosacea. However, it has been well-recognized that some patients lacking clinical severe visible signs would complain of a great influence on their quality of life.Citation21 Additionally, a study in acne showed that even if the visible signs of a disease were resolved, it is relatively difficult to improve patients’ emotional status.Citation39 This situation also happens in rosacea patients. For these patients, the “non-visible” QoL limitations were frequently overlooked by the clinicians. This inconsistent view about the disease severity between the clinicians and patients may interfere with the therapeutic decisions and reduce treatment satisfaction. Recognizing those patients with severe impaired HRQoL is thus essential in the clinical process.
WTP is another method estimating HRQoL from the economic perspective, which may be more intuitive than DLQI. WTP was relatively rarely used in dermatosis in China. In the current study, we used the relative WTP which seems to be income-independent to compare our WTP with other diseases and in other countries. In our study, patients accepted to spend 15.5% (median) of their monthly income (relative WTP) for long-term treatment. According to relative WTP, patients with rosacea have comparable HRQoL impairment to patients with atopic dermatitis, psoriasis, alopecia areata, and port wine stains,Citation17,Citation40,Citation41 but less severe impairment than low-risk melanoma.Citation27 These data indicate a large effect of rosacea on QoL.
Based on our results, about one-third (33.3%) of the individuals were willing to pay a relative WTP more than 20%, with the proportion a little higher than the data reported in Germany (11.4%).Citation23 That may be attributed to a relatively young participant, as in our study age seemed to have a negative correlation to the relative WTP. In addition, we observed a positive correlation between DLQI and WTP. This correlation has been proposed in previous studies about rosacea and other dermatological diseases.Citation15,Citation17,Citation23,Citation42 Unexpectedly, we did not observe any significant associations between WTP and most of the clinical factors including the presence or severity of symptoms and signs, the disease duration, lesion area, as well as family history (data not shown). The possible reason may be explained by the selection bias, as one-third of the participants refused to provide the WTP data. Nevertheless, the good correlations between WTP and DLQI provide the evidence of WTP as a screen indicator for individuals with poor QoL in Chinese rosacea patients.
There may be some limitations in our study. First, the mean age of the study population was relatively young, compared to similar studies in other countries. Additionally, as we mentioned above, the participants included in our study all came from the hospital affiliated to a university, so they might have either more severe rosacea or greater QoL impairment. The consequences of these biases may cause QoL impairment overrated.
In summary, in this study we confirm that rosacea exerts a substantial burden on patients’ life with severe limitations of HRQoL and high values of WTP. There were positive correlations between WTP and DLQI. Patients aged 21–40 years, with high occupational requirement of appearance, with shorter disease duration and severe symptoms tended to have a high possibility of greatly impaired QoL. When admitting these patients, clinicians should attach high importance, HRQoL assessment and psychological counseling are particularly needed.
Abbreviations
DLQI, Dermatology Life Quality Index; HRQoL, health-related quality of life; OR, odds ratio; QoL, quality of life; WTP, willingness to pay.
Ethics Approval and Informed Consent
The research was approved by the ethics review board of Xiangya Hospital Central South University. After having been instructed with this study and granted written informed consent, patients were enrolled. The study has been performed in accordance with the Declaration of Helsinki.
Acknowledgments
We are grateful to all of the participants, dermatologists and staff members involved in this study.
Yaqun Huang and Sha Yan contributed equally to this work and share first authorship.
Disclosure
The authors report no conflicts of interest in this work.
Additional information
Funding
References
- Wilkin J, Dahl M, Detmar M, et al. Standard classification of rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol. 2002;46(4):584–587. doi:10.1067/mjd.2002.120625
- Gether L, Overgaard LK, Egeberg A, Thyssen JP. Incidence and prevalence of rosacea: a systematic review and meta-analysis. Br J Dermatol. 2018;179(2):282–289.
- Li J, Wang B, Deng Y, et al. Epidemiological features of rosacea in Changsha, China: a population-based, cross-sectional study. J Dermatol. 2020;47(5):497–502. doi:10.1111/1346-8138.15301
- Zuo Z, Wang B, Shen M, et al. Skincare habits and rosacea in 3439 Chinese adolescents: a university-based cross-sectional study. Acta Derm Venereol. 2020;100(6):adv00081. doi:10.2340/00015555-3442
- Bewley A, Fowler J, Schöfer H, Kerrouche N, Rives V. Erythema of rosacea impairs health-related quality of life: results of a meta-analysis. Dermatol Ther (Heidelb). 2016;6(2):237–247. doi:10.1007/s13555-016-0106-9
- Wang Z, Xie H, Gong Y, et al. Relationship between rosacea and sleep. J Dermatol. 2020;47(6):592–600. doi:10.1111/1346-8138.15339
- Tan J, Steinhoff M, Bewley A, Gieler U, Rives V. Characterizing high-burden rosacea subjects: a multivariate risk factor analysis from a global survey. J Dermatolog Treat. 2020;31(2):168–174. doi:10.1080/09546634.2019.1623368
- Basra MK, Shahrukh M. Burden of skin diseases. Expert Rev Pharmacoecon Outcomes Res. 2009;9(3):271–283. doi:10.1586/erp.09.23
- Halioua B, Cribier B, Frey M, Tan J. Feelings of stigmatization in patients with rosacea. J Eur Acad Dermatol Venereol. 2017;31(1):163–168. doi:10.1111/jdv.13748
- Böhm D, Schwanitz P, Stock GS, Schmid-Ott G, Schulz W. Symptom severity and psychological sequelae in rosacea: results of a survey. Psychol Health Med. 2014;19(5):586–591. doi:10.1080/13548506.2013.841968
- Su D, Drummond PD. Blushing propensity and psychological distress in people with rosacea. Clin Psychol Psychother. 2012;19(6):488–495. doi:10.1002/cpp.763
- Johnston SA, Krasuska M, Millings A, Lavda AC, Thompson AR. Experiences of rosacea and its treatment: an interpretative phenomenological analysis. Br J Dermatol. 2018;178(1):154–160. doi:10.1111/bjd.15780
- Jansea AJ, Gemkeb RJ, Uiterwaalc CS, Tweeld I, Kimpena JLL, Sinnema G. Quality of life: patients and doctors don’t always agree: a meta-analysis. J Clin Epidemiol. 2004;57(7):653–661. doi:10.1016/j.jclinepi.2003.11.013
- Seidler AM, Bayoumi AM, Goldstein MK, Cruz PD Jr., Chen SC. Willingness to pay in dermatology: assessment of the burden of skin diseases. J Invest Dermatol. 2012;132(7):1785–1790. doi:10.1038/jid.2012.50
- Radtke MA, Schäfer I, Gajur A, Langenbruch A, Augustin M. Willingness-to-pay and quality of life in patients with vitiligo. Br J Dermatol. 2009;161(1):134–139. doi:10.1111/j.1365-2133.2009.09091.x
- Wang KY, Wang KH, Zhang ZP. Health-related quality of life and marital quality of vitiligo patients in China. J Eur Acad Dermatol Venereol. 2011;25(4):429–435. doi:10.1111/j.1468-3083.2010.03808.x
- Beikert FC, Langenbruch AK, Radtke MA, Kornek T, Purwins S, Augustin M. Willingness to pay and quality of life in patients with atopic dermatitis. Arch Dermatol Res. 2014;306(3):279–286. doi:10.1007/s00403-013-1402-1
- Larsen MH, Strumse YAS, Borge CR, Osborne R, Andersen MH, Wahl AK. Health literacy: a new piece of the puzzle in psoriasis care? A cross-sectional study. Br J Dermatol. 2019;180(6):1506–1516. doi:10.1111/bjd.17595
- He Z, Lu C, Basra MK, Ou A, Yan Y, Li L. Psychometric properties of the Chinese version of Dermatology Life Quality Index (DLQI) in 851 Chinese patients with psoriasis. J Eur Acad Dermatol Venereol. 2013;27(1):109–115. doi:10.1111/j.1468-3083.2011.04371.x
- Lesner K, Reich A, Szepietowski JC, et al. Determinants of psychosocial health in psoriatic patients: a multi-national study. Acta Derm Venereol. 2017;97(10):1182–1188. doi:10.2340/00015555-2760
- Schaller M, Almeida LMC, Bewley A, et al. Recommendations for rosacea diagnosis, classification and management: update from the global rosacea consensus 2019 panel. Br J Dermatol. 2020;182(5):1269–1276. doi:10.1111/bjd.18420
- Seidler AM, Kini SP, DeLong LK, Veledar E, Chen SC. Preference-based measures in dermatology: an overview of utilities and willingness to pay. Dermatol Clin. 2012;30(2):223–229. doi:10.1016/j.det.2011.12.002
- Beikert FC, Langenbruch AK, Radtke MA, Augustin M. Willingness to pay and quality of life in patients with rosacea. J Eur Acad Dermatol Venereol. 2013;27(6):734–738. doi:10.1111/j.1468-3083.2012.04549.x
- Gallo RL, Granstein RD, Kang S, et al. Standard classification and pathophysiology of rosacea: the 2017 update by the National Rosacea Society Expert Committee. J Am Acad Dermatol. 2018;78(1):148–155. doi:10.1016/j.jaad.2017.08.037
- Finlay AY, Khan GK. Dermatology Life Quality Index (DLQI)-a simple practical measure for routine clinical use. Clin Exp Dermatol. 1994;19(3):210–216. doi:10.1111/j.1365-2230.1994.tb01167.x
- Hongbo Y, Thomas CL, Harrison MA, Salek MS, Finlay AY. Translating the science of quality of life into practice: what do Dermatology Life Quality Index scores mean? J Invest Dermatol. 2005;125(4):659–664. doi:10.1111/j.0022-202X.2005.23621.x
- Augustin M, Blome C, Forschner A, et al. Willingness to pay for a cure of low-risk melanoma patients in Germany. PLoS One. 2018;13(5):e0197780. doi:10.1371/journal.pone.0197780
- Wollina U. Is rosacea a systemic disease? Clin Dermatol. 2019;37(6):629–635. doi:10.1016/j.clindermatol.2019.07.032
- Zhang H, Tang K, Wang Y, Fang R, Sun Q. Rosacea treatment: review and update. Dermatol Ther (Heidelb). 2021;11(1):13–24. doi:10.1007/s13555-020-00461-0
- Zhang M, Zhang N. Quality of life assessment in patients with alopecia areata and androgenetic alopecia in the People’s Republic of China. Patient Prefer Adherence. 2017;11:151–155. doi:10.2147/PPA.S121218
- Yu NL, Tan H, Song ZQ, Yang XC. Illness perception in patients with androgenetic alopecia and alopecia areata in China. J Psychosom Res. 2016;86:1–6. doi:10.1016/j.jpsychores.2016.04.005
- Chen D, Tuan H, Zhou EY, Liu D, Zhao Y, Picardo M. Quality of life of adult vitiligo patients using camouflage: a survey in a Chinese vitiligo community. PLoS One. 2019;14(1):e0210581. doi:10.1371/journal.pone.0210581
- An JG, Ma JH, Xiao SX, Xiao SB, Yang F. Quality of life in patients with lepromatous leprosy in China. J Eur Acad Dermatol Venereol. 2010;24(7):827–832. doi:10.1111/j.1468-3083.2009.03534.x
- van der Linden MM, van Rappard DC, Daams JG, Sprangers MA, Spuls PI, de Korte J. Health-related quality of life in patients with cutaneous rosacea: a systematic review. Acta Derm Venereol. 2015;95(4):395–400. doi:10.2340/00015555-1976
- Li J, Li M, Chen Q, Fu J, Zhang M, Hao F. Quality of life among patients with rosacea: an investigation of patients in China using two structured questionnaires. J Eur Acad Dermatol Venereol. 2016;30(10):e98–e99. doi:10.1111/jdv.13341
- Aksoy B, Altaykan-Hapa A, Egemen D, Karagöz F, Atakan N. The impact of rosacea on quality of life: effects of demographic and clinical characteristics and various treatment modalities. Br J Dermatol. 2010;163(4):719–725. doi:10.1111/j.1365-2133.2010.09894.x
- Wu Y, Fu C, Zhang W, Li C, Zhang J. The dermatology life quality index (DLQI) and the hospital anxiety and depression (HADS) in Chinese rosacea patients. Psychol Health Med. 2018;23(4):369–374. doi:10.1080/13548506.2017.1361540
- Cardwell LA, Farhangian ME, Alinia H, Kuo S, Feldman SR. Psychological disorders associated with rosacea: analysis of unscripted comments. J Dermatol surg. 2015;19(2):99–103.
- Kellett SC, Gawkrodger DJ. The psychological and emotional impact of acne and the effect of treatment with isotretinoin. Br J Dermatol. 1999;140(2):273–282. doi:10.1046/j.1365-2133.1999.02662.x
- Okhovat JP, Grogan T, Duan L, Goh C. Willingness to pay and quality of life in alopecia areata. J Am Acad Dermatol. 2017;77(6):1183–1184. doi:10.1016/j.jaad.2017.07.023
- Schiffner R, Brunnberg S, Hohenleutner U, Stolz W, Landthaler M. Willingness to pay and time trade-off: useful utility indicators for the assessment of quality of life and patient satisfaction in patients with port wine stains. Br J Dermatol. 2002;146(3):440–447. doi:10.1046/j.1365-2133.2002.04613.x
- Stefanidou M, Evangelou G, Kontodimopoulos N, et al. Willingness to pay and quality of life in patients with pruritic skin disorders. Arch Dermatol Res. 2019;311(3):221–230. doi:10.1007/s00403-019-01900-5